Embed Size (px)
Citation preview

Case ReportEpithelial Cyst in the Posterior Triangle of the Neck:Atypical Branchial Cyst or Cystic Lymph Node Metastasis?
Domenic Vital,1 Gerhard F. Huber,1 Thomas F. Pézier,1 Matthias Rössle,2
Rudolf Probst,1 and Gian-Marco Widmer1
1 Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital of Zurich, Frauenklinikstrasse 24,8091 Zurich, Switzerland
2 Institute of Surgical Pathology, University Hospital of Zurich, Schmelzbergstrasse 12, 8091 Zurich, Switzerland
Correspondence should be addressed to Domenic Vital; [email protected]
Received 14 October 2013; Accepted 16 December 2013; Published 12 January 2014
Academic Editors: N. G. Iyer, M. T. Kalcioglu, and H.-S. Lin
Copyright © 2014 Domenic Vital et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
We report the case of a 66-year-old man with a cervical neck mass located behind the left sternocleidomastoid muscle. To excludemalignancy, a full workup, including clinical, radiological, and cytological examination, was performed but failed to provide adefinitive diagnosis. Histological analysis following excisional biopsy revealed a benign epithelial cyst, consistent with an atypicallylocated branchial cyst.We describe an approach to themanagement of these neckmasses and discuss several theories of the etiologyof branchial cysts and how they may come to be abnormally located.
1. Case Presentation
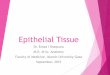
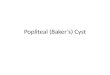
A 66-year-old man was referred to our department with a 2-day history of a painless left cervical neck mass. He deniedany other symptoms and reported that he only occasionallydrank alcohol and had stopped smoking some 30 years agowith a total of 10 pack years. Clinical examination revealed awell-defined, painless neck lump, posterior to the sternoclei-domastoid muscle close to the mastoid. The lump was some5 centimeters in size, roughly oval, and not fixed to adjacentstructures. There were no surrounding skin changes or otherassociated findings. Intraoral examination and transnasalfiber-endoscopy were normal. Cervical ultrasound showedan irregularly walled mass, 5 cm in diameter, with hypere-chogenic reflections in an echo-poor center. The other neckstructures were sonographically normal. Magnetic resonanceimaging (MRI) showed a cystic lesion with an irregularwall lateral and posterior to the sternocleidomastoid muscle(neck level five; see Figures 1 and 2). Repeated fine-needleaspiration cytology (FNAC) revealed squamous epithelialcells without signs of malignancy, consistent with a branchialcleft cyst. However, given the patient’s age and the atypicallocalization, the differential diagnosis included a metastasis
of a well-differentiated squamous cell carcinoma (SCC).We therefore recommended the patient to undergo panen-doscopy and extirpation of the mass with intraoperativefrozen section analysis of the specimen. The patient agreedwith neck dissection in case of malignancy. Panendoscopyrevealed no extra findings, and both intraoperative frozensection and definitive histology of the excisional biopsyconfirmed a branchial cleft cyst. The patient recovered wellafter surgery and was discharged from follow up 12 monthslater.
2. Discussion
In patients older than 40 years, especially with risk factorsfor malignant disease, it is prudent to consider all cysticlesions of the neck as malignant until proven otherwise. Inpatients younger than 40 years, clinicians should be awareof a metastasis of a papillary thyroid carcinoma [1]. Aftera careful history and thorough clinical examination furtherinvestigations should include ultrasonography of the neckincluding FNAC and 3-dimensional imaging either withcomputed tomography (CT) or MRI. Ultrasound-guidedFNAC is often diagnostic but its sensitivity drops from >95%
Hindawi Publishing CorporationCase Reports in OtolaryngologyVolume 2014, Article ID 912347, 3 pageshttp://dx.doi.org/10.1155/2014/912347

