Embed Size (px)
Citation preview

Companion Diagnostics and Cancer Biomarkers
Cell-Free DNA from Ascites and Pleural Effusions:Molecular Insights into Genomic Aberrations andDisease BiologyHatim Husain1, David Nykin1, Nam Bui1, Daniel Quan1, German Gomez1,Brian Woodward1, Sumathi Venkatapathy2, Radha Duttagupta2, Eric Fung2,Scott M. Lippman1, and Razelle Kurzrock1
Abstract
Collection of cell-free DNA (cfDNA) from the blood ofindividuals with cancer has permitted noninvasive tumorgenome analysis. Detection and characterization of cfDNA inascites and pleural effusions have not yet been reported. Here-in, we analyzed cfDNA in the ascites and pleural effusions fromsix individuals with metastatic cancer. In all cases, cfDNA copynumber variations (CNV) were discovered within the effusate.One individual had a relevant alteration with a high copyamplification in EGFR in a never smoker with lung cancer,who showed only MDM2 and CDK4 amplification in a priortissue biopsy. Another subject with metastatic breast cancer had
cytology-positive ascites and an activating PIK3CA mutationidentified in the tissue, blood, and ascites collectively. Thisindividual had tumor regression after the administration of themTOR inhibitor everolimus and had evidence of chromotripsisfrom chromosomal rearrangements noted in the cell-free asciticfluid. These results indicate that cfDNA from ascites and pleuraleffusions may provide additional information not detectedwith tumor and plasma cell-free DNA molecular characteriza-tion, and a context for important insights into tumor biologyand clonal dynamic change within primary tumor and meta-static deposits. Mol Cancer Ther; 16(5); 948–55. �2017 AACR.
IntroductionThe expanding application of targeted treatments for malig-
nancies highlights the importance of monitoring the geneticaberrations of a tumor over time (1). Many treatment paradigmshave relied on the analysis of a single biopsy to provide genomicprofiling of an individual's tumor. Nonetheless, inter-tumoral aswell as intra-tumoral heterogeneity can lead to an incompletegenomic picture when analyzing a sample from a single tissuebiopsy. Smaller subclonal populations of mutations may beundetectable if not present within the specific anatomic locationwithin a biopsied tumor or at distant unbiopsied metastaticsites (2).
It is clear that assays that are able to represent globalmutationalburden across multiple metastatic sites will be a cornerstone ofeffective targeted therapy. Liquid biopsies, specifically the analysisof plasma cell-free DNA (cfDNA), may help overcome the spatialbias of single tissue samples by capturing the global heteroge-neous tumor genomeof both primary andmetastatic lesions froma single fluid sample (3–5). In this investigation, we consider thepotential of analyzing the genetic alterations present in the cfDNA
of ascites or pleural effusion samples from individuals withmetastatic cancer across histologies.
The advantages of monitoring ctDNA from ascites or pleuraleffusions includes the fact that abundant DNA can be obtainedthrough (i) minimally invasive procedures, (ii) are collected forclinically therapeutic and diagnostic purposes, (iii) can be col-lected from advanced stage malignancy, (iv) can have larger DNAquantities for analyses compared with plasma, (v) can be collect-ed serially to understand clonal dynamic change within the cells,and (vi) can be paired with viable cells for patient-derivedxenograft (PDX) analyses. The detection of relevant mutationswill be presented in the context of a larger cohort of individualswho had fluid removed during therapeutic paracenteses andthoracenteses.
Materials and MethodsIdentification of Cases
Samples were collected from eleven subjects receiving thera-peutic removal of ascites or pleural effusions and prepared foranalysis. Of these, samples from seven individuals passed qualitycontrol (QC) thresholds of the median of the absolute values ofall pairwise differences (MAPD;�0.3) and SNP quality control ofnormal diploid markers (ndSNPQC;�26). Four of these subjectshad genomic data fromprevious analysis of solid tumor tissue. Allindividuals gave informed consent in accordance with the Uni-versity of California San Diego Internal Review Board guidelinesand consented for review of medical records.
Isolation of cfDNA from ascites and pleural effusionsOf the seven subjectswhose effusate samples passedQC thresh-
olds, six individuals had metastatic solid tumor including of the
1Division of Hematology and Oncology, University of California San Diego, SanDiego, California. 2ThermoFisher Scientific, Inc, Santa Clara, California.
Corresponding Author: Hatim Husain, UC San Diego Moores Cancer Center,3855 Health Sciences Dr Rm 3011, La Jolla CA 92093. Phone: 858-534-1590; Fax:858-822-6186; E-mail: [email protected]
doi: 10.1158/1535-7163.MCT-16-0436
�2017 American Association for Cancer Research.
MolecularCancerTherapeutics
Mol Cancer Ther; 16(5) May 2017948
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

lung cancer, breast cancer, pancreas cancer, colon cancer, rectalcancer, and renal cell carcinoma. One human sample from anindividual who had cirrhosis served as a negative control. Onesubject who had colon cancer was cytology negative within thepleural effusion and likely had the effusion from a cause otherthan malignancy.
