Embed Size (px)
Citation preview
1046 ACADEMIC EMERGENCY MEDICINE NOV 1997 VOL 4/NO 1 1
Case Management by Physician Assistants and Primary Care Physicians vs Emergency Physicians Alan J. Hirshberg, MD, MPH, C. James Holliman, MD, Richard C. Wuerz, MD, Dane M. Chapman, MD, PhD
I ABSTRACT
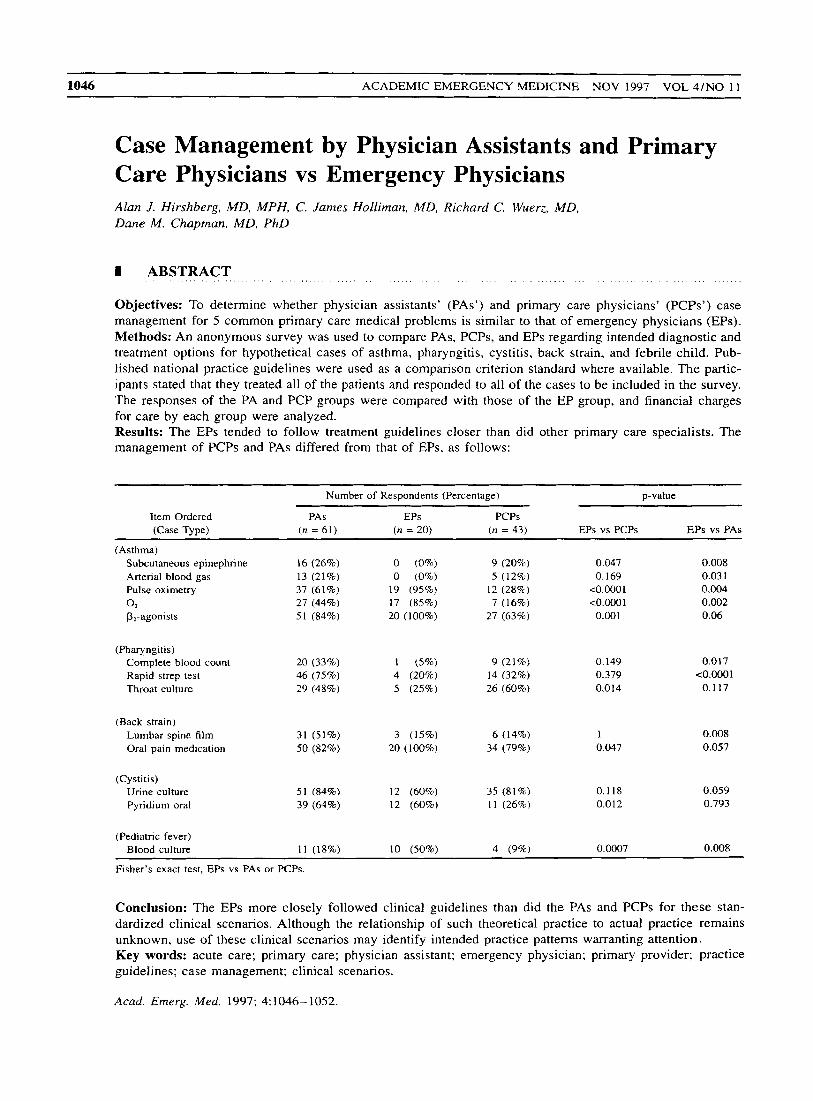
Objectives: To determine whether physician assistants’ (PAS’) and primary care physicians’ (PCPs’) case management for 5 common primary care medical problems is similar to that of emergency physicians (EPs). Methods: An anonymous survey was used to compare PAS, PCPs, and EPs regarding intended diagnostic and treatment options for hypothetical cases of asthma, pharyngitis, cystitis, back strain, and febrile child. Pub- lished national practice guidelines were used as a comparison criterion standard where available. The partic- ipants stated that they treated all of the patients and responded to all of the cases to be included in the survey. The responses of the PA and PCP groups were compared with those of the EP group, and financial charges for care by each group were analyzed. Results: The EPs tended to follow treatment guidelines closer than did other primary care specialists. The management of PCPs and PAS differed from that of EPs, as follows:
Number of Respondents (Percentage) p-value
Item Ordered PAS EPs PCPs (Case Type) (n = 61) (n = 20) f n = 43) EPs vs PCPs EPs vs PAS
(Asthma) Subcutaneous epinephrine 16 (26%) 0 (0%) 9 (20%) 0.047 0.008 Arterial blood gas 13 (21%) 0 (0%) 5 (12%) 0.169 0.03 1 Pulse oximetry 37 (61%) 19 (95%) 12 (28%) co.0001 0.004 0 2 27 (44%) 17 (85%) 7 (16%) <0.0001 0.002 P,-agonists 51 (84%) 20 ( 1 00%) 27 (63%) 0.001 0.06
(Pharyngitis) Complete blood count 20 (33%) 1 (5%) 9 (21%) 0.149 0.01 7
Throat culture 29 (48%) 5 (25%) 26 (60%) 0.014 0.117 Rapid strep test 46 (75%) 4 (20%) 14 (32%) 0.379 <O.o001
(Back strain) Lumbar spine film 31 (51%) 3 (15%) 6 (14%) 1 0.008 Oral pain medication 50 (82%) 20 (100%) 34 (79%) 0.047 0.057
(Cystitis) Urine culture Pyndium oral
51 (84%) 12 (60%) 35 (81%) 0.118 0.059 39 (63%) 12 (60%) 1 1 (26%) 0.012 0.793
(Pediatric fever) Blood culture 1 1 (18%) 10 (50%) 4 (9%) 0.0007 0.008
Fisher’s exact test, EPs vs PAS or PCPs.
