Embed Size (px)
Citation preview
Cardiac Electrophysiology Review 2002;6:93–95©C 2002 Kluwer Academic Publishers. Manufactured in The Netherlands.
Catecholaminergic Polymorphic VentricularTachyarrhythmias in Children
Philippe CoumelHopital Lariboisiere, Paris, France
For the electrophysiologist ventricular fibrilla-tions consist in their typical forms in a truly desyn-chronized, non self-limited ventricular electricalactivity. In fact, so strictly defined ventricular fib-rillation do exist, but the term should be extendedto polymorphic ventricular tachyarrhythmias thatcan be self-limited til they actually deteriorate intotrue ventricular fibrillation. Such tachyarrhyth-mias may occur in the absence of an identifiedstructural heart disease, but this is not sufficientto consider that idiopathic ventricular fibrillationforms a single entity. It simply means that no heartdisease has been detected by the various investi-gations, due to the paucity of the revealing signsand/or the limitations of our tools. Just to quotetwo examples of such a situation, it suffices tomention that prolongation of the ventricular re-polarization no longer permits to eliminate a longQT syndrome, and that limited, purely anatomi-cal forms of right ventricular dysplasia may not bedetectable in the absence of pathological examina-tion. Just considering idiopathic ventricular fibril-lation from the ECG viewpoint, we can distinguishat least three aspects which form different entitiesthat may or may not be related to either long QTsyndrome and Right Ventricular Dysplasia. Theyare the Brugada syndrome [1], the short-coupledtorsade de pointes [2] and the catecholaminergicventricular tachyarrhythmias [3]. Several reasonsmake the latter entity extremely important to rec-ognize. Not only it can be responsible for suddendeath of children and adolescents, but at variancefrom the two other syndromes that require the im-plantation of a defibrillator, patients are amenableto beta-blocking treatment.
Idiopathic catecholaminergic ventricular tach-yarrhythmias provokes syncope and sudden deathin children or adolescents. Some 50 cases of thissyndrome have been published, and since our ini-tial experience we verified the long-term efficacyof beta-blockers in some 20 cases [3]. In this syn-drome the arrhythmia is easy to document (Fig-ure 1) but unfortunately the diagnosis is oftenmissed by non-cardiologists who may not be awareof the syndrome and may be misled by the appear-ance of a normal heart. The revealing symptomsare spells of dizziness or even syncope in other-wise well-being children. Depending on the sever-ity of the disease, the first symptoms exceptionally
occur before the age of 3. Usually they appearbetween 5 and 10, even later in mild forms. For theclinician, the most important diagnostic criterionis that symptoms occur at exercise or emotion, aninformation that looks easy to collect but is in factfrequently missed, particularly in young children.In the absence of this notion the diagnostic isignored because the heart is apparently normalwhen observed in resting conditions or even nor-mal activity. This is the reason why syncope arefrequently attributed to formes frustes of epilepsyand the tachyarrhythmias may be missed foryears, thus leaving the patients at risk of suddendeath which often intervenes around the age of 15.Not exceptionally in our experience, the cardiolo-gist is consulted on the occasion of symptoms inthe context of sudden death of a brother or a sisterhaving experienced the same troubles in his/herhistory. In fact the diagnosis is quite easy thanksto an exercise test or a Holter recording.