Samples were centrifuged at 1,500 rpm for 5 minutes andapproximately 30 mL of the clear supernatant aspirated andfrozen at �80�C. cfDNA was isolated using commercially avail-able DNA purification kits (Plasma/Serum Circulating DNA Puri-fication Maxi Kit, Norgen Bioteck Corp) and quantified using theNanoDrop 2000 UV-Vis Spectrophotometer (Thermo Scientific)and PicoGreen dsDNA quantitation kit (Life Technologies) fol-lowing the manufacturer's protocols.
Hybridization and data analysisGenomic microarray hybridization was performed using the
OncoScan FFPE Assay Kit (Affymetrix, Inc.) using an optimalinput of 80 ng per sample. As ctDNA analyses with this assay havenot been verified in large studies, this was a research use onlyapplication of the assay. The assay may detect clear gains andlosses at input as low as 40 ng (3, 4). The Oncoscan platformcontains more than 220,000 Molecular Inversion Probes inter-rogating approximately 900 cancer genes and relevant somaticmutations, and the assay can detect aberrations inDNA fragmentsof 50–125kb (3, 4). The somaticmutation panel contains hotspot74 mutations over 9 genes (BRAF, EGFR, IDH1, IDH2, KRAS,NRAS, PIK3CA, PTEN, TP53). The complete probe-set informa-tion is available in Supplementary Table S1 including copynumber variations (CNV) and somatic mutations (SMV).
Data files containing the intensity values for individual probeswere converted to probe set analysis results using the OncoScanConsole v1.2 Software using the FFPE reference. All seven samplesmet the recommended quality control thresholds of MAPD(�0.3) and ndSNPQC (�26). MAPD is a global measure of thevariation of all microarray probes across the genome representingthe median of the distribution of changes in log2 ratio betweenadjacent probes and is a measure of short-range noise in themicroarray data. Lower MAPD values are representative of higherquality control. ndSNPQC is a measure of how well genotypealleles are resolved in the microarray data. Larger ndSNPQCvalues are representative of higher quality control.
Copy number calls were calculated and binned using theTuScanAlgorithmanddata visualized inNexus ExpressOncoScan3.1 (BioDiscovery). Somatic mutations were scored for eachindividual, where theMutScores (ameasure of the signal responseof the marker relative to the expected signal distribution of thismarker in the absence of themutation) exceeded a predeterminedthreshold per marker (marker thresholds vary from 5–7). CNVswere scored against a global panel of approximately 900 cancer-related genes and individual amplifications, duplications, andregions exhibiting loss of heterozygosity were scored per sample(Supplementary Table S2 and S3). CNVs were then evaluated inthe COSMIC database to select for genes implicated in carcino-genesis, and this is reported for all seven cases in SupplementaryTable S3. Both somatic mutations and selected CNVs detected bythe Oncoscan FFPE Assay were confirmed using targeted NGS(IlluminaMiSeq). Specific genomic aberrations identified in Case1 were validated by quantitative PCR with remaining sample.Variants were selected for Sanger Sequencing validation if theywere suspected to be oncogenic from the COSMIC database and
had a CNV of 0 or of 3 or higher. Where applicable, samples werecomparedwith tumormolecular profile and plasma cell freeDNAmolecular profile.
Tissue next-generation sequencingFour individuals had tumor tissue frommetastatic sites sent for
targeted NGS (Foundation Medicine) before their ascites cfDNAanalysis. The assay sequenced the entire exons of 236 cancer-related genes, and select introns from19 genes often rearranged incancer (full list available at http://www.foundationone.com/genelist.php#). This method of sequencing allows for detection ofcopy number alterations, gene rearrangements, and somaticmutations with 99% specificity and >99% sensitivity for basesubstitutions at�5 mutant allele frequency and >95% sensitivityfor copy number alterations. A threshold of �8 copies was usedfor gene amplification.
Plasma cfDNA analysisFor the cfDNA analyses, barcoded sequencing libraries were
generated from 5 to 30 ng of plasma cfDNA. The exons of 54cancer genes, including all coding exons of 18 genes and therecurrently mutated exons in an additional 36 genes, were cap-tured using biotinylated custom bait oligonucleotides (Agilent),resulting in a 78,000 base-pair (78 kb) capture footprint. Sampleswere paired-end sequenced on an IlluminaHi-Seq 2500, followedby algorithmic reconstruction of the digitized sequencing signals.The coverage depth across all coding sequences in all samplesaveraged approximately 10,000X. Illumina sequencing readsweremapped to the hg19/GRCh37 human reference sequence, andgenomic alterations in cfDNA were identified from Illuminasequencing data by Guardant Health's proprietary bioinformaticsalgorithms. These algorithms quantify the absolute number ofunique DNA fragments at a given nucleotide position, therebyenabling ctDNA to be quantitatively measured as a fraction oftotal cfDNA. The limit of detection for single-nucleotide variantsin cfDNA by the Guardant360 assay is 0.1% (http://www.guardanthealth.com/).