Conclusion: The EPs more closely followed clinical guidelines than did the PAS and PCPs for these stan- dardized clinical scenarios. Although the relationship of such theoretical practice to actual practice remains unknown, use of these clinical scenarios may identify intended practice patterns warranting attention. Key words: acute care; primary care; physician assistant; emergency physician; primary provider; practice guidelines; case management; clinical scenarios.
Acad. Emerg. Med. 1997; 4:1046-1052.

Case Management by PAsPCPs vs EPs, Hirshberg rt al. 1047
I Emergency physicians (EPs) have been told that their care is “too expensive”’” compared with that of more cost-effective primary care physicians (PCPs) and physi- cian assistants PAS).^.^ However, we can find no objective evidence for these claims. If EPs truly practice more costly care, several situations may be occurring: 1) hos- pital overhead cost shifting may have inflated charges for ambulatory care in the ED and/or 2) EPs may have a more expensive approach to ambulatory problems (e.g., EPs might order more diagnostic tests, administer ineffective therapies, or perform interventions that result in more ad- verse events).
This study focuses on the second premise. While one cannot easily compare ED and primary care practices given individual patient differences and the various prac- tice constraints that each practitioner faces, i t is possible to evaluate how PCPs and PAS approach standardized clinical scenarios. The use of such scenarios allows us to evaluate how different practitioners would approach the same patient in the same situation. While this represents a hypothetical assessment of clinical practice. it does per- mit cross-specialty practice comparisons.
Our objective was to determine whether PAS and PCPs practice case management similar to that of EPs using 5 common primary care medical problems. Where available, we used practice guidelines to define desired practice. As a secondary outcome, we compared workup charges for the different practitioner groups. Our null hypothesis was that all groups would have similar clinical practices.
I METHODS
Study Design: We used an anonymous survey present- ing 5 ambulatory practice-based clinical scenarios to com- pare intended treatment practices and costs of 3 practi- tioner groups. The study participants chose from a menu of tests and treatments to evaluate and treat each case. The survey was administered to participants from Decem- ber 1994 through January 1995. The hypothetical case scenarios were derived from actual patient presentations at the site facility. The study met the expedited review criteria of the local institutional review board.
. . . . . . . . . , . . . . . . , . . . . . . . . . . . . . .
Front ?lie Pennsylvania State Uiii~~et-sity, Tlie Milton S. Hershey Medical Ceitrer. Hersliey9 PA. mid York Hospital. York. PA, YorWHersliey Emer- gency Residency Program (AJH, CJH, RCW, DMC). Current ofilia- rion: Washingtor7 Unii$ersiry School of Medicine. St. Louis, MO. Divi- sion of Eniergenry Medicine (DMC).
Rereir’edr Decrinbei- 3. 1996: revision received: Februaiy 18. 1997; secoiid revision: Apr-il 15. 1997: accepted: April 16. 1997.
Prior presenrarion: SAEM annual meeting, Denver; CO. Mny 1996
Address,for correspondence and reprints: Alan J . Hirshberg, MD. MPH, Certrer,for Eniergenry Medicul Services, Tlw Miltor? S. Hershev Medico1 Ceirter; P.0. Box 850, Hershev, PA 17033-0850. Fax: 717-531-1587: e- mail: ahir-shbe ~iirir.~irig.l inic,psu.edu
