-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
Bonus images for this chapter can be found online
athttp://www.expertconsult.com
Seborrheic Dermatitis, Psoriasis, RecalcitrantPalmoplantar
Eruptions, Pustular Dermatitis,and Erythroderma10
Seborrheic dermatitis
Clinical features
Seborrheic dermatitis is common, occurring in 25% of
thepopulation. It is a chronic, supercial, inammatory diseasewith a
predilection for the scalp, eyebrows, eyelids, nasolabialcreases,
lips, ears (Fig. 10-1), sternal area, axillae, submam-mary folds,
umbilicus, groins, and gluteal crease. The diseaseis characterized
by scaling on an erythematous base. The scaleoften has a yellow,
greasy appearance. Itching may be severe.
Dandruff (pityriasis sicca) represents a mild form of
seborrheicdermatitis. An oily type, pityriasis steatoides, is
accompaniedby erythema and an accumulation of thick crusts.
Other types of seborrheic dermatitis on the scalp
includearcuate, polycyclic, or petaloid patches, and psoriasiform,
exu-dative, or crusted plaques. The disease frequently
spreadsbeyond the hairy scalp to the forehead, ears,
postauricularregions, and neck. On these areas the patches have
convexborders and are reddish-yellow or yellowish. In
dark-skinnedindividuals, arcuate and petaloid lesions commonly
involvethe hairline. In extreme cases the entire scalp is covered
by agreasy, dirty crust with an offensive odor. In infants,
yellowor brown scaling lesions on the scalp, with accumulated
adher-ent epithelial debris, are called cradle cap.
Erythema and scaling are often seen in the eyebrows. The
lids may show yellowish-white, ne scales and faint erythema.The
edges of the lids may be erythematous and granular (mar-ginal
blepharitis), and the conjunctivae may be injected. If theglabella
is involved, ssures in the wrinkles at the inner endof the eyebrow
may accompany the ne scaling. In the naso-labial creases and on the
alae nasi, there may be yellowish orreddish-yellow scaling macules,
sometimes with ssures. Inmen, folliculitis of the beard area is
common.
In the ears, seborrheic dermatitis may be mistaken for
aninfectious otitis externa. There is scaling in the aural
canals,around the auditory meatus, usually with marked pruritus.The
postauricular region and skin under the lobe may beinvolved. In
these areas the skin often becomes red, ssured,and swollen. In the
axillae the eruption begins in the apices,bilaterally, and later
progresses to neighboring skin. This
pattern resembles that of allergic contact dermatitis to
deodor-ant, but differs from that of clothing dermatitis (which
involvesthe periphery of the axillae but spares the vault). The
involve-ment may vary from simple erythema and scaling to
morepronounced petaloid patches with ssures. The inframam-mary
folds and the umbilicus may be involved. The presternalarea is a
favored site on the trunk.
Seborrheic dermatitis is common in the groin and glutealcrease,
where its appearance may closely simulate tinea crurisor
candidiasis. In these areas, the appearance often overlapswith that
of inverse psoriasis. In fact, many of these patientshave an
overlap of the two conditions (sebopsoriasis or sebor-
rhiasis) in the groin, as well as the scalp. The lesions
mabecome generalized and progress to a generalized exfoerythroderma
(erythroderma desquamativum), especiainfants. A minority of these
infants will have evidenimmunosuppression. In adults, generalized
eruptions maccompanied by adenopathy and may simulate mycosigoides
or psoriatic erythroderma.
Seborrheic dermatitis may be associated with severalnal
diseases. Parkinsons disease is often accompanisevere refractory
seborrheic dermatitis involving the scaface, with waxy, profuse
scaling. A unilateral injury innervation of the face, or a stroke,
may lead to unilateral
ized seborrheic dermatitis. Patients with acquired immdeciency
syndrome (AIDS) have an increased incideseborrheic dermatitis. An
increased incidence has alsonoted in patients who are seropositive
for human immdeciency virus (HIV), but have not developed other
siclinical disease. Diabetes mellitus, especially in obese pesprue;
malabsorption disorders; epilepsy; neuroleptic such as haloperidol;
and reactions to arsenic and gold haproduced seborrheic
dermatitis-like eruptions.