ResultsCell-free DNA yields ranged from 3.9 ng to 38.4 ng/mL of
effusate in the seven subjects evaluated, indicating variability inDNA content. In each case (Tables 1 and 2), analysis of the ascitescfDNA found a range of detectable aberrations, and one individ-ual with cirrhosis (patient 7, Table 2) that served as a negativecontrol had minimal copy number variations detected. All evalu-able subjects are listed in Tables 1 and 2 wherein copy numbervariations (CNV) of �3 are listed. All CNVs and CNVs filteredby COSMIC are listed in Supplementary Tables S2 and S3,respectively.
Case PresentationsCase 1
A 63-year-old Asian man (nonsmoker) had a right upper lobemass detected after work-up for persistent cough. While attempt-ing curative surgery for perceived localized disease, intraoperativepleural deposits consistent with extensive tumor progressionwereobserved and the surgery was aborted. Biopsy of the tumor wasconsistent with adenocarcinoma. Hot spot testing by PCR-basedgene sequencingwas negative forALK, EGFR, orROS1 aberrations(Response Genetics). The patient completed five cycles of
Cell-Free DNA from Ascites and Pleural Effusions
www.aacrjournals.org Mol Cancer Ther; 16(5) May 2017 949
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

carboplatin and paclitaxel with bevacizumab, and his tumorburden remained stable for 17 months.
About 24months after diagnosis, the patient was noted to haveprogressive disease with an increase in the size of the pleural-based nodules. A second biopsy sample was taken from a pleuraldeposit, and targeted next-generation sequencing (NGS; Founda-tion Medicine) showed CDK4 and MDM2 amplification, but nosomatic mutations (Table 1; Case 1). The individual began aclinical trial with an anti-PD1 checkpoint antibody. About twomonths later, CT scan showed progression, and he began asubsequent trial with a molecularly matched CDK4 inhibitor. Hewas taken off study because of toxicity with fatigue, nausea, andanorexia. His condition deteriorated, and metastases to the peri-toneal cavity manifested with increased abdominal girth andascites. He needed biweekly paracenteses for symptomatic relief.cfDNA from the ascites was analyzed for CNVusing theOncoScanFFPE Assay Kit (ThermoFisher, Inc.) for research use. The resultsdemonstrated clear high copy EGFR amplification (copy number¼ 15, Table 1, Case 1). EGFR amplification was verified by
quantitative PCR (Supplementary Fig. S1). The patient diedwithout receiving anti-EGFR–directed therapy.
Case 2An 84-year-old woman was found to have a locally advanced
breast cancer. Core biopsy of the primary tumor was estrogenreceptor (ER) 90%positive, progesterone (PR) negative, Her2Neunegative. The patient was started on an aromatase inhibitor andhad a marginal response, and then underwent a mastectomy forlocal control. About three years after the initial diagnosis, thepatient was noted to have a livermetastasis on imagingwhichwasconfirmed as metastatic breast carcinoma on biopsy. She wastreated with a vaccine-based immunotherapy, but had progres-sion with peritoneal carcinomatosis within 7 months of the trialinitiation. The patient was treated with capecitabine at that time,but had significant gastrointestinal toxicity. NGS of her archivaltissuewas performed. Shewas noted to have an activating PIK3CAmutation (PIK3CA E542K) in the tissue, and the patient wastransitioned to exemestane and everolimus therapy. During this
Table 1. Subjects 1 and 2—demographics and molecular analyses
CaseNo. Age/sex Diagnosis Tissue NGSa,c
Date of tissuebiopsy for NGSand site Ascites cfDNAb
Date of ascitesacquisition/cytologyPositivity/DNA yield
1 64/man Adenocarcinoma of thelung, metastasis topleura and peritoneum
CDK4 amplification March 2013 EGFR amplification (CN 15) May 2014MDM2 amplification Pleural mass NOTCH1 loss (CN 1) Cytology positive
16 copy number variations(Supplementary Table S2).
DNA yield: 1153.2 ng30 ml effusate
2 84/woman Breast cancer (ERþ,PR-, Her2-) metastatic to
PIK3CA E542K September 2009 PIK3CA E542K August 2014
liver, omentum, pancreasand bone
NF1 loss Liver NF1 loss (CN 0), CCND1amplification (CN 7)concordant with tissue
Cytology positive
CCND1 amplificationTP53 splice site 993þ1G>AMCL1 amplification MEN1 amplification
(CN 6)
July 2014 cfDNAplasmad: PI3KCAE542K 4.7%, JAK2V617F 33.7%
318 copy number variations(Supplementary TableS2).
