Embed Size (px)
Citation preview

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 1/14
Cauda Equina and Conus Medullaris Syndromes
Author: Segun T Dawodu, MD, JD, MBA, LLM, FAAPMR, FAANEM; Chief Editor: Nicholas Lorenzo, MD,CPE more...
Updated: Mar 6, 2013
Background
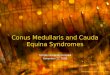
The spinal cord tapers and ends at the level between the first and second lumbar vertebrae in an average adult.The most distal bulbous part of the spinal cord is called the conus medullaris, and its tapering end continues asthe filum terminale. Distal to this end of the spinal cord is a collection of nerve roots, which are horsetail-like inappearance and hence called the cauda equina (Latin for horse's tail). (See the image of cauda equina anatomybelow.)
Illustration demonstrating the relevant anatomy of the cauda equina region
These nerve roots constitute the anatomic connection between the central nervous system (CNS) and theperipheral nervous system (PNS). They are arranged anatomically according to the spinal segments from whichthey originated and are within the cerebrospinal fluid (CSF) in the subarachnoid space with the dural sac ending atthe level of second sacral vertebra.
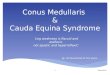
Cauda equina syndrome refers to a characteristic pattern of neuromuscular and urogenital symptoms resultingfrom the simultaneous compression of multiple lumbosacral nerve roots below the level of the conus medullaris(see the image below). These symptoms include low back pain, sciatica (unilateral or, usually, bilateral), saddlesensory disturbances, bladder and bowel dysfunction, and variable lower extremity motor and sensory loss (seeClinical).
Medscape ReferenceReference
NewsReferenceEducationMEDLINE

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 2/14
Although the lesion is technically involves nerve roots and represents a "peripheral" nerve injury, damage may be
irreversible and cauda equina syndrome may be a surgical emergency (see Treatment).[1]
Illustration demonstrating an example of cauda equina syndrome secondary to a spinal neoplasm
Lesions involving the termination of the spinal cord (conus medullaris) are not discussed in this article. Please seethe article Spinal Cord Injuries.
Anatomy
The spinal cord, which is the downward continuation of medulla that starts just below the foramen magnum, servesas a conduit for the ascending and descending fiber tracts that connect the peripheral and spinal nerves to thebrain. The cord projects 31 pairs of spinal nerves on either side (8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1coccygeal) that are connected to the peripheral nerves.
A cross-section of the spinal cord reveals butterfly-shaped gray matter in the middle, surrounded by white matter.As in the cerebrum, the gray matter is composed of cell bodies. The white matter consists of various ascendingand descending tracts of myelinated axon fibers, each with specific functions.
During development, the vertebral column grows more rapidly than the spinal cord. Spinal nerves exit the vertebralcolumn at progressively more oblique angles because of the increasing distance between the spinal cordsegments and the corresponding vertebrae. Lumbar and sacral nerves travel nearly vertically down the spinal canalto reach their exiting foramen.
The spinal cord ends at the intervertebral disc between the first and second lumbar vertebrae as a taperedstructure called the conus medullaris, consisting of sacral spinal cord segments. The upper border of the conusmedullaris is often not well defined. The fibrous extension of the cord, the filum terminale, is a nonneural elementthat extends down to the coccyx.
The cauda equina (CE) is a bundle of intradural nerve roots at the end of the spinal cord, in the subarachnoidspace distal to the conus medullaris. Cauda is Latin for tail, and equina is Latin for horse (ie, the "horse's tail").The CE provides sensory innervation to the saddle area, motor innervation to the sphincters, and parasympatheticinnervation to the bladder and lower bowel (ie, from the left splenic flexure to the rectum).
The nerves in the CE region include lower lumbar and all of the sacral nerve roots. The pelvic splanchnic nervescarry preganglionic parasympathetic fibers from S2-S4 to innervate the detrusor muscle of the urinary bladder.Conversely, somatic lower motor neurons from S2-S4 innervate the voluntary muscles of the external analsphincter and the urethral sphincter via the inferior rectal and the perineal branches of the pudendal nerve,respectively.
Hence, the nerve roots in the CE region carry sensations from the lower extremities, perineal dermatomes, andoutgoing motor fibers to the lower extremity myotomes.
The conus medullaris obtains its blood supply primarily from 3 spinal arterial vessels: the anterior medianlongitudinal arterial trunk and 2 posterolateral trunks. Less prominent sources of blood supply include radiculararterial branches from the aorta, lateral sacral arteries, and the fifth lumbar, iliolumbar, and middle sacral arteries.