Participants: Practitioners were eligible to complete the survey if they stated that they treated patients in their practice similar to those in the scenarios. Survey respon- dents were included only if they completed all 5 cIinical scenarios. Every fifth PA was surveyed from the Pennsyl- vania state registry list (i.e., cross-sectional sample of reg- istered PAS). Physicians (staff PCPs and EPs) were sam- pled at the authors’ institutions, a community hospital Level-2 trauma center and a medical-school-associated Level- 1 trauma center and pediatric hospital. Surveys were distributed at hospital staff meetings. PCPs were de- fined as physicians listing their specialty as family prac- tice, internal medicine, obstetrics and gynecology, and pe- diatrics. The PAS and physicians had 2 months to complete the surveys; and “open book” approach was encouraged. The participants were informed in a cover letter that the anonymous survey “is part of a study to determine current practice patterns for common clinical problems.’ ’
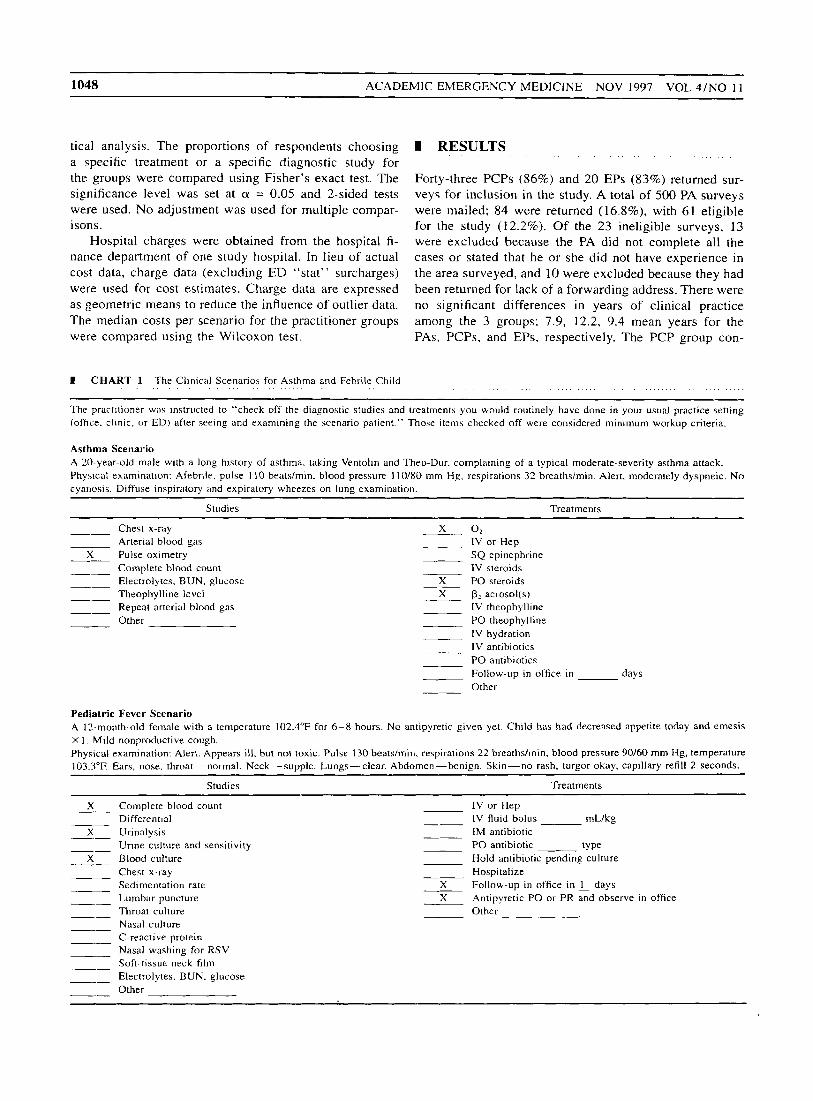
Measurements: The participants were asked to record the tests and treatments they would order for 5 hypothet- ical cases (asthma, pharyngitis, back strain, cystitis, and pediatric fever) according t o a checklist developed from a review of accepted guidelines, clinical experience, and published literature. The scenarios for asthma and pedi- atric fever are shown in Chart 1 . Other scenarios are avail- able from the authors.
National Institutes of Health asthma guidelines were used to compare the responses for the asthma case with a nationally accepted guideline for evaluation and treatment of acute Because there were no nationally ac- cepted guidelines for the other cases at the time of the study, published review articles from peer-reviewed jour- nals or texts dealing with primary care problems and available to primary caregivers were used to identify de- sired practice. Published review articles were used for the pharyngitis case.’.’ A textbook chapter and review article were used for the back strain case.”I0 Review articles were used for the cystitis case.l1.I2 Review articles and a prac- tice guideline were used for the pediatric fever c a ~ e . ’ ~ - ’ ’ Only one of these articles was published in the emergency medicine (EM) literature.
The following items were considered minimum re- quirements for case management: asthnra: P1-agonist aer- osol, oral steroids, O,, and pulse oximetry; pha~yngiris: antibiotic; back strain: pain medication; urirzary tract infection: urinalysis and antibiotic; and pediatric fever: antipyretic, blood culture, urinalysis, complete blood count, and follow-up visit in 1 day.
Data Analysis: Responses were entered into a Lotus 1-2-3 Version 2.4 spreadsheet (Lotus Development Cor- poration, Cambridge, MA) and KwikStat 4.0 statistical program (Texasoft. Cedar Hill, TX) for descriptive statis-
- 1048 ACADEMIC EMERGENCY MEDICINE NOV 1997 VOL 4/NO 1 1
tical analysis. The proportions of respondents choosing a specific treatment or a specific diagnostic study for the groups were compared using Fisher’s exact test. The significance level was set at (Y = 0.05 and 2-sided tests were used. No adjustment was used for multiple compar- isons.
Hospital charges were obtained from the hospital fi- nance department of one study hospital. In lieu of actual cost data, charge data (excluding ED “stat” surcharges) were used for cost estimates. Charge data are expressed as geometric means to reduce the influence of outlier data. The median costs per scenario for the practitioner groups were compared using the Wilcoxon test.