2 Case Reports in Otolaryngology
Figure 1: Axial slides of T1-weighted MRI showing a hyperintensecystic lesion behind the left sternocleidomastoid muscle in the necklevel five.
Figure 2: Axial slides of T2-weighted MRI showing a hyperintensecystic lesion behind the left sternocleidomastoid muscle in the necklevel five.
in solid tumors [2–4] to 50%–73% in cystic lesions [5–7]. IfFNAC fails to provide a definitive diagnosis, we recommendfurther diagnostic steps including panendoscopy of the upperaerodigestive tract and excision of the cystwith intraoperativefrozen section.
In terms of malignant lesions, squamous cell carcinoma(SCC) of Waldeyer’s ring (e.g., palatine and lingual tonsils)and papillary thyroid cancers have a predilection for cysticlymph node metastases [2, 8, 9]. However, the exact mecha-nism for the development of cystic lymph node metastasesis unclear. Tumor necrosis forming a pseudocyst has beenfound as well as true cystic cavities lined by neoplasticepithelium. Indeed, the expression of cytokeratin 7 has ledsome to hypothesize that a subset of SCC of Waldeyer’s ringmight originate from excretory ducts ofminor salivary glandsand therefore show the tendency to form cystic lesions [10].
The aetiology of benign cervical cysts is also unclear. Themost popular, but still controversial, theory is the branchialapparatus theory first described by Von Ascherson in 1832.Unfortunately, atypical locations of branchial cysts are poorlyexplained by this theory, and alternatives have been proposedsuch as the cervical sinus theory, the thymopharyngealtheory, and the inclusion theory [11–13]. The cervical sinustheory is an extension of the branchial apparatus theoryfocusing on lateral cervical cysts. It considers that branchialfistulae were related to the cervical sinus rather than thepharyngeal clefts and pouches. Other authors hypothesizedthat the development of lateral cervical cysts is linked to theembryology of the thymus, which originates from the thirdpharyngeal pouch via the thymopharyngeal duct.
Consequently, the thymopharyngeal theory indicates thatlateral cervical cysts are a result of an incomplete obliterationof the thymopharyngeal duct [14].
Reporting a similar case to our own, Grignon et al.[15] proposed that the location of the branchial cyst wasthe result of the organogenesis of the sternocleidomastoidmuscle, which is independent of the development of thebranchial apparatus and proceeds in a craniocaudal anddorsoventral fashion. It therefore would predict that cranialbranchial cysts would be located anteriorly to the muscle,and a caudal branchial cyst posteriorly [15]. Bhaskar andBernier [13] examined 468 specimens of branchial cysts andproposed that most of the branchial cysts represent cysts inlymph nodes, which originated from inclusion of epitheliumduring embryogenesis (so-called “inclusion theory”). Theirconclusions helped to explain three findings which seeminconsistent with Grignon’s theory: (1) the presence of sur-rounding lymphoid tissue such as sinusoids in the cysts, (2)size fluctuations during infections of the upper aerodigestivetract, and (3) the fact that the cysts are hardly ever seenat birth. Consequently, it was proposed to use the term“benign lymphoepithelial cyst” instead of “branchial cyst” [13].Furthermore, this theory also explains the rare cyst locationposterior to the sternocleidomastoid muscle. Indeed, in theirseries, Bhaskar and Bernier found 5 of the 468 cysts locatedin the posterior part of the neck triangle (neck level five) [13].
3. Conclusion
The diagnosis of a branchial cyst should—especially inpatients older than 40 years—only be considered oncemalignancy has been excluded and should not be discountedbecause of an atypical location. Whilst in older patientsmetastatic SCC is more likely, in younger patients metastaticpapillary thyroid cancer should be considered. Several theo-ries exist as to the aetiology of branchial cyst formation, andsome, such as the inclusion theory, are better able to explainabnormal locations.
Conflict of Interests
The authors declare no conflict of interests.

Case Reports in Otolaryngology 3
References
[1] J. Sira andZ.G.G.Makura, “Differential diagnosis of cystic necklesions,”The Annals of Otology, Rhinology and Laryngology, vol.120, no. 6, pp. 409–413, 2011.
[2] P. Firat, C. Ersoz, A. Uguz, and S. Onder, “Cystic lesions ofthe head and neck: cytohistological correlation in 63 cases,”Cytopathology, vol. 18, no. 3, pp. 184–190, 2007.
[3] U. Engzell and J. Zajicek, “Aspiration biopsy of tumors of theneck. I. Aspiration biopsy and cytologic findings in 100 cases ofcongenital cysts,” Acta Cytologica, vol. 14, no. 2, pp. 51–57, 1970.
[4] A. Dejmek and K. Lindholm, “Fine needle aspiration biopsy ofcystic lesions of the head and neck, excluding the thyroid,” ActaCytologica, vol. 34, no. 3, pp. 443–448, 1990.
[5] P. Sheahan, G. O’Leary, G. Lee, and J. Fitzgibbon, “Cysticcervical metastases: incidence and diagnosis using fine needleaspiration biopsy,” Otolaryngology—Head and Neck Surgery,vol. 127, no. 4, pp. 294–298, 2002.
[6] G. Granstrom and S. Edstrom, “The relationship betweencervical cysts and tonsillar carcinoma in adults,” Journal of Oraland Maxillofacial Surgery, vol. 47, no. 1, pp. 16–20, 1989.
[7] C. G. Gourin and J. T. Johnson, “Incidence of unsuspectedmetastases in lateral cervical cysts,” Laryngoscope, vol. 110, no.10, pp. 1637–1641, 2000.
[8] Y. Mallet, B. Lallemant, Y. M. Robin, and J. L. Lefebvre,“Cystic lymph node metastases of head and neck squamous cellcarcinoma: pitfalls and controversies,” Oral Oncology, vol. 41,no. 4, pp. 429–434, 2005.
[9] D. Goldenberg, J. Sciubba, and W. M. Koch, “Cystic metastasisfrom head and neck squamous cell cancer: a distinct diseasevariant?” Head and Neck, vol. 28, no. 7, pp. 633–638, 2006.
[10] S. Regauer, A. Beham, and S. Mannweiler, “CK7 expression incarcinomas of the Waldeyer’s ring area,” Human Pathology, vol.31, no. 9, pp. 1096–1101, 2000.
[11] N. Papadogeorgakis, V. Petsinis, E. Parara, K. Papaspyrou, L.Goutzanis, and C. Alexandridis, “Branchial cleft cysts in adults.Diagnostic procedures and treatment in a series of 18 cases,”Oral and Maxillofacial Surgery, vol. 13, no. 2, pp. 79–85, 2009.
[12] S. S. Choi and G. H. Zalzal, “Branchial anomalies: a review of 52cases,” Laryngoscope, vol. 105, no. 9, pp. 909–913, 1995.
[13] S. N. Bhaskar and J. L. Bernier, “Histogenesis of branchial cysts:a report of 468 cases,” The American journal of pathology, vol.35, no. 2, pp. 407–443, 1959.
[14] J. Golledge and H. Ellis, “The aetiology of lateral cervical(branchial) cysts: past and present theories,” The Journal ofLaryngology and Otology, vol. 108, no. 8, pp. 653–659, 1994.
[15] B. Grignon, F. Pierucci, M. Wayoff, and J. Roland, “Branchialcyst of unusual localization: report of a case and considerationson organogenesis,”Morphologie, vol. 81, no. 254, pp. 9–11, 1997.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com