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 3/14
The latter contribute more to the vascular supply of the cauda equina, although not in a segmental fashion, unlikethe blood supply to the peripheral nerves.
The nerve roots may also be supplied by diffusion from the surrounding CSF. Moreover, a proximal area of thenerve roots may have a zone of relative hypovascularity.
Pathophysiology
In understanding the pathological basis of any disease involving the conus medullaris, keep in mind that thisstructure constitutes part of the spinal cord (the distal part of the cord) and is in proximity to the nerve roots. Thus,injuries to this area often yield a combination of upper motor neuron (UMN) and lower motor neuron (LMN)symptoms and signs in the dermatomes and myotomes of the affected segments. On the other hand, a caudaequina lesion is an LMN lesion because the nerve roots are part of the PNS.
Cauda equina syndrome may result from any lesion that compresses CE nerve roots. These nerve roots areparticularly susceptible to injury, since they have a poorly developed epineurium. A well-developed epineurium, asperipheral nerves have, protects against compressive and tensile stresses.
The microvascular systems of nerve roots have a region of relative hypovascularity in their proximal third. Increasedvascular permeability and subsequent diffusion from the surrounding cerebral spinal fluid supplement the nutritionalsupply. This property of increased permeability may be related to the tendency toward edema formation of thenerve roots, which may result in edema compounding initial and sometimes seemingly slight injury.
Several studies in different animal models have assessed the pathophysiology of cauda equina syndrome.[2, 3]
Olmarker et al, using a graded balloon pressure method in a porcine model, reported that the venules in the CEregion begin to compress at a pressure as low as 5 mm Hg and the arterioles begin to occlude as the balloon
pressure surpasses the mean arterial pressure.[4, 5, 6, 2, 7] Despite this, even a pressure as high as 200 mm Hgfailed to completely shut off nutritional supply to the CE.
These studies showed that not only the magnitude but also the length and the speed of obstruction were also
important in damaging the CE region.[8] Similar results were reported in other studies. Takahashi et al reported areduction in blood flow to the intermediate nerve segment when 2 pressure points were applied along the path of
the nerve in the CE.[9]
Others have studied compound action potentials in afferent and efferent segments of nerves in the CE region after
application of balloon compression.[10, 11, 12] These researchers reported that 0-50 mm Hg of pressure did notaffect the action potentials (the threshold for disturbances in action potentials was 50-75 mm Hg), and significantdeficits were observed when pressure rose to 100-200 mm Hg.
Etiology
Cauda equina syndrome is caused by any narrowing of the spinal canal that compresses the nerve roots below the
level of the spinal cord.[13] Numerous causes of cauda equina syndrome have been reported, including discherniation, intradural disc rupture, spinal stenosis secondary to other spinal conditions, traumatic injury, primarytumors such as ependymomas and schwannomas, metastatic tumors, infectious conditions, arteriovenous
malformation or hemorrhage, and iatrogenic injury.[13, 14]
The most common causes of cauda equina and conus medullaris syndromes are the following:
Lumbar stenosis (multilevel)
Spinal trauma including fractures[15]
Herniated nucleus pulposus (cause of 2-6% of cases of cauda equina syndrome)[16, 17, 18]
Neoplasm, including metastases, astrocytoma, neurofibroma, and meningioma; 20% of all spinal tumorsaffect this areaSpinal infection/abscess (eg, tuberculosis, herpes simplex virus, meningitis, meningovascular syphilis,
cytomegalovirus, schistosomiasis)[19]
Idiopathic (eg, spinal anesthesia[20] ): these syndromes may occur as complications of the procedure or of

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 4/14
the anesthetic agent (eg, hyperbaric lidocaine, tetracaine)
Spina bifida and subsequent tethered cord syndrome[21]
Other, rare causes include the following:
Spinal hemorrhage, especially subdural and epidural hemorrhage causing compression within the spinalcanalIntravascular lymphomatosisCongenital anomalies of the spine/filum terminale, including tethered cord syndromeConus medullaris lipomasMultiple sclerosisSpinal arteriovenous malformationsLate-stage ankylosing spondylitisNeurosarcoidosisDeep venous thrombosis of the spinal veins (propagated)
Inferior vena cava thrombosis[22]
A retrospective study of 66 consecutive cases of patients admitted to a neurosurgical unit with suspected cauda
equina syndrome found that almost half had no evidence of structural pathology on MRI.[23] These researcherssuggested that the symptoms have a functional origin in such cases.
Trauma
Traumatic events leading to fracture or subluxation can lead to compression of the cauda equina.[15, 24, 25, 26, 27]
Penetrating trauma can cause damage or compression of the cauda equina. Spinal manipulation resulting in
subluxation has caused cauda equina syndrome.[28] Rare cases of sacral insufficiency fractures have been
reported to cause cauda equina syndrome.[29] Acute and delayed presentations of CES due to hematomas and
posttraumatic arachnoid cysts have also been reported.[30, 31, 32]
Herniated disk
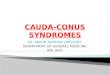
The reported incidence of cauda equina syndrome resulting from herniated lumbar disk (see the image below)
varies from 1-15%.[33, 34, 18] Ninety percent of lumbar disk herniations occur either at L4-L5 or L5-S1.[35, 36]
Sagittal MRI of a patient w ith cauda equina syndrome secondary to a large lumbar disk herniation
Of cases of herniated disks leading to cauda equina syndrome, 70% occur in patients with a history of chronic low
back pain; in 30%, cauda equina syndrome is the first symptom of lumbar disk herniation.[17] Men in the fourth
and fifth decades of life are most prone to cauda equina syndrome secondary to disk herniation.[37]
Most cases of cauda equina syndrome secondary to disk herniation involve either a large central disc or an
extruded disc fragment that compromises a significant amount of the spinal canal diameter.[38] The presentation
may be acute or that of a more protracted course, with the latter bearing a better prognosis.[34] Individuals withcongenital stenosis who sustain a disk herniation are more likely to develop cauda equina syndrome because even