1 CHART 1 The Clinicdl Scenario5 for Asthma and Febrile Child
I RESULTS
Forty-three PCPs (86%) and 20 EPs (83%) returned sur- veys for inclusion in the study. A total of 500 PA surveys were mailed; 84 were returned (16.8%), with 61 eligible for the study (12.2%). Of the 23 ineligible surveys, 13 were excluded because the PA did not complete all the cases or stated that he or she did not have experience in the area surveyed, and 10 were excluded because they had been returned for lack of a forwarding address. There were no significant differences in years of clinical practice among the 3 groups; 7.9, 12.2, 9.4 mean years for the PAS, PCPs, and EPs, respectively. The PCP group con-
The practitioner was instructed to “check off the diagnostic studies and treatments you would routinely have done in your usual practice setting (office. clinic, or ED) after seeing and examining the scenario patient.” Those items checked off were considered minimum workup criteria.
Asthma Scenario A 10-year-old male with a long history of asthma. taking Ventolin and Theo-Dur. complaining of a typical moderate-severity asthma attack. Physical examination: Afebrile. pulse 1 10 bentdmin. blood pressure I 1 O B O mm Hg, respirations 32 breathsfinin. Alert, moderately dyspneic. No cyariosis. Diffuse inspiratory and expiratory wheezes on lung examination.
Studies Treatments
_- Chest x-ray x 0 2
Arterial blood gas IV or Hep
Complete blood count IV steroids Electrolytes, BUN, glucose X PO steroids Theophylline level X p2 aerosol(s) Repeat arterial blood gas IV theophylline Other PO theophylline
1V hydration IV antibiotics PO antibiotics Follow-up in office in days Other
-- X Pulse oximetry SQ epinephrine
__ __- -- __-
Pediatric Fever Scenario A 12-month-old female with a temperature 102.4”F for 6-8 hours. No antipyretic given yet. Child has had decreased appetite today and emesis X 1 . Mild nonproductive cough. Physical examination: Alert. Appears ill. but not toxic. Pulse 130 beatsimin, respirations 22 breathshin. blood pressure 90/60 mm Hg, temperature 103.:V’F. Ears, nose. throat-normal. Neck-supple. Lungs-clear. Abdomen-benign. Skin-no rash, turgor okay, capillary refill 2 seconds.
Studies Treatments
X Complete blood count IV or Hep Differential IV fluid bolus mUkg
X Urinalysis IM antibiotic Urine culture and sensitivity PO antibiotic type
X Blood culture Hold antibiotic pending culture Chest x-ray Hospitalize Sedimentation rate X Follow-up in office in 1 days Lumbar puncture Throat culture Other Nasal culture C-reactive protein Nasal washing for RSV Soft-tissue neck film Electrolytes. BUN. glucose Other
-- ___ ~- -- -- ___
X Antipyretic PO or PR and observe in office -_ ~- ~-
~- ~- -- -- __-
Case Management by PAsL'CPs vs EPs, Hirshber-E et ul. 1049
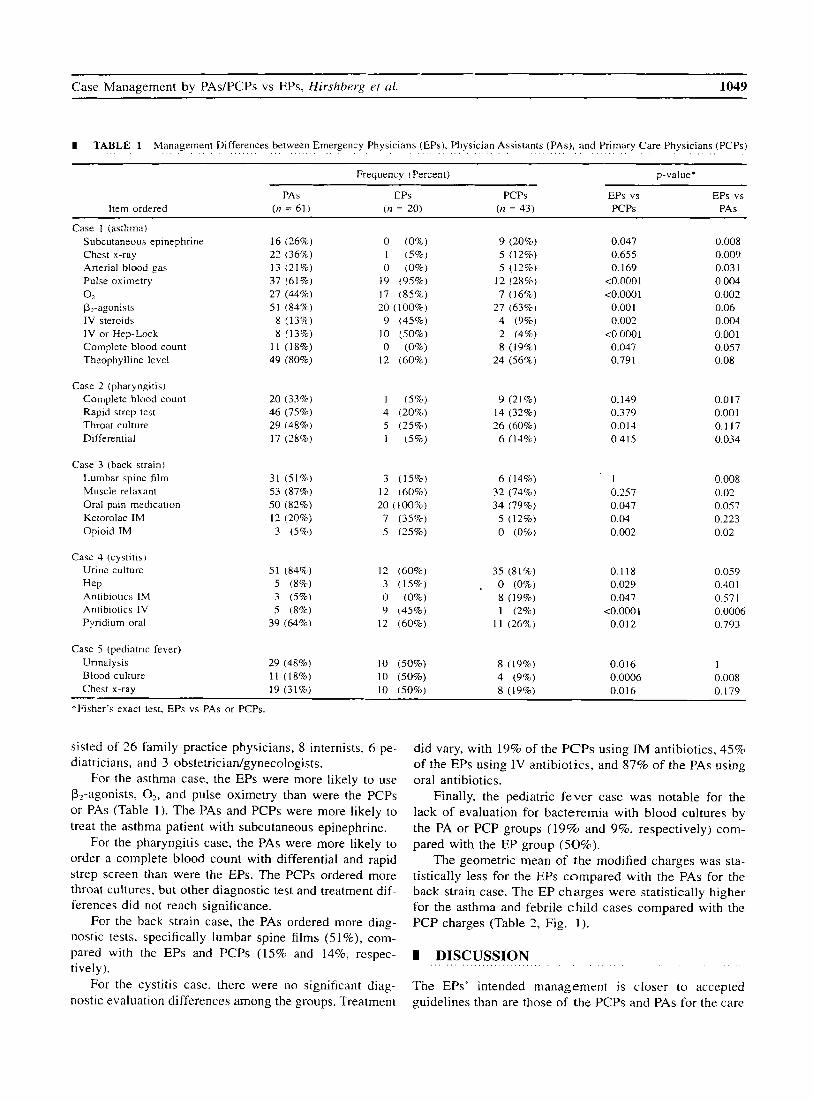
