Embed Size (px)
DESCRIPTION
Cervical Spine Workshop. Chris Dillon, MD Regions Emergency Medicine Residency Program. Why is this important?. Cervical spine injuries are both common and potentially devastating. Incidence (USA) 7,000 to 10,000 patients with cervical spine injuries who present for treatment annually. - PowerPoint PPT Presentation
Citation preview

Cervical Spine WorkshopCervical Spine Workshop
Chris Dillon, MDChris Dillon, MD
Regions Emergency Medicine Regions Emergency Medicine Residency ProgramResidency Program

Why is this important?Why is this important?
• Cervical spine injuries are both Cervical spine injuries are both common and potentially devastating.common and potentially devastating.
• IncidenceIncidence(USA)(USA)– 7,000 to 10,000 patients with cervical 7,000 to 10,000 patients with cervical
spine injuries who present for treatment spine injuries who present for treatment annually. annually.
• An estimated 5,000 additional patients An estimated 5,000 additional patients with cervical spine injuries die at the with cervical spine injuries die at the scene of the accident. scene of the accident.
• Half of cervical spine injuries are Half of cervical spine injuries are associated with spinal cord injury. associated with spinal cord injury.
• Consequences of neck injuries range Consequences of neck injuries range from simple neck pain, to quadriplegia, from simple neck pain, to quadriplegia, or even deathor even death
• Spinal cord injury occurs at the time of Spinal cord injury occurs at the time of trauma in 85% of patients and as a trauma in 85% of patients and as a late complication in 15%. late complication in 15%.
• Delayed recognition of an injury or Delayed recognition of an injury or improper stabilization of the cervical improper stabilization of the cervical spine may lead to irreversible spinal spine may lead to irreversible spinal cord injury and permanent neurologic cord injury and permanent neurologic damage.damage.

Who and whyWho and why
• Spinal cord injury most Spinal cord injury most often occurs in teenagers often occurs in teenagers and young adults. and young adults.
• Mean age 30.7, most Mean age 30.7, most commonly occurs at age commonly occurs at age 1919
• 82% males82% males
• motor vehicle accident motor vehicle accident (50%)(50%)
• falls (25%)falls (25%)
• sports injuries (10%).sports injuries (10%).

CostCost
• Direct costs for the first year after Direct costs for the first year after injuryinjury
• High of $417,067 for ventilator High of $417,067 for ventilator dependent quadriplegics patients to dependent quadriplegics patients to a low of $122,914 in the group with a low of $122,914 in the group with near normal neurologic function. near normal neurologic function.
• Indirect costs often greatly exceed Indirect costs often greatly exceed the direct costs. the direct costs.

We see these patients every We see these patients every dayday
• Due to high morbidity Due to high morbidity and mortality of injuriesand mortality of injuries
• Regions Hospital EMS Regions Hospital EMS GuidelinesGuidelines
• ““Backboard patient with Backboard patient with C-collar if patient C-collar if patient complains of head, neck, complains of head, neck, or back pain, or if or back pain, or if suggested by mechanism suggested by mechanism of injury, or if history is of injury, or if history is unreliable due to unreliable due to unconsciousness or unconsciousness or altered mental status.”altered mental status.”

Anatomy and types of injuryAnatomy and types of injury

Upper Cervical Spine Upper Cervical Spine InjuriesInjuries• Most common injury is Most common injury is
flexion.flexion.• Fracture of odontoid process.Fracture of odontoid process.• Extension injuries may occur, Extension injuries may occur,
but are rare.but are rare.• Rotation-rare, possible Rotation-rare, possible
unilateral facet joint unilateral facet joint dislocation.dislocation.
• Axial loading-fracture of Axial loading-fracture of thinner parts of atlas thinner parts of atlas anteriorly and posteriorlyanteriorly and posteriorly
• Neurologic deficit is rare Neurologic deficit is rare because of size of vertebral because of size of vertebral foramen.foramen.

• The atlas articulates with the The atlas articulates with the occipital condyle superiorly and the occipital condyle superiorly and the axis inferiorly. Atlanto-occipital axis inferiorly. Atlanto-occipital articulation is important in the flexion articulation is important in the flexion and extension of the neck. and extension of the neck.
• Atlas-axis articulation is important in Atlas-axis articulation is important in the lateral rotation of the neck. the lateral rotation of the neck.

Lower Cervical Spine InjuriesLower Cervical Spine Injuries C3-C7 C3-C7• Spinal Canal less spaciousSpinal Canal less spacious
• Injuries associated with Injuries associated with forces applied to spineforces applied to spine– Flexion-Dislocated facets Flexion-Dislocated facets
and fracture.and fracture.– Extension-Damage to Extension-Damage to
anterior structures and anterior structures and compression of posterior compression of posterior structures.structures.
– Facet joints at 45º-lateral Facet joints at 45º-lateral rotation is limited, but rotation is limited, but injuries may still occur.injuries may still occur.
– Axial loading-combined with Axial loading-combined with flexion injury.flexion injury.

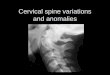
Normal Anatomy-C4Normal Anatomy-C4
• Typical cervical Typical cervical vertebra of C3 - C7.vertebra of C3 - C7.
• Vertebral body is equal Vertebral body is equal in height anteriorly and in height anteriorly and posteriorly.posteriorly.
• Vertebra articulates Vertebra articulates with the next vertebra with the next vertebra at the body and the at the body and the articular processes. articular processes.
• Vertebral artery passes Vertebral artery passes through the transverse through the transverse foramen.foramen.

StabilityStability
The determination of whether a given The determination of whether a given injury is stable is extremely injury is stable is extremely important in the initial evaluation of important in the initial evaluation of cervical spine trauma. The stability cervical spine trauma. The stability of the cervical spine is provided by of the cervical spine is provided by the two vertical columns. the two vertical columns.
Anterior column consists of the Anterior column consists of the vertebral bodies, the disc spaces, vertebral bodies, the disc spaces, the anterior and posterior the anterior and posterior longitudinal ligaments and annulus longitudinal ligaments and annulus fibrosus.fibrosus.
Posterior column consists of the Posterior column consists of the pedicles, facets and apophyseal pedicles, facets and apophyseal joints, laminar spinous processes joints, laminar spinous processes and the posterior ligament and the posterior ligament complex. complex.
Generally speaking, if one of the two Generally speaking, if one of the two columns is intact, the injury is columns is intact, the injury is stable, if both columns are stable, if both columns are disrupted, the injury is unstable. disrupted, the injury is unstable.

Plain filmsPlain films
• Plain films provide the quickest way to Plain films provide the quickest way to survey the cervical spinesurvey the cervical spine
• An adequate spine series includes three An adequate spine series includes three views:views:– true lateral view (which must include all seven.true lateral view (which must include all seven.– cervical vertebrae as well as the C7-T1 cervical vertebrae as well as the C7-T1
junction)junction)– AP view.AP view.– open-mouth odontoid view. open-mouth odontoid view.

Lateral ViewLateral View
• The single most important radiographic examination of the The single most important radiographic examination of the acutely injured cervical spine is the horizontal-beam lateral acutely injured cervical spine is the horizontal-beam lateral radiograph that is obtained before patient is moved. This radiograph that is obtained before patient is moved. This film should be obtained and examined before any other film should be obtained and examined before any other films are taken. All 7 cervical vertebrae and C7-T1 junction films are taken. All 7 cervical vertebrae and C7-T1 junction must be visualized because the cervicothoracic junction is a must be visualized because the cervicothoracic junction is a common place for traumatic injury. common place for traumatic injury.
Visualization of C7-T1 may be limited by the amount of soft Visualization of C7-T1 may be limited by the amount of soft tissue in the shoulder region and can be enhanced by: tissue in the shoulder region and can be enhanced by: 1. traction on arms if no arm injury is present, or, 1. traction on arms if no arm injury is present, or, 2. swimmer's view (taken with one arm extended over the 2. swimmer's view (taken with one arm extended over the head). head).


Lateral viewLateral view

AP and Open-Mouth ViewsAP and Open-Mouth Views
• The complete radiographic examination includes AP The complete radiographic examination includes AP and open-mouth views.and open-mouth views.If there are no obvious fractures or dislocations on the If there are no obvious fractures or dislocations on the lateral view and the patient's condition permits, then lateral view and the patient's condition permits, then proceed with the AP and the open-mouth views. proceed with the AP and the open-mouth views.
It is important to obtain technically adequate films. It is important to obtain technically adequate films. The most frequent cause of overlooked injury is an The most frequent cause of overlooked injury is an inadequate film series. Patient should be maintained inadequate film series. Patient should be maintained in cervical immobilization, and plain films should be in cervical immobilization, and plain films should be repeated or CT scans obtained until all vertebrae are repeated or CT scans obtained until all vertebrae are clearly visible. clearly visible.
The AP view and Odontoid view are obtained as The AP view and Odontoid view are obtained as follows follows

AP/OdontoidAP/Odontoid

APAP

OdontoidOdontoid

CTCT
• Up to 20 % of fractures are missed on conventional radiographs. CT can help.Up to 20 % of fractures are missed on conventional radiographs. CT can help.
CT scan is not mandatory for every patient with cervical spine injury. Most injuries CT scan is not mandatory for every patient with cervical spine injury. Most injuries can be diagnosed by plain films. However, if there is a question on the radiograph, CT can be diagnosed by plain films. However, if there is a question on the radiograph, CT of the cervical spine should be obtained. CT scan are particularly useful in fractures of the cervical spine should be obtained. CT scan are particularly useful in fractures that result in neurologic deficit and in fractures of the posterior elements of the that result in neurologic deficit and in fractures of the posterior elements of the cervical canal (e.g. Jefferson's fracture) because the axial display eliminates the cervical canal (e.g. Jefferson's fracture) because the axial display eliminates the superimposition of bony structures.superimposition of bony structures.
The The advantagesadvantages of CT are: of CT are: 1. CT is excellent for characterizing fractures and identifying osseous compromise of 1. CT is excellent for characterizing fractures and identifying osseous compromise of the vertebral canal because of the absence of superimposition from the transverse the vertebral canal because of the absence of superimposition from the transverse view. The higher contrast resolution of CT also provides improved visualization of view. The higher contrast resolution of CT also provides improved visualization of subtle fractures.subtle fractures.2. CT provides patient comfort by being able to reconstruct images in the axial, 2. CT provides patient comfort by being able to reconstruct images in the axial, sagittal, coronal, and oblique planes from one patient positioning.sagittal, coronal, and oblique planes from one patient positioning.
TheThe limitations limitations of CT are: of CT are: 1. difficult to identify those fractures oriented in axial plane (e.g. dens fractures).1. difficult to identify those fractures oriented in axial plane (e.g. dens fractures).2. unable to show ligamentous injuries. 2. unable to show ligamentous injuries. 3. relatively high costs. 3. relatively high costs.
Sagittal, coronal, 3D reconstructions are possible.Sagittal, coronal, 3D reconstructions are possible.

CTCT

MRIMRI
• MRI is MRI is indicatedindicated in cervical fractures that have spinal canal involvement, in cervical fractures that have spinal canal involvement, clinical neurologic deficits or ligamentous injuries. MRI provides the best clinical neurologic deficits or ligamentous injuries. MRI provides the best visualization of the soft tissues, including ligaments, intervertebral disks, spinal visualization of the soft tissues, including ligaments, intervertebral disks, spinal cord, and epidural hematomas.cord, and epidural hematomas.
TheThe advantages advantages of MRI are: of MRI are: 1. excellent soft tissue constrast, making it the study of choice for spinal cord 1. excellent soft tissue constrast, making it the study of choice for spinal cord survey, hematoma, and ligamentous injuries.survey, hematoma, and ligamentous injuries.2. provides good general overview because of its ability to show information in 2. provides good general overview because of its ability to show information in different planes (e.g. sagital, coronal, etc.).different planes (e.g. sagital, coronal, etc.).3. ability to demostrate vertebral arteries, which is useful in evaluating 3. ability to demostrate vertebral arteries, which is useful in evaluating fractures involving the course of the vertebral arteries.fractures involving the course of the vertebral arteries.4. no ionizing radiation.4. no ionizing radiation.
TheThe disadvantages disadvantages of MRI are: of MRI are:1. loss of bony details.1. loss of bony details.2. relatively high cost. 2. relatively high cost.
Here is an example of a MRI image of the cervical spine demostrating a Here is an example of a MRI image of the cervical spine demostrating a ligamentous injury. Notice that the spinal cord is also very well delinated. A ligamentous injury. Notice that the spinal cord is also very well delinated. A dens fracture is not obvious on the lateral film, but is clearly revealed on MRI.dens fracture is not obvious on the lateral film, but is clearly revealed on MRI.


Evaluation of imagesEvaluation of images
• A adequacyA adequacy
• A alignmentA alignment
• B boneB bone
• C cartilageC cartilage
• D discD disc
• S soft tissueS soft tissue

Lateral ViewLateral View
• The lateral view is the most important film of The lateral view is the most important film of all. all.
• Interpretation follows the mnemonic AABCDS. Interpretation follows the mnemonic AABCDS.
• First, is the film First, is the film AdequateAdequate? ?
• An adequate film should include all 7 An adequate film should include all 7 vertebrae and C7-T1 junction.vertebrae and C7-T1 junction.
• It should also have correct density and show It should also have correct density and show the soft tissue and bony structures well.the soft tissue and bony structures well.


AlignmentAlignment
• Assess four parallel lines. These are: Assess four parallel lines. These are:
1. Anterior vertebral line (anterior margin of vertebral 1. Anterior vertebral line (anterior margin of vertebral bodies) bodies) 2. Posterior vertebral line (posterior margin of vertebral 2. Posterior vertebral line (posterior margin of vertebral bodies)bodies)3. Spinolaminar line (posterior margin of spinal canal)3. Spinolaminar line (posterior margin of spinal canal)4. Posterior spinous line (tips of the spinous processes) 4. Posterior spinous line (tips of the spinous processes)
These lines should follow a slightly lordotic curve, smooth These lines should follow a slightly lordotic curve, smooth and without step-offs. Any malalignment should be and without step-offs. Any malalignment should be considered evidence of ligmentous injury or occult fracture, considered evidence of ligmentous injury or occult fracture, and cervical spine immobilization should be maintained and cervical spine immobilization should be maintained until a definitive diagnosis is made.until a definitive diagnosis is made.

AlignmentAlignment

Bony LandmarksBony Landmarks
• Trace the unbroken outline of each vertebrae Trace the unbroken outline of each vertebrae (including Odontoid on C2). The vertebral (including Odontoid on C2). The vertebral bodies should line up with a gentle arch (normal bodies should line up with a gentle arch (normal cervical lordosis) using the anterior and cervical lordosis) using the anterior and posterior marginal lines on the lateral view. posterior marginal lines on the lateral view. Each body should be rectangular in shape and Each body should be rectangular in shape and roughly equal in size although some variability roughly equal in size although some variability is allowed (overall height of C4 and C5 may be is allowed (overall height of C4 and C5 may be slightly less than C3 and C6) . The anterior slightly less than C3 and C6) . The anterior height should roughly equal posterior height height should roughly equal posterior height (posterior may normally be slightly greater, up (posterior may normally be slightly greater, up to 3mm).to 3mm).

Bony LandmarksBony Landmarks

Bony LandmarksBony Landmarks
• PediclesPedicles project posteriorly to support the articular pillars, project posteriorly to support the articular pillars, forming the superior and inferior margins of the intervertebral forming the superior and inferior margins of the intervertebral foramen. The left and right pedicels should superimpose on true foramen. The left and right pedicels should superimpose on true lateral views. If fracture is suspected, get oblique views or CT. lateral views. If fracture is suspected, get oblique views or CT.
• FacetsFacets: the articular pillars are osseous masses connected to the : the articular pillars are osseous masses connected to the posterolateral aspect of vertebral bodies via the pedicles. The posterolateral aspect of vertebral bodies via the pedicles. The facet joints are formed between each lateral mass. On the lateral facet joints are formed between each lateral mass. On the lateral view, the lateral masses appear as rhomboid-shaped structures view, the lateral masses appear as rhomboid-shaped structures projecting downward and posterior. "Double cortical lines" results projecting downward and posterior. "Double cortical lines" results from slight obliquity from lateral projection. The distance of the from slight obliquity from lateral projection. The distance of the joint space should be roughly equal at all levels. joint space should be roughly equal at all levels.
• LaminaLamina: the posterior elements are seen poorly on the lateral : the posterior elements are seen poorly on the lateral film. They are best demostrated by CT.film. They are best demostrated by CT.
• Spinous process:Spinous process: generally get progressively larger in the lower generally get progressively larger in the lower vertebral bodies. The C7 cervical spine is usually the largest.vertebral bodies. The C7 cervical spine is usually the largest.

Bony LandmarksBony Landmarks

Cartilaginous SpaceCartilaginous Space
• The Predental space (distance from dens to The Predental space (distance from dens to C1 body) should not measure more than 3 C1 body) should not measure more than 3 mm in adults and 5mm in children. If the mm in adults and 5mm in children. If the space is increased, a fracture of the space is increased, a fracture of the Odontoid process or disruption of the Odontoid process or disruption of the transverse ligament is likely. If fracture is transverse ligament is likely. If fracture is suspected, CT should be obtained. If suspected, CT should be obtained. If ligamentous disruption is suspected, a MRI ligamentous disruption is suspected, a MRI should be obtained.should be obtained.
• Predental space should be:Predental space should be:– < 3 mm in adults.< 3 mm in adults.

Predental spacePredental space

Disc SpacesDisc Spaces
• Disc spaces should be roughly equal in Disc spaces should be roughly equal in height at anterior and posterior margins. height at anterior and posterior margins.
• Disc spaces should be symmetric. Disc spaces should be symmetric.
• Disc space height should also be Disc space height should also be approximately equal at all levels. In older approximately equal at all levels. In older patients, degenative diseases may lead patients, degenative diseases may lead to spurring and loss of disc height.to spurring and loss of disc height.

Disc SpacesDisc Spaces

Soft Tissue SpaceSoft Tissue Space
• Preverteral soft tissue swelling is important in trauma because it Preverteral soft tissue swelling is important in trauma because it is usually due to hematoma formation secondary to occult is usually due to hematoma formation secondary to occult fractures. Unfortunately, it is extremely variable and nonspecific. fractures. Unfortunately, it is extremely variable and nonspecific.
Maximum allowable thickness of preverteral spaces is as follows: Maximum allowable thickness of preverteral spaces is as follows:
Nasopharyngeal space (C1) - 10 mm (adult)Nasopharyngeal space (C1) - 10 mm (adult)Retropharyngeal space (C2-C4) - 5-7 mmRetropharyngeal space (C2-C4) - 5-7 mmRetrotracheal space (C5-C7) - 14 mm (children), 22 mm (adults). Retrotracheal space (C5-C7) - 14 mm (children), 22 mm (adults). Soft tissue swelling in symptomatic patients should be Soft tissue swelling in symptomatic patients should be considered an indication for further radiographic evaluation. If considered an indication for further radiographic evaluation. If the space between the lower anterior border of C3 and the the space between the lower anterior border of C3 and the pharyngeal air shadow is > 7 mm, one should suspect pharyngeal air shadow is > 7 mm, one should suspect retropharyngeal swelling (e.g. hemorrhage). This is often a useful retropharyngeal swelling (e.g. hemorrhage). This is often a useful indirect sign of a C2 fracture. Space between lower cervical indirect sign of a C2 fracture. Space between lower cervical vertebrae and trachea should be < 1 vertebral body. vertebrae and trachea should be < 1 vertebral body.

Soft Tissue SpaceSoft Tissue Space

AP ViewAP View
• Alignment on the A-P view should be evaluated Alignment on the A-P view should be evaluated using the edges of the vertebral bodies and using the edges of the vertebral bodies and articular pillars.articular pillars.
The height of the cervical vertebral bodies should The height of the cervical vertebral bodies should be approximately equal on the AP view.be approximately equal on the AP view.
The height of each joint space should be roughly The height of each joint space should be roughly equal at all levels.equal at all levels.
Spinous process should be in midline and in good Spinous process should be in midline and in good alignment. If one of the spinous process is displaced alignment. If one of the spinous process is displaced to one side, a facet dislocation should be suspected.to one side, a facet dislocation should be suspected.

APAP

Odontoid ViewOdontoid View
• Adequate?Adequate?• An adequate film should include the entire odontoid and the lateral borders of An adequate film should include the entire odontoid and the lateral borders of
C1-C2. C1-C2.
• Alignment?Alignment?• Occipital condyles should line up with the lateral masses and superior articular Occipital condyles should line up with the lateral masses and superior articular
facet of C1.facet of C1.
The distance from the dens to the lateral masses of C1 should be equal The distance from the dens to the lateral masses of C1 should be equal bilaterally Any asymmetry is suggestive of a fracture of C1 or C2 or rotational bilaterally Any asymmetry is suggestive of a fracture of C1 or C2 or rotational abnormality. It may also be caused by tilting of the head, so if the vertebrae is abnormality. It may also be caused by tilting of the head, so if the vertebrae is shifted in on one side, then it should be shifted out on the other side. shifted in on one side, then it should be shifted out on the other side.
The tips of lateral mass of C1 should line up with the lateral margins of the The tips of lateral mass of C1 should line up with the lateral margins of the superior articular facet of C2. If not, a fracture of C1 should be suspected.superior articular facet of C2. If not, a fracture of C1 should be suspected.
• Bony MarginsBony Margins..the Odontoid should have uninterrupted cortical margins blending with the the Odontoid should have uninterrupted cortical margins blending with the body of C2. body of C2.

Odontoid ViewOdontoid View

Mechanism of InjuryMechanism of Injury
• The cervical spine may be subjected The cervical spine may be subjected to forces of different directions and to forces of different directions and magnitude. The most common magnitude. The most common mechanisms of cervical spine injury mechanisms of cervical spine injury are hyperflexion, hyperextension and are hyperflexion, hyperextension and compression. compression.

HyperflexionHyperflexion
• Excessive flexion of Excessive flexion of the neck in the sagital the neck in the sagital plane. It results in plane. It results in disruption of the disruption of the posterior ligament. A posterior ligament. A common cause of common cause of hyperflexion injury is hyperflexion injury is diving in shallow diving in shallow water, which may water, which may result in flexion tear result in flexion tear drop fracture.drop fracture.

HyperextensionHyperextension
• Excessive extension Excessive extension of the neck in the of the neck in the sagital plane. A sagital plane. A common cause of common cause of hyperextension hyperextension injury is hitting the injury is hitting the dash board in MVA, dash board in MVA, which may result in which may result in Hangman's fracture.Hangman's fracture.

Axial compressionAxial compression
• Force applied Force applied directly over the directly over the vertex in the caudal vertex in the caudal direction. This direction. This compression force compression force "like smashing a "like smashing a cracker" may result cracker" may result in Jefferson fracture, in Jefferson fracture, a bursting fracture a bursting fracture on the atlas.on the atlas.

Atlanto-occipital Atlanto-occipital DisassociationDisassociation
• DescriptionDescription: Disruption of the atlanto-occipital junction involving : Disruption of the atlanto-occipital junction involving the atlanto-occipital articulations. the atlanto-occipital articulations.
MechanismMechanism: Hyperflexion or hyperextension.: Hyperflexion or hyperextension.
Radiographic featuresRadiographic features: :
1. Malposition of occipital condyles in relation to the superior 1. Malposition of occipital condyles in relation to the superior articulating facets of the atlas.articulating facets of the atlas.2. Increased ratio of Basion - spinolaminar line of C1 to Opisthion - 2. Increased ratio of Basion - spinolaminar line of C1 to Opisthion - posterior cortex of C1 anterior arch for incomplete anterior posterior cortex of C1 anterior arch for incomplete anterior atlanto-occipital dislocation. (Refer to atlanto-occipital alignment atlanto-occipital dislocation. (Refer to atlanto-occipital alignment for further explaination).for further explaination).3. Cervicocranial prevertebral soft tissue swelling. 3. Cervicocranial prevertebral soft tissue swelling.
StabilityStability: unstable : unstable

Atlanto-occipital Atlanto-occipital DisassociationDisassociation

Jefferson FractureJefferson Fracture
• DescriptionDescription: compression fracture of the bony ring of : compression fracture of the bony ring of vertebra C1, characterized by lateral masses splitting and vertebra C1, characterized by lateral masses splitting and transverse ligament tear.transverse ligament tear.
MechanismMechanism: axial blow to the vertex of the head (e.g. : axial blow to the vertex of the head (e.g. diving injury).diving injury).
Radiographic features:Radiographic features: the key radiographic view is the the key radiographic view is the AP open mouth, which shows displacement of the lateral AP open mouth, which shows displacement of the lateral masses of vertebrae C1 beyond the margins of the body of masses of vertebrae C1 beyond the margins of the body of vertebra C2. A lateral displacement of >2 mm or unilateral vertebra C2. A lateral displacement of >2 mm or unilateral displacement may be indicative of a C1 fracture. CT is displacement may be indicative of a C1 fracture. CT is required to define the extent of fracture and to detect required to define the extent of fracture and to detect fragments in the spinal canal. fragments in the spinal canal.
StabilityStability: unstable : unstable

Jefferson FractureJefferson Fracture

Jefferson FractureJefferson Fracture

Odontoid FracturesOdontoid Fractures
• Radiographic featuresRadiographic features: fracture is best : fracture is best seen on lateral view. seen on lateral view. Fracture of the odontoid should be suspected Fracture of the odontoid should be suspected if there is an anterior tilt of odontoid on if there is an anterior tilt of odontoid on lateral view. The lucent fracture line may be lateral view. The lucent fracture line may be better delineated by plain film tomogram or better delineated by plain film tomogram or CT. Sometimes the only sign of fracture may CT. Sometimes the only sign of fracture may be just prevertebral soft tissue swelling. be just prevertebral soft tissue swelling. Odontoid fractures are generally divided into Odontoid fractures are generally divided into three types.three types.

Dens Fracture Type IDens Fracture Type I
• Type I Odontoid Type I Odontoid fracturefracture: fracture : fracture in superior tip of in superior tip of the odontoid.the odontoid.
• Potentially Potentially unstable. unstable.
• Rare fracture. Rare fracture.

Dens Fracture Type IIDens Fracture Type II
• Type II Odontoid Type II Odontoid FractureFracture: fracture : fracture at base of at base of odontoid. odontoid.
• most common type most common type of odontoid of odontoid fracture. fracture.
• unstable fracture.unstable fracture.

Dens Fracture Type IIDens Fracture Type II

Dens Fracture Type IIIDens Fracture Type III
• Type III Odontoid Type III Odontoid FractureFracture: fracture : fracture through base of through base of odontoid into body odontoid into body of axis.of axis.
• It has the best It has the best prognosis.prognosis.

Dens Fracture Type IIIDens Fracture Type III

Hangman's FractureHangman's Fracture
• DescriptionDescription: fractures through the pars interaticularis of : fractures through the pars interaticularis of the axis resulting from hyperextension and distraction.the axis resulting from hyperextension and distraction.
MechanismMechanism: hyperextension (e.g. hanging, chin hits : hyperextension (e.g. hanging, chin hits dashboard in MVA). dashboard in MVA).
Radiographic featuresRadiographic features: (best seen on lateral view) : (best seen on lateral view)
1. Prevertebral soft tissue swelling.1. Prevertebral soft tissue swelling.2. Avulsion of anterior inferior corner of C2 associated with 2. Avulsion of anterior inferior corner of C2 associated with rupture of the anterior longitudinal ligament. rupture of the anterior longitudinal ligament. 3. Anterior dislocation of the C2 vertebral body. 3. Anterior dislocation of the C2 vertebral body. 4. Bilateral C2 pars interarticularis fractures. 4. Bilateral C2 pars interarticularis fractures.
StabilityStability: unstable : unstable

Hangman's FractureHangman's Fracture

Flexion Teardrop FractureFlexion Teardrop Fracture
• DescriptionDescription: posterior ligament disruption and anterior : posterior ligament disruption and anterior compression fracture of the vertebral body which results from a compression fracture of the vertebral body which results from a severe flexion injury.severe flexion injury.
MechanismMechanism: hyperflexion and compression (e.g. diving into : hyperflexion and compression (e.g. diving into shallow water)shallow water)
Radiographic featuresRadiographic features: (best seen on lateral view): (best seen on lateral view)
1. Prevertebral swelling associated with anterior longitudinal 1. Prevertebral swelling associated with anterior longitudinal ligament tear.ligament tear.2. Teardrop fragment from anterior vertebral body avulsion 2. Teardrop fragment from anterior vertebral body avulsion fracture.fracture.3. Posterior vertebral body subluxation into the spinal canal.3. Posterior vertebral body subluxation into the spinal canal.4. Spinal cord compression from vertebral body displacement.4. Spinal cord compression from vertebral body displacement.5. Fracture of the spinous process.5. Fracture of the spinous process.
StabilityStability: unstable : unstable

Flexion Teardrop Flexion Teardrop FractureFracture

Flexion Teardrop Flexion Teardrop FractureFracture

Bilateral Facet Bilateral Facet DislocationDislocation• DescriptionDescription: complete anterior dislocation of the vertebral : complete anterior dislocation of the vertebral
body resulting from extreme hyperflexion injury. It is body resulting from extreme hyperflexion injury. It is associated with a very high risk of cord damage.associated with a very high risk of cord damage.
MechanismMechanism: extreme flexion of head and neck without : extreme flexion of head and neck without axial compression.axial compression.
Radiographic featuresRadiographic features: (best seen on lateral view): (best seen on lateral view)
1. Complete anterior dislocation of affected vertebral body 1. Complete anterior dislocation of affected vertebral body by half or more of the vertebral body AP diameter.by half or more of the vertebral body AP diameter.2. Disruption of the posterior ligament complex and the 2. Disruption of the posterior ligament complex and the anterior longitudinal ligament.anterior longitudinal ligament.3. "Bow tie" or " bat wing" appearance of the locked facets.3. "Bow tie" or " bat wing" appearance of the locked facets.
StabilityStability: unstable: unstable

Bilateral Facet Bilateral Facet DislocationDislocation

Unilateral Facet Unilateral Facet DislocationDislocation• DescriptionDescription: facet joint dislocation and rupture of the : facet joint dislocation and rupture of the
apophyseal joint ligaments resulting from rotatory injury of the apophyseal joint ligaments resulting from rotatory injury of the cervical vertebrae. cervical vertebrae.
MechanismMechanism: simultaneous flexion and rotation: simultaneous flexion and rotation
Radiographic featuresRadiographic features: (best seen on lateral or oblique views): (best seen on lateral or oblique views)
1. Anterior dislocation of affected vertebral body by less than half 1. Anterior dislocation of affected vertebral body by less than half of the vertebral body AP diameter. of the vertebral body AP diameter. 2. Discordant rotation above and below involved level.2. Discordant rotation above and below involved level.3. Facet within intervertebral foramen on oblique view.3. Facet within intervertebral foramen on oblique view.4. Widening of the disk space.4. Widening of the disk space.5. "Bow tie" or "bat wing" appearance of the overriding locked 5. "Bow tie" or "bat wing" appearance of the overriding locked facets.facets.
StabilityStability: stable: stable

Unilateral Facet Unilateral Facet DislocationDislocation

Anterior SubluxationAnterior Subluxation
• Description Description : disruption of the posterior ligamentous complex resulting from : disruption of the posterior ligamentous complex resulting from hyperflexion. It may be difficult to diagnose because muscle spasm may result in hyperflexion. It may be difficult to diagnose because muscle spasm may result in similar findings on the radiograph. Subluxation may be stable initially, but it similar findings on the radiograph. Subluxation may be stable initially, but it associates with 20%-50% delayed instability. Flexion and extension views are helpful associates with 20%-50% delayed instability. Flexion and extension views are helpful in further evaluation. in further evaluation.
MechanismMechanism: hyperflexion of neck: hyperflexion of neck
Radiographic featuresRadiographic features::
1. Loss of normal cervical lordosis.1. Loss of normal cervical lordosis.2. Anterior displacement of the vertebral body.2. Anterior displacement of the vertebral body.3. Fanning of the interspinous distance. 3. Fanning of the interspinous distance.
Radiographic features of unstable injuryRadiographic features of unstable injury::
1. Anterior subluxation of more than 4mm. 1. Anterior subluxation of more than 4mm. 2. Associated compression fracture of more than 25 % of the affected vertebral body.2. Associated compression fracture of more than 25 % of the affected vertebral body.3. Increase or decrease in normal disk space.3. Increase or decrease in normal disk space.4. Fanning of the interspinous distance.4. Fanning of the interspinous distance.

Clay Shoveler's FractureClay Shoveler's Fracture
• DescriptionDescription: fracture of a spinous process C6-T1: fracture of a spinous process C6-T1
MechanismMechanism: powerful hyperflexion, usually combined with : powerful hyperflexion, usually combined with contraction of paraspinous muscles pulling on spinous contraction of paraspinous muscles pulling on spinous processes (e.g. shoveling).processes (e.g. shoveling).
Radiographic featuresRadiographic features: (best seen on lateral view): (best seen on lateral view)
1. Spinous process fracture on lateral view.1. Spinous process fracture on lateral view.2. Ghost sign on AP view (i.e. double spinous process of C6 2. Ghost sign on AP view (i.e. double spinous process of C6 or C7 resulting from displaced fractured spinous process). or C7 resulting from displaced fractured spinous process).
StabilityStability: stable: stable

Clay Shoveler's FractureClay Shoveler's Fracture

Wedge FractureWedge Fracture
• DescriptionDescription: compression fracture resulting : compression fracture resulting from flexion.from flexion.
MechanismMechanism: hyperflexion and compression: hyperflexion and compression
Radiographic featuresRadiographic features: : 1. Buckled anterior cortex. 1. Buckled anterior cortex. 2. Loss of height of anterior vertebral body. 2. Loss of height of anterior vertebral body. 3. Anterosuperior fracture of vertebral body. 3. Anterosuperior fracture of vertebral body.
StabilityStability: stable : stable

Wedge FractureWedge Fracture

Burst FractureBurst Fracture
• DescriptionDescription: fracture of C3-C7 that results : fracture of C3-C7 that results from axial compression. Injury to spinal from axial compression. Injury to spinal cord, secondary to displacement of cord, secondary to displacement of posterior fragments, is common. CT is posterior fragments, is common. CT is required for all patient to evaluate extent of required for all patient to evaluate extent of injury. injury.
MechanismMechanism: axial compression : axial compression
StabilityStability: stable : stable

Burst FractureBurst Fracture

ClassificationClassification
• By stabilityBy stability
• StableStable– Anterior subluxationAnterior subluxation
Unilateral interfacetal dislocationUnilateral interfacetal dislocationSimple wedge fractureSimple wedge fractureBurst fracture, lower cervical spineBurst fracture, lower cervical spineClay Shoveler's fractureClay Shoveler's fracture
• UnstableUnstable– Anterior subluxationAnterior subluxation
Bilateral interfacetal dislocationBilateral interfacetal dislocationFlexion teardrop fractureFlexion teardrop fractureHangman's fractureHangman's fractureJefferson fracture of atlasJefferson fracture of atlas

ManagementManagement
• General PrinciplesGeneral PrinciplesOutcome for the spine trauma patient often depends upon action Outcome for the spine trauma patient often depends upon action taken by the emergency team in the first 6 to 12 hours after taken by the emergency team in the first 6 to 12 hours after injury. The main objective in cervical trauma management is to injury. The main objective in cervical trauma management is to prevent cord injury and to minimize any secondary injuries to prevent cord injury and to minimize any secondary injuries to spinal cord tissue as a result of inadequate immobilization, spinal cord tissue as a result of inadequate immobilization, persistent spinal cord compression, poor blood flow or persistent spinal cord compression, poor blood flow or oxygenation. The goal is to optimize the environment for the oxygenation. The goal is to optimize the environment for the spinal cord to recover as much as possible.spinal cord to recover as much as possible.
• If a cervical fracture or dislocation is found. Orthopedic or If a cervical fracture or dislocation is found. Orthopedic or neurosurgical consultation should be obtained immediately.neurosurgical consultation should be obtained immediately.
• There are three indications for surgical intervention in cervical There are three indications for surgical intervention in cervical spine trauma.spine trauma.– Neurologic deficitNeurologic deficit– Spinal instabilitySpinal instability– Intractable painIntractable pain

ManagementManagement
• Some fractures, such as unilateral facet dislocation, Some fractures, such as unilateral facet dislocation, may required skeletal traction and reduction. may required skeletal traction and reduction. Physicians should perform these procedures with Physicians should perform these procedures with minimum amont of sedation so that the patient can minimum amont of sedation so that the patient can provide instant neurologic feedback.provide instant neurologic feedback.
• High suspicion for cervical fracture should be High suspicion for cervical fracture should be maintained in all trauma situations because there maintained in all trauma situations because there are no signs of neurologic injury in many cervical are no signs of neurologic injury in many cervical fractures. Cervical immobolization is usually fractures. Cervical immobolization is usually achieved by a Philadelphia-type collar or a halo achieved by a Philadelphia-type collar or a halo vest.vest.


Management of Specific Management of Specific FracturesFractures• Jefferson fractureJefferson fracture is treated with halo immobilization for 12 is treated with halo immobilization for 12
weeks, which usually results in primary union of the ring of C1 weeks, which usually results in primary union of the ring of C1 and stability of C1 with respect to C2. Surgical fusion may be and stability of C1 with respect to C2. Surgical fusion may be needed if there is atlantoaxial instability after removal of halo.needed if there is atlantoaxial instability after removal of halo.
• Hangman's fractureHangman's fracture is unstable. It usually heals with halo is unstable. It usually heals with halo immobilization for 12 weeks. Surgical fusion is rarely indicatedimmobilization for 12 weeks. Surgical fusion is rarely indicated
• Odontoid fractureOdontoid fracture::
– Type IType I is rare. It usually does not have any neurologic symptoms. is rare. It usually does not have any neurologic symptoms. It is treated with Philadelphia collar.It is treated with Philadelphia collar.
– Type IIType II is the most difficult type to treat in the halo vest. Even is the most difficult type to treat in the halo vest. Even with proper management, the nonunion rate is still as high as 30-with proper management, the nonunion rate is still as high as 30-60%. If nonunion persists, surgical posterior fusion is indicated.60%. If nonunion persists, surgical posterior fusion is indicated.
– Type IIIType III is treated with halo immobilization. It usually has a high is treated with halo immobilization. It usually has a high rate of union.rate of union.

Management of Specific Management of Specific FracturesFractures• Fractures and dislocations of lower cervical spineFractures and dislocations of lower cervical spine::
• Vertical compression fracturesVertical compression fractures are normally treated are normally treated initially with traction to reduce fragmentation and initially with traction to reduce fragmentation and subsequently with halo vest. They tend to heal well with halo subsequently with halo vest. They tend to heal well with halo immobilizationimmobilization..
• Unilateral facet dislocations Unilateral facet dislocations do fairly well with halo do fairly well with halo immobilization.immobilization.
• Bilateral facet dislocationsBilateral facet dislocations are treated conservatively. are treated conservatively. The facet joints are reduced and immobilized. The posterior The facet joints are reduced and immobilized. The posterior ligament usually heals poorly.ligament usually heals poorly.
• Clay Shoveler's fracturesClay Shoveler's fractures are treated with soft collar for are treated with soft collar for comfort. Prognosis is excellent.comfort. Prognosis is excellent.

Who needs imaging?Who needs imaging?
• Not all trauma patients with a Not all trauma patients with a significant injury need c-spine films. significant injury need c-spine films.

Canadian C-spine RuleCanadian C-spine Rule• Context High levels of variation and inefficiency exist in current clinical practice regarding use of cervical spine (C-spine) radiography in
alert and stable trauma patients.
• Objective To derive a clinical decision rule that is highly sensitive for detecting acute C-spine injury and will allow emergency department (ED) physicians to be more selective in use of radiography in alert and stable trauma patients.
• Design Prospective cohort study conducted from October 1996 to April 1999, in which physicians evaluated patients for 20 standardized clinical findings prior to radiography. In some cases, a second physician performed independent interobserver assessments.
• Setting Ten EDs in large Canadian community and university hospitals.
• Patients Convenience sample of 8924 adults (mean age, 37 years) who presented to the ED with blunt trauma to the head/neck, stable vital signs, and a Glasgow Coma Scale score of 15.
• Main Outcome Measure Clinically important C-spine injury, evaluated by plain radiography, computed tomography, and a structured follow-up telephone interview. The clinical decision rule was derived using the coefficient, logistic regression analysis, and 2 recursive partitioning techniques.
• Results Among the study sample, 151 (1.7%) had important C-spine injury. The resultant model and final Canadian C-Spine Rule comprises 3 main questions: (1) is there any high-risk factor present that mandates radiography (ie, age 65 years, dangerous mechanism, or paresthesias in extremities)? (2) is there any low-risk factor present that allows safe assessment of range of motion (ie, simple rear-end motor vehicle collision, sitting position in ED, ambulatory at any time since injury, delayed onset of neck pain, or absence of midline C-spine tenderness)? and (3) is the patient able to actively rotate neck 45° to the left and right? By cross-validation, this rule had 100% sensitivity (95% confidence interval [CI], 98%-100%) and 42.5% specificity (95% CI, 40%-44%) for identifying 151 clinically important C-spine injuries. The potential radiography ordering rate would be 58.2%.
• Conclusion We have derived the Canadian C-Spine Rule, a highly sensitive decision rule for use of C-spine radiography in alert and stable trauma patients. If prospectively validated in other cohorts, this rule has the potential to significantly reduce practice variation and inefficiency in ED use of C-spine radiography.
JAMA. 2001;286:1841-1848

Canadian C-spine RuleCanadian C-spine Rule
• For patients alert w/GCS=15, stable (SBP>90, RR=10-24):For patients alert w/GCS=15, stable (SBP>90, RR=10-24):
• (1) Any high risk factor that mandates xray?(1) Any high risk factor that mandates xray?• --age>65 y/o or --age>65 y/o or • --dangerous mechanism (fall>5 stairs, axial load to head, mvc>60 mph, rollover, --dangerous mechanism (fall>5 stairs, axial load to head, mvc>60 mph, rollover,
ejection) or ejection) or • --paresthesias in ext--paresthesias in ext• **if yes then xray; if no then #2**if yes then xray; if no then #2
• (2) Any low risk factor that allows safe assessment of ROM(2) Any low risk factor that allows safe assessment of ROM• --simple rear-end mvc or --simple rear-end mvc or • --sitting position in ED or --sitting position in ED or • --ambulatory at any time or --ambulatory at any time or • --delayed onset of neck pain or --delayed onset of neck pain or • --absence of midline c-spine tend--absence of midline c-spine tend• **lf no then xray; lf yes then to #3**lf no then xray; lf yes then to #3
• (3) Able to actively rotate neck 45 degrees left & right?(3) Able to actively rotate neck 45 degrees left & right?• **if no then xray; if yes then no xray**if no then xray; if yes then no xray

NEXUS NEXUS (National Emergency X-ray Utilization (National Emergency X-ray Utilization Study)Study)• Background: Because clinicians fear missing occult cervical-spine injuries, they obtain
cervical radiographs for nearly all patients who present with blunt trauma. Previous research suggests that a set of clinical criteria (decision instrument) can identify patients who have an extremely low probability of injury and who consequently have no need for imaging studies.
• Methods: We conducted a prospective, observational study of such a decision instrument at 21 centers across the United States. The decision instrument required patients to meet five criteria in order to be classified as having a low probability of injury: no midline cervical tenderness, no focal neurologic deficit, normal alertness, no intoxication, and no painful, distracting injury. We examined the performance of the decision instrument in 34,069 patients who underwent radiography of the cervical spine after blunt trauma.
• Results: The decision instrument identified all but 8 of the 818 patients who had cervical-spine injury (sensitivity, 99.0 percent [95 percent confidence interval, 98.0 to 99.6 percent]). The negative predictive value was 99.8 percent (95 percent confidence interval, 99.6 to 100 percent), the specificity was 12.9 percent, and the positive predictive value was 2.7 percent. Only two of the patients classified as unlikely to have an injury according to the decision instrument met the preset definition of a clinically significant injury (sensitivity, 99.6 percent [95 percent confidence interval, 98.6 to 100 percent]; negative predictive value, 99.9 percent [95 percent confidence interval, 99.8 to 100 percent]; specificity, 12.9 percent; positive predictive value, 1.9 percent), and only one of these two patients received surgical treatment. According to the results of assessment with the decision instrument, radiographic imaging could have been avoided in the cases of 4309 (12.6 percent) of the 34,069 evaluated patients.
• Conclusions: A simple decision instrument based on clinical criteria can help physicians to identify reliably the patients who need radiography of the cervical spine after blunt trauma. Application of this instrument could reduce the use of imaging in such patients.
• N Engl J Med 2000;343:94-9.

NEXUSNEXUS
• Radiography is not recommended if a patient meets all of the Radiography is not recommended if a patient meets all of the following criteria:following criteria:
• Absence of tenderness at the posterior midline of the C-spineAbsence of tenderness at the posterior midline of the C-spine
• Absence of a focal neurologic deficitAbsence of a focal neurologic deficit
• Normal level of alertnessNormal level of alertness
• No evidence of intoxicationNo evidence of intoxication
• Absence of clinically apparent pain that might distract the Absence of clinically apparent pain that might distract the patient from the pain of a C-spine injurypatient from the pain of a C-spine injury

ComparisonComparison
• Among the 8283 patients, 169 (2.0 percent) had Among the 8283 patients, 169 (2.0 percent) had clinically important cervical-spine injuries. In 845 (10.2 clinically important cervical-spine injuries. In 845 (10.2 percent) of the patients, physicians did not evaluate percent) of the patients, physicians did not evaluate range of motion as required by the CCR algorithm range of motion as required by the CCR algorithm
• prospective cohort study in nine Canadian emergency prospective cohort study in nine Canadian emergency departments comparing the CCR and NLC as applied to departments comparing the CCR and NLC as applied to alert patients with trauma who were in stable condition alert patients with trauma who were in stable condition
• CCR was more sensitive than the NLC (99.4 percent vs. CCR was more sensitive than the NLC (99.4 percent vs. 90.7 percent, P<0.001) and more specific (45.1 90.7 percent, P<0.001) and more specific (45.1 percent vs. 36.8 percent, P<0.001 percent vs. 36.8 percent, P<0.001
• For alert patients with trauma who are in stable For alert patients with trauma who are in stable condition, the CCR is superior to the NLC with respect condition, the CCR is superior to the NLC with respect to sensitivity and specificity for cervical-spine injury, to sensitivity and specificity for cervical-spine injury, and its use would result in reduced rates of and its use would result in reduced rates of radiography radiography

Clinical clearanceClinical clearance
• EvaluateEvaluate
• StrengthStrength
• SensationSensation
• TendernessTenderness
• ROMROM
• ?image?image
• ClearClear

Initial immobilizationInitial immobilization


ReferencesReferences
• Stiell IG, Wells GA, Vandemheen K, et al. The Stiell IG, Wells GA, Vandemheen K, et al. The Canadian Cervical Spine Radiography Rule for Canadian Cervical Spine Radiography Rule for alert and stable trauma patients. JAMA alert and stable trauma patients. JAMA 2001;286:1841-8. 2001;286:1841-8.
• Stiell IG, Clement C, McKnight RD, et al. The Stiell IG, Clement C, McKnight RD, et al. The Canadian C-Spine Rule versus the NEXUS low-risk Canadian C-Spine Rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med criteria in patients with trauma. N Engl J Med 2003;349:2510-8. 2003;349:2510-8.
• N Engl J Med 2000;343:94-9.• JAMA. 2001;286:1841-1848• http://www.med-ed.virginia.edu/courses/rad/cspinhttp://www.med-ed.virginia.edu/courses/rad/cspin
e/e/