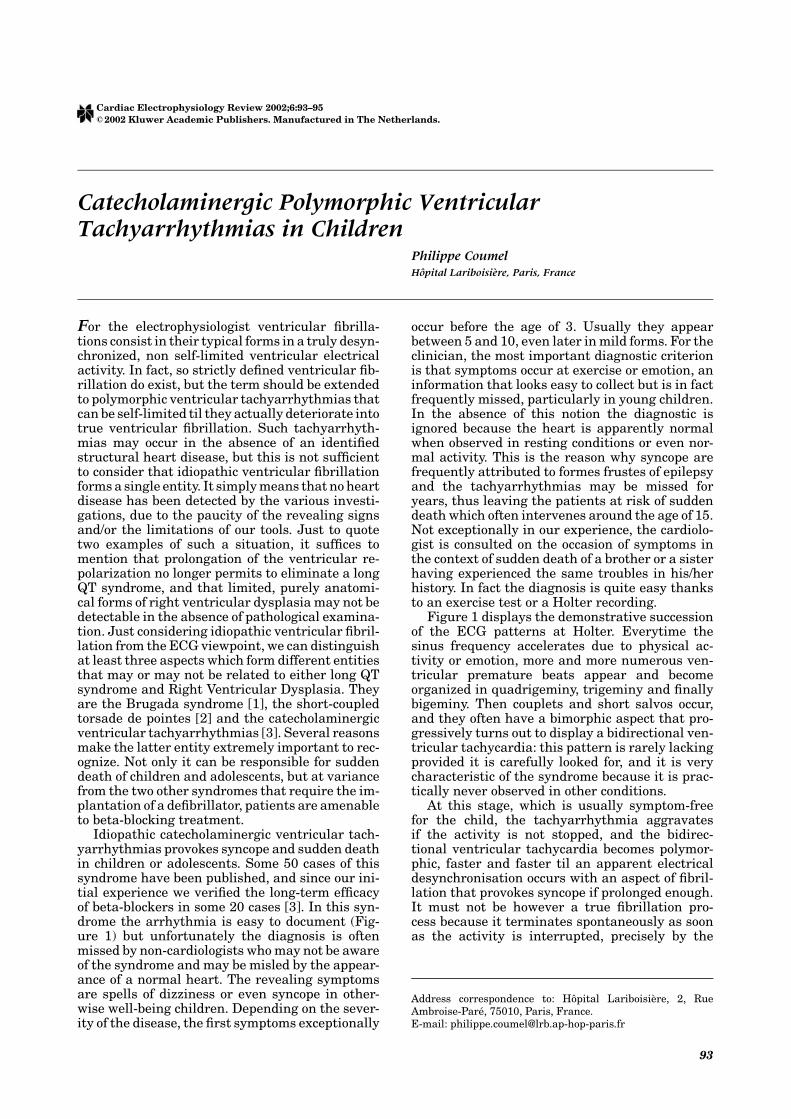
Figure 1 displays the demonstrative successionof the ECG patterns at Holter. Everytime thesinus frequency accelerates due to physical ac-tivity or emotion, more and more numerous ven-tricular premature beats appear and becomeorganized in quadrigeminy, trigeminy and finallybigeminy. Then couplets and short salvos occur,and they often have a bimorphic aspect that pro-gressively turns out to display a bidirectional ven-tricular tachycardia: this pattern is rarely lackingprovided it is carefully looked for, and it is verycharacteristic of the syndrome because it is prac-tically never observed in other conditions.
At this stage, which is usually symptom-freefor the child, the tachyarrhythmia aggravatesif the activity is not stopped, and the bidirec-tional ventricular tachycardia becomes polymor-phic, faster and faster til an apparent electricaldesynchronisation occurs with an aspect of fibril-lation that provokes syncope if prolonged enough.It must not be however a true fibrillation pro-cess because it terminates spontaneously as soonas the activity is interrupted, precisely by the
Address correspondence to: Hopital Lariboisiere, 2, RueAmbroise-Pare, 75010, Paris, France.E-mail: [email protected]
93
94 Coumel CEPR 2002; Vol. 6, No. 1/2
Fig. 1. Catecholaminergic polymorphic ventriculartachycardia in a child. A time-limited exercise isperformed during the Holter recording, and all theaspects characteristic of the syndrome are easilyevidenced in the young patient with a history of effort-and emotion induced syncope: premature beats appearas soon as the sinus rhythm accelerates to 105/min andprogressively form bigeminy, then polymorphicdoublets, then a bidirectional ventricular tachycardiaand an extremely rapid and irregular ventriculartachyarrhythmia that does not degenerate intoventricular fibrillation because the exercise wasimmediately stopped. It is important to observe thatwith the end of exercise all arrhythmias progressivelydisappear in the reverse order. They terminate when thelevel of adrenergic stimulation, as assessed from thesinus rate, is back to its initial value of about 100/min.