I TABLE 1 Management Differences between Emergency Physicians (EPs), Physician Assistants (PAS), and Primary Care Physicians (PCPs)
Frequency (Percent) p-value*
PAS EPs PCPs EPs vs EPs vs Item ordered (n = 61) ( n = 20) (n = 43) PCPs PAS
Case 1 (asthma) Subcutaneous epinephrine Chest x-ray Arterial blood gas Pulse oximetry
P,-agonists IV steroids IV or Hep-Lock Complete blood count Theophylline level
0 2
16 (26%)
13 (21%) 37 (61%) 27 (44%) 51 (84%)
8 (13%) 1 1 (18%)
22 (36%)
8 (13%')
49 (80%)
0 (0%) 1 ( 5 % ) 0 (0%)
19 (95%) 17 (85%) 20 ( 100%) 9 (45%)
10 (50%) 0 (0%)
12 (60%)
9 (20%) 5 (12%) 5 (12%)
12 (28%) 7 (16%)
4 (9%)
8 (19%) 24 (56%)
27 (63%)
2 (4%)
0.047 0.655 0.169
<o.ooo 1 <0.0001
0.001 0.002
<0.0001 0.047 0.791
0.008 0.009 0.03 1 0.004 0.002 0.06 0.004 0.001 0.057 0.08
Case 2 (pharyngitis) Complete blood count 20 (33%) 1 ( 5 % ) 9 (21%) 0.149 0.017
Throat culture 29 (48%) 5 (25%) 26 (60%) 0.014 0.1 17 Differential 17 (28%) 1 (5%) 6 (14%) 0.415 0.034
Rapid strep test 46 (75%) 4 (20%8) 14 (32%) 0.379 0.001
Case 3 (back strain) Lumbar spine film Muscle relaxant Oral pain medication Ketorolac IM Opioid IM
Case 4 (cystitis) Urine culture
Antibiotics IM Antibiotics I V Pyridium oral
HeP
31 (51%) 3 (15%) 6 (14%) 1 0.008 53 (87%) 12 ( 6 0 8 ) 32 (74%) 0.257 0.02 50 (82%) 20 (100%) 34 (79%) 0.047 0.057 12 (20%) 7 (35%) 5 (12%) 0.04 0.223 3 ( 5 % ) 5 (15%) 0 (0%) 0.002 0.02
51 (84%) 12 (60%) 35 (81%) 0.118 0.059 5 (8%) 3 (15%) . 0 (0%) 0.029 0.401 3 (5%) 0 (0%) 8 (19%) 0.047 0.57 I
39 (64%) 12 (60%) 11 (26%) 0.01 2 0.793 0.0006 <0.0001 5 (8%) 9 (45%) 1 (2%)
Case 5 (pediatric fever) Urinalysis 29 (48%) 10 (50%) 8 (19%) 0.0 16 1 Blood culture 11 (18%) 10 (50%) 4 (9%) 0.0006 0.008 Chest x-ray 19 (31%) 10 (50%) 8 (19%) 0.016 0.179
*Fisher's exact test, EPs vs PAS or PCPs.
sisted of 26 family practice physicians, 8 internists, 6 pe- diatricians, and 3 obstetrician/gynecologists.
For the asthma case, the EPs were more likely to use P2-agonists, O?, and pulse oximetry than were the PCPs or PAS (Table 1). The PAS and PCPs were more likely to treat the asthma patient with subcutaneous epinephrine.
For the pharyngitis case, the PAS were more likely to order a complete blood count with differential and rapid strep screen than were the EPs. The PCPs ordered more throat cultures, but other diagnostic test and treatment dif- ferences did not reach significance.
For the back strain case, the PAS ordered more diag- nostic tests, specifically lumbar spine films ( 5 1 %), com-
did vary, with 19% of the PCPs using IM antibiotics, 45% of the EPs using IV antibiotics, and 87% of the PAS using oral antibiotics.
Finally, the pediatric fever case was notable for the lack of evaluation for bacteremia with blood cultures by the PA or PCP groups (19% and 9%. respectively) com- pared with the EP group (50%).