Etiology and pathogenesis
The etiology of this common disorder is complex, but mrelated to
the presence of the lipophilic yeast Pityrosovale, which produces
bioactive indoles. The density ofhas been correlated with the
severity of the disease, and rtion of the yeast occurs with
response to therapy. P. ovaalso be abundant on the scalps of
patients who have no csigns of the disease, and the yeast may only
be pathogepredisposed individuals.
Patients with seborrheic dermatitis may show upreguof interferon
(IFN)-gamma, expressed interleukin expressed IL-1, and IL-4.
Expression of cytotoxicity-actiligands and recruitment of natural
killer (NK) cells havbeen noted.
Histology
The epidermis demonstrates regular acanthosis with
thinning of the suprapapillary plates. Varying degrspongiosis
and lymphocyte exocytosis are noted. A charistic nding is the
presence of a focal scale crust adjacthe follicular ostia.
Differential diagnosis
Some cases of seborrheic dermatitis bear a close clinical
rblance to psoriasis, and the two conditions may ovPsoriasis tends
to have more pronounced erythema and hsilvery scales that peel in
layers. Removal of scales in psomay disclose bleeding points
(Auspitz sign). This s
http://www.expertconsult.com/http://www.expertconsult.com/
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
Fig. 10-1Seborrheic dermatitis.
common but lacks great specicity. Severe itching favors
seb-orrheic dermatitis. Characteristic psoriasis elsewhere
(nailpitting, balanitis) may resolve the question. Impetigo of
thescalp, especially when associated with pediculosis, may
causedifculty in differentiation. Scalp impetigo can be an
indolentcrusted dermatosis associated with failure to thrive.
Langerhanscell histiocytosis may also resemble seborrheic
dermatitis, buttypically demonstrates yellowbrown perifollicular
papulesand groin ssuring. Crusted scabies of the scalp can also
beconfused with seborrheic dermatitis, and Trichophyton
ton-suransoften produces a subtle seborrheic scale. In subtle
casesof tinea, a moist gauze pad rubbed vigorously on the scalp
willtypically dislodge short, broken KOH-positive hairs. This canbe
the fastest way to make the diagnosis.
Treatment
Agents suitable for use on glabrous skin include
corticosteroidcreams, gels, sprays and foam. Corticosteroids tend
to producea rapid effect, but on the face even mid-potency
corticosteroidscan produce steroid rosacea. For this reason,
antifungal agentsand topical calcineurin inhibitors are often
preferred.Ketoconazole, ciclopirox, tacrolimus, zinc pyrithione,
andpimecrolimus preparations are all effective alone and in
com-bination. The antifungals are now available in a wide rangeof
vehicles to include foams, gels, and liquids. Bifonazoleshampoo has
been shown to be effective in treating infants andsmall children.
Topical calcineurin inhibitors may be associ-
ated with a burning sensation, especially on moist skin, andmay
produce ushing if patients consume alcohol. Patientsgenerally
tolerate these agents better after initial treatmentwith a
corticosteroid. An open, randomized, prospective, com-parative
study of topical pimecrolimus 1% cream vs topicalketoconazole 2%
cream found the two to be equally effective,but side effects were
somewhat more common with pime-crolimus. Preliminary studies
suggest oral itraconazole andoral terbinane may show some efcacy.
Oral uconazoleshowed marginal benet. Study results with topical
metroni-dazole have been mixed.
When secondary bacterial infection is present, a topical ororal
antibiotic may be required. In patients infected with HIV,
lithium succinate ointment (Efalith) has been used for
facdisease. Lithium gluconate 8% ointment has also been showto
compare favorably with ketoconazole 2% emulsion healthy adults and
was more effective in terms of control scaling and symptoms. Sodium
sulfacetamide products, wor without sulfur, are effective in some
refractory patients.
