Embed Size (px)
DESCRIPTION
Ophthalmology
Citation preview

Cataracts in congenital toxoplasmosis
Veena Arun, MD,a A. Gwendolyn Noble, MD, PhDb
and other members of the Toxoplasmosis Study Group
PURPOSE To determine the incidence and natural history of cataracts in children with congenitaltoxoplasmosis.
METHODS Children referred to the National Collaborative Chicago-based Congenital Toxoplasmo-sis Study (NCCCTS) between 1981 and 2005 were examined by ophthalmologists atpredetermined times according to a specific protocol. The clinical course and treatmentof patients who developed cataracts were reviewed.
RESULTS In the first year of life, 134 of 173 children examined were treated with pyrimethamine,sulfadiazine, and leukovorin, while the remaining 39 were not treated. Cataracts occurredin 27 eyes of 20 patients (11.6%, 95% confidence interval [7.2%, 17.3%]). Fourteencataracts were present at birth and 13 developed postnatally. Locations of the cataractsincluded anterior polar (three eyes), anterior subcapsular (six eyes), nuclear (five eyes),posterior subcapsular (seven eyes), and unknown (six eyes). Thirteen cataracts were partial,nine total, and five with unknown complexity. Twelve cataracts remained stable, 12progressed, and progression was not known for 3. Five of 27 eyes had cataract surgery,with 2 of these developing glaucoma. Sixteen eyes of 11 patients had retinal detachmentand cataract. All eyes with cataracts had additional ocular lesions.
CONCLUSIONS In the NCCCTS cohort, 11.6% of patients were diagnosed with cataracts. There wasconsiderable variability in the presentation, morphology, and progression of the cataracts.Associated intraocular pathology was an important cause of morbidity. ( J AAPOS 2007;11:551–554)
C ongenital toxoplasmosis causes substantial visual andneurologic morbidity.1-11 Even treatment initiated atbirth may commence too late to prevent ocular dam-
age.1,2,8,11 Cataracts in children with congenital toxoplasmo-sis have been described by others.11 We previously describedour experience in the National Collaborative Chicago-basedCongenital Toxoplasmosis Study (NCCCTS) for the first 75children, of whom 7 (9.3%) had cataracts.8 To better un-derstand how cataracts manifest in children with congen-ital toxoplasmosis, we further studied the characteristicsand natural history of cataracts in the updated NCCCTScohort of 173 children followed prospectively and longi-tudinally from 1981 to 2005.1
Author affiliations: aDepartment of Ophthalmology and Visual Sciences, The Universityof Chicago, Chicago, Illinois; bDivision of Ophthalmology, Children’s MemorialHospital, Northwestern University Feinberg School of Medicine, Chicago, Illinois
This work was not presented at the AAPOS annual meeting or any other nationalmeeting. This work was supported by Grant RO1 AI27530 from NIAID-TMP and theResearch to Prevent Blindness Foundation.
Submitted October 11, 2006.Revision accepted March 7, 2007.Reprint requests: Rima McLeod, MD, The University of Chicago, AMBH S208,
5841 S. Maryland Ave., Chicago, IL 60637 (e-mail: [email protected]).Copyright © 2007 by the American Association for Pediatric Ophthalmology and
Strabismus.
1091-8531/2007/$35.00 � 0doi:10.1016/j.jaapos.2007.03.017Journal of AAPOS
Materials and Methods
Patient Treatments and EvaluationsThis work was performed with Institutional Review Boardapproval granted from the University of Chicago. Informedconsent was obtained for all participants in accordance withHealth Insurance Portability and Accountability Act of 1996guidelines.
One hundred seventy-three children with congenital toxo-plasmosis were diagnosed serologically and referred to ourstudy as previously described.1 One hundred twenty-four chil-dren were treated at diagnosis with 100 mg/kg of sulfadiazine (EliLilly and Company, Indianalopis, IN; Eon Labs, Laurelton, NY)taken daily in two divided doses for 12 months, and 1 mg/kg ofpyrimethamine (Burroughs Wellcome, Research Triangle Park,NC; GlaxoSmithKline, Philadelphia, PA) taken once daily foreither 2 months (Treatment 1) or 6 months (Treatment 2). BothTreatments 1 and 2 were followed by the same dosage ofleucovorin (Lederle Pharmaceuticals, Madison, NJ; BedfordLaboratories, Bedford, OH) (folinic acid) as described and py-rimethamine was administered on Mondays, Wednesdays, andFridays for the remainder of a year.1 The children’s physiciansmanaged treatment with the consultation of the study’s principalinvestigators. Ten children received treatment different than thepreviously described recommendation,1 with varying regimensincluding one or all of spiramycin, pyrimethamine, sulfonamides,and folinic acid. Thirty-nine children, referred to as “historical
patients,” were not diagnosed with congenital toxoplasmosis un-551

Volume 11 Number 6 / December 2007552 Arun et al
til after their first year of life, and therefore, they did not receivetreatment during this time.