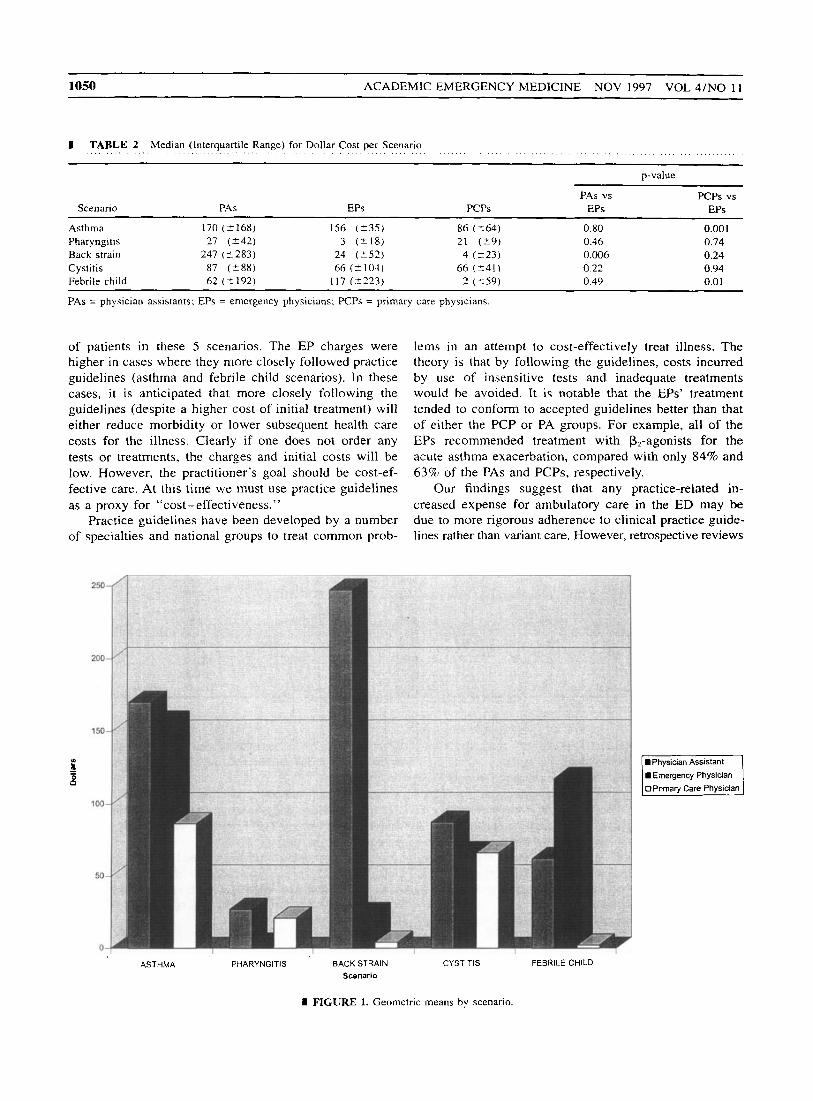
The geometric mean of the modified charges was sta- tistically less for the EPs compared with the PAS for the back strain case. The EP charges were statistically higher for the asthma and febrile child cases compared with the PCP charges (Table 2, Fig. 1).
pared w~th the EPs and PCPs (15% and 14%, respec- I DISCUSSION tively).
For the cystitis case, there were no significant diag- nostic evaluation differences among the groups. Treatment
The EPs' intended management is closer to accepted guidelines than are those of the PCPs and PAS for the care
~~
1050 ACADEMIC EMERGENCY MEDICINE NOV 1997 VOL 4/NO 11
I TABLE 2 Median (Interquartile Range) for Dollar Cost per Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ( . . _ ( . .
~ ~~~
p-value
PAS vs PCPS vs Scenario PAS EPs PCPS EPs EPs
Asthma 170 (2168) 156 ( 2 3 5 ) 86 (264) 0.80 0.001 Pharyngi tis 27 (242) 3 (218) 21 (Z9) 0.46 0.74 Back strain 247 (5283) 24 ( 2 5 2 ) 4 (223) 0.006 0.24 Cystitis 87 (588) 66 (2104) 66 (+41) 0.22 0.94 Febrile child 62 (2192) 117 (2223) 2 ( 2 5 9 ) 0.49 0.01
PAS = physician assistants; EPs = emergency physicians; PCPs = primary care physicians
of patients in these 5 scenarios. The EP charges were higher in cases where they more closely followed practice guidelines (asthma and febrile child scenarios). In these cases, i t is anticipated that more closely following the guidelines (despite a higher cost of initial treatment) will either reduce morbidity or lower subsequent health care costs for the illness. Clearly if one does not order any tests or treatments, the charges and initial costs will be low. However, the practitioner’s goal should be cost-ef- fective care. At this time we must use practice guidelines as a proxy for “cost-effectiveness.”
Practice guidelines have been developed by a number of speci
250
2GO
150
r - - 0 0
100
50
ies and national groups to treat common prob-
lems in an attempt to cost-effectively treat illness. The theory is that by following the guidelines, costs incurred by use of insensitive tests and inadequate treatments would be avoided. It is notable that the EPs’ treatment tended to conform to accepted guidelines better than that of either the PCP or PA groups. For example, all of the EPs recommended treatment with P,-agonists for the acute asthma exacerbation, compared with only 84% and 63% of the PAS and PCPs, respectively.
Our findings suggest that any practice-related in- creased expense for ambulatory care in the ED may be due to more rigorous adherence to clinical practice guide- lines rather than variant care. However, retrospective reviews
Emergency Physician
ASTHMA PHARYNGlTiS BACK STRAIN CYSTITIS FEBRILE CHILD Scenario
I FIGURE 1. Geometric means by scenario.