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 5/14
a small herniation can drastically limit the space available for the nerve roots.
Rare cases of intradural disk herniations have been reported to cause cauda equina syndrome.[39] Myelography inthese instances typically demonstrates a complete block of the contrast material. If an intradural disc fragment isidentified, transdural removal of the extruded disc fragment may be helpful to prevent further stretching of thealready compromised nerve root.
Spinal stenosis
Narrowing of the spinal canal can be due to a developmental abnormality or degenerative process. Althoughunusual, cauda equina syndrome from spinal stenosis secondary to spinal disorders such as ankylosing
spondylitis, spondylosis, and spondylolisthesis have all been reported.[40, 41, 42, 43, 44, 45, 46]
Neoplasms
Cauda equina syndrome can be caused by primary or metastatic spinal neoplasms. Among the primary tumorsable to cause CES include myxopapillary ependymoma, schwannoma, and paraganglioma.
Myxopapillary ependymoma is the most common tumor of the filum. Recovery of the function after surgery
depends on the duration of symptoms and the presence or absence of sphincter dysfunction[47] Paraganglioma of
the filum, when present, needs to be differentiated from other tumors of this region.[48] Although rare, this entitymay present as CES.
Schwannomas are benign encapsulated neoplasms that are structurally identical to a syncytium of Schwann
cells.[49] These growths may arise from peripheral or sympathetic nerves. Schwannomas, whether solitary or as apart of a syndrome, may cause CES if present at the level of the conus or filum terminale. Primary tumors thataffect the sacrum, such as chordoma and giant cell tumor of the bone, may produce similar symptoms as a result
of bony destruction and collapse.[50]
Ependymomas are gliomas derived from relatively undifferentiated ependymal cells. They often originate from thecentral canal of the spinal cord and tend to be arranged radially around blood vessels. Ependymomas are foundmost commonly in patients aged approximately 35 years. They can lead to increased intracranial pressure (ICP),and cerebrospinal fluid (CSF) has an increased protein level.
Metastatic lesions of the spine are being reported with increasing frequency because of earlier diagnosis, betterimaging, and more effective treatment modalities. Although metastasis accounts for most tumors in the spine ingeneral, metastatic tumors in the cauda equina are relatively rare compared with primary tumors.
For the spine in general, sources of spinal metastases are as follows[51] :
Lung cancer (40-85%)Breast cancer (11%)Renal cell carcinoma (4%)Lymphatic cancer (3%)Colorectal cancer (3%)
Although lung cancer is the most common source of spine metastases, in one study, only 0.7% of the lungcancer metastases to the spine produced cauda equina syndrome; most of the metastatic lesions were not at the
level of the cauda equina.[51] Up to 8% of patients with prostate cancer experience malignant spinal cord
compression; however, the percentage of cases involving cauda equina syndrome is unknown.[52]
The CE region is also a favored site for drop metastases from intracranial ependymoma, germinoma, and other
tumors.[53] Other unusual metastatic spread from genitourinary and gynecologic cancer have also been reported at
the conus region, causing neurological compromise.[54, 55]
Inflammatory and infectious conditions
Long-lasting inflammatory conditions of the spine, including Paget disease and ankylosing spondylitis, can lead to

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 6/14
cauda equina syndrome secondary to spinal stenosis or fracture.
Infectious conditions, including epidural abscess, can lead to deformity of the nerve roots and spinal cord.[56]
Symptoms generally include severe back pain and a rapidly progressing motor weakness.
Infectious causes for cauda equina syndrome may be pyogenic or nonpyogenic. Pyogenic abscesses aregenerally found in an immunocompromised or poorly nourished host. Staphylococcus aureus causes epiduralabscesses in 25-60% of cases, but, recently, an increasing incidence of infections with methicillin-resistant Saureus, Pseudomonas species, and Escherichia coli have been recorded. A high index of suspicion is helpful in
correct diagnosis and management.[56]
Nonpyogenic causes for abscess are rare and include tuberculosis. Resurgence of tuberculosis secondary toimmunocompromise in individuals with HIV infection requires a high index of suspicion, as the development of
cauda equina syndrome may follow an indolent course.[57] Other uncommon organisms, such as Nocardiaasteroides and Streptococcus milleri, have also been reported as a cause of abscess that leads to the
development of CES.[58, 59]
Iatrogenic causes
Complications of spinal instrumentation have been reported to cause cases of cauda equina syndrome, including
misplaced pedicle screws[60] and laminar hooks.[61, 62] Continuous spinal anesthesia also has been linked to
cases of cauda equina syndrome.[63]
Rare cases of cauda equina syndrome caused by epidural steroid injections, fibrin glue injection,[64] and
placement of a free-fat graft have been reported.[65]
Several cases have involved the use of hyperbaric 5% lidocaine for spinal anesthesia. Recommendations are thathyperbaric lidocaine not be administered in concentrations greater than 2%, with a total dose not to exceed 60
mg.[66, 67]
Medical and surgical situations such as bone screw fixation, fat grafts, lumbar arthrodesis for spondylolisthesis,lumbar discectomy, intradiscal therapy, lumbar puncture forming an epidural hematoma, chiropractic manipulation,and a bolus injection of anesthetic during spinal anesthesia have been related to the development of cauda equina
syndrome–like syndromes.[34, 68, 69, 70, 71, 72]
Epidemiology
Cauda equina and conus medullaris syndromes are classified as clinical syndromes of the spinal cord;epidemiological data on the 2 syndromes are often not available separately from the general data on spinal cordinjury.
Cauda equina syndrome is uncommon, both atraumatically as well as traumatically. It is often reported as a casereport due to its rarity. Although infrequent, it is a diagnosis that must be considered in patients who complain oflow back pain coupled with neurologic complaints, especially urinary symptoms.
Age-related differences in incidence
Traumatic cauda equina syndrome is not age specific. Atraumatic cauda equina syndrome occurs primarily inadults as a result of surgical morbidity, spinal disk disease, metastatic cancer, or epidural abscess.
Prognosis
Morbidity and especially mortality rates are determined by the underlying etiology. Multiple conditions can result incauda equina or conus medullaris syndrome. The prognosis improves if a definitive cause is identified andappropriate treatment occurs early in the course. Surgical decompression may be performed emergently, or, insome patients, delayed, depending on the etiology. Residual weakness, incontinence, impotence, and/or sensory

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 7/14
abnormalities are potential problems if therapy is delayed.
Investigators have attempted to identify specific criteria that can aid in predicting the prognosis of patients withcauda equina syndrome. Patients with bilateral sciatica have been reported to have a less favorable prognosis thanpatients with unilateral pain. Patients with complete perineal anesthesia are more likely to have permanent
paralysis of the bladder.[38]
The extent of perineal or saddle sensory deficit has been reported to be the most important predictor of recovery.[73] Patients with unilateral deficits have a better prognosis than patients with bilateral deficits. Females and
patients with bowel dysfunction have been reported to have worse outcomes postoperatively.[74]
Prognosis can be predicted with the American Spinal Injury Association (ASIA) impairment scale (see PhysicalExamination ), as follows:
ASIA A: 90% of patients remain incapable of functional ambulation (reciprocal gait of 200 feet or more)ASIA B: 72% of patients are unable to attain functional ambulationASIA C/D: 13% are unable to attain functional ambulation 1 year after injury
Ambulatory motor index also is used to predict ambulatory capability. It is calculated by scoring hip flexion, hipabduction, hip extension, knee extension, and knee flexion on both sides, using a 4-point scale (0=absent,1=trace/poor, 2=fair, 3=good or normal); the score is expressed as a percentage of the maximum score of 30.Prognostic significance is as follows:
A patient with a score of 60% or more has a good chance for community ambulation with no more than oneknee-ankle-foot orthosis (KAFO)A patient with a score of 79% or higher may not need an orthosisA patient with a score of 40% or less may require 2 KAFOs for community ambulation
Patient Education
Patient education needs will vary with the type and severity of persistent deficits, and may include the following:
Training in self-catheterization and finger fecal disimpaction, if requiredUse of measures to prevent pressure ulcers, such as skin inspection/care, positioning, turning andtransferring tactics, use of skin protectors, or pressure-reducing support surfacesMaintenance of endurance and strength-training exercisesRegular follow-up by the consulting teams who treated the patient in the hospitalInstructions on how and when medications should be taken and when follow-up laboratory tests should beperformed
For patient education information, see the Erectile Dysfunction Center and Brain and Nervous System Center, aswell as Impotence/Erectile Dysfunction, Erectile Dysfunction FAQs, and Cauda Equina Syndrome.
Contributor Information and DisclosuresAuthorSegun T Dawodu, MD, JD, MBA, LLM, FAAPMR, FAANEM Associate Professor of Rehabilitation Medicineand Interventional Pain Medicine, Albany Medical College
Segun T Dawodu, MD, JD, MBA, LLM, FAAPMR, FAANEM is a member of the following medical societies:American Academy of Physical Medicine and Rehabilitation, American Association of Neuromuscular andElectrodiagnostic Medicine, American College of Sports Medicine, American Medical Association, AmericanMedical Informatics Association, Association of Academic Physiatrists, International Society of Physical andRehabilitation Medicine, and Royal College of Surgeons of England
Disclosure: Nothing to disclose.
Coauthor(s)Kirsten A Bechtel, MD Associate Professor, Department of Pediatrics, Yale University School of Medicine;

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 8/14
Attending Physician, Department of Pediatric Emergency Medicine, Yale-New Haven Children's Hospital
Kirsten A Bechtel, MD is a member of the following medical societies: American Academy of Pediatrics
Disclosure: Nothing to disclose.
Michael S Beeson, MD, MBA, FACEP Professor of Emergency Medicine, Northeastern Ohio UniversitiesCollege of Medicine and Pharmacy; Attending Faculty, Akron General Medical Center
Michael S Beeson, MD, MBA, FACEP is a member of the following medical societies: American College ofEmergency Physicians, Council of Emergency Medicine Residency Directors, National Association of EMSPhysicians, and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Scott D Hodges, DO Consulting Surgeon, Department of Orthopedic Surgery, Center for Sports Medicine andOrthopedics
Scott D Hodges, DO is a member of the following medical societies: American Academy of DisabilityEvaluating Physicians, American Medical Association, American Osteopathic Association, American SpinalInjury Association, North American Spine Society, Southern Medical Association, Southern OrthopaedicAssociation, and Tennessee Medical Association
Disclosure: Medtronic Royalty Consulting; Biomet Spine Royalty Consulting
S Craig Humphreys, MD Orthopedic Spine Surgeon, Department of Orthopedic Surgery, Center for SportsMedicine and Orthopedics
S Craig Humphreys, MD is a member of the following medical societies: Alpha Omega Alpha, AmericanAcademy of Orthopaedic Surgeons, American Medical Association, American Spinal Injury Association, NorthAmerican Spine Society, Southern Medical Association, Southern Orthopaedic Association, and TennesseeMedical Association
Disclosure: Nothing to disclose.
James F Kellam, MD Vice-Chair, Department of Orthopedic Surgery, Director of Orthopedic Trauma andEducation, Carolinas Medical Center
James F Kellam, MD is a member of the following medical societies: American Academy of OrthopaedicSurgeons, Orthopaedic Trauma Association, and Royal College of Physicians and Surgeons of Canada
Disclosure: Nothing to disclose.
Specialty Editor BoardMilind J Kothari, DO Professor, Department of Neurology, Pennsylvania State University College of Medicine;Consulting Staff, Department of Neurology, Penn State Milton S Hershey Medical Center
Milind J Kothari, DO is a member of the following medical societies: American Academy of Neurology,American Association of Neuromuscular and Electrodiagnostic Medicine, and American NeurologicalAssociation
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical CenterCollege of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Medscape Salary Employment
J Stephen Huff, MD Associate Professor of Emergency Medicine and Neurology, Department of Emergency