To remove economic barriers that might affect the ability offamilies to participate in the study, all patients were providedcomplimentary accommodations and travel for 1-day evaluationsin Chicago. The children participating in these comprehensiveevaluations were at or as close as possible to the ages of �2.5months, 1, 3.5, 5, 7.5, 10, 15, or 20 years old. The evaluationincluded a review of medical history, general physical examina-tion, ophthalmologic evaluation, psychological and developmen-tal testing, a neurologic examination, audiology testing, and he-matologic laboratory testing (ie, complete blood count includingdifferential, white blood cell, and platelet counts). A brain com-puted tomographic scan was obtained in the newborn period.
Ophthalmologic data were collected for each study participantand entered into a database. Twenty study patients who hadcataracts were identified and characteristics of their cataractswere determined including morphology, complexity, associatedconditions, and natural history ( progression).
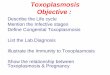
ResultsCharacteristics of Children in This StudyChildren were referred from throughout the United Stateswith predominance from the New York, Chicago, and LosAngeles metropolitan areas. Ophthalmologic manifesta-tions in these children are summarized in Figure 1. Al-though chorioretinal scars were the most frequent finding,20 of 173 patients (11.6%, 95% confidence interval [7.2%,17.3%]) had cataracts.
Identification and Characterization of CataractsTwenty children (27 eyes) had cataracts. Seven were bi-lateral; 13 were unilateral and all occurred in the presenceof other ocular lesions. There were 16 children (21 eyes)with cataracts among the 134 children treated in their firstyear of life and 4 children (6 eyes) with cataracts amongthe 39 children diagnosed after their first year of life. All ofthe 16 children who were treated in the first year of lifeand developed cataracts had severe disease with neurologicsigns at birth. It is unknown whether the four childrendiagnosed after their first year of life, rather than at birth,had severe neurologic disease at birth that might have beenidentified with brain computed tomography scans or de-tailed neurologic examinations.
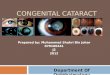
Posterior subcapsular cataracts were noted most often(7); however, nuclear (5), anterior subcapsular (6), andanterior polar cataracts (3) also were observed frequently.The morphology of six cataracts was unknown. Othercharacterization of the cataracts includes complexity, timeof development, and natural history. Thirteen were partial(48.1%), 9 were total (33.3%), and 5 were unknown(18.5%) (Figure 2). Fourteen cataracts (51.9%) were de-tected at birth and 13 (48.1%) were observed postnatally.Twelve were stable (44.4%); 12 were progressive (44.4%),and the natural history was not known for three cataracts
(11.1%).Five of 27 cataractous eyes had surgery (18.5%). One ora combination of the following surgeries was performed:extracapsular cataract extraction, pars plana vitrectomy,pars plana lensectomy, membrane peeling, pupilloplasty,and peripheral iridectomy. Two of 27 eyes with cataractsalso had glaucoma (7.4%) and 16 of 27 eyes with cataractsalso had retinal detachment (59.3%). Two patients hadpersistent fetal vasculature ( persistent hyaloid artery andpersistent hyperplasia of the primary vitreous). One eye of27 (3.7%) was enucleated.
Additional features of the demographics, patient char-acteristics, cataract morphology, and a representative caseare illustrated in the e-Supplement, available at jaapos.org.