For scalp disease, selenium sulde, ketoconazole, tar,
zpyrithione, uocinolone, and resorcin shampoos are effectivIn many
patients, these agents may be used 23 times a wewith a regular
shampoo used in between as requireAntifungal foams and gels, as
well as corticosteroid solutiofoams, gels, and sprays, are often
preferred by Caucasipatients, while ointment or oil preparations
are preferred some black patients.
Itching of the external ear canal usually responds to a
topicorticosteroid, calcineurin inhibitors, or antifungals such
ketoconazole or ciclopirox. Some patients require the use oclass 1
corticosteroid on weekends to control refractory prutus.
Cortisporin otic suspension can bring about prompt cleing, but
contact dermatitis to neomycin may complicate tuse of some
Cortisporin products. Desonide otic lotion (0.0desonide and 2%
acetic acid) is also effective and may be bettolerated than
Domeboro otic solution.
Sodium sulfacetamide drops or ointment may be effectifor
seborrheic blepharitis. Oral tetracyclines can also be efftive, and
have been shown to decrease the density of micr
organisms in the affected follicles. Steroid preparations
asuitable for short-term use, but may induce glaucoma acataracts.
Daily gentle cleansing with a cotton-tipped applictor and baby
shampoo in water can reduce symptoms. severe cases, oral
antibiotics or oral antifungals may be cobined with topical
agents.
BerkT, et al:Seborrheic dermatitis. P.T. 2010 Jun;
35(6):348352.CmertA, et al:Efficacy of oral fluconazole in the
treatment ofseborrheic dermatitis: a placebo-controlled study. Am J
Clin Dermat2007; 8(4):235238.DawsonTLJr:Malassezia globosa
andrestricta: breakthroughunderstanding of the etiology and
treatment of dandruff andseborrheic dermatitis through whole-genome
analysis. J InvestigDermatol Symp Proc 2007; 12(2):1519.ElewskiB,
et al:Efficacy and safety of a new once-daily topicalketoconazole
2% gel in the treatment of seborrheic dermatitis: a pha
III trial. J Drugs Dermatol 2006; 5(7):646650.FiroozA, et
al:Pimecrolimus cream, 1%, vs hydrocortisone acetatecream, 1%, in
the treatment of facial seborrheic dermatitis: arandomized,
investigator-blind, clinical trial. Arch Dermatol
2006;142(8):10661067.Food and Drug Administration, HHS:Dandruff,
seborrheic dermatitis, anpsoriasis drug products containing coal
tar and menthol for over-thecounter human use; amendment to the
monograph. Final rule. FedRegist 2007; 72(43):98499852.GaitanisG,
et al:AhR ligands, malassezin, and indolo[3,2-b]carbazolare
selectively produced by Malassezia furfur strains isolated
fromseborrheic dermatitis. J Invest Dermatol 2008;
128(7):16201625.GeeBC:Seborrhoeic dermatitis. Clin Evid 2004;
12:2344.HighWA, et al:Pilot trial of 1% pimecrolimus cream in the
treatment seborrheic dermatitis in African American adults with
associatedhypopigmentation. J Am Acad Dermatol 2006;
54(6):10831088.
JacksonWB:Blepharitis: current strategies for diagnosis
andmanagement. Can J Ophthalmol 2008; 43(2):170179.KircikL:The
evolving role of therapeutic shampoos for targetingsymptoms of
inflammatory scalp disorders. J Drugs Dermatol 2010;9(1):4148.KocE,
et al:An open, randomized, prospective, comparative study otopical
pimecrolimus 1% cream and topical ketoconazole 2% cream
the treatment of seborrheic dermatitis. J Dermatolog Treat 2008;
1:1OzcanH, et al:Is metronidazole 0.75% gel effective in the
treatment oseborrhoeic dermatitis? A double-blind, placebo
controlled study. EuJ Dermatol 2007; 17(4):313316.SeckinD, et
al:Metronidazole 0.75% gel vs. ketoconazole 2% cream the treatment
of facial seborrheic dermatitis: a randomized, double-blind study.
J Eur Acad Dermatol Venereol 2007; 21(3):345350.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
190
SeborrheicDermatitis,
Psoriasis,
RecalcitrantPalmoplantarEruptions
10
Fig. 10-2 Psoriasis.
Fig. 10-3 Pustular psoriasis of the hand.
Fig. 10-4 Nail pitting and distal onycholysis in psoriasis.
ShemerA, et al:Treatment of moderate to severe facial
seborrheicdermatitis with itraconazole: an open non-comparative
study. Isr MedAssoc J 2008; 10(6):417418.SiadatAH, et al:The
efficacy of 1% metronidazole gel in facialseborrheic dermatitis: a
double blind study. Indian J Dermatol VenereolLeprol 2006;
72(4):266269.TajimaM, et al:Molecular analysis of
Malasseziamicroflora inseborrheic dermatitis patients: comparison
with other diseases andhealthy subjects. J Invest Dermatol 2008;
128(2):345351.VenaGA, et al:Oral terbinafine in the treatment of
multi-site seborrheicdermatitis: a multicenter, double-blind
placebo-controlled study. Int JImmunopathol Pharmacol 2005;
18(4):745753.WaldroupW, et al:Medicated shampoos for the treatment
of seborrheic
dermatitis. J Drugs Dermatol 2008; 7(7):699703.WarshawEM, et
al:Results of a randomized, double-blind, vehicle-controlled
efficacy trial of pimecrolimus cream 1% for the treatment
ofmoderate to severe facial seborrheic dermatitis. J Am Acad
Dermatol2007; 57(2):257264.
Psoriasis
Clinical features
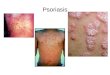
Psoriasis is a common, chronic, and recurrent inammatorydisease
of the skin characterized by circumscribed, erythema-tous, dry,
scaling plaques of various sizes. The lesions areusually covered by
silvery white lamellar scales. The lesionshave a predilection for
the scalp, nails, extensor surfaces of thelimbs, umbilical region,
and sacrum. The eruption is usuallysymmetrical. It usually develops
slowly but may be exanthema-tous, with the sudden onset of numerous
guttate (droplike)lesions (Fig. 10-2). Subjective symptoms, such as
itching orburning, may be present and may cause extreme
discomfort.
The early lesions are small erythematous macules, whichfrom the
beginning are covered with dry, silvery scales. Thelesions increase
in size by peripheral extension and coales-cence. The scales are
micaceous, meaning that they peel inlayers. They are looser toward
the periphery and adherentcentrally. When removed, bleeding points
appear (Auspitzsign). Although plaques typically predominate,
lesions may beannular or polycyclic. Old patches may be thick and
coveredwith tough lamellar scales like the outside of an oyster
shell
(psoriasis ostracea). Various other descriptive terms have inthe
past been applied to the diverse appearances of the
lesions:psoriasis guttata, in which the lesions are the size of
waterdrops; psoriasis follicularis, in which tiny, scaly lesions
arelocated at the orices of hair follicles; psoriasis gurata,
pso-riasis annulata, and psoriasis gyrata, in which curved
linearpatterns are produced by central involution; psoriasis
discoi-
dea, in which central involution does not occur andpatches
persist; and psoriasis rupioides, in which clesions occur,
resembling syphilitic rupia. The term cplaque psoriasis is often
applied to stable lesions of theand extremities. Inverse psoriasis
predominates in intenous areas. Pustular variants of psoriasis may
be chrothe palms and soles (Fig. 10-3), or may be eruptive and
apanied by severe toxicity and hypocalcemia.
Involved nails (Fig. 10-4) can demonstrate distal onlysis,
random pitting (the result of parakeratosis the proximal matrix),
oil spots (yellow areas of subuparakeratosis from the distal
matrix), or salmon p(nailbed psoriasis). Thick subungual
hyperkeratosisresemble onychomycosis.
Types
Seborrheic-like psoriasisSome cases of psoriasis overlap with
seborrheic dermSeborrheic lesions may predominate on the face,
und
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
4. oligoarthritis with swelling and tenosynovitis of one ofew
hand joints (70%)
5. ankylosing spondylitis alone or with peripheral
arthr(5%).
Most radiographic ndings resemble those in rheumatoarthritis,
but certain ndings are highly suggestive of psoriasThese include
erosion of terminal phalangeal tufts (acrostelysis), tapering or
whittling of phalanges or metacarpwith cupping of proximal ends of
phalanges (pencil in a cdeformity), bony ankylosis, osteolysis of
metatarsals, prediltion for distal interphalangeal and proximal
interphalang
joints, relative sparing of metacarpal phalangeal and metatsal
phalangeal joints, paravertebral ossication, asymmetrisacroiliitis,
and rarity of bamboo spine when the spineinvolved. Nearly half the
patients with psoriatic arthritis hatype human leukocyte antigen
(HLA)-B27.
Rest, splinting, passive motion, and nonsteroidal aninammatory
drugs (NSAIDs) may provide symptomarelief but do not prevent
deformity. Methotrexate, cyclosporitacrolimus, and biologic agents
are disease-modifying druthat prevent deformity.
Guttate psoriasisIn this distinctive form of psoriasis typical
lesions are the siof water drops, 25 mm in diameter. Lesions
typically occas an abrupt eruption following some acute infection,
such
a streptococcal pharyngitis. Guttate psoriasis occurs
mostlypatients under age 30. This type of psoriasis usually
responrapidly to broad-band ultraviolet (UV) B at erythemogedoses.
Suberythemogenic doses often have little impact on tlesions. This
is one of the few forms of psoriasis where broaband UVB may have an
advantage over narrow-band UVMinimal erythemogenic dose (MED)
testing is recommendto allow for appropriately aggressive
treatment. Recurrent esodes may be related to pharyngeal carriage
of the responsibstreptococcus by the patient or a close contact. A
course osemisynthetic penicillin (such as dicloxacillin, 250 mg
fotimes a day for 10 days) with rifampin (600 mg/day for adult) may
be required to clear chronic streptococcarriage.
Generalized pustular psoriasis (von Zumbusch)Typical patients
have had plaque psoriasis and often psoriaarthritis. The onset is
sudden, with formation of lakes of pperiungually, on the palms, and
at the edge of psoriaplaques. Erythema occurs in the exures before
the generized eruption appears. This is followed by a generalized
ethema and more pustules (Fig. 10-7). Pruritus and intenFig. 10-5
Penile psoriasis with erythema and silver scale.
Fig. 10-6Psoriatic arthritis.
breasts, and in the scalp, exures, and axillae. Lesions in
theseareas are moist and erythematous, with yellow, greasy,
softscales, rather than dry and micaceous scales. Terms such
assebopsoriasis and seborrhiasis may be used to describe
thecondition of such patients.
Inverse psoriasisThis form selectively and often exclusively
involves folds,recesses, and exor surfaces such as the ears,
axillae, groins,inframammary folds, navel, intergluteal crease,
penis (Fig.10-5), lips, and web spaces. Other areas, such as the
scalp andnails, may be involved.
Napkin psoriasisNapkin psoriasis, or psoriasis in the diaper
area, is character-istically seen in infants between 2 and 8 months
of age. Lesionsappear as brightly erythematous, sharply demarcated
patchesof skin involving much of the diaper area. The lesions
typicallyclear with topical therapy, but psoriasis may reappear
inadulthood.
Psoriatic arthritisFive clinical patterns of arthritis
occur:
1. asymmetrical distal interphalangeal joint involvementwith
nail damage (16%)
2. arthritis mutilans with osteolysis of phalanges and meta-
carpals (5%) (Fig. 10-6)3. symmetrical polyarthritis-like
rheumatoid arthritis, with
claw hands (15%)
Fig. 10-7Pustular psoriasis.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
192
SeborrheicDermatitis,
Psoriasis,
RecalcitrantPalmoplantarEruptions
10
burning are often present. Mucous membrane lesions arecommon.
The lips may be red and scaly, and supercial ulcera-tions of the
tongue and mouth occur. Geographic or ssuredtongue frequently
occurs (Fig. 10-8).
The patient is frequently ill with fever, erythroderma,
hypo-calcemia, and cachexia. A number of cases of acute
respiratorydistress syndrome associated with pustular and
erythroder-
mic psoriasis have been reported. Other systemic complica-tions
include pneumonia, congestive heart failure, andhepatitis.
Episodes are often provoked by withdrawal of systemic
cor-ticosteroids. The authors have also observed generalized
pus-tular psoriasis as the presenting sign of Cushings
disease.Other implicated drugs include iodides, coal tar,
terbinane,minocycline, hydroxychloroquine, acetazolamide, and
sali-cylates. There is usually a strong familial history of
psoriasis.Generalized pustular psoriasis may occur in infants and
chil-dren with no implicated drug. It may also occur as an
episodicevent punctuating the course of localized acral
pustularpsoriasis.
Acitretin is the drug of choice in this severe disease.
Theresponse is generally rapid. Isotretinoin is also effective.
Cyclosporine, methotrexate, and biologicals are
alternatives.Sometimes dapsone is effective in doses of 50100
mg/day.
Acrodermatitis continua of HallopeauTypical patients develop
acral erythematous plaques studdedwith pustules. The nailbeds are
heavily involved, and the n-gernails oat away on lakes of pus,
resulting in anonychia.Hyperkeratosis often ensues, and the
ngertips becomeincreasingly painful, tapering to long keratotic
points.Occasionally, patients may develop generalized pustular
ares(Fig. 10-9). Acrodermatitis continua is discussed in more
detailbelow.
Impetigo herpetiformisThis term has been applied to generalized
pustular psoriasis
of pregnancy. Flexural erythema, studded with pustules,
oftenoccurs initially, followed by a generalized pustular are
andincreasing toxicity. As the patients are pregnant,
systemicretinoids are not appropriate. Many patients only respond
todelivery, and early delivery should be strongly considered assoon
as it is safe for the infant. Alternatively, patients mayrespond to
prednisone at a dose of 1 mg/kg/day. The cortico-steroid can also
contribute to neonatal lung maturity.
Keratoderma blennorrhagicum (Reiter syndrome)Keratoderma
blennorrhagicum resembles psoriasis both histo-logically and
clinically, except for its tendency for thicker kera-
Fig. 10-8 Geographic tongue in pustular psoriasis.
Fig. 10-9 Generalized pustular flare in a patient with
acrodermcontinua.
Fig. 10-10Erythrodermic psoriasis.
totic lesions. Patients are often positive for HLA-B2develop
reactive arthritis and skin disease after a bout othritis or
enteritis.
Erythrodermic psoriasis
Patients with psoriasis may develop a generalized erderma (Fig.
10-10). Erythrodermic psoriasis is covergreater detail under
exfoliative dermatitis.
Course
The course of psoriasis is unpredictable. It usually begthe
scalp or elbows, and may remain localized in the orregion for
years. Chronic disease may also be almost enlimited to the
ngernails. Involvement over the sacrumeasily be confused with
candidiasis or tinea. Onset mabe sudden and widespread.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
Two of the chief features of psoriasis are its tendency torecur
and its persistence. The isomorphic response (Koebnerphenomenon) is
the appearance of typical lesions of psoriasisat sites of even
trivial injury (Fig. 10-11). Lesions may occur atsites of
scratches, incisions, and burns. Lesions may rstappear after a
viral exanthema or following pityriasis rosea.The isomorphic
response may occur if psoriatic lesions areseverely burned during
phototherapy. With a reduction inlight dosage, the erythema and
burning resolve, and theplaques begin to clear. Woronoffs ring is
concentric blanchingof the erythematous skin at or near the
periphery of a healingpsoriatic plaque. It is often the rst sign
that the patientspsoriasis is responding to phototherapy.
The palms and soles are sometimes exclusively affected,showing
discrete erythematous dry scaling patches, circum-scribed verrucous
thickenings, or pustules on an erythematousbase. The patches
usually begin in the mid-portions of thepalms or on the soles, and
gradually expand. Psoriasis of thepalms and soles is typically
chronic and extremely resistant totreatment.
Many studies report an association between hepatitis C
andpsoriasis, and hepatitis C has also been implicated in
psoriaticarthritis. If treatment of psoriasis is to include a
potentiallyhepatotoxic drug, such as methotrexate, a hepatitis C
serologyshould be obtained. It should also be noted that
interferontreatment of the hepatitis can further exacerbate or
inducepsoriasis. Anti-tumor necrosis factor (TNF)- therapy
showspromise in the treatment of psoriasis, even in the setting
of
chronic hepatitis C infection.
Inheritance
In a large study of psoriasis in monozygotic twins,
heritabilitywas high and environmental inuence low. Patients with
pso-riasis often have relatives with the disease, and the
incidencetypically increases in successive generations.
Multifactorialinheritance is likely. Analysis of population-specic
HLA hap-lotypes has provided evidence that susceptibility to
psoriasisis linked to the class I and II major histocompatibility
complex(MHC) on human chromosome 6. A number of genetic loci
are
Fig. 10-11 Koebner phenomenon in psoriasis.
linked to psoriasis, including PSORS1on chromosome 6 awithin the
MHC, and PSORS2on chromosome 17q. It has abeen shown that there are
two subsets that differ in ageonset and in the frequency of HLA
associations. Early onsetype I psoriasis and is associated mostly
with Cw6, B57, aDR7. Late onset is type II and this predominantly
featurCw2. PSORS9has also been conrmed as a susceptibility locfor
psoriasis.
A variety of other HLA associations have been reportedis
believed that any individual who has B13 or B17 carrieve-fold risk
of developing psoriasis. In pustular psoriaHLA-B27 may be seen,
whereas B13 and B17 are increasedguttate and erythrodermic
psoriasis. In palmoplantar pustusis, there is an association with
HLA-B8, Bw35, Cw7, and DRHLA typing is a research tool for
population-based studibut is of limited value in assessing an
individual patient.
Epidemiology
Psoriasis occurs with equal frequency in both sexes. Betwe1 and
2% of the US population has psoriasis. It occurs lfrequently in the
tropics. It is less common in North Americand West African black
persons. Native Americans and natFijians rarely have psoriasis. The
onset of psoriasis is at a meage of 27 years, but the range is
wide, from the neonatal perito the seventies. Severe emotional
stress tends to aggrav
psoriasis in almost half of those studied.In pregnancy there is
a distinct tendency for improveme
or even temporary disappearance of lesions in the majorof women
studied. After childbirth there is a tendenfor exacerbation of
lesions. Paradoxically, pregnancy is athe milieu for impetigo
herpetiformis, and psoriasis mbehave differently from one pregnancy
to another in the sampatient.
A high prevalence of celiac disease has been noted in patienwith
psoriasis. Lymphoma also has an increased incidencethese patients,
and psoriasis has been linked to the metabosyndrome and a higher
risk of cardiovascular disease.
