Embed Size (px)
Citation preview

Changing epidemiology of maternal mortality in rural India:
time to reset strategies for MDG-5
Pankaj Shah1, Shobha Shah1, Raman V. Kutty2 and Dhiren Modi1
1 Community Health Department, SEWA-Rural, Jhagadia, India2 Achutha Menon Centre for Health Science Studies, Sree Chitra Tirunal Institute for Medical Sciences and Technology,Thiruvananthapuram, India
Abstract objective To understand changes in epidemiology of maternal mortality in rural India in the
context of increasing institutional deliveries and implementation of community-based interventions
that can inform policies to reach MDG-5.
methods This study is a secondary analysis of prospectively collected community-based data of
every pregnancy and its outcomes from 2002 to 2011 in a rural, tribal area of Gujarat, India as part
of safe-motherhood programme implemented by voluntary organisation, SEWA Rural. The
programme consisted of community-based interventions supported by a first referral unit, and
promotion of institutional deliveries. For every maternal death, a verbal autopsy was conducted. The
incidence rates for maternal mortality according to place, cause and timing of maternal deaths in
relation to pregnancy were computed. Annual incidence rate ratios (IRR) and 95% confidence
intervals, adjusted for caste and maternal education, were estimated using Poisson regression to test
for linear trend in reduction in mortality during the study period.
results Thirty-two thousand eight hundred and ninety-three pregnancies, 29 817 live births and 80
maternal deaths were recorded. Maternal mortality ratio improved from 607 (19 deaths) in 2002–2003 to 161 (five deaths) in 2010–2011. The institutional delivery rate increased from 23% to 65%.
The trend of falling maternal deaths was significant over time, with an annual reduction of 17%
(adjusted IRR 0.83 CI 0.75–0.91, P-value <0.001). There were significant reductions in adjusted
incidence rate of maternal deaths due to direct causes, during intrapartum and post-partum periods,
and those which occurred at home. However, reductions in incidence of maternal deaths due to
indirect causes, at hospital and during antepartum period were not statistically significant. Most
maternal deaths are now occurring at hospitals and due to indirect causes.
conclusion Gains in institutional deliveries and community-based interventions resulting in fewer
maternal deaths due to direct causes should be maintained. However, it would be essential to now
prioritise management of indirect causes of maternal mortality during pregnancy at community and
hospitals for further reduction in maternal deaths to achieve MDG-5.
keywords skilled birth attendance, maternal mortality ratio, epidemiology, institutional delivery,
Millennium Development Goal-5
Introduction
The epidemiology of maternal mortality is well known
(Ronsman et al. 2006). Most maternal deaths occur in
poor countries and are clustered around delivery and the
immediate post-partum period, although there are varia-
tions depending upon the population. The majority of
deaths occur due to direct causes such as bleeding, hyper-
tensive disorders and infections (Ronsman et al. 2006).
Guided by epidemiology of maternal mortality, institu-
tional delivery has been promoted to prevent maternal
deaths at the time of delivery (Bale et al. 2003; WHO
2005; Campbell & Graham 2006). India launched Janani
Suraksha Yojana (JSY) in 2005–2006, a conditional cash-
transfer programme to promote institutional deliveries.
Under JSY, a woman living below the poverty line is enti-
tled to Rs. 700 (US $ 14) in rural areas and Rs. 600 in
urban areas if she delivers in a public or accredited pri-
vate health facility. JSY is implemented through commu-
nity-based front-line workers who also are incentivised
for motivating women for delivering in a health facility
(Ministry of Health & Family Welfare 2005). Some state
568 © 2014 John Wiley & Sons Ltd
Tropical Medicine and International Health doi:10.1111/tmi.12282
volume 19 no 5 pp 568–575 may 2014

governments in India initiated their own schemes, such as
free emergency transportation for women in labour to
reach a hospital and innovative public–private partner-
ship (called Chiranjeevi scheme in Gujarat) to involve
obstetricians from private sector (Mavalankar et al.
2009). At the same time, cadres of village-based front-
line workers were established in all villages to motivate
women to deliver at health facilities and facilitate deliv-
ery of community-based-interventions (National Rural
Health Mission 2013). These efforts have resulted in a
significant increase in the institutional delivery rate from
24.4% in 2005 to 61% in 2010 (Office of Registrar Gen-
eral, India 2008, 2010). The maternal mortality ratio
(MMR) has fallen from 407 deaths per 100 000 live
births in 1997–1998 to 212 in 2007–2009 (Sample regis-
tration system, Office of Registrar General, India 1998,
2012). The increase in institutional deliveries with
improved referral linkages is one of the important reasons
thought to have resulted in reduction in MMR in India
(Kumar et al. 2010).