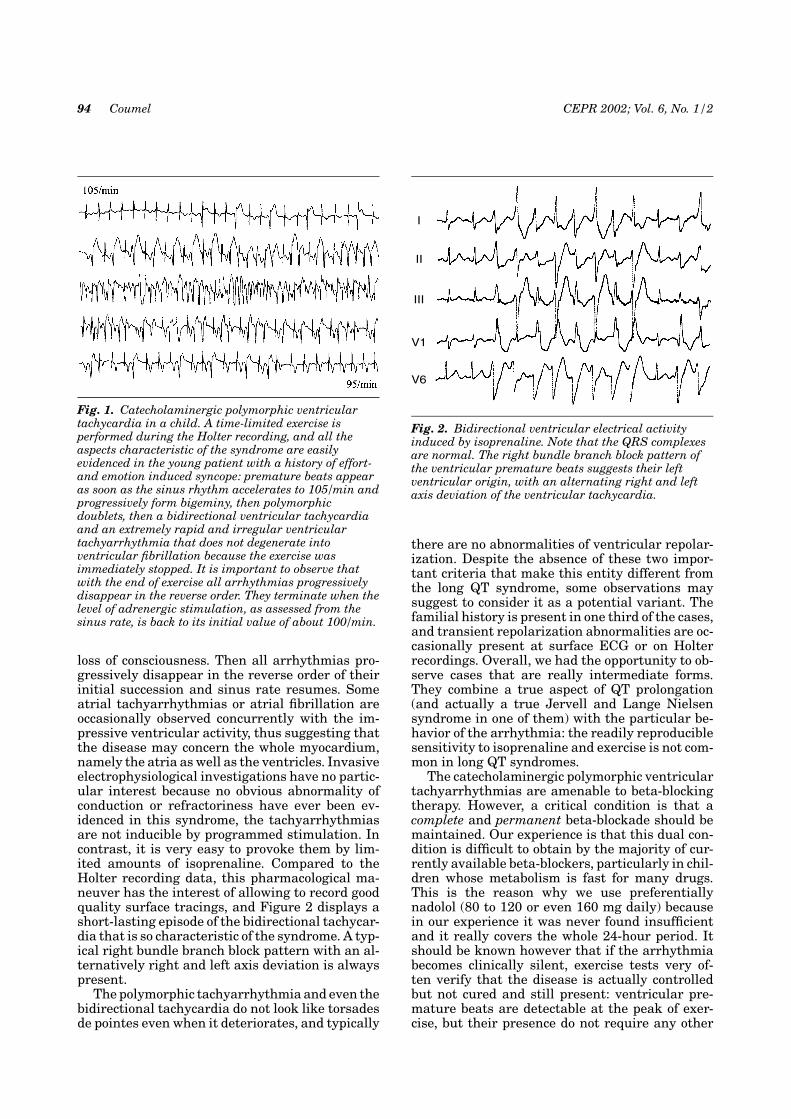
loss of consciousness. Then all arrhythmias pro-gressively disappear in the reverse order of theirinitial succession and sinus rate resumes. Someatrial tachyarrhythmias or atrial fibrillation areoccasionally observed concurrently with the im-pressive ventricular activity, thus suggesting thatthe disease may concern the whole myocardium,namely the atria as well as the ventricles. Invasiveelectrophysiological investigations have no partic-ular interest because no obvious abnormality ofconduction or refractoriness have ever been ev-idenced in this syndrome, the tachyarrhythmiasare not inducible by programmed stimulation. Incontrast, it is very easy to provoke them by lim-ited amounts of isoprenaline. Compared to theHolter recording data, this pharmacological ma-neuver has the interest of allowing to record goodquality surface tracings, and Figure 2 displays ashort-lasting episode of the bidirectional tachycar-dia that is so characteristic of the syndrome. A typ-ical right bundle branch block pattern with an al-ternatively right and left axis deviation is alwayspresent.
The polymorphic tachyarrhythmia and even thebidirectional tachycardia do not look like torsadesde pointes even when it deteriorates, and typically
I
II
III
V1
V6
Fig. 2. Bidirectional ventricular electrical activityinduced by isoprenaline. Note that the QRS complexesare normal. The right bundle branch block pattern ofthe ventricular premature beats suggests their leftventricular origin, with an alternating right and leftaxis deviation of the ventricular tachycardia.
there are no abnormalities of ventricular repolar-ization. Despite the absence of these two impor-tant criteria that make this entity different fromthe long QT syndrome, some observations maysuggest to consider it as a potential variant. Thefamilial history is present in one third of the cases,and transient repolarization abnormalities are oc-casionally present at surface ECG or on Holterrecordings. Overall, we had the opportunity to ob-serve cases that are really intermediate forms.They combine a true aspect of QT prolongation(and actually a true Jervell and Lange Nielsensyndrome in one of them) with the particular be-havior of the arrhythmia: the readily reproduciblesensitivity to isoprenaline and exercise is not com-mon in long QT syndromes.