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 9/14
Medicine, University of Virginia School of Medicine
J Stephen Huff, MD is a member of the following medical societies: American Academy of EmergencyMedicine, American Academy of Neurology, American College of Emergency Physicians, and Society forAcademic Emergency Medicine
Disclosure: Nothing to disclose.
Chief EditorNicholas Lorenzo, MD, CPE Chairman and CEO, Neurology Specialists and Consultants; Senior VicePresident, Founding Executive Director, Continuing Medical Education, Gannett Education (Division GannettHealthcare Group)
Nicholas Lorenzo, MD, CPE is a member of the following medical societies: Alpha Omega Alpha, AmericanAcademy of Neurology, and American College of Physician Executives
Disclosure: Nothing to disclose.
Additional ContributorsThe authors and editors of Medscape Reference gratefully acknowledge the contributions of previous authorJason C Eck, DO, MS,to the development and writing of a source article.
References
1. Mauffrey C, Randhawa K, Lewis C, Brewster M, Dabke H. Cauda equina syndrome: an anatomicallydriven review. Br J Hosp Med (Lond). Jun 2008;69(6):344-7. [Medline].
2. Olmarker K, Rydevik B, Hansson T, Holm S. Compression-induced changes of the nutritional supply tothe porcine cauda equina. J Spinal Disord. Mar 1990;3(1):25-9. [Medline].
3. Delamarter RB, Sherman JE, Carr JB. 1991 Volvo Award in experimental studies. Cauda equinasyndrome: neurologic recovery following immediate, early, or late decompression. Spine (Phila Pa 1976).Sep 1991;16(9):1022-9. [Medline].
4. Olmarker K, Rydevik B, Holm S. Edema formation in spinal nerve roots induced by experimental, gradedcompression. An experimental study on the pig cauda equina with special reference to differences ineffects between rapid and slow onset of compression. Spine (Phila Pa 1976). Jun 1989;14(6):569-73.[Medline].
5. Olmarker K, Rydevik B, Holm S, Bagge U. Effects of experimental graded compression on blood flow inspinal nerve roots. A vital microscopic study on the porcine cauda equina. J Orthop Res. 1989;7(6):817-23. [Medline].
6. Olmarker K, Holm S, Rydevik B. Importance of compression onset rate for the degree of impairment ofimpulse propagation in experimental compression injury of the porcine cauda equina. Spine (Phila Pa1976). May 1990;15(5):416-9. [Medline].
7. Olmarker K, Holm S, Rosenqvist AL, Rydevik B. Experimental nerve root compression. A model of acute,graded compression of the porcine cauda equina and an analysis of neural and vascular anatomy. Spine(Phila Pa 1976). Jan 1991;16(1):61-9. [Medline].
8. Metser U, Lerman H, Blank A, Lievshitz G, Bokstein F, Even-Sapir E. Malignant involvement of the spine:assessment by 18F-FDG PET/CT. J Nucl Med. Feb 2004;45(2):279-84. [Medline].
9. Takahashi K, Olmarker K, Holm S, Porter RW, Rydevik B. Double-level cauda equina compression: anexperimental study with continuous monitoring of intraneural blood flow in the porcine cauda equina. JOrthop Res. Jan 1993;11(1):104-9. [Medline].
10. Rydevik BL, Pedowitz RA, Hargens AR, Swenson MR, Myers RR, Garfin SR. Effects of acute, graded

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 10/14
compression on spinal nerve root function and structure. An experimental study of the pig cauda equina.Spine (Phila Pa 1976). May 1991;16(5):487-93. [Medline].
11. Rydevik B. Neurophysiology of cauda equina compression. Acta Orthop Scand Suppl. 1993;251:52-5.[Medline].
12. Pedowitz RA, Garfin SR, Massie JB, Hargens AR, Swenson MR, Myers RR, et al. Effects of magnitudeand duration of compression on spinal nerve root conduction. Spine (Phila Pa 1976). Feb 1992;17(2):194-9. [Medline].
13. Todd NV. An algorithm for suspected cauda equina syndrome. Ann R Coll Surg Engl. May2009;91(4):358-9; author reply 359-60. [Medline]. [Full Text].
14. Olivero WC, Wang H, Hanigan WC, Henderson JP, Tracy PT, Elwood PW, et al. Cauda equina syndrome(CES) from lumbar disc herniations. J Spinal Disord Tech. May 2009;22(3):202-6. [Medline].
15. Kingwell SP, Curt A, Dvorak MF. Factors affecting neurological outcome in traumatic conus medullarisand cauda equina injuries. Neurosurgical Focus. 2008;25(5):E7. [Medline].
16. Fujisawa H, Igarashi S, Koyama T. Acute cauda equina syndrome secondary to lumbar disc herniationmimicking pure conus medullaris syndrome--case report. Neurol Med Chir (Tokyo). Jul 1998;38(7):429-31.[Medline].
17. Raj D, Coleman N. Cauda equina syndrome secondary to lumbar disc herniation. Acta Orthop Belg. Aug2008;74(4):522-7. [Medline].
18. Gleave JR, MacFarlane R. Prognosis for recovery of bladder function following lumbar central discprolapse. Br J Neurosurg. 1990;4(3):205-9. [Medline].
19. Gellido CL, Onesti S, Llena J. Spinal schistosomiasis. Neurology. Jan 25 2000;54(2):527. [Medline].
20. Waters JH, Watson TB, Ward MG. Conus medullaris injury following both tetracaine and lidocaine spinalanesthesia. J Clin Anesth. Dec 1996;8(8):656-8. [Medline].
21. Kothbauer K, Seiler RW. [Tethered spinal cord syndrome in adults]. Nervenarzt. Apr 1997;68(4):285-91.[Medline].
22. Widge AS, Tomycz ND, Kanter AS. Sacral preservation in cauda equina syndrome from inferior vena cavathrombosis. J Neurosurg Spine. Mar 2009;10(3):257-9. [Medline].
23. Rooney A, Statham PF, Stone J. Cauda equina syndrome with normal MR imaging. J Neurol. May2009;256(5):721-5. [Medline].
24. Harrop JS, Hunt GE Jr, Vaccaro AR. Conus medullaris and cauda equina syndrome as a result oftraumatic injuries: management principles. Neurosurg Focus. Jun 15 2004;16(6):e4. [Medline].
25. Fisher RG. Sacral fracture with compression of cauda equina: surgical treatment. J Trauma. Dec1988;28(12):1678-80. [Medline].
26. Schizas C, Ballesteros C, Roy P. Cauda equina compression after trauma: an unusual presentation ofspinal epidural lipoma. Spine (Phila Pa 1976). Apr 15 2003;28(8):E148-51. [Medline].
27. Thongtrangan I, Le H, Park J, Kim DH. Cauda equina syndrome in patients with low lumbar fractures.Neurosurg Focus. Jun 15 2004;16(6):e6. [Medline].
28. Haldeman S, Rubinstein SM. Cauda equina syndrome in patients undergoing manipulation of the lumbarspine. Spine (Phila Pa 1976). Dec 1992;17(12):1469-73. [Medline].
29. Muthukumar T, Butt SH, Cassar-Pullicino VN, McCall IW. Cauda equina syndrome presentation of sacralinsufficiency fractures. Skeletal Radiol. Apr 2007;36(4):309-13. [Medline].
30. Kebaish KM, Awad JN. Spinal epidural hematoma causing acute cauda equina syndrome. Neurosurg