DiscussionThe pathogenesis of cataracts in congenital toxoplasmosisis not known. The retina and choroid are generally af-fected first; then iridocyclitis and cataracts can develop, assecondary complications of retinochoroiditis. In sequentialclinical examinations carried out on the eyes of mice thathad been infected in utero with Toxoplasma gondii, threepatterns of clinical disease were seen. These patterns
FIG 1. Summary of ophthalmologic manifestations in 173 patients withcongenital toxoplasmosis. Chorioretinal scars were the most commonfinding with a high incidence of strabismus. CR � chorioretinal.
included crystalliform cataracts, acute uveitis that pro-
Journal of AAPOS

s. C. P
Volume 11 Number 6 / December 2007 Arun et al 553
gressed into a chronic inflammatory disease with sec-ondary opaque cataracts, and multiple discrete foci ofdeep retinal disturbances. Immunocytochemical stainingfor Toxoplasma antigen revealed only intraretinal Toxo-plasma cysts, but no free organisms or extracystic antigenwere demonstrated. Selective photoreceptor destructionwas the most prominent histopathological feature.12 Inone study of a murine model, DNA deposition led tocataract formation.13 It may be that both parasite replica-tion and inflammatory cells arriving via the hyaloid arteryduring lens development cause such DNA deposition inthe lens in congenital toxoplasmosis.
The incidence of cataracts was 11.6% in our NCCCTScohort, most commonly occurring in those with the mostsevere disease. These cataracts affected any part of the lensand they varied in complexity from partial to total. In 11children (16 eyes) in our study, cataracts were associatedwith such severe intraocular pathology (eg, retinal detach-ment) that intervention was not performed. Some of thesepatients eventually had no light perception and phthisis. Itis important to evaluate the retina of children with con-genital toxoplasmosis and cataracts.
The child discussed in Case 1 in the online supplementwas treated for toxoplasmosis prior to, at the time of, andafter his cataract surgery. It is important to administerantiparasitic medication during surgery because reactiva-tions of chorioretinitis have accompanied surgery for cat-aracts in patients with congenital toxoplasmosis.14
Intraocular pressure measurements may be overlookedwhen treating young children with active disease. Westfalland colleagues15 suggested that as many as 38% of olderchildren and adults who have active lesions consistent withtoxoplasmic chorioretinitis have elevated intraocular pres-sure. We have cared for a patient with eye pain duringactive toxoplasmic chorioretinitis in whom intraocularpressure was elevated (unpublished observation, February24, 2006).
In conclusion, patients with congenital toxoplasmosisare at high risk for cataracts and other intraocular pathol-ogy and may benefit from cataract removal.
AcknowledgmentsThis work was supported by Research to Prevent Blindness and the
FIG 2. A. Total cataract. B. A cataract that clinically was of unknown typrevealed an anterior subcapsular plaque and marked cataractous change
National Institutes of Health RO1 AI27530. The Hyatt Hotel Foun-
Journal of AAPOS
dation provided complimentary lodging. The authors thank the familiesand physicians who permitted us to follow these children together withthem. We also want to gratefully acknowledge the following airlines forproviding complimentary transportation during patient trips to Chi-cago: United Airline’s Friendly Skies Program, Braniff InternationalAirways, American Airlines, Air Canada, Angel Flight America, andSouthwest Airlines.
Other members of the Toxoplasmosis Study Group include BarbaraDanis, Mark Stein, Linda Pfiffner, Jeanne Perkins, Sanford Meyers,Michael Kipp, Balaji Gupta, Ahmed Abdelsalam, Huiyuan Zhang,John Marcinak, Saeid Mojatahedi, Dianna Bardo, MarishaHumphries, Douglas Mack, Michael J. Kirisits, Diana Chamot,Ernest Mui, Ronald Thisted, and Adrian Esquivel (University ofChicago); Lazlo Stein (Northwestern University, Chicago; deceased);Andrew Suth (Argosy University, Chicago); Audrey Cameron (MountSinai Hospital, Chicago); Marie Weissbourd (Northwestern UniversityHospital, Chicago); James McAuley (Rush University Medical Center,Chicago); Joyce Hopkins (Illinois Institute of Technology, Chicago);Dushyant Patel (Michael Reese Medical Center, Chicago); and DaveMcLone (Children’s Memorial Hospital, Chicago).
References
1. McLeod R, Boyer K, Karrison T, Kasza K, Swisher C, Roizen N,et al. Outcome of treatment for congenital toxoplasmosis, 1981-2004: The National Collaborative Chicago-Based, Congenital Tox-oplasmosis Study. Clin Infect Dis 2006;42:1383-94.