DNA Yield: 136.9 ng30 ml Effusate
Table 2. Subjects 3–7—demographics and molecular analyses
CaseNo. Age/sex Diagnosis Tissue NGSa,c
Date of tissueacquisition forNGS and site Ascites /pleural effusion cfDNAb
Date of effusateacquisition/cytologypositivity/DNA yield
3 74/male Pancreaticadenocarcinomametastastic
Not done N/A Ascites July 2014HMGA1 amplification (CNV ¼ 3 copies) Cytology positiveCBL amplification (CNV ¼ 3 copies) DNA Yield: 878.2 ng/30 ml
4 40/female Colon cancer metastaticto lung, liver
KRAS G12D July 2014 Pleural effusion August 2014APC K1165, I1580fs�69 Pelvic mass No CNVs �3 copies Cytology negative
Multiple CNVs <3 were found(Supplementary Table S3)
ctDNA plasma negativeCDKN1B truncationFOXP1 A506T DNA Yield: 141.7 ng/30 mlTP53 P190fs�57
5 62/female Renal cell carcinomametastatic to pancreas,lung
PTEN E114� April 2013 Ascites July 2014VHL P71fs�79 Kidney No CNVs �3 copies Cytology positiveAPC truncation, intron 12 Multiple CNVs <3 were found
(Supplementary Table S3)DNA Yield: 251.4 ng/30 ml
MLL2 T1246M6 58/female Rectal cancer metastatic
to liver, lungNot done N/A Ascites August 2014
YWHAE amplification (CNV ¼ 3 copies) Cytology: Not doneMultiple CNVs <3 were found(Supplementary Table S3)
DNA Yield: 119.3 ng/30 ml
7 55/female Cirrhosis (controlpatient)
Not done N/A Ascites August 2014No CNVs �3 copies Cytology negative
DNA Yield: 250.7 ng/30 mlaFoundationOne, Cambridge, Massachusetts.bAffymetrix, Santa Clara, California. CNVs with high copy gains and losses in actionable genes are reported.cAmplification infers � 8 copies.dGuardant cfDNA plasma assay.
Husain et al.
Mol Cancer Ther; 16(5) May 2017 Molecular Cancer Therapeutics950
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

treatment regimen, the patient showed tumor regression in theomental lesions and peritoneal thickening on imaging (Figure 1),and showed a decrease in tumor marker CA15.3 from 585 to 341U/mL. The patient eventually required hospitalization for pneu-monitis thought to be drug induced by the everolimus, andthe exemestane and everolimus were discontinued. The patientwas then given additional chemotherapy with capecitabine andnavelbine but, upon progression, opted for a palliative treatmentplan. Of note, the ascites cfDNA from a palliative paracentesisshowed the original PIK3CA E542Kmutation found in the tumortissue NGS. Plasma cfDNA also showed this alteration (Guar-dant360 assay, 54 gene assay; http://www.guardanthealth.com/guardant360/).
Effusate cfDNA Fragment Sizes and DNAYield
Estimation of ascitic cell-free DNA size based on fluorescence-based capillary electrophoresis demonstrates an effusate cfDNAfragment size of approximately 150–160 bp and a smaller peakbetween 300–400 bp. A representative capillary electrophoresisprofile is shown in Fig. 2. These fragment sizes correlatewith thosefragment sizes seen in plasmawhich are typically centered around
166 bp, approximately the length of DNA wrapped around anucleosome plus linker, and a minor peak at approximately 340bphas also been reported (5, 6).Within 30mLof effusatematerialobtained from the seven subjects, DNAyield ranged from119.3 to1,153.2 ng (Tables 1 and 2). The MIP probes have 2 arms whichare each about 20 bp long and 1 bp between the two arms. Thismakes the smallest fragment of intact DNA that may be recog-nized approximately 45–50 bases long.
Observations on subjects 1 through 7Subject number 1 with metastatic lung cancer showed high
copy gain of EGFR (CNV ¼ 15) in ascites cfDNA that was notfound in the analysis of solid tumor tissue (Table 1; Fig. 3A and B,Case 1). Primary tumor tissue showed only CDK4 and MDM2amplification. Altogether, the ascites cfDNA sample from Subject1 displayed 16 copy number alterations (Supplementary TableS2) and those that are citedwithin theCOSMICdatabase are listedin Table 1 and Supplementary Table S3. The HFN1B gene onchromosome 17 (copy number¼ 11; Fig. 3A and B) and the EGFRaberration was further verified by quantitative PCR assay (Sup-plementary Fig. S1). These alterations were distinct from theCDK4 and MDM2 amplification identified in the solid tumortissue. Detailed characterization of the genomic data revealed that
Case 2: Pretreatment CT scan;Before everolimus therapy
Case 2: Posttreatment CT scan at about two months; After everolimus therapy
Figure 1.
Index Subject 2 was noted to havea PI3KCA E542K mutation in blood,tissue, and ascites. The patientreceived everolimus withexemestane and had a responsein omental lesions on serial scans.