Case Management by PAs/PCPs vs EPs, Hirshberg et al. 1051
of ED care and charges that are based on diagnostic- related group (DRG) codes as derived from ED final diagnoses are p r ~ b l e m a t i c . ' ~ - ' ~ Such reviews do not ac- count for the prospective evaluation of more serious en- tities with a similar clinical presentation nor do they ad- dress hospital cost shifting. Cost-shifted charges occur as the hospital attempts to offset uncompensated care (in the ED or elsewhere in the hospital), thus increasing the charge to the paying patient andor the third-party payer for the emergency services.
Interestingly, a recent analysis suggests that despite hospital cost shifting, the marginal cost of managing pa- tients with common primary care problems in the ED may be comparable to that of other practice settings, especially during times when primary care sites are closed.'' Fur- thermore, others have suggested that the proportion of health care costs that is devoted to ED care for ambulatory problems represents ~ 0 . 5 % of health care costs.2' Hence, efforts to nationally save health care dollars by shifting ambulatory care may be better focused elsewhere.
I LIMITATIONS AND FUTURE QUESTIONS
The study has several limitations. First, intended treatment plans were surveyed, and the actual care provided was not measured. As noted previously, it would be costly and logistically challenging to identify similar patients in each of these categories who were treated by each of the prac- titioners for a fair comparison of actual practices. Mock (standardized) patients might be one method to perform such an investigation.
Second, a number of sample biases exist. We were dependent on respondent volunteerism. Given the low re- sponse rate of the PA group, one must question the rep- resentativeness of that group. However, many of the PAS who received a survey did not treat primary care problems (i.e., they dealt with specialized care such as neurosurgical or cardiac bypass patients) and therefore could not be in- cluded in the data analysis. Also, it is likely that those PAS who responded may be the most committed to their practice. Yet, these PAS at best are representative of PAS in Pennsylvania. Evaluation of PAS from other states using these or similar scenarios is warranted. Furthermore, we sampled clinicians at only 2 teaching institutions. Re- gional biases and differences between clinical practices at a pure community hospital vs an academic institution must also be acknowledged.
Third, the selection of articles for documentation of desired practice was arbitrary. However. the choice was biased toward articles outside the EM literature. There- fore, clinical practice by the PCPs would be favored.
Fourth, the actual costs of treatments and diagnostic studies are unknown; however, we applied the same es- timates to all practitioners. Hence, while there may be
. . . . . . . . . . . . . . . . . . . . . . . . . . .
some treatments or diagnostic studies that were dispro- portionately high, the estimated costs associated with sce- nario management by all practitioner groups were equally affected.
Future studies can use these and other clinical scenar- ios to clarify intended practice patterns among practitioner groups. Such analyses could compare intended practice with clinical practice guidelines. Used in this manner, practice guidelines that clash with stated intended practice should be carefully scrutinized to ascertain the source of the conflict. Where the guidelines are based on outcomes evidence, such a conflict highlights the need for clinical guidelines dissemination. Where the guidelines are based on expert opinion, such a conflict should stimulate objec- tive investigation to sort fact from preference.
I CONCLUSIONS
The intended practice of EPs in these standardized patient scenarios more closely followed accepted practice guide- lines than did that of the surveyed PCPs and PAS. The use of clinical scenarios to track intended practice among spe- cialties may be a valuable tool for evaluating clinical prac- tice guideline acceptance. The role of these hypothetical case scenarios as a marker for actual clinical practice re- quires further evaluation.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
The authors thank Donna Rentzel for her work in preparing the man- uscript and Dr. Vernon Chinchilli and the Penn State University Center for Biostatistics for their review a n d confirmation of the statistical anal- ysis.
I REFERENCES
1. Remarks by the President and the First Lady to the medical com- munity of Johns Hopkins University, Oct 28, 1993, Newton White Ath- letic Center. Baltimore. MD, The White House. Office of the Press Secretary. 2. Address of the President to the Joint Session of Congress, U.S. Cap- itol. Sept 22. 1993, The White House, Office of the Press Secretary. 3. Baker LC, Baker LS. Excess cost of emergency department visits for nonurgent care. Health Aff (Millwood). 1994; 13:162-71. 4. Frank B. Emergency room care drives up costs: doctors. Houston Post. Jan 23, 1994, p A26. 5. Executive Summary: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: NHLBI, NIH Publication No. 91-3042A. Jun 1991, pp 21 -36. 6. International consensus report on diagnosis and treatment of asthma. Bethesda, MD: NHLBI. NIH Publication No. 92-3091. Eur Respir J.
7. Paradise JL. Etiology, diagnosis, and antimicrobial treatment of phar- yngitis and pharyngotonsillitis. A n n Otol Rhino1 Laryngol. 1981 ; 9O(suppl 3):75-8. 8. Kline JA. Runge JW. Streptococcal pharyngitis: a review of patho- physiology. diagnosis. and management. J Emerg Med. 1994; 12:665- 80. 9. Branch WT Jr (ed). Office Practice of Medicine, 2nd Edition. Phil- adelphia: W. B. Saunders, 1987, p p 875-97. 10. Margo K. Diagnosis. treatment and prognosis in patients with low back pain. Am Fam Physician. 1994; 49:171-9, 183-4. 11. Childs S. Current diagnosis a n d treatment of urinary tract infec-
1992; 5:601-41.