2. McAuley J, Boyer K, Patel D, Mets M, Swisher C, Roizen N, et al.Early and longitudinal evaluations of treated infants and childrenand untreated historical patients with congenital toxoplasmosis.The Chicago Collaborative Treatment Trial. Clin Infect Dis 1994;18:38-72.
3. Roizen N, Kasza K, Karrison T, Mets M, Noble AG, Boyer K, et al.Impact of visual impairment on measures of cognitive function forchildren with congenital toxoplasmosis. Pediatrics 2006;118:e379-90. Epub 2006 Jul 24.
4. Eichenwald HF. A study of congenital toxoplasmosis, with particularemphasis on clinical manifestations, sequelae, and therapy. In: Siim JC,editor. Human Toxoplasmosis. Copenhagen, Demark: Munksgaard;1960. p. 41-9.
5. Wilson CB, Remington JS, Stagno S, Reynolds DW. Developmentof adverse sequelae in children born with subclinical congenitalToxoplasma infection. Pediatrics 1980;66:767-74.
6. Koppe JG, Loewer-Sieger DH, DeRoever-Bonnet H. Results of20-year follow-up of congenital toxoplasmosis. Lancet 1986;1:254-6.
7. Saxon SA, Knight W, Reynolds DW, Stagno S, Alford CA. Intellec-tual deficits in children born with subclinical congenital toxoplasmo-
e time of the examination. Later the eye was enucleated and pathologyartial cataract (anterior polar).
e at th
sis: A preliminary report. J Pediatr 1973;82:792.

Volume 11 Number 6 / December 2007554 Arun et al
8. Mets M, Holfels E, Boyer KM, Swisher C, Roizen N, Stein L, et al.Eye manifestations of congenital toxoplasmosis. Am J Ophthalmol1996;122:309-24.
9. Roizen N, Swisher C, Stein M, Hopkins J, Boyer KM, Holfels E, et al.Neurologic and developmental outcome in treated congenital toxoplas-mosis. Pediatrics 1995;95:11-20.
10. Brezin AP, Thulliez P, Couvreur J, Nobre R, McLeod R. Ophthal-mic outcomes after prenatal and postnatal treatment of congenitaltoxoplasmosis. Am J Ophthalmol 2003;135:779-84.
11. Vutova K, Peicheva Z, Popova A, Markova V, Mincheva N, TodorovT. Congenital toxoplasmosis: Eye manifestations in infants and chil-
dren. Ann Trop Paediatr 2002;22:213-8.12. Dutton GN. Graefes Clinicopathological features of a congenitalmurine model of ocular toxoplasmosis. Arch Clin Exp Ophthal1986;224:256-64.
13. Nishimoto S, Kawane K, Watanabe-Fukunaga R, Fukuyama H,Ohsawa Y, Uchiyama Y, et al. Nuclear cataract caused by a lack ofDNA degradation in the mouse eye lens. Nature 2003;424:1071-4.
14. Bosch-Driessen LH, Plaisier MB, Stilma JS, Van der Lelij A,Rothova A. Reactivations of ocular toxoplasmosis after cataract ex-traction. Ophthalmology 2002;109:41-5.
15. Westfall AC, Lauer AK, Suhler EB, Rosenbaum JT. Toxoplasmosisretinochoroiditis and elevated intraocular pressure: A retrospective
study. J Glaucoma 2005;14:3-10.An Eye on the Arts – The Arts on the Eye
“I had friends, once,” Mercy went on, “who had a daughter. Beautiful, beautifulchild—but all you had to do was take one look at her to see there was something wrong.She had one crossed eye . . .”
“What is cross-eye?”“Where the eyes don’t focus together. Her left eye was locked in place, staring only to
the right . . .”“Like in movies. They do it so you can laugh.”“Well—I guess so—yes. But this was serious. I wasn’t the only one who noticed it. The
parents knew, but they kept saying it would fix itself. She was very young, this child—notyet two years old. But nothing was done. They did nothing. Nothing. And such a beautifulchild. By the time she was eighteen, the eye was so badly damaged it had to be removed.
“God’s will.”“No dammit!” Mercy flared. “Not God’s will. Parental stupidity. Pride. That’s what it
amounted to. They couldn’t admit their perfect daughter had a defect—but if they hadtaken her to a specialist before she was three or four years old, the eye could have beencorrected and today she would be whole.”
—Timothy Findley (from Spadework, Harper Collins, 2001)
Journal of AAPOS