2,150LM UM
RFU
2,125
2,100
2,075
2,050
2,025
2,000
1,975
1,950
1,925
1,891
35 100
200
300
400
Size (bp)
500
600
700
800
900
1,00
01,
200
1,50
02,
000
3,00
0
6,00
0
Figure 2.
Capillary electrophoresis of ascitescfDNA. Fragment sizes of ascitescfDNA species are centered around166 base pairs, approximately thelength of DNA around a nucleosomeplus linker and a minor peak at 340base pairs. This correlates withfragments sizes in plasma.
Cell-Free DNA from Ascites and Pleural Effusions
www.aacrjournals.org Mol Cancer Ther; 16(5) May 2017 951
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

0.31% of the cfDNA genome detected in the ascites was impactedby chromosomal changes.
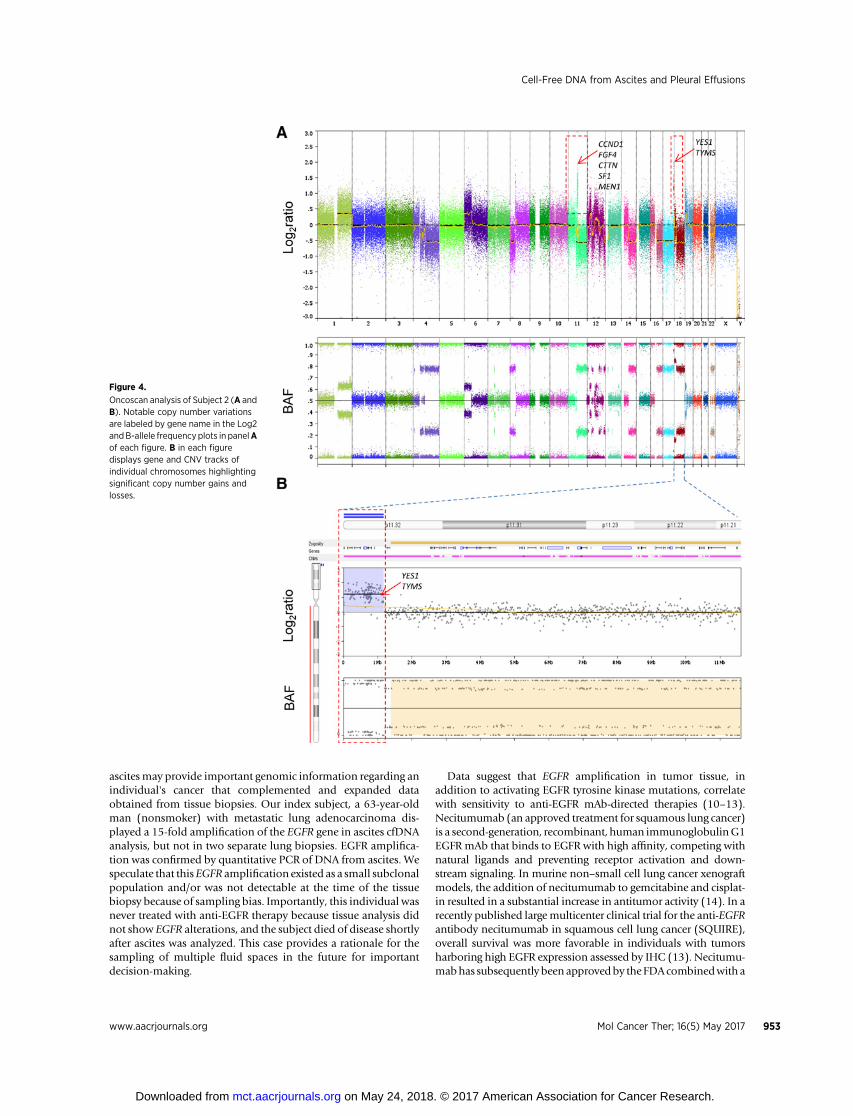
For Subject number 2, the ascites cfDNA detected a PIK3CAE542 point mutation that was also present in the originaltissue biopsy and in blood based cfDNA analysis (Table 1;Fig. 4A and B, Case 2). This mutation was confirmed in theascites by directed NGS through Illumina MiSeq v2 chemistry.Furthermore, the patient received PIK3CA-directed therapywith everolimus and had response with decrease in the sizeof her tumor (Fig. 1) and declining tumor marker CA15.3. Atthe time of the individual's paracentesis, which was 6 monthsafter treatment with everolimus, a total of 318 copy numberalterations were observed in the ascites (Supplementary TableS2). High copy gains (copy number ¼ 6) were observed inchromosome 11 (CCND1), and copy loss of NF1 gene wasdetected in chromosome 22 (Fig. 4A and B). The alterationswere consistent with tissue NGS results from the tumor biopsy.Additional alterations were seen, and a significant number of
copy number alterations were observed to cluster on chromo-some 12.
The remaining four individuals with cancer had genetic altera-tions identified that were subsequently filtered by correlatingthose with the COSMIC database (Table 2; Supplementary TableS3).One individualwith cancer (Table 2, subject 4)with cytology-negative disease did not have high expression of CNVs in theirpleural effusion, and the subject likely had an effusion from anetiology other than malignancy. An individual with cirrhosisshowed only minor alterations in their ascites (Table 2, subject7; Supplementary Table S3).
Discussion
There is emerging evidence that cfDNA isolated from blood orplasma can be used to detect DNA shed from metastatic solidtumors (7–9). To the best of our knowledge, our data demon-strate, for the first time, that analysis of cfDNA isolated from
Figure 3.
Oncoscan analysis of Case study 1(A and B). Subject 1 had very highexpression of EGFR and HFN1B. Wholegenome evaluation of copy numberalterations are ordered sequentially bychromosomes represented differentcolors. Notable copy number variationsare labeled by gene name in the Log2 andB-allele frequency plots in panelA of eachfigure. B in each figure displays gene andCNV tracks of individual chromosomeshighlighting significant copy numbergains and losses.
Husain et al.
Mol Cancer Ther; 16(5) May 2017 Molecular Cancer Therapeutics952
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
ascitesmay provide important genomic information regarding anindividual's cancer that complemented and expanded dataobtained from tissue biopsies. Our index subject, a 63-year-oldman (nonsmoker) with metastatic lung adenocarcinoma dis-played a 15-fold amplification of the EGFR gene in ascites cfDNAanalysis, but not in two separate lung biopsies. EGFR amplifica-tion was confirmed by quantitative PCR of DNA from ascites. Wespeculate that thisEGFR amplification existed as a small subclonalpopulation and/or was not detectable at the time of the tissuebiopsy because of sampling bias. Importantly, this individual wasnever treated with anti-EGFR therapy because tissue analysis didnot show EGFR alterations, and the subject died of disease shortlyafter ascites was analyzed. This case provides a rationale for thesampling of multiple fluid spaces in the future for importantdecision-making.
Data suggest that EGFR amplification in tumor tissue, inaddition to activating EGFR tyrosine kinase mutations, correlatewith sensitivity to anti-EGFR mAb-directed therapies (10–13).Necitumumab (an approved treatment for squamous lung cancer)is a second-generation, recombinant, human immunoglobulinG1EGFR mAb that binds to EGFR with high affinity, competing withnatural ligands and preventing receptor activation and down-stream signaling. In murine non–small cell lung cancer xenograftmodels, the addition of necitumumab to gemcitabine and cisplat-in resulted in a substantial increase in antitumor activity (14). In arecently published largemulticenter clinical trial for the anti-EGFRantibody necitumumab in squamous cell lung cancer (SQUIRE),overall survival was more favorable in individuals with tumorsharboring high EGFR expression assessed by IHC (13). Necitumu-mabhas subsequently been approvedby theFDAcombinedwith a
Figure 4.
Oncoscan analysis of Subject 2 (A andB). Notable copy number variationsare labeled by gene name in the Log2andB-allele frequencyplots in panelAof each figure. B in each figuredisplays gene and CNV tracks ofindividual chromosomes highlightingsignificant copy number gains andlosses.
Cell-Free DNA from Ascites and Pleural Effusions
www.aacrjournals.org Mol Cancer Ther; 16(5) May 2017 953
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

platinum-based doublet chemotherapy. An additional studyassessed disease response to gefitinib in patients with EGFR ampli-fication as detected by FISH, and there was a nonstatisticallysignificant trend toward benefit. In this study, disease control wasdemonstrated in 63% of EGFR/FISH-positive patients versus 39%of FISH-negative patients (10). Further studies may consider thevalue of CNV data compared with IHC and FISH to direct therapyagainst EGFR amplification and characterize its association withresponse to anti-EGFR–based therapy.
Our second index subject was a woman with breast cancer whohad a PIK3CA E542K mutation identified in her tumor tissue,cfDNA from blood plasma, and cfDNA from ascites. This subjectreceived the approved regimen of everolimus with antiendocrineexemestane therapy, which correlated with radiologic tumorregression onCT scans (Fig. 1) and a serologic response in proteintumormarkers. PIK3CAE542K is an activatingmutation foundonexon 9 of the PIK3CA gene (15). The BOLERO-2 trial whichassessed the efficacy of everolimus plus exemestane for Her2-Neu-negative breast cancer showed a greater progression-freesurvival benefit with everolimus compared with placebo forpatients with a PIK3CA exon 9 mutation compared with thosewith other PIK3CA mutations (16, 17). A recent correlativeanalysis of genetic alterations and everolimus benefit in hor-mone-positive breast cancer demonstrated more efficacy in indi-viduals with exon-specificmutations in PIK3CA exon 9 comparedwith exon 20 (17). Preclinically, in MCF7 breast cancer cellsharboring the PI3KCA E542K mutation, the combination ofeverolimus with antiestrogen therapy can inhibit proliferationand trigger apoptotic cell death (18). Individuals who had higherchromosomal instability did less well than those who had lowerchromosomal instability (17).