Despite these achievements, India is not on track to
reach the Millennium Development Goal-5 (MDG-5),
which is to reduce number of maternal deaths by 75%
between 1990 and 2015 (United Nations 2012). At this
critical juncture, it would be important to understand
changes in epidemiology of maternal deaths to evaluate
current strategies and guide development of new ones to
achieve MDG-5. The objective of this study was to
examine changes in epidemiology of maternal mortality
in context of increasing institutional deliveries and imple-
mentation of community-based interventions in a rural
block of Gujarat, India from 2002 to 2011. We tested
the hypothesis that there was no change in incidence of
maternal deaths, its causes, time and place in this popula-
tion before and after 2004.
Methods
Study setting
This study is based on prospectively collected community-
based data by field-based front-line workers (FLWs) of
SEWA Rural. SEWA Rural (SR) is a voluntary organisa-
tion in Jhagadia block of Gujarat state in western India.
The population of Gujarat was almost 60 million in 2011,
and per capita annual income was Rs. 22 553 (US $ 450)
(Government of Gujarat 2010, 2012). Gujarat’s MMR
was 148 and infant mortality rate was 50/1000 live births
with institution delivery rate of 56% in 2007–2009(Ministry of Health & Family Welfare 2010, 2012; Office
of Registrar General, India 2012). After collecting baseline
information for 2 years from 1 April 2002 to 30 March
2004, SEWA Rural implemented a family-centred safe-
motherhood and new-born survival project for 7 years
from 1 April 2004 to 31 March 2011 which catered to the
entire Jhagadia block consisting of 168 villages with a
population of 175 000, which is mainly tribal, rural and
poor (SEWA Rural 2011; Kutty et al. 2013).
Community-level interventions were implemented by
FLWs and traditional birth attendants (TBAs) to provide
antepartum, intrapartum and post-partum care. The fol-
lowing method was used to ensure completeness of preg-
nancy registration: The FLWs conducted house-to-house
visits in her village every week and registered all new
pregnancies. Additionally, two cluster supervisors made
monthly door-to-door field visits in all villages to find
and register any remaining new pregnancies, which might
have been missed by FLWs. This resulted in more than
90% complete pregnancy registration of the expected
number of registration based on birth rate of Gujarat.
The FLW visited a pregnant woman five times antepar-
tum and nine times post-partum. During home visits,
FLW’s responsibility was to ensure early registration of
pregnancy, satisfactory birth-preparedness and complica-
tion-readiness, complete antepartum check-up, identifica-
tion and referral of high-risk mothers, counselling of
woman and her family in case of unintended pregnancy
with availability of referral services for termination of
pregnancy, motivate the mother for delivery at hospital,
safe delivery by trained TBA in case of home delivery,
immediate newborn care and post-partum follow-up of
mothers and neonates up to 6 weeks after delivery. Com-
plicated cases were referred to the SEWA Rural hospital,
which is a government and UNICEF approved first refer-
ral unit (FRU) providing Comprehensive Emergency
Obstetrics and Newborn Care attending to almost 2400
deliveries every year. Along with SEWA Rural’s efforts,
Governments of India and Gujarat introduced various
schemes during the same time period to promote
institutional deliveries as described above.