1052 ACADEMIC EMERGENCY MEDICINE NOV 1997 VOL 4 / N O 1 1
tions. Urology. 1992; 40:295-9. 12. Johnson JR. Stamm WE. Urinary tract infections in women: diag- nosis and treatment. Ann Intern Med. 1989; 11 I :906- 17. 13. Baraff LJ. Bass JW, Fleisher GR. et al. Practice guidelines for the management of infants and children 0 to 36 months of age with fever without source. Pediatrics. 1993: 92: 1 - I 1 . 14. AItieri MF. Bothner J. Avner JR. Controversies in pediatric emer- gency medicine. To do or not to do. Pediatr Emerg Care. 1993; 9: I71 - 3 . 15. Ipp M, Jaffe D. Physicians' attitudes toward the diagnosis and man- agement of fever in children 3 months to 2 years of age. Clin Pediatr. 1993; 32:66-70. 16. Fleming N. Jones H. The impact of outpatient and emergency room use on costs in the Texas Medicaid program. Med Care. 1983; 21:
892-910. 17. Mufioz E, Laughlin A. Regan DM. Teicher I , Margolis IB, Wise L. The financial effects of emergency department-generated admissions under prospective payment systems. JAMA. 1985; 254: 1763-71. 18. Muiioz E, Soldano R. Laughlin A. Margolis IB. Wise L. Source of admission and cost: public hospitals face financial risk. Am J Public Health. 1986; 76:696-7. 19. Lapidus CS. Schwarz DF, Honig PJ. Atopic dermatitis in children: Who cares? Who pays? J Am Acad Dermatol. 1993; 28:699-703. 20. Williams RM. The costs of visits to emergency departments. N Engl J Med. 1996; 334:642-6. 21. Tyrance PH Jr, Himmelstein DU. Woolhandler S. US emergency department costs: no emergency. Am J Public Health. 1996; 86:1527- 31.
Victimization from Physical Violence in Pennsylvania: Prevalence and Health Care Use Samuel N. Forjuoh, MB. ChB. DrPH, Janet M. Kinnnne, MD. Jeffrey H. Coben. MD, Stephen R. Deamwter: MS, Thomas J. Songer: PhD
I ABSTRACT
Objectives: To determine the prevalence of interpersonal physical violence (IPV) among Pennsylvania adults, to identify the personal characteristics of the victims, and to determine their health care use for resulting injuries. Methods: Population-based data describing physical violence were obtained through a statewide telephone survey of 3,620 Pennsylvania adults selected from households by random-digit dialing in 1994. The prevalence and 95% confidence interval (95% CI) of victimization from IPV along with ED or other medical care facility use for IPV-related injuries were computed by several personal characteristics. Logistic regression was used to compare victims of IPV and their levels of health care use. Results: The prevalence of reported victimization from IPV was 5.6% (95% CI = 4.9, 6.3). Significantly more victimization was reported by males, persons aged 18-29 years, those employed, and unmarried persons. The proportion of victims who reported to have gone to an ED or other medical care facility for IPV-related injury treatment was 12.9%. Significantly more persons with annual household incomes <$20,000 reported health care use for injuries resulting from IPV than did those with incomes of 2$20,000 (OR = 3.98; 95% CI = 1.27, 12.48). Health care use for injuries was not found to be related to gender, age. race, employment, or marital status. Conclusions: This population-based study of health care use for IPV-related injuries found that victims of physical violence in Pennsylvania were not only young and unmarried men, but also employed. Health care use for resulting injuries was greater among persons with lower incomes. Key words: health care use; emergency department, Pennsylvania; physical violence; injury; prevalence: victimization.
Acad. Emerg. Med. 1997; 4: 1052- 1058.
From the Unitvrsim of Pittsburgh. Pirtsburgll, PA, Department of Received: January 29. 1997: revision received: April 21, 1997; ac- Emerxency Medicine and Center f o r l n j u y Research and Control (SNF. J M K . JHC. SRD) and Department of Epideniiology (TJS): Chil- dren Y Hospital of Pittsburgh. Pittsburgh. PA, Department of Pediar- rics. Division of Emeyqencv Medicine (JMK): and the Deportment of Heulrh Services Adminisrration. University of Pirr.rburgh, Pittsburgh. PA (JHC). Current afiliarrori: Allegheny Uni t~ers ih~ of the Henlth Sci- ences. Pittsburgh. PA. Depurtnient of Emergency Medicine ( S N E JHC, SRD). sforjuoh @pgh.auhs.edu
cepted: April 26, 1997; updated: May 10. 1997.
Address f o r correspondence and reprints: Samuel N. Forjuoh. MB. ChB. DrPH. Center f o r Violence arid Iii juty Control. Department of Emergency Medicine, Allegheny University of the Health Sciences, 320 East North AL'enue. Pitrshurgh. PA 15212. Fax: 412-330-6122: e-mail: