Embed Size (px)
Citation preview

Cellular Electrophysiology of Amlodipine: Probing the Cardiac L-Type Calcium Channel
Robert S. Kass, PhD, Joseph P. Arena, PhD, and Stefan Chin, BS
The eie&ophysioiogk pmpertb of amiodipine in mgusneagig VenMcular cells were! investi- gated.Tbedegwwofio&Mionofthedrugmole- adewasfoundtoaffectboththedeveiopmentof MdUU?t%COV~flWllbiOCkOfL-typeC&kllbl chameis. Under agudins comlitiot~s, when most of thedrugisinaneutralform,theactionsofamlodi- pine resembh previousiy described neutrd dihydro- Pyric#ne MfP) compouwb. under these conditions, caBciwnchannetblockbyamIodipinsisreversWy mgdated by cell msmbrina potential, i.e., bbck is morspronouncedatvoltagesposttiveto-SOmV and compieteiy reiieved at vottages negative to -80 mV. When the drug molec& is ionized, Mock de- vehps very siowiy at podtive msnlbrane potentiais andisvsrydiffk4Htorelieveanretwningthe membrane poteihi to msre negative voltages. It is canck&dthatthedegreeofkmiHionoftheduug mdeudeiimits accesstotheDHPreceptorandthat the dfug-bound recepbr can be titrated by extra- cdluiar hydrogen ions. Thess results place limita- SonsonthekcstionoftheDHPrecepWwithinths cardiac sarcokmmai membrane.
(Am J Cardid 1989;64:3S 142 I)
From the Department of Physiology, University of Rochester Medical Center, Rochester, New York.
Address for reprints: Robert S. Kass, PhD, University of Rochester Medical Center, Department of Physiology Box 642, 601 Elmwood Avenue, Rochester, New York 14642.
A mlodipine is a diiydropyridine (DHP) compound with a pKa of 8.6. It has been shown to displace nitrendipine bindingt and to inhibit calcium-de-
pendent contractions. These amlodipine effects, unlike those of other DHP compounds, take several hours to develop.1*2 In contrast to amlodipine, other DHP com- pounds such as nisoldipine and nitrendipine, have pK,s below 3.0 and are neutral at physiologic pH. Because 94% of amlodipine molecules are ionized under physiologic conditions, it was of interest to determine whether the degree of ionization affects the manner in which this compound blocks calcium channels and, perhaps, ac- counts for the unique kinetic properties of this drug.
The importance of DHP derivatives as probes of L- type calcium channels is clear (reviewed by Triggle and Venter3); however the manner in which these compounds reach the receptor that causes inhibition of channel activ- ity has not been systematically investigated. In the case of the nerve sodium channel, a great deal of information about channel structure has been obtained by probing channel block by neutral and charged local anesthetic molecules. The modulated receptor hypothesis of Hille4q5 and Hondeghem and Katzung6 was based on the results of these experiments. According to that hypothesis, drugs may bind to different states of a voltage-gated ion chan- nel with varying affinity, but drug access to the receptor is dictated by molecular charge. Neutral drugs can move through hydrophilic or hydrophobic pathways, whereas ionized molecules are restricted and cannot easily move through hydrophobic regions of the membrane lipid bi- layer.
Although the modulated receptor hypothesis has been useful in interpreting the voltage-dependent block of cal- cium channels by neutral DHP compounds,7p8 tests of the influence of drug ionization on channel modulation have not been performed.
In the work summarized in this paper and reported on in more detail by Kass and Arena,9 we were interested in determinmg how the ionization of arnlodipine affected its block of calcium channels in the heart. In addition, we were interested in using this information to provide in- sight into the structure of the heart L-type calcium chan- nel. Our results indicate that drug ionization affects block of heart calcium channels in a manner that is very similar to local anesthetic block of nerve sodium channels, but that access to the DHP receptor occurs through a path- way that is quite different than that of local anesthetics in the sodium channel.
THE AMERICAN JOURNAL OF CARDIOLOGY NOVEMBER7,1989 35 I

A SYMFDSIUM: PRARMACDLDDY AND TRERAPEUTIC CDNSIDERATIDNS OF AMLDDIPINE
0 -A k
2 -400 ,o z’ i+
II ,’
5 A u -800
l- “1
IL- -1200
I I
0 20 40 60 ‘id@
TIME AT -50 mV (set)
METHODS The experiments summarized in this article were per-
formed in single ventricular myocytes that had been iso- lated after the procedure of Mitra and Morad.*O Experi- mental details are provided in Kass and Arena9 but are briefly summarized here. Membrane currents were re- corded using a whole cell arrangement of the patch clamp procedure.tl Potassium currents were eliminated by re- placing internal and external potassium with cesium. So- dium current was eliminated by choice of membrane potential, sodium replacement with tetramethylammo- nium ion or tris(hydroxymethyl)-aminomethane, or by the addition of 10 to 50 PM tetrodotoxin. Pipette solution also contained 3 mM adenosine triphosphate and 11 mM EGTA. Calcium or barium ions were used as charge carries of Ia. Solutions were changed by way of gravity- fed chambers that could be selected with an electronic valve. Drugs were dissolved in mM stock solutions and diluted down appropriately for each experiment. Solu- tions were buffered as described in Krafte and Kass12 over a range of external pH 6.0 to 10.0.
Amlodipine, a gift from Pfizer Central Research (Sandwich, United Kingdom) was dissolved in water. Amlodipine has a pK, of 8.6 and is thus 94% charged at pH 7.4 and is 96% neutral at pH 10.0.
Voltage protocols were designed to investigate the kinetics of the development of and recovery from block of Ia. We were thus interested in the DHP receptor associ- ated with “antagonism” of calcium channel currents. 13-i5 Trains of pulses were applied to minimize experimental time. To study onset of block, the cell holding potential (HP) was set at a negative voltage (usually -80 mV) under stimulation-free conditions for at least 2 minutes. Then, the HP was changed to less negative levels (-30 to
-50 mV) and a series of pulses were applied to measure Iti. The pulse frequency and duration, which were var- ied, are noted in each figure legend. Recovery from block was studied using a similar approach, but in this case the cell was held at a positive conditioning voltage ( 10 to - 10 mV) for a given duration, Then, the membrane was stepped to a negative voltage (usually -80 mV) and pulses were applied to activate and measure 1~~.
RESULTS Neutralrmbdipivw-vott8g~bbckWith-
out repaitive pukingr It is well-established that neutral DHPs such as nisoldipine and nifedipine are much more potent if applied to depolarized cells. Inhibition of 1~ by these compounds is rapidly relieved on returning the cell to negative membrane potentials, and repetitive pulses to voltages that cause channels to open are not required to promote block.8 In the fust set of experiments of the present study we were interested in determining whether the neutral amlodipine molecule had similar characteris- tics.
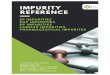
These experiments were performed in solutions buff- ered to pH, 10.0, where greater than 96% of amlodipine molecules are neutral. Figure 1 shows that, under these conditions, amlodipine acts in a manner that resembles previously described neutral DHPs. The figure summa- rizes an experiment in which pulse trains were applied as HP was changed from -80 to -50 mV. In the absence of drug, the amplitude of 1~ was constant during the train of pulses, whereas in the presence of amlodipine, current is virtually completely inhibited within 60 seconds.
After block had been induced by this train protocol, cell membrane potential was returned to -80 mV with- out stimulation for 2 minutes. A train of very brief pulses
36 1 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 64

-2500 0 10 20
TIME AT -80 mV (seconds)
PULSE-DEPENDENT BLOCK IN pH 7.4 -40 mV/40 ms pulses
-10004 0
A 20 40 60 80 100
TIME AT -40 mV (set)
applied once every 30 seconds was then resumed. Two important points emerged: The first pulse of the train evoked a current as large as the first pulse of the previous train and block redeveloped at roughly the same rate. Thus, as had been shown for other neutral DHPs, block which is enhanced at positive voltages is readily relieved on return to negative membrane potentials, and repetitive pulsing to voltages that cause channels to open is not necessary to promote voltage-dependent block.
The kinetics of recovery from block by neutral amlo- dipine are illustrated in Figure 2. The figure shows recov- ery of 1~ at -80 mV after application of 20-second conditioning pulses in the absence and presence of a drug. In control, Iti recovers from pulse-induced inactivation in less than 1 second. Amlodipine induces a slow component to the recovering current. This process, which was char- acterized by a time constant on the order of 10 seconds, most likely reflects recovery from drug-blocked channels.
Blockbyionizedam~devebps*wiyandis CifKadtto reverse: As was the case for neutral drugs, block of Ica by ionized amlodipine (pHO 7.4) was en- hanced by depolarized cell voltages, but the development of block was very slow if trains of brief pulses are applied (Fig. 3). However, in contrast to neutral drugs, develop ment of block by ionized amlodipine was more rapid if pulse width was increased during the train (Fig. 4). This result is consistent with, but not proof of, the hypothesis that requires the channels to first open before ionized amlodipine can produce block (but see next).
Figure 4 also illustrates another difference between ionized and neutral drug block: poor reversal of block at negative voltages. In the experiment of Figure 4, two pulse trains were applied in the presence of the drug. At first, brief pulses were applied infrequently (compare with Fig. 1) and then the cell was returned to -80 mV for 2 minutes without pulsing. A second pulse train was im-
THE AMERICAN JOURNAL OF CARDIOLOGY NOVEMBER 7,1989 37 1

A SYMPOSIUM: PHARMACOLOGY AND THERAPEUTIC CONSIDERAYIONS OF AMLOMPINE
.PA*,,, * nA-aA
-1300J 0 20 40 60 a0 100
TIME AT -50 mV (set)
posed with longer duration pulses and block redeveloped; however, there was little evidence of recovery from block under these conditions. Thus, in addition to promoting a very slow onset of block, the ionized drug molecules react- ed much differently to membrane potential once the channel had been blocked.
One possible explanation consistent with our findings for ionized amlodipine is that the DHP receptor lies with- in the calcium channel pore and that ionized drug mole- cules can only reach it after channels have opened. Fur- thermore, once bound to the DHP receptor, ionized amlo- dipine molecules can only unblock the channel if channels are forced to open again.
To test for this possibility, we first wanted to deter- mine whether the DHP receptor was located near the outer or inner surface of the cell membrane. Here we used the marked contrast in activity of the charged and neutral drug molecules to determine whether external H+ ions could reach and affect the drug-bound DHP receptor.
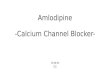
Extemalhy&ogeniancanreadntheth@awldi- hythpyddb mcepto~ We performed an, experiment in which changes in channel block induced by external pH were monitored in the same cell. In this protocol we exposed a cell to amlodipine in a solution buffered to pH 6.0. At thii pH, less than 0.25% of amlodipine molecules
38 I THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 64
are neutral. As expected, a depolarizing voltage pulse train promoted block, but now the rate of block was extremely slow with no recovery from block on returning to -80 mV (Fig. 5A). We then changed to an external solution buffered to pH 10.0 and measured recovery from block at -80 mV. Block was relieved within 30 seconds of the solution change.
This experiment demonstrated several points. First, it confirmed the fmding that the degree of ionization of the drug molecule does, in fact, affect the onset of and recov- ery from block. Block is even slower and more difficult to reverse if a greater fraction of drug molecules is charged. In addition, it showed that the drug-bound receptor was accessible to external H+ because block could be relieved by decreasing the external H+ concentration (Fig. 5B).
Because of this result, it was concluded that limits could be placed on the location of the DHP receptor. First, the receptor could lie within the channel as suggest- ed, but if so, a pathway must exist for H+ ions to reach the receptor even if channels are blocked. Second, the recep- tor could lie within the membrane bilayer but near the outer face of the cell surface. If the latter possibility proves correct, then channel block and unblock by the ionized drug molecule does not involve a trapping mecha- nism within the channel pore.

-250
-400 0 50 100 150 200 250
TIME (seconds)
B
3 -400 0-O ONSET pH 6.0
5
E
O-0 RECObERY pH 6.0
-600 A RECMRY pH 10.0
z
-800
TIME (seconds)
9lockisnotpromotdby-smkapine: We applied amlodipine intracellularly to test for an intra- porebinding site. In this experiment (Fig. 6) a high amlo- dipine concentration (50 PM) in the patch pipette was included and train protocols were applied that caused block when amlodipine was applied extracellularly. The currents recorded with the train protocol immediately after breaking through the membrane to establish whole cell recording conditions showed no voltagedependent block and there was no evidence of additional block after another 15 minutes. Intracellular and pipette concentra- tions are expected to equilibrate within 12 minutes for pipette and cell dimensions of our experimentsr6 Thus,
our result strongly suggests that ionized amlodipine does not reach the DHP receptor through a channel pore path- way but, instead, through the cell membrane.
CONCLUSION We have shown that external pH mod&s the block
of 1~ by amlodipine over a pH range in which the degree of ionization of the drug molecule is changed. These re- sults have important implications for the actions of this drug as well as for the calcium channel that it modu- lates.
Because block by neutral amlodipine is enhanced by depolarization without concomitant pulses and is revers-
THE AMERICAN JOURNAL OF CARDIOLOGY NOVEMBER 7.1989 39 I

A SYMPOSIUM: PHARMAWLDDY AND THERAPEUTIC CDNSlDERAllONS DF AMLDDIPINE
INTERNAL AMLODIPINE
1 MN 15 MN
“ r
0 i0 40 $0 ii0
Time at -40 mV (set) m-0 1’ A-A 15’
ibly relieved at negative voltages, our work shows that the amlodipine molecule is capable of modulating calcium channel activity in a manner consistent with previously investigated DHPs. However, ionized amlodipine block of Ica at positive potentials is augmented by pulses that open channels and promote inactivation. Block by ionized amlodipine is also only partially relieved on hyperpolari- ration and the time course of the recovery that is observed is 10 times slower than that for neutral drug (see Kass and Arenal for details). Thus, it is the degree of ioniza- tion of the amlodipine molecule that gives this drug its unique properties. L2
Furthermore influence of pII,, on drug ionization and, in turn, on drug action may have important implications for the usefulness of amlodipine in treating electrical dis- orders related to the ischemic heart. For example, since PI-&, decreases during &hernia the fraction of ionized amlodipine molecules should increase. Block by ionized amlodipine is more persistent than for neutral drug so it may be more potent during ischemia and offer the protec- tive effects proposed for blockade of 1~a.r~
In many ways, the results of our studies resembled the effects of pH,, on local anesthetic block of sodium chan- nels that has been well character&d by the modulated receptor formalism.“6 This would be particularly inter- esting because of the homology between the 2 channel types already documented from molecular studies (re
40 1 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 64
viewed by CatteraW9). However, some important diier- ences also emerged. In contrast to the local anesthetic receptor of sodium channels, the DHP receptor is not accessed by intracelhrlarly applied amlodipine, making a channel pore pathway an unlikely possibility for the charged DHP.
If ionized amlodipine does not reach the DHP recep tor through the channel pore, it is likely that it acts through a membranebound pathway. This is possible if all but the polar headgroup of the amlodipine molecule partitions into the membrane bilayer as suggested by Mason et al.” In this case, ionized amlodipine would be restricted in its interactions with the DHP receptor and conformational changes of the channel protein induced by membrane potential would underlie the voltage-de pendence of block that we have measured.
Our experimental results place limitations on the loca- tion of the DHP receptor responsible for antagonistic activity. The drug-bound receptor is accessible to external hydrogen ions. Thus, the receptor either lies within the channel pore but near the external surface of the cell membrane or the receptor lies within the lipid bilayer adjacent to the channel pore but also near the external surface of the membrane. Ongoing experiments are de signed to distinguish between these 2 possibilities and to determine the mechanism that underlies the irreversibili- ty of block by the ionized molecule.

REFERENCES 1. Burges RA, Carter AJ, Gardiner DF, Higgins AJ. Amlodipine, a new dihydro- pyridine calcium channel blocker with slow onset and long duration of action (abstr). Br J Pharmacol 1985;85:281P. 2. Burges RA, Gardiner DG, Gwilt M, Higgins AJ, Blackbum KJ, Campbell SF, Cross PE, Stubbs JK. Calcium channel blocking properties of amlodipine in vascular smooth muscle and cardiac muscle in vitro: evidence for voltage modula- tion of vascular dihydropyridine receptors. J Cardiwax Phnrmacol1987,9;1 IO- 119. 3. Triggle DJ, Venter JC. Structure and Physiology of the Slow Inward Calcium Channel. New York Alan R. Liss, 1987:1-281. 4. Hille B. The pHdependent rate of action of local anesthetics on the Node of Ranvier. J Gen Physiol 1977,69:475-496. 1. Hille B. Local anesthetics: hydrophilic and hydrophobic pathways for the drug- receptor reaction. J Gen Physiol 1977.69:497-515. 6. Hondeghem LM, Katzung BG. Time and voltage dependent interaction of antiarrhythmic drugs with cardiac sodium channels. B&him Biophys Acta 1977;472:373-398. 7. Bean BP. Nitrendipine block of cardiac calcium channels: high-afftnity binding to the inactivated state. Pros Nat1 Acad Sci USA 1984;81:63886392. 8. Sanguinetti MC, Kass RS. Voltage-dependent block of calcium channel cur- rent in the calf cardiac Purkinje fiber by dihydropyridine calcium channel antago nists. Circ Res 1984;55:336-348. 9. Kass RS, Arena JP. Irdluence of pH, on calcium channel block by amlodipine, a charged dihydropyridine compound. J Gen Physiol1989,93:1109-1127. 10. Mitra R, Morad M. A uniform enzymatic method for dissociation of myo- cytes from hearts and stomachs of vertebrates. Am J Physiol1985;249:HlO56- HMO. 11. Hamill OP, Marty A, Neher E, Sakmann B, Sigworth FJ. Improved patch- clamp techniques for high-resolution current recording from cells and cell-free membrane patches. Pfrugers Arch 1981;391:85-IW. 12. Krafte DS, Kass RS. Hydrogen ion modulation of Ca channel current in cardiac ventricular cells: evidence for multiple mechanisms. J Gen Physiol 1988.91.641-657. 13. Kokubun S, Pm&horn B, Becker C, Porzig H, Reuter H. Studies on Ca channels in intact cardiac cells voltage-dependent effects and cooperative interac- tions of dihydropyridine enantiomers. Mel Pharmacol1987;30:571-584. 14. Williams JS, Grupp IL, Grupp G, Vaghy PL, Dumont L, Schwartz A, Yatani A, Hamilton S, Brown AM. Profile of the oppositely acting enantiomers of the dihydropyridine 202-79 I in cardiic preparations: receptor binding, electrophysio- logical and pharmacological studies. Biochem Biophys Res Commun 1985;131: 13-21. 1s. Hamilton SL, Yatani A, Brush K, Schwartz A, Brown AM. A comparison between the binding and electrophysiological effects of dihydropyridines on cardi- ac membranes. Mel Pharmacol 1987;31:221-231. 16. Pusch M, Neher E. Rates of diiusional exchange between small cells and a measuring patch pipette. Pflugers Arch 1988:411:204-21 I. 17. Hescheler J, Pelzer D, Trube G, Trautwein W. Does the organic calcium channel blocker D6CNl act from the inside or outside on the cardiac cell mem- brane? Pflugers Arch 1982;393:287-291. 18. Nayler WG, Dillon JS, Sturrock WJ. Dihydropyridines and the protection of the ischaemic and anoxic myccardium. In: Fleckenstein A, Van Breeman C, Gross R, Hoffmeister F, eds. Cardiovascular Effects of Dihydropyridine-Type Calcium Antagonists and Agonists. Heidelberg Springer-Verlag, 1986460-471. 19. Catterall WA. Structure and function of voltage-sensitive ion channels. Sci- ence 1988:242:50-61. 20. Mason RP, Chester DW, Gonye GB, Hertctte LG. The effects of drug charge and membrane structure on the partitioning and location of l+dihydro- pyridine in model and native lipid bilayers (abstr). Biophys J 1988;53:348a. 21. Kass RS, Arena JP, Cbin S. Modulation of calcium channels by charged and neutral dihydropyridmes. In: Wray DW, Norman RI, Hess P, eds. Calcium Channels: Structure and Function. New York: Ann NYAcadSci, 1989:189-197.
PANEL DISCUSSION
Dr. VanhaMe (Rochedr, Mii): I would like to ask a question about the agonistic properties of the compound, i.e., the augmentation of the calcium current. Is it something that occurs with lower concentration of the agent?
Dr. Kass (Rochester, New York): No, we don’t see a concentration-dependent difference between the agonism and the block, but what I would like to test is the apparent difference in the time-course of the onset. When we see agonism, it is immediate and at negative holding poten- tials. We don’t have to depolarize the cell in order for the agonism to occur. That is the same as for neutral dihydro-
pyridines and occurs whether the drug is charged or neu- tral. So that to me is suggesting it may be a different site.
Dr. Vanhoutte: Again, to come back to what Mr. Burges told us earlier and the question I asked about the release of endothelial-dependent relaxing factor (EDRF). Agonists at calcium channels can be very po- tent releasers of EDRF so that particular aspect of your presentation makes the question I asked before even more interesting.
Dr. Lwchesi (Ann Arber, Milgan): You have looked at the effects of amlodipine on the channel, under conditions of normal oxygenation of tissue. Would you speculate as to what might occur under conditions of ischemia, where, I would assume, these charges on the membrane itself would be altered?
Dr. Kass: I think ischemia offers a very interesting challenge, if you will, for this particular kind of com- pound, because of the fact that locally, you would expect differences in hydrogen ion concentrations, around the ischemic tissue. Probably the most important difference between the neutral and charged form of the drug is the time course of onset of block and removal of block. Those of us who work at the cellular and molecular level tend to think that dihydropyridines change the conformation of the channel. They don’t physically block the pore, but they tell the channel to stay shut in an inactivated or unavailable form. One of the things that I am fascinated by with the charged drugs is that when the channel is locked in that nonconducting form, it doesn’t come back quickly. It is very difficult to reverse and that it is pH- or drug-ionization dependent. In regions where cells are more acidic, that feature of the drug is going to be en- hanced more, so that you might have a case where there are channels that are locked in a blocked configuration, and as long as the environment of the cell is acidic, those channels will not be available to conduct. If calcium entry via those channels is causing myocardial damage, it is very likely that this will be useful. In terms of oxygen though and the charge of the membrane, I don’t have any comments about that.
Dr. Lueebesir Would you have any data with respect to diltiazem on this issue?
Dr. Kassr No, I don’t. I would suspect that it is charged and I suspect that it might be similar, although it is a different receptor, and so, the access to that receptor will be different. To really understand diltiazem, someone should do these kinds of experiments and systematically determine where that receptor is and how does the drug get to it.
Dr. Lueehesi: You might suspect a similar conforma- tional change even though it is a different receptor?
Dr. Kassr Maybe less dramatic because the pK, of diltiazem is lower.
Dr. sdrwartf (Cincinnati, Ohio): If I may follow up a question about verapamil: You have done verapamil which is also charged at a physiological pH, is it not? What are the results with verapamil?
Dr. Kess: I have never looked at the influence of pH on the onset of verapamil. When we first did our work 5 or 6 years ago with nisoldipine, the only charged drugs we
THE AMERICAN JOURNAL OF CARDIOLOGY NOVEMBER 7,1989 41 I

could get our hands on were nicardipine, which is also a dihydropyridine and verapamil, which is not. The devel- opment of block by verapamil is similar to that with the charged dihydropyridine. In other words, channel open- ings appear to be important in the development of block, whereas they are not important for neutral dihydropyri- dines. What is the pK of verapamil? Do you know?
Mr. Burges (Sandwich, England): It is almost the same as amlodipine.
Dr. Kassr You could do the same experiments. But again’for verapamil, from Trautwein’s work, the receptor for verapamil is accessible from inside the cell.
b. Sehwartzr So the long 200-second recovery would not occur but would be much faster with verapamil?
Dr. Kassr It is faster. Dr. sehwarh: And it is faster with diltiazem. So this
is more evidence that the dihydropyridine receptors are different in location.
R. Gm (I-, Audia): A question about the chemistry: Isn’t amlodipine a drug with a chiial center?
Dr. Kau: Yes. R. w So the whole electrophysiology and
pharmacokinetics is a little bit in danger I think. Did you work with a racemate or a pure enantiomer?
Dr. Kar: Well, I have been trying to get enantiomers, but I haven’t managed to get any.
Dr. Gkumann: I ask thii because we know that in some cases, the enantiomers can differ significantly in many aspects.
Mr. Burges: We will be showing data a little bit later demonstrating a very large difference between the 2 en- antiomers.
Dr. Van Breemen (Miami, Rorida): Mr. Burges men- tioned that the association rate was slow because of a direct, slow association rate with the receptor, but in your last model, it could be that lateral diffusion through the lipid has slowed down. So, do you have to neutralize it in order to put it back in the lipid for it to dissociate?
R. Kau: I agree with that picture. I tend to think that it is really a question of lateral diffusion, and that charges on the drug restricted the molecule somehow. I don’t have a good biophysical answer to that. I haven’t tried to figure out how much the diffusion would be slowed, but I think even the charged drug is in the lipid. If you believe Her- bette’s data, even the charged drug is sticking in with its polar head sticking out. I think we have some data that is at least supportive of that picture. So I don’t think it’s a question of dissolving in the lipid, but I think it’s a matter of being able to move more freely if it’s neutral rather than charged.
Dr. Van Breamen: But it is coming off. That is very interesting. If you have it in the charged form, all inside, why doesn’t it come off at all?
Dr. Kassr That to me right now is one of the most
interesting aspects of the drug. The direction that we are looking in is actually fairly biophysical so I don’t want to bore you with it, but there are pictures of how calcium channels select for calcium over different kinds of ions where the channel is thought of as a pore, a protein pore, that binds ions in 2 different sites within the pore. We think that somehow the charge carrier itself, by binding to those internal sites, interacts indirectly with the drug- bound dihydropyridine receptor, and somehow the charged drug is causing a very stable state of the channel, where some ions can’t get through. It looks like other ions can even when the drug is charged. We are looking into that, but we have a long way to go. I think it is fascinating. It is going to tell us a lot about the channel.
Dr. Marshal (Naw York, New York): L-channels, are they all over the place? Are they in neurons or are they in different glands? The follow up to that: Because of the rate dependency, can we look at the smooth onset of action of this compound as having a number of different actions rather than just restricting it to, say, vascular smooth muscle?
Dr. Kassr In almost all tissue, one can show that there is a wide range of calcium channel types and the “L” type is just one kind. At the moment, the kinds of dihydropyri- dines that are available are more specific for the L-type channels. These channels are characteristic of having slowly inactivating pores. The key differential between the various channel types are individual conductances of single channels, the voltage dependencies, where the channels open and where they are inactivate and how fast they inactivate. L-channels inactive the slowest, and they open at more depolarized voltages than others. T-chan- nels inactivate the quickest, and they open at the most negative voltages. Almost all cells have all of these chan- nels, but the distribution and densities differ. Ventricular cells, e.g., have mostly L-type channels although they have a low density of T-channels. The physiological role of channel types differs from cell to cell; in ventricular cells because of long-lasting calcium entry, L-channels are associated mostly with the filling of calcium ions crossing the cell and filling internal stores. T-channels might be related to the release of calcium from internal stores that are somehow coupled to E-C coupling. In neuronal tissue, it appears that neither of these two types of channels is important for neurotransmission; another kind of channel, an N-type channel, might be more im- portant. I think it is a rich field. We are going to learn more and more about the molecular differences among channel types, and I suspect there is a lot of pharmacolo- gy to be done to develop specific probes for the different kinds of channels that might affect function differently in different cells.
Dr. !5chwartzr What we have then, is a drug with a large volume of distribution, a long half-life, long recov- ery, and certainly is pH-dependent.
42 1 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 64

![Development and Validation of Amlodipine Impurities in Amlodipine … · 2016-12-28 · tion of amlodipine alone or in combination with other drugs using HPLC, HPTLC, and LC-MS [2]-[13]](https://img.pdfslide.net/doc/110x75/5e358bf42f46e7726953fdf2/development-and-validation-of-amlodipine-impurities-in-amlodipine-2016-12-28-tion.jpg)