Embed Size (px)
Citation preview
traaNte
bmSb
hNwcpo
R
1
1
1
1
1
1
1
1
1
1
2
J6
R
C
p
4
N
©
0
d
1976 CERVICOFACIAL SUBCUTANEOUS EMPHYSEMA
herapeutic decision making. Sclerosing agents, ste-oids, radiotherapy, lasers, cryotherapy, embolization,nd even continued observation represent reasonablepproaches to the vascular aspect of the lesion.6,7
evertheless, when feasible, surgical excision is thereatment method of choice and will also succeed inliminating the phlebolith.Our patient with the IMH opted for no treatment
ecause she stated that other than a moderate cos-etic asymmetry, she had no subjective problems.
he did agree to return every 6 months for evaluation,ut she failed to present for further follow-up.In our patient with the VM, significant symptoms
ad developed that prompted her to seek therapy.ormal masticatory function inevitably caused traumaith associated hemorrhage. Furthermore, she be-
ame increasingly embarrassed about her speech im-ediment. She was referred to an interventional radi-logist who plans to embolize the lesion.
eferences1. Shemilt P: The origin of phleboliths. Br J Surg 59:695, 19722. Ribbert H: Die phlebolithen. Virchows Arch 223:339, 19173. Sano K, Ogawa A, Inokuchi T, et al: Buccal hemangioma with
phlebolith. Oral Surg Oral Med Oral Pathol 65:151, 19884. Morris SJ, Adams H: Case report: Paediatric intramuscular he-
mangiomata—Don’t overlook the phlebolith! Br J Radiol 68:208, 1995
5. Elahi M, Parnes L, Fox A: Hemangioma of the masseter muscle.J Otolaryngol 21:177, 1992
Julius Berger
Sp1alesmaaawc1oi:10.1016/j.joms.2010.02.018
6. Rossiter JL, Hendrix RA, Tom LWC, et al: Intramuscular he-mangioma of the head and neck. Otolaryngol Head Neck Surg108:18, 1993
7. Yang WT, Ahuja A, Metreweli C: Sonographic features of headand neck hemangiomas and vascular malformations: A reviewof 23 patients. J Ultrasound Med 16:39, 1997
8. Avci G, Yim S, Misirliogolu A, et al: Intramasseteric hemangi-oma. Plast Reconstr Surg 109:1748, 2002
9. Mulliken JB, Glowacki J: Hemangiomas and vascular malforma-tions in infants and children: A classification based on endo-thelial characteristics. Plast Reconstr Surg 69:412, 1982
0. Glowacki J, Mulliken JB: Mast cells in hemangiomas and vas-cular malformations. Pediatrics 70:48, 1982
1. Gampper T, Morgan RF, Sadove AM: Vascular anomalies: He-mangiomas. Plast Reconstr Surg 110:572, 2002
2. Wolf GT, Daniel F, Krause CJ, et al: Intramuscular hemangiomaof the head and neck. Laryngoscope 95:210, 1985
3. Cohen MM: Vasculogenesis, angiogenesis, hemangiomas, andvascular malformations. Am J Med Genet 108:265, 2002
4. Beck D, Gosain AK: The presentation and management ofhemangiomas. Plast Reconstr Surg 123:181e, 2009
5. Addante RR, Donovan MG: Right facial mass. J Oral MaxillofacSurg 52:1061, 1994
6. Odabasi AO, Metin KK, Mutlu C, et al: Intramuscular heman-gioma of the masseter muscle. Eur Arch Otorhinolaryngol 256:366, 1999
7. Robertson JS, Wiegand D, Schaitkin BM: Life-threatening he-mangioma arising from the parotid gland. Otolaryngol HeadNeck Surg 104:858, 1991
8. Hessel AC, Vora N, Kountakis SE, et al: Vascular lesion of themasseter presenting with phlebolith. Otolaryngol Head NeckSurg 120:548, 1999
9. Scolozzi P, Laurent F, Lombardi T, et al: Intraoral venousmalformation presenting with multiple phleboliths. Oral SurgOral Med Oral Pathol Oral Radiol Endod 96:197, 2003
0. Baker LL, Dillon WP, Hieshima GB, et al: Hemangiomas and
vascular malformations of the head and neck: MR characteriza-tion. AJNR Am J Neuroradiol 14:307, 1993Oral Maxillofac Surg8:1976-1982, 2010
Cervicofacial Subcutaneous Emphysema:Case Report and Review of Literature
Nishul Patel, DMD,* Stewart K. Lazow, MD, DDS,† and
, DDS‡
eceived from Department of Oral and Maxillofacial Surgery, Kings
ounty Hospital, Brooklyn, NY.
*Chief Resident.
†Director of Service.
‡Chief of Service.
Address correspondence and reprint requests to Dr Patel: De-
artment of Oral and Maxillofacial Surgery, Kings County Hospital,
51 Clarkson Avenue, E-Building, Brooklyn, NY 11203; e-mail:
2010 American Association of Oral and Maxillofacial Surgeons
278-2391/10/6808-0038$36.00/0
ubcutaneous emphysema is by no means a contem-orary discovery, having been mentioned more than80 years ago. Previously described as pneumomedi-stinum, Laenec, in 1827, termed the disease “inter-obar emphysema.”1 Reports described subcutaneousmphysema in a patient with a violent coughing epi-ode in 1850.2 The first official report by an anony-ous investigator of the phenomenon stemmed frommusician playing the bugle after a dental extraction
t the beginning of the 20th century.3 Macklin in 1939nd 1944 proposed a pathophysiologic clarification,2
hich led to the rudimentary 4-tier classification ac-ording to the etiology of cervicofacial emphysema in
957, derived by Shovelton. The various etiologies of
ctaAfthtrciccbfHotpob
R
sbCsmOmnhtstms
Ohttodpassiaasw
btnwfTnpNptstmpsct
ctptacohh
B
P
F
N
DaP
P
PATEL, LAZOW, AND BERGER 1977
ervicofacial emphysema have included increased in-raoral pressure at the site of a mucosal injury or thellowance of compressed air into an intraoral wound.dditional causes were theorized, such as trauma
rom a challenging extraction, especially a mandibularhird molar, and, finally, no apparent cause.3 Non-ead and neck injuries, such as penetrating trauma tohe gastrointestinal or respiratory systems, can alsoesult in the disease. Gases trapped under the tissuean lead to infection, such as gas gangrene.4 Iatrogen-cally, improper placement of, or a nonfunctioning,hest tube for treatment of a pneumothorax can alsoause it.2 This can lead to the pressure of the alveolieing greater than the surrounding tissues.4 Cervico-acial emphysema can be associated with a positiveamman’s sign, which is a crunching sound heardver the pericardium, and is associated with medias-inal emphysema. The etiology of subcutaneous em-hysema, whether traumatic, iatrogenic, incidental,r pathologic, all stems from the introduction of gasetween the tissue layers (Table 1).2,4-21
eport of a Case
On August 5, 2007, an 18-year-old black man who hadustained blunt trauma from fists to his head, but no otherodily trauma, presented to the Kings County Hospitalenter Emergency Department. He was admitted to theurgical intensive care unit by the trauma service for airwayonitoring owing to the substantial cervicofacial edema.n consultation, the patient complained primarily of leftandibular pain and swelling but not of dyspnea or orthop-
ea. He reported a medical history of uncomplicated child-ood asthma with no hospitalizations, intubations, or at-acks during the previous 10 years. The patient had aurgical history of an appendectomy but no history of facialrauma. He denied known drug or food allergies, denied anyedication use, intravenous drug abuse, or tobacco con-
umption; however, he was intoxicated and uncooperative.
Table 1. ETIOLOGY OF SUBCUTANEOUS EMPHYSEMA
Trauma Iatrogenic
lunt chest2,10,19 (27% ofrib fractures, tensionpneumothorax)
Anesthesia8,9,17 (endotrachealnasotracheal intubation,laparoscopy)
enetrating chest9,21
(stabbing, gunshot)Chest surgery7,20 (improper c
tube placement,pneumonectomy, thoracoto
acial bones5 (sinusfractures)
Neck surgery8 (esophageal,cricothrotomy)
eck12,16 (tracheal/laryngeal tears,esophageal rupture)
Pneumatic tools15 (dental higspeed handpieces)
ata from Parker et al,2 Maunder et al,4 Wong and McGuire,nd Vanner,11 Findlay et al,12 Criner and D’Alonzo,13 Ranan,17 Conetta et al,18 Schnyder and Wintermark,19 Long e
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphysema. J O
n admission, the patient was hemodynamically stable andad a low-grade fever. During the head and neck examina-ion, the patient had significant left facial swelling inconsis-ent with the severity of the left mandible fracture. Thecclusion was stable and reproducible without any stepeformities or mobile segments. Although the patient com-lained of left inferior alveolar nerve paresthesia, this wasttributed to the severe left facial edema. The neck demon-trated bilateral crepitus that extended medially from bothternocleidomastoid muscles to the thyroid cartilage andnferiorly from the border of the mandible to the claviclend suprasternal notch. This crepitus was most notablelong the clavicle, zone 1 region, of the neck owing to hislim frame. The remaining physical examination findingsere nonsignificant.After the appropriate workup, consisting of a complete
lood count, comprehensive chemistry panel, and coagula-ion studies, only the white blood cell count of 21,000 wasotable. Head and facial computed tomography (CT) scansith respective reconstructions demonstrated air tracking
rom the face caudally. A barium swallow test was negative.he neck CT scan demonstrated a large amount of air in theeck and retropharyngeal space (Figs 1, 2). Chest radiogra-hy and noncontrast chest CT scan were obtained (Fig 3).o pneumothorax was present, but the subcutaneous em-hysema extended through the superior mediastinum tohe level of the carina. Otolaryngology and cardiothoracicurgery staff were consulted, and they wished to follow-uphe patient closely in a monitored setting. Regarding the leftandible fracture, the facial CT scan showed a nondis-laced left body of the mandible fracture. Dental panoramictudies were later obtained with the patient in a more stableondition to better study the fractures and the dental rela-ionships (Fig 4).
The treatment plan for the left angle mandible fractureonsisted of a closed reduction of the left angle owing tohe nondisplaced nature of the left angle fracture to beerformed in the clinic with the patient under local anes-hesia. After optimization and clearance from the traumand cardiothoracic service, the patient underwent the pro-edure without issue and was then treated directly by theral and maxillofacial service. The patient, since admission,ad been receiving intravenous clindamycin 600 mg every 6ours and dexamethasone 8 mg every 8 hours. For his
Incidental Pathologic
Barotrauma2,6,13,14,18 (diving,positive pressureventilation)
Infections5 (anaerobic,clostridia, mixed,gas-formingfacultative aerobic)
Labor2,11 (1 in 2000-100,000deliveries)
Neoplasia5
Foreign body12
Heimlich maneuver2
ris and Roussos,6 Lefor,7 Brooks,8 Peart,9 Wicky et al,10 Jaint al,14 van der Molen,15 Kosmas and Polychronopoulos,16
and DeGowin.21
/
hest
my)
h-
5 Papikine et al,20
ral Maxillofac Surg 2010.
rwlmtt
hitstdmTtesviciaposnctudto D
sodttfs
Fs
Ps
Fe
Ps
1978 CERVICOFACIAL SUBCUTANEOUS EMPHYSEMA
emaining stay, a broader spectrum antibiotic, ampicillin 2 gith sulbactam 1 g, was given every 6 hours. Because of the
imited oral intake, the patient’s liquid diet was supple-ented with intravenous fluid for hydration. Supplemen-
ary oxygen using a mask or cannula was not given duringhe patient’s hospitalization.
Throughout his stay, the patient remained afebrile, withis other vital signs within an acceptable range. While in the
ntensive care unit, blood was taken for serial laboratoryests, and the chest radiography and chest and neck CTcans were repeated (Figs 5-7). The emphysema appearedo be resolving, and the white blood cell count initiallyecreased to 12,000 but then increased slightly to 15,000,ost likely owing to the systemic steroid administration.he patient’s general clinical improvement was evident in
he resolution of the crepitus of the left neck, decreaseddema, and overall disposition. He tolerated the hospitaltay, procedure, and diet and returned to normal activitiesery well by discharge 5 days later. He was discharged withnstructions to take oral amoxicillin trihydrate 875 mg andlavulanic acid 125 mg for 7 days. The patient followed upn the dental clinic approximately 7 days after discharge for
panoramic radiograph and evaluation (Fig 7). After ap-roximately 2 weeks, a preliminary chest radiograph wasbtained that demonstrated significant resolution of theubcutaneous emphysema. Although mildly evident in theeck, it had disappeared from the mediastinal region. Be-ause of the patient’s vast clinical improvement, no addi-ional radiologic studies were performed. He was followedp on successive weekly intervals and had his maxilloman-ibular fixation released and removed 1 month postopera-ively. During follow-up, no additional signs of subcutane-us emphysema were evident.
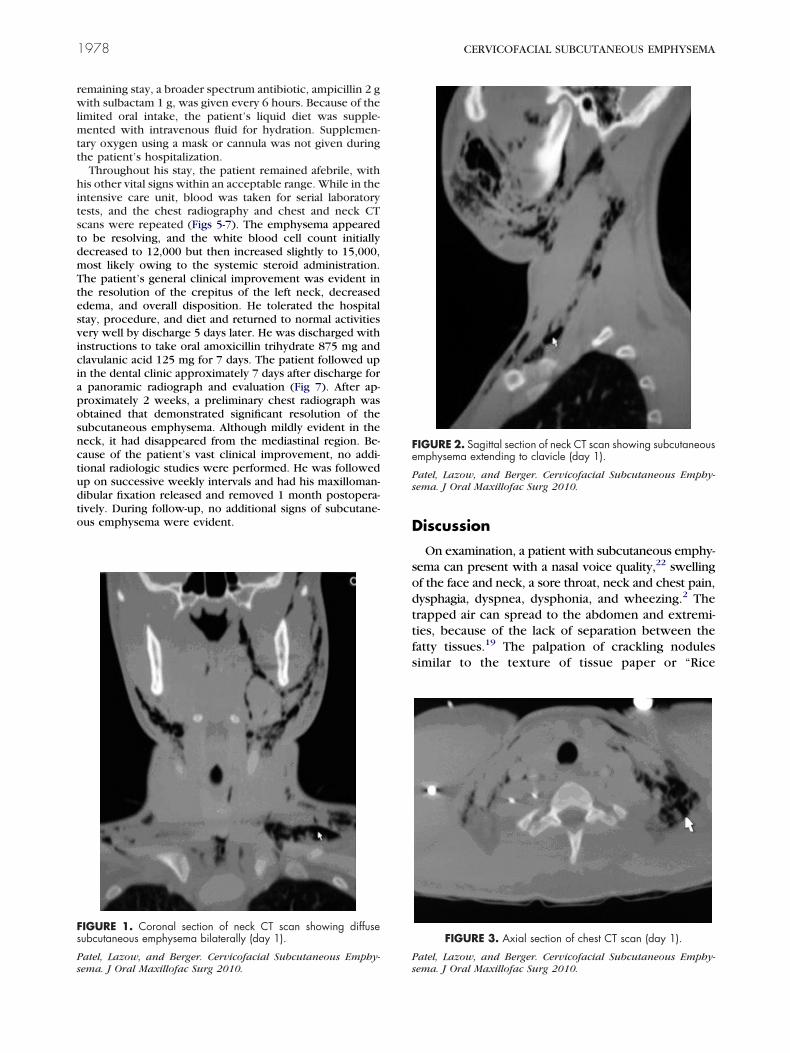
IGURE 1. Coronal section of neck CT scan showing diffuseubcutaneous emphysema bilaterally (day 1).
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
Ps
iscussion
On examination, a patient with subcutaneous emphy-ema can present with a nasal voice quality,22 swellingf the face and neck, a sore throat, neck and chest pain,ysphagia, dyspnea, dysphonia, and wheezing.2 Therapped air can spread to the abdomen and extremi-ies, because of the lack of separation between theatty tissues.19 The palpation of crackling nodulesimilar to the texture of tissue paper or “Rice
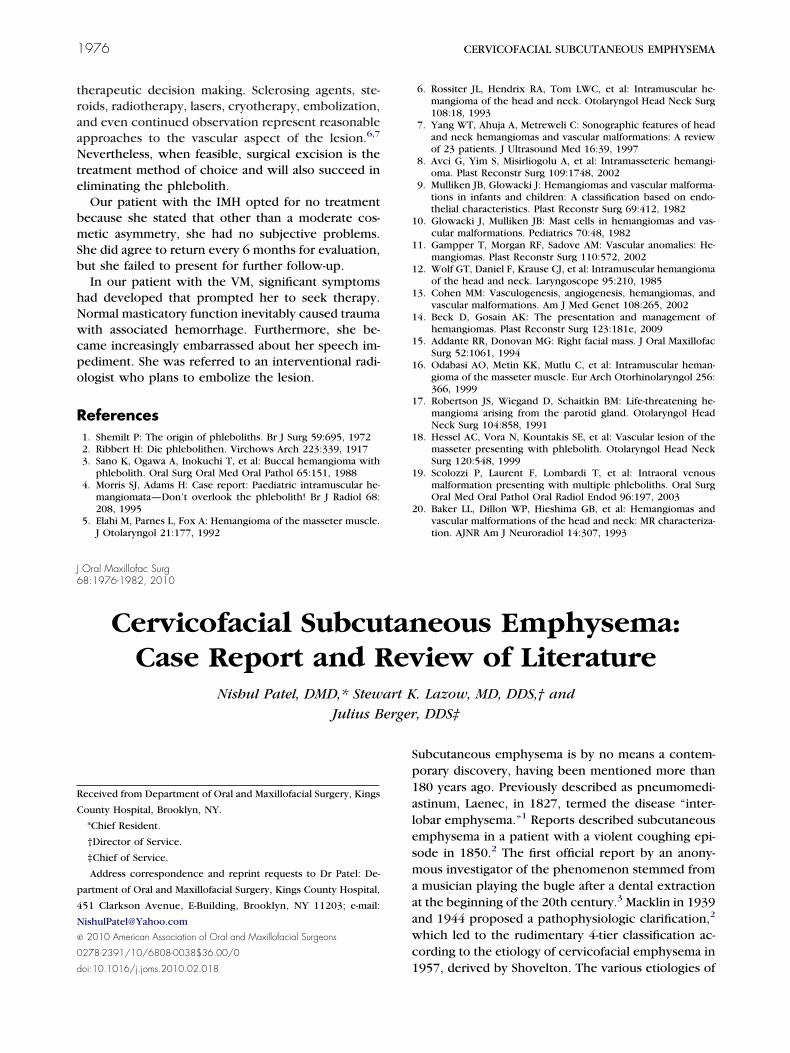
IGURE 2. Sagittal section of neck CT scan showing subcutaneousmphysema extending to clavicle (day 1).
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
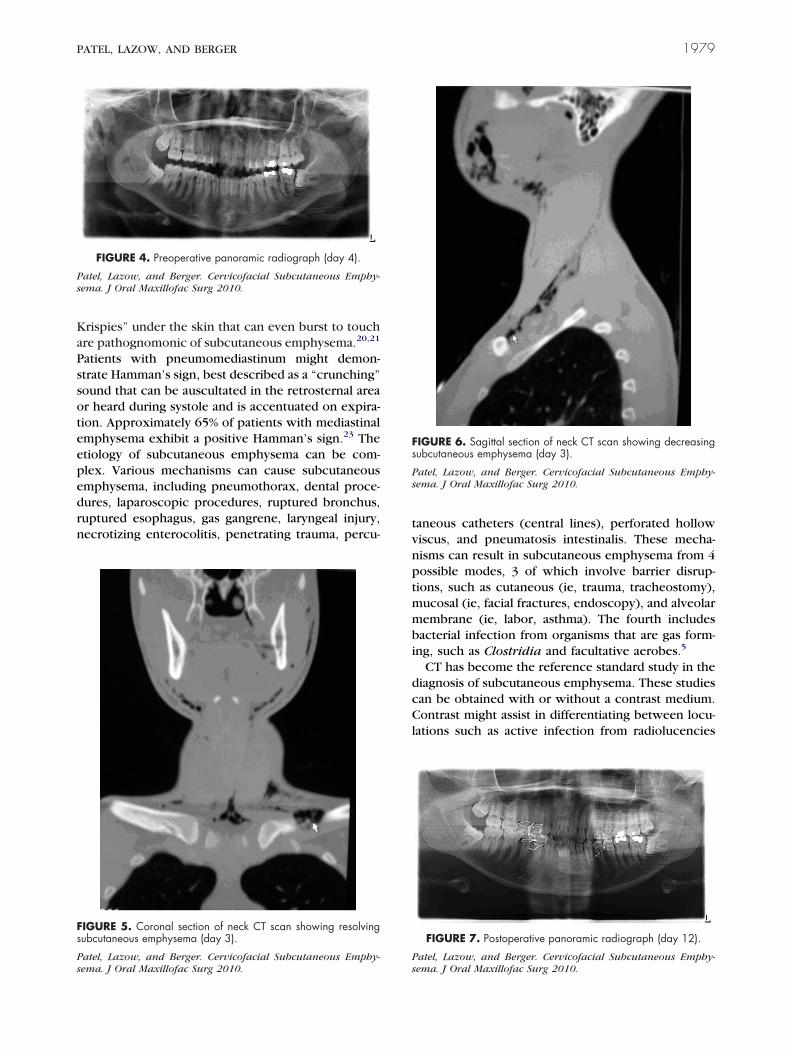
FIGURE 3. Axial section of chest CT scan (day 1).
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
KaPssoteepedrn
tvnptmmbi
dcCl
Ps
Fs
Ps
Fs
Ps
PATEL, LAZOW, AND BERGER 1979
rispies” under the skin that can even burst to touchre pathognomonic of subcutaneous emphysema.20,21
atients with pneumomediastinum might demon-trate Hamman’s sign, best described as a “crunching”ound that can be auscultated in the retrosternal arear heard during systole and is accentuated on expira-ion. Approximately 65% of patients with mediastinalmphysema exhibit a positive Hamman’s sign.23 Thetiology of subcutaneous emphysema can be com-lex. Various mechanisms can cause subcutaneousmphysema, including pneumothorax, dental proce-ures, laparoscopic procedures, ruptured bronchus,uptured esophagus, gas gangrene, laryngeal injury,ecrotizing enterocolitis, penetrating trauma, percu-
FIGURE 4. Preoperative panoramic radiograph (day 4).
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
IGURE 5. Coronal section of neck CT scan showing resolvingubcutaneous emphysema (day 3).
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
Ps
aneous catheters (central lines), perforated hollowiscus, and pneumatosis intestinalis. These mecha-isms can result in subcutaneous emphysema from 4ossible modes, 3 of which involve barrier disrup-ions, such as cutaneous (ie, trauma, tracheostomy),ucosal (ie, facial fractures, endoscopy), and alveolarembrane (ie, labor, asthma). The fourth includes
acterial infection from organisms that are gas form-ng, such as Clostridia and facultative aerobes.5
CT has become the reference standard study in theiagnosis of subcutaneous emphysema. These studiesan be obtained with or without a contrast medium.ontrast might assist in differentiating between locu-
ations such as active infection from radiolucencies
IGURE 6. Sagittal section of neck CT scan showing decreasingubcutaneous emphysema (day 3).
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
FIGURE 7. Postoperative panoramic radiograph (day 12).
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
sqgHptcraaspbcHttsu
teg
iSlcweettssapspmrrnppnwnvc
witwmcas
Fs
Ps
D
Ps
F(
Ps
1980 CERVICOFACIAL SUBCUTANEOUS EMPHYSEMA
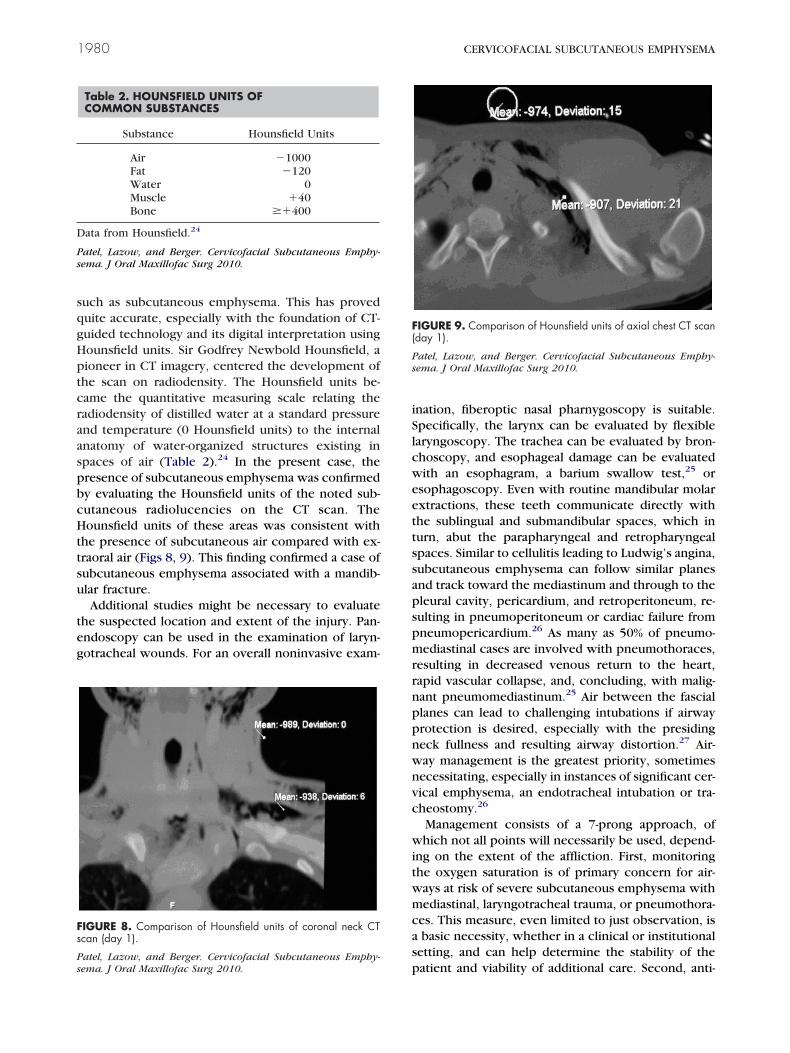
uch as subcutaneous emphysema. This has proveduite accurate, especially with the foundation of CT-uided technology and its digital interpretation usingounsfield units. Sir Godfrey Newbold Hounsfield, aioneer in CT imagery, centered the development ofhe scan on radiodensity. The Hounsfield units be-ame the quantitative measuring scale relating theadiodensity of distilled water at a standard pressurend temperature (0 Hounsfield units) to the internalnatomy of water-organized structures existing inpaces of air (Table 2).24 In the present case, theresence of subcutaneous emphysema was confirmedy evaluating the Hounsfield units of the noted sub-utaneous radiolucencies on the CT scan. Theounsfield units of these areas was consistent with
he presence of subcutaneous air compared with ex-raoral air (Figs 8, 9). This finding confirmed a case ofubcutaneous emphysema associated with a mandib-lar fracture.Additional studies might be necessary to evaluate
he suspected location and extent of the injury. Pan-ndoscopy can be used in the examination of laryn-otracheal wounds. For an overall noninvasive exam-
IGURE 8. Comparison of Hounsfield units of coronal neck CTcan (day 1).
Table 2. HOUNSFIELD UNITS OFCOMMON SUBSTANCES
Substance Hounsfield Units
Air �1000Fat �120Water 0Muscle �40Bone ��400
ata from Hounsfield.24
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
patel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
nation, fiberoptic nasal pharnygoscopy is suitable.pecifically, the larynx can be evaluated by flexiblearyngoscopy. The trachea can be evaluated by bron-hoscopy, and esophageal damage can be evaluatedith an esophagram, a barium swallow test,25 or
sophagoscopy. Even with routine mandibular molarxtractions, these teeth communicate directly withhe sublingual and submandibular spaces, which inurn, abut the parapharyngeal and retropharyngealpaces. Similar to cellulitis leading to Ludwig’s angina,ubcutaneous emphysema can follow similar planesnd track toward the mediastinum and through to theleural cavity, pericardium, and retroperitoneum, re-ulting in pneumoperitoneum or cardiac failure fromneumopericardium.26 As many as 50% of pneumo-ediastinal cases are involved with pneumothoraces,
esulting in decreased venous return to the heart,apid vascular collapse, and, concluding, with malig-ant pneumomediastinum.25 Air between the fasciallanes can lead to challenging intubations if airwayrotection is desired, especially with the presidingeck fullness and resulting airway distortion.27 Air-ay management is the greatest priority, sometimesecessitating, especially in instances of significant cer-ical emphysema, an endotracheal intubation or tra-heostomy.26
Management consists of a 7-prong approach, ofhich not all points will necessarily be used, depend-
ng on the extent of the affliction. First, monitoringhe oxygen saturation is of primary concern for air-ays at risk of severe subcutaneous emphysema withediastinal, laryngotracheal trauma, or pneumothora-
es. This measure, even limited to just observation, isbasic necessity, whether in a clinical or institutional
etting, and can help determine the stability of the
IGURE 9. Comparison of Hounsfield units of axial chest CT scanday 1).
atel, Lazow, and Berger. Cervicofacial Subcutaneous Emphy-ema. J Oral Maxillofac Surg 2010.
atient and viability of additional care. Second, anti-

bempeaasaggagpuip7giptoppespanoisppis
mwaptbppgtt
iopard
eolssgmittFttstetfmtotetm
R
1
1
1
1
1
1
PATEL, LAZOW, AND BERGER 1981
iotic coverage with a broad-spectrum agent that cov-rs the more common head, neck, sinus, and skinicroflora is recommended and should include pro-hylaxis against necrotizing fasciitis.28 With knowl-dge of the location and mechanism, the appropriatentibiotic can be selected: penicillin, or, alternatively,
cephalosporin, because oral/pharyngeal flora areensitive to both.27 Of concern is that contaminatedir that is forced subcutaneously could lead to gasangrene with bacteria such as Clostridium perfrin-ens, group A streptococci, Staphylococcus aureus,nd Vibrio vulnificus. Certain data have reported thatas gangrene is a major cause of subcutaneous em-hysema from gas-producing organisms.29 Third, these of 100% oxygen therapy by way of a nonrebreath-
ng mask or even nasal cannula can resolve the em-hysema.3 The composition of air is approximately8% nitrogen and 21% oxygen, with traces of otherases. Oxygen is more readily absorbed than nitrogenn the soft tissues. Because of oxygen’s increasedressure gradient, nitrogen is resorbed from the softissue.25,27 Regarding gas gangrene, hyperbaricxygen therapy has been suggested, especially foratients with an unknown etiology.29 Fourth, sup-ressors of the offending mechanism to reduce orliminate additional injury; stool softeners to decreasetrong Valsalva maneuvers, decongestants as a sinusrecaution to reduce the forceful passage of air, andntitussives to suppress coughs can be used.5 Intrave-ous fluids are purely for hydration in cases in which therofacial edema, laryngeal damage, or dysphagia prohib-
ts or hinders oral intake for a short period.6 Systemicteroids can be used to reduce the soft tissue edema,rovided the patient has no contraindications such asoorly controlled diabetes.7 Serial CT scans are not only
mportant for diagnosis, but also to gauge the progres-ion of treatment and patient improvement.
With subcutaneous emphysema spread past theediastinum, the risk of pneumothorax is increasedith positive pressure ventilation such as a general
nesthetic procedure without a chest tube for decom-ression. Overall, positive pressure ventilation is con-raindicated. Avoidance of nitrous oxide is important,ecause it can exacerbate a pneumomediastinum orneumothorax. This occurs because the blood/gasartition coefficient of nitrous oxide is 34 timesreater than that of nitrogen, leading to an inflation ofhe gas in the air-filled cavity owing to the inability ofhe nitrogen to escape.23
The etiology is key if subcutaneous emphysema isncluded in a differential diagnosis. However, the eti-logy of the present case remains a mystery. Theatient denied any loss of consciousness from thettack and claimed to recall the entire event accu-ately. He also did not admit to any adverse behavior
uring or after the assault that could have led to thepisode of emphysema. The extent of the subcutane-us emphysema and the point of fracture as the most
ikely cause of the subcutaneous emphysema did noteem to correlate with each other. Perhaps defen-ively, after being struck, the patient might have beenasping, and his inspirations and expirations wereeeting resistance. The expirations might have mim-
cked a Valsalva-like maneuver and forced air throughhe gingival and mucosal lacerations the patient sus-ained from his left angle of the mandible fracture.rom there the air traveled to the floor of the moutho the sublingual space and posteriorly. Once encoun-ering the pterygomandibular and lateral pharyngealpaces, the air traveled in the deep fascial spaces ofhe neck.23 Regardless of the mechanism of injury, itstiology, or severity, the treatment protocol of subcu-aneous emphysema involves airway management, in-ection prophylaxis, and radiologic assessment. Thisanagement, whether medical or surgical, is left to
he judgment of the clinician, concerning the extentf the measures to be taken and the overall stability ofhe patient. Although the treatment of subcutaneousmphysema is conservative and observatory, if notreated, it can lead to a compromised airway, pneu-omediastinum, or, even, pneumothorax.
eferences1. Minton G, Tu HK: Pneumomediastinum, pneumothorax, and
cervical emphysema following mandibular fractures. J OralSurg 57:490, 1984
2. Parker GS, Mosborg DA, Foley RW, et al: Spontaneous cervicaland mediastinal emphysema. Laryngoscope 100:938, 1990
3. Josephson GD, Wambach BA, Noordzji JP: Subcutaneous cer-vicofacial and mediastinal emphysema after dental instrumen-tation. Otolaryngol Head Neck Surg 124:170, 2001
4. Maunder RJ, Pierson DJ, Hudson LD: Subcutaneous and medi-astinal emphysema: Pathophysiology, diagnosis, and manage-ment. Arch Intern Med 144:1447, 1984
5. Wong DT, McGuire GP: Subcutaneous emphysema followingtrans-cricothyroid membrane injection of local anesthetic. CanJ Anesth 47:165, 2000
6. Papiris SA, Roussos C: Pleural disease in the intensive care unit:Lung biology in health and disease, in Bouros D (ed). PleuralDisease. New York, NY, Marcel Dekker, 2004, pp 771-777
7. Lefor AT: On call. Crit Care 238, 20028. Brooks DR: Current review of minimally invasive surgery. Curr
Med 36, 19989. Peart O: Subcutaneous emphysema. Radiol Technol 77:4:296,
20060. Wicky S, Wintermark M, Schnyder P, et al: Imaging of blunt
chest trauma. Eur Radiol 10:1524, 20001. Jain P, Vanner T: Subcutaneous emphysema with pneumome-
diastinum during the second stage of labour: A rare intrapartumcomplication. Internet J Obstet Gynaecol 9:1, 2008
2. Findlay DA, Morrissey S, Paton JY: Subcutaneous emphysemasecondary to foreign body aspiration. Pediatr Pulm 36:81, 2003
3. Criner GJ, D’Alonzo GE: Critical Care Study Guide: Text andReview. Berlin, Germany, Springer, 2002
4. Rankine JJ, Thomas AN, Fluechter D: Diagnosis of pneumotho-rax in critically ill adults. Postgrad Med J 76:399, 2000
5. van der Molen AB, Birndorf M, Dzwierzynski WW, et al: Sub-cutaneous tissue emphysema of the hand secondary to nonin-
fectious etiology: A report of two cases. J Hand Surg (Am)24:638, 1999
1
1
1
1
2
2
2
2
2
2
2
2
2
2
J6
Tdagntcmp
u
R
M
f
D
C
P
a
©
0
d
1982 NEVOID BASAL CELL CARCINOMA SYNDROME
6. Kosmas EN, Polychronopoulos VS: Pleural effusions in gastro-intestinal tract diseases, in Bouros D (ed). Pleural Disease. NewYork, NY, Marcel Dekker, 2004, p 798
7. Pan PH: Perioperative subcutaneous emphysema: Review ofdifferential diagnosis, complications, management, and anes-thetic implications. J Clin Anesth 1:457, 1989
8. Conetta R, Barman AA, Iakovou D, et al: Acute ventilatoryfailure from massive subcutaneous emphysema. Chest 104:978, 1993
9. Schnyder P, Wintermark M: Radiology of Blunt Trauma of theChest. New York, NY, Springer, 2000, pp 10-11
0. Long BC, Cassmeyer V, Phipps WJ: Adult Nursing: NursingProcess Approach. St Louis, MO, Mosby, 1995, p 328
1. DeGowin RL, LeBlond RF, Brown DR: DeGowin’s DiagnosticExamination. New York, NY, McGraw-Hill Medical PublishingDivision, 2004, pp 388-552
2. Mattox KL, Allen MK: Systemic approach to pneumothorax,haemothorax, pneumomediastinum, and subcutaneous emphy-
sema. Injury 17:309, 1986Ataollah Habibi, DDS, MSc,* Ham
detmmc
ajbbtp
R
wg
ptruotboi:10.1016/j.joms.2009.09.032
3. Sansevere JJ, Badwal RS, Najjar TA: Cervical and mediastinalemphysema secondary to mandible fracture: Case report andreview of the literature. Int J Oral Maxillofac Surg 22:278, 1993
4. Hounsfield GN: Computed medical imaging. Med Phys 7:283,1980
5. Oliver AJ, Diaz EM, Helfrick JF: Air emphysema secondary tomandibular fracture. J Oral Maxillofac Surg 51:1143, 1993
6. Frühauf J, Weinke R, Pilger U, et al: Soft tissue cervicofacialemphysema after dental treatment: Report of 2 cases withemphasis on the differential diagnosis of angioedema. ArchDermatol 141:1437, 2005
7. Anderson JA, Tucker MR, Foley WL, et al: Subcutaneous em-physema producing airway compromise after anesthesia forreduction of a mandibular fracture. Oral Surg Oral Med OralPathol 71:275, 1991
8. Hata T, Hosoda M: Cervicofacial subcutaneous emphysemaafter oral surgery. Br J Oral Maxillofac Surg 39:161, 2000
9. Balas P, Oeconomidis M, Tzamouranis D, et al: Spontaneous
subcutaneous emphysema. Am J Surg 127:755, 1974Oral Maxillofac Surg8:1982-1986, 2010
Squamous Cell Carcinoma of theMaxillary Sinus Associated With NevoidBasal Cell Carcinoma Syndrome: Report
of a Case With 21-Year Evaluation
id Jafarzadeh, DDS, MSc†he first recognition of nevoid basal cell carcinoma syn-rome (NBCCS) occurred in 1960 by 2 scientists, Gorlinnd Goltz.1 It is an autosomal dominant syndrome distin-uished by various signs and symptoms. The major diag-ostic features include multiple keratocystic odontogenicumors (KCOTs) of the maxilla and mandible, multipleutaneous basal cell carcinomas, skeletal abnormalities, pal-ar pits, calcification of the falx cerebri, parietal and tem-oral bossing, and mental retardation.1-3
Because the chief complaint of these patients issually related to the infected jaw cysts, the first
eceived from the Faculty of Dentistry and Dental Research Center,
ashhad University of Medical Sciences, Mashhad, Iran.
*Associate Professor and Head, Department of Oral and Maxillo-
acial Surgery.
†Assistant Professor, Department of Endodontics.
Address correspondence and reprint requests to Dr Jafarzadeh:
epartment of Endodontics, Faculty of Dentistry and Dental Research
enter, Mashhad University of Medical Sciences, Vakilabad Boulevard,
O Box 91735-984, Mashhad, Iran; e-mail: JafarzadehBH@mums.
c.ir
2010 American Association of Oral and Maxillofacial Surgeons
278-2391/10/6808-0039$36.00/0
iagnosis is usually performed by a dentist. The pres-nce of accompanying neoplasms is also very critical;hey can include medulloblastoma,4-6 ovarian fibro-a,7 rhabdomyosarcoma, melanoma,8,9 meningio-a,4 breast tumor, uterine tumor, thyroid tumor,
ardiac tumor, and Hodgkin’s disease.8,10,11
In the oral and maxillofacial area, fibrosarcoma,12
meloblastoma, odontogenic myxoma of the upperaw,13 squamous cell carcinoma (SCC) of the mandi-le,14,15 and 1 case of SCC of the maxillary sinus haveeen reported.11 In the present study, we report onhe occurrence of SCC of the maxillary sinus in aatient with NBCCS.
eport of a Case
An 8-year-old boy with a cystic lesion of the left mandibleas seen in the Department of Oral and Maxillofacial Sur-
ery of Mashhad Faculty of Dentistry in 1987 (Fig 1).Under local anesthesia, marsupialization of the cyst was
erformed. Follow-up radiography (Fig 2) in 1988 revealedhe eruption of the lower left premolars. Despite our strongecommendation to continue treatment, he did not returnntil 11 years later (in 1998). The chief complaint on thisccasion was severe infection owing to a mandibular frac-ure due to a traumatic accident. Large cystic lesions in the
ody of the left mandible and ramus of the right mandible




