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 11/14
Focus. Jun 15 2004;16(6):e1. [Medline].
31. Chen HJ, Liang CL, Lu K, Liliang PC, Tsai YD. Cauda equina syndrome caused by delayed traumaticspinal subdural haematoma. Injury. Jul 2001;32(6):505-7. [Medline].
32. Zuccarello M, Powers G, Tobler WD, Sawaya R, Hakim SZ. Chronic posttraumatic lumbar intraduralarachnoid cyst with cauda equina compression: case report. Neurosurgery. Apr 1987;20(4):636-8.[Medline].
33. Raaf J. Removal of protruded lumbar intervertebral discs. J Neurosurg. May 1970;32(5):604-11. [Medline].
34. Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar discherniation. J Bone Joint Surg Am. Mar 1986;68(3):386-91. [Medline].
35. Shapiro S. Cauda equina syndrome secondary to lumbar disc herniation. Neurosurgery. May1993;32(5):743-6; discussion 746-7. [Medline].
36. Shapiro S. Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine (PhilaPa 1976). Feb 1 2000;25(3):348-51; discussion 352. [Medline].
37. Ahn UM, Ahn NU, Buchowski JM, Garrett ES, Sieber AN, Kostuik JP. Cauda equina syndromesecondary to lumbar disc herniation: a meta-analysis of surgical outcomes. Spine (Phila Pa 1976). Jun 152000;25(12):1515-22. [Medline].
38. Scott PJ. Bladder paralysis in cauda equina lesions from disc prolapse. J Bone Joint Surg.1965;47B:224-235.
39. Dinning TA, Schaeffer HR. Discogenic compression of the cauda equina: a surgical emergency. Aust N ZJ Surg. Dec 1993;63(12):927-34. [Medline].
40. Shaw M, Birch N. Facet joint cysts causing cauda equina compression. J Spinal Disord Tech. Oct2004;17(5):442-5. [Medline].
41. Ahn NU, Ahn UM, Nallamshetty L, Springer BD, Buchowski JM, Funches L, et al. Cauda equinasyndrome in ankylosing spondylitis (the CES-AS syndrome): meta-analysis of outcomes after medicaland surgical treatments. J Spinal Disord. Oct 2001;14(5):427-33. [Medline].
42. Tullous MW, Skerhut HE, Story JL, Brown WE Jr, Eidelberg E, Dadsetan MR, et al. Cauda equinasyndrome of long-standing ankylosing spondylitis. Case report and review of the literature. J Neurosurg.Sep 1990;73(3):441-7. [Medline].
43. Devlin GP, Sheppeard H. Cauda equina syndrome in ankylosing spondylitis diagnosed by computedtomography. N Z Med J. Oct 28 1987;100(834):651-2. [Medline].
44. Rubenstein DJ, Ghelman B. Case report 477: Cauda equina syndrome (CES) complicating long-standingankylosing spondylitis (AS). Skeletal Radiol. 1988;17(3):212-5. [Medline].
45. Indrieri RJ. Lumbosacral stenosis and injury of the cauda equina. Vet Clin North Am Small Anim Pract.May 1988;18(3):697-710. [Medline].
46. Baba H, Maezawa Y, Furusawa N, Imura S, Tomita K. The role of calcium deposition in the ligamentumflavum causing a cauda equina syndrome and lumbar radiculopathy. Paraplegia. Apr 1995;33(4):219-23.[Medline].
47. Schweitzer JS, Batzdorf U. Ependymoma of the cauda equina region: diagnosis, treatment, and outcomein 15 patients. Neurosurgery. Feb 1992;30(2):202-7. [Medline].
48. Anderson JR, Gullan RW. Paraganglioma of the cauda equina: a case report. J Neurol NeurosurgPsychiatry. Jan 1987;50(1):100-3. [Medline]. [Full Text].
49. Kagaya H, Abe E, Sato K, Shimada Y, Kimura A. Giant cauda equina schwannoma. A case report. Spine(Phila Pa 1976). Jan 15 2000;25(2):268-72. [Medline].