Data collection
Front-line workers used a data collection card to record
information related to demographics, risk factors, deliv-
ery of services, place of delivery, pregnancy outcome and
survival status at 6 weeks post-partum. FLWs also
recorded every maternal death and all female deaths in
their village. Maternal death was defined as ‘[t]he death
of a woman while pregnant or within 42 days of termi-
nation of pregnancy, irrespective of the duration and site
of the pregnancy, from any cause related to or aggravated
by the pregnancy or its management but not from acci-
dental or incidental causes’ (WHO/UNICEF/UNFPA/
© 2014 John Wiley & Sons Ltd 569
Tropical Medicine and International Health volume 19 no 5 pp 568–575 may 2014
P. Shah et al. Changing epidemiology of maternal mortality in rural India

World Bank 2010). A verbal autopsy tool, consisting of
open and close ended questions, was developed by SEWA
Rural based on prevalent WHO guidelines for conducting
verbal autopsy for maternal deaths (WHO 1994). An
experienced supervisor visited the deceased woman’s
home within 1 month of death and conducted a verbal
autopsy by interviewing close family members, TBA and
those who were present at the time of death. Once the
field team confirmed occurrence of maternal death, a
team consisting of a senior obstetrician–gynaecologist,public health professionals and field staff discussed every
maternal death to ascertain cause of death. A primary
and secondary cause of death was assigned and coded by
the team based on International Classification of Dis-
eases-10. The information from the verbal autopsy tool
was entered into to a database at headquarters. Quality
and completeness of data were monitored by programme
managers, obstetricians and statisticians during weekly
meetings, field visits and by comparing field-level data
with SEWA Rural hospital records.
Variables of interest and statistical analysis
Statistical software ‘R’ and STATA 10 were used for
analysis and creating figures (StataCorp 2007; R Core
Team 2012). Information about all pregnancies, preg-
nancy outcomes and maternal deaths among all women
who were resident of the project areas was included for
this study. Every primary cause of death was categorised
in one of two categories: direct and indirect causes.
Deaths from direct causes were defined as ‘those resulting
from obstetric complications of the pregnant state (i.e.
pregnancy, labour and the puerperium), from interven-
tions, omissions or incorrect treatment, or from a chain
of events resulting from any of the above’. Deaths from
indirect causes were defined as ‘those resulting from a
previously existing disease or a disease that developed
during pregnancy and which was not due to direct obstet-
ric causes but which was aggravated by the physiological
effects of pregnancy’ (WHO/UNICEF/UNFPA/World
Bank 2010). Intrapartum period was considered from
onset of labour to end of third stage of labour (Stedman’s
medical dictionary 2005). Institutional delivery rate was
defined as number of deliveries in institution per 100
deliveries including live and still births.
We chose incidence rate of maternal deaths per
100 000 pregnancies for the analysis instead of MMR.
Because a large proportion of maternal deaths occurred
during antepartum period and was due to unsafe abor-
tion where delivery did not take place, MMR (which is
number of maternal deaths per 100 000 live births) was
not sufficient to capture these deaths for analysis.
The incidence rate of maternal deaths per 100 000
pregnancies was estimated by dividing the number of
maternal deaths by total number of pregnancies accord-
ing to place, cause and timing of maternal death in rela-
tion to pregnancy. The trend in reduction in maternal
deaths over the study period was tested using Poisson
regression with calendar year entered in the model as a
single, continuous variable while adjusting for maternal
education and caste. Annual incidence rate ratios (IRR)
covering 2002–2011 with 95% confidence intervals are
reported for each type of maternal death. Changes in pro-
portion of maternal deaths according to its time, place
and cause were also displayed in form of a bar diagram.
Ethical considerations
This study is based on secondary analysis of data col-
lected for project monitoring; thus, ethical review was
not sought. Permission from the scientific committee of
SEWA Rural was obtained as it hosts the data.
Results
In total, 32 893 pregnancies were registered from 2002 to
2011. There were 29 837 (90.7%) live births, 613 (1.9%)
still births, 827 (2.5%) surgical terminations of pregnan-
cies and 1616 (4.9%) spontaneous abortions. Eighty
maternal deaths were recorded from 2002 to 2011. As seen
in Table 1, characteristics of women who had live births
during baseline and project periods were similar, except
literacy, caste and institutional delivery rate improved
during project period. Information about covariates such
as maternal age, caste and maternal education was missing
from 177 (0.5%), 253 (0.7%) and 1493 (4.5%) pregnant
women, respectively. Mean age of deceased women was
26 years, 10 (13%) had unwanted pregnancy and 70
(87%) of women belonged to a scheduled tribe. Only 18
(22%) women who suffered maternal death delivered at
hospital. There were 36 deaths (45%), which occurred
before delivery either during antepartum period or due to
unsafe abortion practices. Twenty-three (28.8%) women
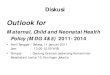
had to seek care at two or more hospitals. Figure 1 shows
the reduction in MMR over time against the institutional
delivery rate. MMR declined sharply during first 4 years
of project; however, a plateau was observed afterwards.
The initial sharp reduction was due to fewer women dying
from haemorrhage (from 11 to 1) and unsafe abortion
(from five to one). The trend in fall of number of maternal
deaths over the study period was significant (P < 0.001).
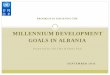
Figure 2(a) shows primary causes of all 80 maternal
deaths. Of all 41 maternal deaths due to indirect causes,
21 occurred antepartum, two intrapartum and 18
570 © 2014 John Wiley & Sons Ltd
Tropical Medicine and International Health volume 19 no 5 pp 568–575 may 2014
P. Shah et al. Changing epidemiology of maternal mortality in rural India

post-partum. Sickle cell anaemia, severe anaemia, malaria
and ectopic pregnancy were some of the most common
causes of maternal deaths, which occurred during ante-
partum period. Eighty-four per cent of the deaths, which
occurred antepartum, were due to indirect causes. Of 11
deaths due to unsafe abortion practices, eight occurred
during first 4 years and only three deaths occurred in last
5 years.
The proportion of deaths, which occurred antepartum,
at hospitals and due to indirect causes has increased
(Figure 3). Major causes of maternal deaths occurring in
hospital were sickle cell disease (21%) and haemorrhage
(21%). Of 38 maternal deaths at hospital, 60% occurred
on the day of admission. Most maternal deaths are now
occurring because of indirect causes and at hospitals
throughout pregnancy.
As seen in Table 2, there was a 17% reduction in
adjusted incidence rate of maternal deaths annually (IRR
0.83, CI 0.75–0.91, P < 0.001). There were significant
reductions in adjusted incidence rate of maternal deaths
every year due to direct causes, during intrapartum, post-
partum period and those which occurred at home. How-
ever, annual reductions in incidence rate of maternal
deaths occurring during the antenatal period (adjusted
IRR 0.89, CI 0.76–1.05, P-value 0.16), at hospital
(adjusted IRR 0.92, CI 0.81–1.05, P-value 0.22) and due
to indirect causes (adjusted IRR 0.93, CI 0.82–1.05,P-value 0.23) were not significant.
Discussion
The epidemiology of maternal mortality underwent a
major shift in Jhagadia block during last decade.
Understanding of this change in epidemiology provides
important lessons for way forward to reach MDG-5 in
India. There is a reduction in overall, time, cause and
place-specific incidence rate of maternal deaths.
Table 1 Profile of all women who had live birth (n = 29 837) inJhagadia block from 2002 to 2011
Baseline
(2002–2003and 2003–04)
Project period
(2004–05 to
2010–11)
Live births, n 6356 23 481
Mean maternalage (years)
25 24
Scheduled tribe (ST)
women, n (%)
4404 (69%) 17 357 (74%)*
Illiterate women,n (%)
3029 (48%) 8685 (37%)*
*P-value <0.001.
600
400
200
060
4020
0
% h
ospi
tal d
eliv
ery
MM
R/1
00 0
00
02–03
19
16
1210
6
Numbers indicatetotal maternal deaths
4 5 53
PROJECTSTARTED
JSY & CYSTARTED
EMRI SERVICESSTARTED
04–05 06–07YEAR
08–09 10–11
Figure 1 Maternal mortality ratio (MMR) and institutionaldelivery rates from 2002 to 2011 in Jhagadia block (Population:
175 000). JSY, Janani Suraksha Yojana; CY, Chiranjeevi
Yojana; EMRI, Emergency Management and Research Institute
free ambulance services.
Ectopic-3 ( 3.75%)
Haemorrhage - 18 ( 22.5 %)
Hepatitis - 3( 3.75)Hypertensive
Disorder-3 (3.75%)
Malaria-3 ( 3.75%)Others-14 (17.5%)Puerpereal Sepsis-3
( 3.75%)
Severe Anaemia-8( 10.0%)
Sickle Cell Disease-10
( 12.5%)
Unsafe Abortion-11 ( 13.7%)
Pulmonary embolism- 2 (2.5)%
Tuberculosis,- 2 (2.5%)
0
100
200
300
400
500
600
700
800
All Cause MMR Direct Causes MMR Indirect Causes MMR
MM
R w
ith 9
5% C
I BaselineDuring project
(a)
(b)
Figure 2 Causes of maternal deaths in Jhagadia block, (n = 80)
(a) Primary cause of death between 2002 and 2011 (b) All-cause
and cause specific maternal mortality ratio (MMR) for baselineand project period.
© 2014 John Wiley & Sons Ltd 571
Tropical Medicine and International Health volume 19 no 5 pp 568–575 may 2014
P. Shah et al. Changing epidemiology of maternal mortality in rural India

Reduction in maternal deaths due to direct causes after
promotion of institutional deliveries has been observed in
other countries (Cross et al. 2010). Two separate
estimates from the Government of India stated that direct
causes were responsible for 73% and 66% of deaths,
though this was before a sharp increase in institutional
65.71%
40.00%31.25% 33.33% 40.00%
34.29%
60.00%68.75% 66.67% 60.00%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2002–04(n = 35)
2004–06(n = 15)
2006–08(n = 16)
2008–10(n = 9)
2010–11(n = 5)
Pro
port
ion
of m
ater
nal d
eath
Year (n = number of maternal deaths)
2002–04(n = 35)
2004–06(n = 15)
2006–08(n = 16)
2008–10(n = 9)
2010–11(n = 5)
Year (n = number of maternal deaths)
2002–04(n = 35)
2004–06(n = 15)
2006–08(n = 16)
2008–10(n = 9)
2010–11(n = 5)
Year (n = number of maternal deaths)
Deaths due to indirect causesDeaths due to directcauses
60.00% 60.00%50.00%
33.33%20.00%
40.00% 40.00%50.00%
66.67%80.00%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pro
port
ion
of m
ater
nal d
eath
Deaths at hospital
Deaths at home and on-the-way
28.57%13.33%
43.75%33.33%
60.00%
71.43%86.67%
56.25%66.67%
40.00%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pro
port
ion
of m
ater
nal d
eath
Deaths during intra and post partum period
Deaths during ante partum period
(a)
(b)
(c)
Figure 3 Proportion of maternal deaths
according to (a) cause, (b) place and (c)
time of death recorded in Jhagadia block,2002–11 (n = 80).
572 © 2014 John Wiley & Sons Ltd
Tropical Medicine and International Health volume 19 no 5 pp 568–575 may 2014
P. Shah et al. Changing epidemiology of maternal mortality in rural India

delivery rate (Ministry of statistics & programme imple-
mentation, Government of India 2005; Office of Regis-
trar General 2008). Two hospital-based studies in North
India reported that indirect causes were responsible for
18% (total number of maternal deaths in study = 1223)
and 51% (total number of maternal deaths in
study = 192) of deaths, respectively (Bhattacharyya et al.
2008; Jain et al. 2009). A nationwide sample survey in
India observed that 23.4% deaths occurred during ante-
partum period, 21% deaths were due to indirect causes,
and 59.1% deaths occurred in health facilities in 2003
(Institute of research in medical statistics, Indian council
of Medical research 2003).
The trend observed in this study might be due to
reduction in deaths due to direct causes occurring around
the time of delivery because of increase in institutional
delivery (or skilled birth attendance) (UNFPA & Univer-
sity of Aberdeen 2004). Community-based efforts aimed
at early identification of unintended pregnancies followed
by sensitive counselling might have helped pregnant
women and their families to make the right decisions and
avoid unsafe abortions. Large reduction in number of
deaths at home and increase in institutional deliveries
might have contributed towards increase in proportion of
maternal deaths at hospital; however, absolute risk of
dying at hospital has fallen.
The findings of this study are important for plan-
ning, implementing and evaluating current and future
safe-motherhood interventions and research. Existing
efforts to promote institutional and safe deliveries
along with increasing coverage and quality of commu-
nity-based interventions should continue. However,
study of maternal deaths in Jhagadia block provides a
‘best case scenario’ for maternal mortality with high
coverage of community-based interventions and increase
in institutional deliveries supported by referral linkages
with functional FRU. Even with that, MMR in Jhag-
adia (161) was slightly more than the India’s MDG-5
target (MMR of 109 deaths/100 000 live births) (Sam-
ple Registration Survey 2011). Therefore, it might be
essential to prioritise management of indirect causes of
maternal mortality during pregnancy for further reduc-
tion in maternal deaths now if India is to achieve
MDG-5.
There is increasing concern regarding the ‘third delay’,
which occurs after a woman reaches a health facility,
especially now as institutional deliveries and proportion
of maternal deaths in hospitals are increasing
Table 2 Maternal deaths in Jhagadia block, by cause, time and place: 2002–2011* (number and incidence per 100 000 pregnancies)
2002–2003and
2003–2004
2004–2005and
2005–2006
2006–2007and
2007–2008
2008–2009and
2009–2010 2010–2011 Annual trend, 2002–2011
Number of deaths (incidence of maternal mortality)
Adjusted incidence
rate ratio† (CI) P-value
Maternal deaths (overall) 35 (520) 15 (186) 16 (218) 9 (122) 5(146) 0.83 (0.75–0.91) <0.0001Maternal deaths due to
direct causes
25 (372) 6 (74) 5 (68) 3 (41) 2 (58) 0.72 (0.61–0.83) <0.0001
Maternal deaths due to
indirect causes
12 (178) 9 (112) 11 (150) 6 (81) 3 (88) 0.92 (0.81–1.05) 0.23
Maternal deaths duringantenatal period
10 (149) 2 (25) 7 (95) 3 (41) 3 (88) 0.89 (0.75–1.04) 0.16
Maternal deaths during
intranatal and post-natal
period
25 (371) 13 (161) 9 (123) 6 (81) 2 (58) 0.79 (0.7–0.9) 0.0002
Maternal deaths at home
and on the way
21 (312) 9 (112) 8 (109) 3 (41) 1 (29) 0.74 (0.64–0.85) <0.001
Maternal deaths at
hospital
14 (208) 6 (74) 8 (109) 6 (81) 4(117) 0.91 (0.81–1.05) 0.22
Total number of
pregnancies
6730 8048 7331 7362 3422 –
*2002–2003 refers to 1/4/2002–31/3/2003; 2003–2004 refers to 1/4/2003 to 31/3/2004; 2004–2005 refers to 1/4/2004 to 31/3/2005;
2005–2006 refers to 1/4/2005 to 31/3/2006; 2006–2007 refers to 1/4/2006–31/3/2007; 2008–2009 refers to 1/4/2008–31/3/2009; 2010–2011 refers to 1/4/2010–31/3/2011.†Estimate is based on the Poisson model treating calendar year as a single linear variable, adjusted for caste and education.
© 2014 John Wiley & Sons Ltd 573
Tropical Medicine and International Health volume 19 no 5 pp 568–575 may 2014
P. Shah et al. Changing epidemiology of maternal mortality in rural India

(Ramanathan 2009). It was observed in this study that
23 (28.8%) women had to seek care at two or more hos-
pitals. There are anecdotal reports where complicated
maternal cases would be referred from one facility to
another without established referral and communication
linkages; thus, resulting in frustration, higher cost, poor
quality of care and ultimately death, in some cases (Sri
et al. 2012). Strengthening referral and communication
linkages between community-level workers to first refer-
ral-facility and to higher referral centres along with
increasing quality of care to manage medial diseases dur-
ing pregnancy could be an important element of prevent-
ing deaths resulting from third delay in hospitals.
There is a concern regarding under-reporting of mater-
nal deaths, which occur during the antepartum period or
due to indirect causes globally (Cross et al. 2010). A
large number of deaths occurred antepartum in this
study, which emphasises importance of tracking every
pregnancy, counting every female death and getting infor-
mation about all epidemiologic aspects including cause of
death. The recently introduced online Mother and Child
Tracking System (MCTS) in India holds promise to track
every pregnancy and its outcome. The MCTS is an
online, name-based tracking system where information
about all pregnant women and children gets entered in
software, and each pregnant woman is tracked until final
outcome; thus, it aims to provide health-managers real-
time, up-to-date information about every pregnancy. Such
solutions could be studied regarding their effectiveness,
feasibility and scalability so that every maternal death is
counted and complete information about its determinants
is available.
One of the important limitations of this study is com-
paratively small sample size. In spite of that, there is a
clear and consistent trend of maternal mortality and
some of its epidemiological determinants. Considering the
predominantly tribal population of Jhagadia block, one
should be careful before generalising these findings to a
wider population. There always remains the concern
about completeness of data while calculating maternal
deaths. This study is based on prospectively collected
data having outcome information for all registered preg-
nancies, including large number of unintended pregnan-
cies. Additionally, SEWA Rural recorded every death
among women of all age groups. These facts give confi-
dence about completeness of reporting of all maternal
deaths. More than one reason might have contributed
towards occurrence of death and assigning single cause of
death can hide the importance of secondary but impor-
tant causes of death. Also, there are inherent limitations
of using verbal autopsy for assigning cause of death
including inadequate diagnostic accuracy for certain
diagnoses and its dependence on quality of data collec-
tion and standardisation (Garenne & Fauveau 2006).
Conclusion
Since 2004, there has been large reduction in number of
maternal deaths due to direct causes. However, it would
be essential to prioritise management of indirect causes of
maternal mortality during pregnancy at community level
and hospitals for further reduction in maternal deaths so
that MDG-5 can be achieved in India.
Acknowledgements
We thank the John D and Catherine T MacArthur Foun-
dation for generously supporting Safe Motherhood and
Newborn Survival Project. We are grateful to Drs. Maya
Hazra, Gayatri Desai and Lata Desai for their extra-
ordinary support throughout the project. We thank all
members of community of Jhagadia, including front-line
workers, link-workers, supervisors and government
health staff for their contribution. We are grateful to
Dr. Shivani Patel for her invaluable help towards
analysis.
References
Stedman’s Medical Dictionary (28th edn) (2005) Lippincott
Williams & Wilkins, Philadelphia.
Bale J, Stoll B, Mack A et al. (2003) Improving Birth Outcomes:
Meeting the Challenges in the Developing World. National
Academy of Sciences and Institute of Medicine, Washington,
DC.
Bhattacharyya SK, Majhi AK, Seal SL et al. (2008) Maternal
mortality in India: a 20-year study from a large referral medi-
cal college hospital, West Bengal. Journal of Obstetrics and
Gynaecology Research 34, 499–503. PMID: 18937703.
Campbell OM & Graham WJ (2006) Strategies for reducing
maternal mortality: getting on with what works. Lancet 368,
1284–1299. PMID: 17027735.
Cross S, Bell JS & Graham WJ (2010) What you count is what
you target: the implications of maternal death classification for
tracking progress towards reducing maternal mortality in
developing countries. Bulletin of the World Health Organiza-
tion 88, 147–153. PMID: 20428372.
Garenne M & Fauveau V (2006) Potentials and limitations of
verbal autopsies. Bulletin of the World Health Organization
84, 164–165.
Government of Gujarat (2010) Socio-economic review, Gujarat
state, 2007–08. http://www.gujaratindia.com/pdf/ser0708.pdf,
accessed October 29, 2010.
Government of Gujarat (2012) State profile. http://www.gujarat-
india.com/state-profile/demography.htm, accessed October 10,
2012.
574 © 2014 John Wiley & Sons Ltd
Tropical Medicine and International Health volume 19 no 5 pp 568–575 may 2014
P. Shah et al. Changing epidemiology of maternal mortality in rural India

Institute of research in medical statistics, Indian council of Medical
research (2003) Estimates of maternal mortality ratio in India
and its states: A pilot study, 2003 http://www.icmr.nic.in/final/
Final%20Pilot%20Report.pdf, accessed on 20 March 2013.
Jain A, Gupta SC, Misra SK et al. (2009) Trend and causes of
maternal mortality among women delivering in S. N. Medical
College Hospital, Agra. Indian Journal of Public Health 53,
47–48. PMID: 19806831.
Kumar R, Singh SK & Dikid T (2010) Maternal mortality trends
in India: has policy of promoting institutional delivery paid
off? Indian Journal of Medical Research 132, 458–459. PMID:
20966527.
Kutty VR, Shah P, Modi D et al. (2013) Reducing neonatal
mortality in Jhagadia block, Gujarat: we need to go beyond
promoting hospital deliveries. Journal of Tropical Pediatrics
59, 49–53. PMID: 22964552.
Mavalankar D, Singh A, Patel SR, Desai A & Singh PV (2009)
Saving mothers and newborns through an innovative partner-
ship with private sector obstetricians: Chiranjeevi scheme of
Gujarat, India. International Journal of Gynaecology and
Obstetrics 107, 271–276. PMID: 19846090.
Ministry of Health & Family Welfare (2005) Janani Suraksha
Yojana: Guidelines for Implementation. Government of India,
New Delhi, India.
Ministry of Health and Family Welfare (2010) District Level
Health and Facility Survey-3, 2007–08. http://www.gujhealth.
gov.in/Portal/Tender/1/3_dlhs2.pdf, accessed on 10 October,
2012.
Ministry of Health and Family Welfare (2012) Gujarat profile.
http://mohfw.nic.in/NRHM/State%20Files/gujarat.htm,
accessed on 10 October, 2012.
Ministry of statistics and programme implementation, Govern-
ment of India (2005) Millennium Development Goals: India
country report, 2005. http://www.unicef.org/india/
ssd04_2005_final.pdf, accessed on 20 March 2013.
National Rural Health Mission (2013) ASHA. Accredited Social
Health Activist. http://nrhm.gov.in/communitisation/asha/about
-asha.html, accessed 11 September 2013.
Office of Registrar General (2008) Maternal mortality in India:
1997–2003. Trends, causes, and risk factors. http://webdev.sil-
vertouch.com/GujHealth/pdf/maternal_mortal-
ity_in_india_1997-2003.pdf, accessed on 20 March 2013.
Office of Registrar General (2012) Maternal and child mortality
and total fertility rates, 2011. http://censusindia.gov.in/
vital_statistics/SRS_Bulletins/MMR_release_070711.pdf,
accessed 10 October, 2012.
R Core Team (2012) R: A language and environment for
statistical computing. R Foundation for Statistical Computing,
Vienna, Austria.
Ramanathan M (2009) Addressing the ‘third delay’ in maternal
mortality: need for reform. Indian Journal of Medical Ethics
6, 211–212. PMID: 19839550.
Ronsman C, Graham WJ (2006) Maternal mortality: who,
when, where, and why. Lancet 368, 1189–1200. PMID:
17011946.
Sample registration survey, Office of Registrar General (2012)
Special bulletin on maternal mortality in India 2007–2009.
Ministry of Home Affairs, Government of India, New Delhi.
http://www.censusindia.gov.in/vital_statistics/SRS_Bulletins/
Final-MMR%20Bulletin-2007-09_070711.pdf.
Sample registration system, Office of Registrar General (1998)
Statistical Report 1998. Ministry of Home Affairs, Govern-
ment of India, New Delhi, India.
Sample registration system, Office of Registrar General (2008)
Statistical Report 2008, Report No. 1. Ministry of Home
Affairs, Government of India, New Delhi, India.
Sample registration system, Office of Registrar General (2010)
Executive summary 2010. http://www.censusindia.gov.in/
vital_statistics/srs/Executive_Summary_2010.pdf, accessed on
12 October 2012.
Sample registration system, Office of Registrar General (2011)
Maternal and child mortality and total fertility rates, 2011.
http://censusindia.gov.in/vital_statistics/SRS_Bulletins/
MMR_release_070711.pdf. Accessed on 20 March 2013.
SEWA Rural (2011) Report on Family Centered Safe Motherhood
and Newborn Care Project. SEWA Rural, Jhagadia, India.
Sri BS, Sarojini N & Khanna R (2012) An investigation of
maternal deaths following public protests in a tribal district of
Madhya Pradesh, central India. Reproductive Health Matters
20, 11–20. PMID: 22789078.
StataCorp (2007) Stata Statistical Software: Release 10. Stata-
Corp LP, College Station, TX.
UNFPA and University of Aberdeen (2004) Maternal mortality
update 2004. Delivering in good hands. http://www.unfpa.org/
upload/lib_pub_file/381_filename_mmupdate05_eng21.pdf,
accessed on 10 October 2012.
United Nations (2012) The Millennium Development Goals
2012 Report. http://mdgs.un.org/unsd/mdg/Resources/Static/
Products/Progress2012/English2012.pdf, accessed 12 October,
2012.
WHO (1994) Verbal autopsies for maternal deaths: Report of a
WHO workshop, London, 10–13 January 1995. WHO, Gen-
eva.
WHO (2005) The World Health Report 2005: Make Every
Mother and Child Count. WHO, Geneva.
WHO/UNICEF/UNFPA/World Bank (2010) Trends in maternal
mortality: 1990 to 2008. WHO, Geneva. http://whqlibdoc.
who.int/publications/2010/9789241500265_eng.pdf.
Corresponding Author Pankaj Shah, SEWA-Rural, Jhagadia, Bharuch District, Gujarat 393110, India. Tel.: +91 2645 220021,
+91 9426120316; Fax +91 2645 220313; E-mail: [email protected]
© 2014 John Wiley & Sons Ltd 575
Tropical Medicine and International Health volume 19 no 5 pp 568–575 may 2014
P. Shah et al. Changing epidemiology of maternal mortality in rural India