In the cases represented, analyses of ascites cfDNA demonstrat-ed the presence of tumorigenic CNVs in cancer-associated genes(Supplementary Table S2 and S3). For Subject 2, PIK3CA E542Kmutation, NF1 loss, and high copy CCND1 amplification wasfound in both tissue and ascites. For Subject 1, the CDK4 andMDM2 amplification present in the lung tumor was not detectedin the ascites. Complete concordance between tumor tissue DNAand cfDNA may be confounded by timing of sample collection,therapy that a patient has received, and the use of differentsequencing assays. It remains possible that some subset of tumorcells have a specificmolecular profile thatmaybe important in celladhesion, migration, and metastasis to the peritoneal cavity,which would lead to these alterations to be disproportionallydetected in ascites cfDNA.
Taken together, this analysis provides a potential rationale fora strategy of molecular analysis across fluid spaces includingtissue, plasma, and effusions to provide a comprehensive analysisof relevant targets. Some of the limitations of this study includethe fact that further analyses will need to be done to set appro-priate thresholds geared toward therapeutic action-ability andaddress the hierarchy of subclonal populations. The significanceof detecting discordant alterations in primary tissue versus bloodversus effusions is unclear, and further studies will need to assesstherapeutic predictive capacity with all versus any one of these
modalities. This was a small sample size, and a larger study isunderway to evaluate the predictive capacity of genetic alterationsin effusions caused by cancer of various histologies, and anunderstanding of the predictive value of characterizing viablecells within various effusates versus effusate cfDNA. Furthermore,theOncoscanwas used for researchuseonly to illustrate a biologicconcept and, as the assay has not been verified for ctDNA eval-uation, and further evaluation will be needed to characterize anyindications beyond its intended use.
Our data demonstrate that cfDNA containing potentiallyactionable oncogenic alterations such as somatic mutationsand CNVs can be discovered in ascites and pleural effusions.This information may be of significance when developingtherapeutic strategies and anticipating different mechanismsof resistance. Through serial collection, one can obtain alongitudinal perspective of genomic change through time andunder selective pressure by therapy. The ability to access viablecells in ascites and pleural effusions is a distinguishing factorwhich may have important implications in the creation ofpatient derived xenograft models and RNA and protein anal-yses. Ongoing studies are investigating concordance betweentissue DNA, plasma cfDNA, and ascites cfDNA at the same timepoint and in a larger cohort of samples.
Disclosure of Potential Conflicts of InterestE. Fung is an employee at ThermoFisher Scientific. R. Kurzrock has ownership
interest in Novena, Inc. and Curematch, Inc., reports receiving a commercialresearch grant from Genentech, Merck Serono, Pfizer, Sequenom, FoundationMedicine, and Guardant, and is a consultant/advisory board member forSequenom, Actuate Therapeutics, and XBiotech. Hatim Husain has receivedresearch support from Trovagene, Inc. and Affymetrix and served on an advisoryboard for FoundationMedicine.Nopotential conflicts of interest were disclosedby the other authors.
Authors' ContributionsConception and design: H. HusainDevelopment of methodology: H. Husain, G. Gomez, E. FungAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): H. Husain, D. Quan, G. Gomez, B. Woodward,S. Venkatapathy, R. DuttaguptaAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): H. Husain, D. Nykin, N. Bui, S. Venkatapathy,R. Duttagupta, E. Fung, S.M. Lippman, R. KurzrockWriting, review, and/or revision of the manuscript: H. Husain, D. Nykin,N. Bui, R. Duttagupta, S.M. LippmanAdministrative, technical, or material support (i.e., reporting or organizingdata, constructingdatabases):H.Husain,D.Nykin,B.Woodward,S.M.LippmanStudy supervision: H. Husain, B. Woodward
Grant SupportThis project was funded by institutional funds at The University of Cali-
fornia, San Diego. Funded in part by the National Cancer Institute grant P30CA016672 (R. Kurzrock).
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received July 5, 2016; revised November 21, 2016; accepted December 7,2016; published online May 3, 2017.
References1. Diaz LA Jr, Williams RT, Wu J, Kinde I, Hecht JR, Vogelstein B, et al. The
molecular evolution of acquired resistance to targeted EGFR blockade incolorectal cancers. Nature 2012;486:537–40.
2. Gerlinger M, Rowan AJ, Horswell S, Larkin J, Endesfelder D, Gronroos E,et al. Intra-tumor heterogeneity and branched evolution revealed bymulti-region sequencing. N Engl J Med 2012;366:883–92.
Mol Cancer Ther; 16(5) May 2017 Molecular Cancer Therapeutics954
Husain et al.