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 12/14
50. Bagley CA, Gokaslan ZL. Cauda equina syndrome caused by primary and metastatic neoplasms.Neurosurg Focus. Jun 15 2004;16(6):e3. [Medline].
51. Ampil FL, Mills GM, Burton GV. A retrospective study of metastatic lung cancer compression of thecauda equina. Chest. Nov 2001;120(5):1754-5. [Medline].
52. Saad F, Clarke N, Colombel M. Natural history and treatment of bone complications in prostate cancer.Eur Urol. Mar 2006;49(3):429-40. [Medline].
53. Natale M, Spennato P, Savarese L, Bocchetti A, Esposito S, Barbato R. Anaplastic oligodendrogliomapresenting with drop metastases in the cauda equina. Clin Neurol Neurosurg. Aug 2005;107(5):417-20.[Medline].
54. den Boon J, Avezaat CJ, van der Gaast A, Koops W, Huikeshoven FJ. Conus-cauda syndrome as apresenting symptom of endodermal sinus tumor of the ovary. Gynecol Oncol. Apr 1995;57(1):121-5.[Medline].
55. Bourezgui M, Rafai MA, El Moutawakkil B, Boulaajaj FZ, Sibai M, Lezar S, et al. [Cauda equinasyndrome revealing neuroblastoma]. Rev Neurol (Paris). Dec 2008;164(12):1048-51. [Medline].
56. Lenehan B, Sullivan P, Street J, Dudeney S. Epidural abscess causing cauda equina syndrome. Ir J MedSci. Jul-Sep 2005;174(3):88-91. [Medline].
57. Kapoor SK, Garg V, Dhaon BK, Jindal M. Tuberculosis of the posterior vertebral elements: a rare cause ofcompression of the cauda equina. A case report. J Bone Joint Surg Am. Feb 2005;87(2):391-4. [Medline].
58. Faraj A, Krishna M, Mehdian SM. Cauda equina syndrome secondary to lumbar spondylodiscitis causedby Streptococcus milleri. Eur Spine J. 1996;5(2):134-6. [Medline].
59. Brecker SJ, Pugey CD. Nocardia asteroides infection of the cauda equina. J Neurol Neurosurg Psychiatry.Feb 1988;51(2):309-11. [Medline]. [Full Text].
60. Donovan DJ, Polly DW Jr, Ondra SL. The removal of a transdural pedicle screw placed for thoracolumbarspine fracture. Spine (Phila Pa 1976). Nov 1 1996;21(21):2495-8; discussion 2499. [Medline].
61. Rittmeister M, Leyendecker K, Kurth A, Schmitt E. Cauda equina compression due to a laminar hook: Alate complication of posterior instrumentation in scoliosis surgery. Eur Spine J. 1999;8(5):417-20.[Medline].
62. Mineiro J, Weinstein SL. Delayed postoperative paraparesis in scoliosis surgery. A case report. Spine(Phila Pa 1976). Jul 15 1997;22(14):1668-72. [Medline].
63. Ilias WK, Klimscha W, Skrbensky G, Weinstabl R, Widhalm A. Continuous microspinal anaesthesia:another perspective on mechanisms inducing cauda equina syndrome. Anaesthesia. Jul 1998;53(7):618-23. [Medline].
64. Wera GD, Dean CL, Nho S, Ahn UM, Cassinelli EH, Liu RW, et al. Cauda equina syndrome resultingfrom treatment of dural ectasia with fibrin glue injection. J Spinal Disord Tech. Apr 2006;19(2):148-50.[Medline].
65. Imran Y, Halim Y. Acute cauda equina syndrome secondary to free fat graft following spinaldecompression. Singapore Med J. Jan 2005;46(1):25-7. [Medline].
66. Johnson ME. Potential neurotoxicity of spinal anesthesia with lidocaine. Mayo Clin Proc. Sep2000;75(9):921-32. [Medline].
67. Loo CC, Irestedt L. Cauda equina syndrome after spinal anaesthesia with hyperbaric 5% lignocaine: areview of six cases of cauda equina syndrome reported to the Swedish Pharmaceutical Insurance 1993-1997. Acta Anaesthesiol Scand. Apr 1999;43(4):371-9. [Medline].
68. Liu YC, Wu RS, Wong CS. Unexpected complication of attempted epidural anaesthesia: cauda equina