The catecholaminergic polymorphic ventriculartachyarrhythmias are amenable to beta-blockingtherapy. However, a critical condition is that acomplete and permanent beta-blockade should bemaintained. Our experience is that this dual con-dition is difficult to obtain by the majority of cur-rently available beta-blockers, particularly in chil-dren whose metabolism is fast for many drugs.This is the reason why we use preferentiallynadolol (80 to 120 or even 160 mg daily) becausein our experience it was never found insufficientand it really covers the whole 24-hour period. Itshould be known however that if the arrhythmiabecomes clinically silent, exercise tests very of-ten verify that the disease is actually controlledbut not cured and still present: ventricular pre-mature beats are detectable at the peak of exer-cise, but their presence do not require any other

CEPR 2002; Vol. 6, No. 1/2 Catecholaminergic Polymorphic Ventricular Tachyarrhythmias 95
therapeutic approach. This particularly refers todrug combinations (type I drugs or even amio-darone) that in our experience are useless or evendangerous.
We never had to propose the implantation ofa defibrillator in any of these patients, an optionwhich is very difficult to take in children. Onthe other hand rejecting this indication may bedangerous because it supposes that one is confi-dent in the protection offered by pharmacologicaltreatment. This is why we find crucial to formallyinform the young patient as soon as possible in hislife, and in any case from the beginning his family,that any treatment discontinuation, even limitedto a single day, implies a definite risk of poten-tially severe accident including sudden death.Finally, after a more than 15-year follow-up ofmany patients, we never saw on the long termthe development of any structural heart disease,including cardiomyopathy and right ventriculardysplasia.
The absence of a substrate that could be ex-plored by provocative maneuvers is an importantcharacteristic of primary tachyarrhythmias with-out heart disease. This is in contrast with what isknown in patients with well identified anatomicalsubstrates like a prior myocardial infarction, car-diomyopathy, or right ventricular dysplasia in itsusual form. One can conceive that a reentrant sub-strate, surrounded by relatively healthy or at leasthomogeneous myocardial tissue can be activatedso that an organized tachyarrhythmia can be re-produced. The lack of inducibility, and the poly-morphic electrical activity predominantly suggest-ing a left ventricular origin present in the abovedescribed syndrome suggests that the whole my-ocardium is involved in the electrical disease, butthat the initial trigger is not amenable to ourconventional approaches. Otherwise, no abnormallevel of circulating catecholamines has ever beenfound in those children.
Recently, catecholergic ventricular tachycardiahas been found to be related to mutations onthe ryanodine receptor gene hRyR2 located in
I-q42-q43, that codes for a calcium channel [4].Occasionally, this fits very well with the patternof bidirectional ventricular tachycardia known inthe context of digitalis intoxication in diseasedhearts. The syndrome must be heterogeneous be-cause in our own cases no mutation was found inthis gene. That this entity would form a variantof right ventricular dysplasia is much improba-ble not only because we never observed the de-velopment of this disease on the long term but be-cause the tachyarrhythmia clearly originates fromthe left ventricle (Figure 2) and its behavior is fardifferent.
In conclusion, it is extremely important to rec-ognize this rare but dangerous form of idiopathicventricular tachyarrhythmia, and to suspect iteverytime a child experiences loss of consciousnesswithout any obvious reason, particularly of neuro-logic origin. The consequence of the diagnostic lag-time, that in our experience may last up to severalyears, is potentially sudden death, a catastrophicoutcome for a medically curable entity.
References
1. Brugada P, Brugada J. Right bundle branch block,persistent ST segment elevation and sudden car-diac death: A distinct clinical and electrocardio-graphic syndrome. A multicenter report. J Am CollCardiol 1992;20:1391–1396.
2. Leenhardt A, Glaser E, Burguera M, et al. Short-coupled variant of Torsades de Pointes; a new elec-trocardiographic entity in the spectrum of idio-pathic ventricular tachyarrhythmias? Circulation1994;89:206–215.
3. Leenhardt A, Lucet V, Denjoy I, et al. Cate-cholaminergic polymorphic ventricular tachycardiain children: A 7-year follow-up of 21 patients. Cir-culation 1995;91:1512–1519.
4. Priori SG, Napolitano C, Tiso N, Memmi M,Vignati G, Bloise F, Sorrentino V, Danieli GA.Mutations in the cardiac ryanodine receptorgene (hRyR2) underlie catecholaminergic polymor-phic ventricular tachycardia. Circulation 2001;103:196–202.


![Catecholaminergic polymorphic ventricular tachycardia ... · ECG findings during exercise or emotional stress.[1,5] In this article, we report a case of CPVT detected by an ILR in](https://img.pdfslide.net/doc/110x75/5f02db0d7e708231d40658dd/catecholaminergic-polymorphic-ventricular-tachycardia-ecg-findings-during-exercise.jpg)