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

3. Yang Y, Cottman M, Schiffman JD. Molecular inversion probes: a novelmicroarray technology and its application in cancer research. Cancer Genet2012;205:341–55.
4. Wang Y, Carlton VE, Karlin-Neumann G, Sapolsky R, Zhang L, Faham M,et al. High quality copy number and genotype data from FFPE samplesusing Molecular Inversion Probe (MIP) microarrays. BMC Med Genomics2009;2:8.
5. Lo YM, Chan KC, SunH, Chen EZ, Jiang P, Chiu RW, et al. Maternal plasmaDNA sequencing reveals the genome-wide genetic and mutational profileof the fetus. Sci Trans Med 2010;2:61ra91.
6. Fan HC, Blumenfeld YJ, Chitkara U, Hudgins L, Quake SR. Analysis of thesize distributions of fetal and maternal cell-free DNA by paired-endsequencing. Clin Chem 2010;56:1279.
7. Crowley E, Di Nicolantonio F, Loupakis F, Bardelli A. Liquid biopsy:monitoring cancer-genetics in the blood. Nat Rev Clin Oncol 2013;10:472–84.
8. Bettegowda C, Sausen M, Leary RJ, Kinde I, Wang Y, Diaz LA Jr, et al.Detection of circulating tumor DNA in early- and late-stage humanmalignancies. Sci Transl Med 2014;6:224ra24.
9. HaberDA, Velculescu VE. Blood-based analyses of cancer: cell-free cells andcell-free DNA. Cancer Discov 2014;4:650–61.
10. Hirsch FR, Varella-Garcia M, McCoy J, West H, Xavier AC, SouthwestOncology Group, et al. Increased epidermal growth factor receptor genecopy number detected by fluorescence in situ hybridization associateswith increased sensitivity to gefitinib in patients with bronchioloalveolarcarcinoma subtypes: a Southwest Oncology Group Study. J Clin Oncol2005;23:6838–45.
11. Pirker R, Pereira JR, von Pawel J, Krzakowski M, Ramlau R, Park K, et al.EGFR expression as a predictor of survival for first-line chemotherapyplus cetuximab in patients with advanced non-small-cell lung cancer:
analysis of data from the phase 3 FLEX study. Lancet Oncol 2012;13:33–42.
12. Bell DW, Lynch TJ, Haserlat SM, Harris PL, Okimoto RA, Brannigan BW,et al. Epidermal growth factor receptor mutations and gene amplificationin non–small-cell lung cancer: Molecular analysis of the IDEAL/INTACTgefitinib trials. J Clin Oncol 2005;23:8081–92.
13. Thatcher N, Hirsch FR, Luft AV, Szczesna A, Ciuleanu TE, Dediu M, et al.Necitumumab plus gemcitabine and cisplatin versus gemcitabine andcisplatin alone as first-line therapy in patients with stage IV squamousnon-small-cell lung cancer (SQUIRE): an open-label, randomised, con-trolled phase 3 trial. Lancet Oncol 2015;16:763–74.
14. Samakoglu S, Deevi DS, Li H, Wang S, Murphy M, Tonra JR, et al.Preclinical rationale for combining an EGFR antibody with cisplatin/gemcitabine for the treatment of NSCLC. Cancer Genomics Proteomics2012;9:77–92.
15. Sohye K, Bader AG, Vogt PK. Phosphatidylinositol 3-kinase mutationsidentified in human cancer are oncogenic. Proc Nat Acad Sci U S A 2005;102:802–7.
16. Baselga J, Campone M, Piccart M, Burris HA III, Rugo HS, Hortobagyi GN,et al. Everolimus in postmenopausal hormone-receptor-positive advancedbreast cancer. N Engl J Med 2012;366:520.
17. Hortobagyi GN, Chen D2, Piccart M, Rugo HS, Burnstein HA, Baselga J,et al. Correlative analysis of genetic alterations and everolimus benefit inhormone receptor-positive, human epidermal growth factor receptor2-negative advanced breast cancer: results from BOLERO-2. J Clin Oncol2016;34:419–26.
18. Boulay A, Rudloff J, Ye J, Zumstein-Mecker S, O'Reilly T, Lane HA, et al.Dual inhibition of mTOR and estrogen receptor signaling in vitroinduces cell death in models of breast cancer. Clin Cancer Res 2005;11:5319–28.
www.aacrjournals.org Mol Cancer Ther; 16(5) May 2017 955
Cell-Free DNA from Ascites and Pleural Effusions
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
2017;16:948-955. Mol Cancer Ther Hatim Husain, David Nykin, Nam Bui, et al. Insights into Genomic Aberrations and Disease BiologyCell-Free DNA from Ascites and Pleural Effusions: Molecular
Updated version
http://mct.aacrjournals.org/content/16/5/948
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2017/05/04/16.5.948.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/16/5/948.full#ref-list-1
This article cites 18 articles, 9 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/16/5/948To request permission to re-use all or part of this article, use this link
on May 24, 2018. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from