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 13/14
syndrome. Anaesth Intensive Care. Aug 2003;31(4):461-4. [Medline].
69. Pouchot J, Si-Hassen C, Damade R, Bayeux MC, Mathieu A, Vinceneux P. Cauda equina compressionby epidural lipomatosis in obesity. Effectiveness of weight reduction. J Rheumatol. Sep 1995;22(9):1771-5. [Medline].
70. Diaz JH. Permanent paraparesis and cauda equina syndrome after epidural blood patch for postduralpuncture headache. Anesthesiology. Jun 2002;96(6):1515-7. [Medline].
71. Prusick VR, Lint DS, Bruder WJ. Cauda equina syndrome as a complication of free epidural fat-grafting. Areport of two cases and a review of the literature. J Bone Joint Surg Am. Sep 1988;70(8):1256-8.[Medline].
72. Lambert DH. Bupivacaine spinal block cauda equina syndrome: why did it happen?. Anesthesiology. Jun2005;102(6):1285-6; author reply 1287-8. [Medline].
73. Shaw A, Anwar H, Targett J, Lafferty K. Cauda equina syndrome versus saddle embolism. Ann R CollSurg Engl. Sep 2008;90(6):W6-8. [Medline]. [Full Text].
74. O'Laughlin SJ, Kokosinski E. Cauda equina syndrome in a pregnant woman referred to physical therapyfor low back pain. J Orthop Sports Phys Ther. Nov 2008;38(11):721. [Medline].
75. Bell DA, Collie D, Statham PF. Cauda equina syndrome: what is the correlation between clinicalassessment and MRI scanning?. Br J Neurosurg. Apr 2007;21(2):201-3. [Medline].
76. Ma B, Wu H, Jia LS, Yuan W, Shi GD, Shi JG. Cauda equina syndrome: a review of clinical progress.Chin Med J (Engl). May 20 2009;122(10):1214-22. [Medline].
77. Balzer JR, Rose RD, Welch WC, Sclabassi RJ. Simultaneous somatosensory evoked potential andelectromyographic recordings during lumbosacral decompression and instrumentation. Neurosurgery. Jun1998;42(6):1318-24; discussion 1324-5. [Medline].
78. Mathew P, Todd NV. Diagnosis of intradural conus and cauda equina tumours. Br J Hosp Med. Aug 18-311993;50(4):169-70, 172-4. [Medline].
79. Bell DA, Collie D, Statham PF. Cauda equina syndrome: what is the correlation between clinicalassessment and MRI scanning?. Br J Neurosurg. Apr 2007;21(2):201-3. [Medline].
80. Coscia M, Leipzig T, Cooper D. Acute cauda equina syndrome. Diagnostic advantage of MRI. Spine. Feb15 1994;19(4):475-8. [Medline].
81. Mailleux R, Redant C, Milbouw G. MR diagnosis of transdural disc herniation causing cauda equinesyndrome. JBR-BTR. Nov-Dec 2006;89(6):303-5. [Medline].
82. Kikuchi M, Nagao K, Muraosa Y, Ohnuma S, Hoshino H. Cauda equina syndrome complicatingpneumococcal meningitis. Pediatr Neurol. Feb 1999;20(2):152-4. [Medline].
83. Spencer TS, Campellone JV, Maldonado I, et al. Clinical and magnetic resonance imaging manifestationsof neurosarcoidosis. Semin Arthritis Rheum. 2005;34(4):649-661. [Medline].
84. Podnar S. Electromyography of the anal sphincter: which muscle to examine?. Muscle Nerve. Sep2003;28(3):377-9. [Medline].
85. Gleave JR, Macfarlane R. Cauda equina syndrome: what is the relationship between timing of surgery andoutcome?. Br J Neurosurg. Aug 2002;16(4):325-8. [Medline].
86. Hussain SA, Gullan RW, Chitnavis BP. Cauda equina syndrome: outcome and implications formanagement. Br J Neurosurg. Apr 2003;17(2):164-7. [Medline].
87. Institute for Clinical Systems Improvement (ICSI). Adult low back pain. Bloomington (MN): Institute forClinical Systems Improvement (ICSI); Nov 2008:[Full Text].

6/14/13 Cauda Equina and Conus Medullaris Syndromes
emedicine.medscape.com/article/1148690-overview 14/14
Medscape Reference © 2011 WebMD, LLC
88. Michigan Quality Improvement Consortium. Management of acute low back pain. Southfield (MI):Michigan Quality Improvement Consortium; Mar 2008:[Full Text].
89. Bussières AE, Taylor JA, Peterson C. Diagnostic imaging practice guidelines for musculoskeletalcomplaints in adults-an evidence-based approach-part 3: spinal disorders. J Manipulative Physiol Ther.Jan 2008;31(1):33-88. [Medline]. [Full Text].
90. Herschorn S, Gajewski J, Ethans K, Corcos J, Carlson K, Bailly G, et al. Efficacy of botulinum toxin Ainjection for neurogenic detrusor overactivity and urinary incontinence: a randomized, double-blind trial. JUrol. Jun 2011;185(6):2229-35. [Medline].
91. Cruz F, Herschorn S, Aliotta P, Brin M, Thompson C, Lam W, et al. Efficacy and Safety ofOnabotulinumtoxinA in Patients with Urinary Incontinence Due to Neurogenic Detrusor Overactivity: ARandomised, Double-Blind, Placebo-Controlled Trial. Eur Urol. Jul 13 2011;[Medline].
92. Ginsberg D, et al. Phase 3 Efficacy and Safety Study of OnabotulinumtoxinA in Patients With UrinaryIncontinence Due to Neurogenic Detrusor Overactivity. Presented at 107th Annual Meeting of theAmerican Urological Association, Washington, DC. May, 2011.
93. McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-termfunctional and sphincteric outcome. Spine (Phila Pa 1976). Jan 15 2007;32(2):207-16. [Medline].
94. O'Laoire SA, Crockard HA, Thomas DG. Prognosis for sphincter recovery after operation for cauda equinacompression owing to lumbar disc prolapse. Br Med J (Clin Res Ed). Jun 6 1981;282(6279):1852-4.[Medline]. [Full Text].
95. Weninger P, Schultz A, Hertz H. Conservative management of thoracolumbar and lumbar spinecompression and burst fractures: functional and radiographic outcomes in 136 cases treated by closedreduction and casting. Arch Orthop Trauma Surg. Feb 2009;129(2):207-19. [Medline].
96. Sayegh FE, Kapetanos GA, Symeonides PP, Anogiannakis G, Madentzidis M. Functional outcome afterexperimental cauda equina compression. J Bone Joint Surg Br. Jul 1997;79(4):670-4. [Medline].









![Textdefinition Algorithmus - gqhnet.de · S34.0 Kontusion und Ödem des lumbalen Rückenmarkes [Conus medullaris] S34.10 Komplette Querschnittverletzung des lumbalen Rückenmarkes](https://img.pdfslide.net/doc/110x75/5d5b4a5a88c993b5258b5f2d/textdefinition-algorithmus-s340-kontusion-und-oedem-des-lumbalen-rueckenmarkes.jpg)













![Conus-cauda Syndrom Edit.pptx [Autosaved]](https://img.pdfslide.net/doc/110x75/5695d2f21a28ab9b029c487d/conus-cauda-syndrom-editpptx-autosaved.jpg)