Pathogenesis
Psoriasis is a hyperproliferative disorder, but the
proliferatiis driven by a complex cascade of inammatory
mediatoPsoriasis appears to represent a mixed T-helper (Th)1 aTh17
inammatory disease. Th17 cells appear to be more proimal in the
inammatory cascade. T cells and cytokines plpivotal roles in the
pathophysiology of psoriasis. Overexpressiof type 1 cytokines, such
as IL-2, IL-6, IL-8, IL-12, IFN-aTNF-, has been demonstrated, and
overexpression of ILleads to the accumulation of neutrophils. The
main signal Th1 development is IL-12, which promotes intracellular
IFNproduction. In animal models, shifting from Th1 to Tresponses
improves psoriasis. IL-4 is capable of inducing Tresponses and
improving psoriasis. Reduced expression of tanti-inammatory
cytokines IL-1RA and IL-10 has been foun
and polymorphisms for IL-10 genes correlate with psoriasIL-10 is
a type 2 cytokine with major inuences on immunregulation,
inhibiting type 1 proinammatory cytokine pduction. Patients on
established traditional therapies shorising levels of IL-10 mRNA
expression, suggesting that IL-may have antipsoriatic capacity.
The response to biologic agents has demonstrated that
CDlymphocytes, CD-11a and TNF-are important in the pathgenesis of
psoriasis. IL-15 triggers inammatory cell recrument, angiogenesis,
and production of inammatory cytokinincluding IFN-, TNF-, and
IL-17, all of which are upreglated in psoriatic lesions. The
interplay is complex, but IL-
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
194
SeborrheicDermatitis,
Psoriasis,
RecalcitrantPalmoplantarEruptions
10appears to be proinammatory, while IL-22 may serve toretard
keratinocyte differentiation. IL-23 stimulates survival,as well as
proliferation of Th17 cells. Circulating NK cells arereduced in
psoriasis.
Specic targets for therapy include TNF-,
leukocytefunction-associated antigen-1 (LFA-1)/intercellular
adhesionmolecule-1 (ICAM-1) binding, and LFA-3/CD2 binding. AnIL-15
monoclonal antibody has been shown to be effective ina mouse model
of psoriasis.
StreptococciStreptococci play a role in some patients. Patients
with psoria-sis report sore throat more often than controls.
Beta-hemolyticstreptococci of Lanceeld groups A, C, and G can cause
exac-erbation of chronic plaque psoriasis. Th1 cells recognize
cell-wall extract isolated from group A streptococci. HLA
variationhas a signicant effect on the immune response to group
Astreptococci.
StressVarious studies have shown a positive correlation
betweenstress and severity of disease. In almost half of patients
studied,stress appears to play a signicant role.
Drug-induced psoriasisPsoriasis may be induced by -blockers,
lithium, antimalarials,
terbinane, calcium channel blockers, captopril,
glyburide,granulocyte colony-stimulating factor, interleukins,
interfer-ons, and lipid-lowering drugs. Systemic steroids may
causerebound or pustular ares. Antimalarials are associated
witherythrodermic ares, but patients traveling to
malaria-endemicregions should take appropriate prophylaxis. Often,
drugssuch as doxycycline or meoquine are appropriate for
thegeographic area, but when a quinine derivative offers the
bestprotection, it is generally better to take the prophylactic
dosesof a quinine derivative than to risk disease and
full-dosetreatment.
Pathology
Histologically, all psoriasis is pustular. The microscopic
pus-tules include spongiform intraepidermal pustules, and
Munromicroabscesses within the stratum corneum. In early
guttatelesions, focal parakeratosis is noted within the
stratumcorneum. The parakeratotic focus typically has an
outlineresembling a childs rendition of a seagull. Neutrophils
aregenerally noted immediately above the focus of parakeratosis,but
in some sections, the neutrophils will not be visible as aresult of
sampling error. In plaque psoriasis, neutrophilic fociare so
numerous that they are rarely missed. Neutrophilicmicroabscesses
are generally present at multiple levels in thestratum corneum,
usually on top of small foci of parakeratosis.These foci generally
alternate with areas of orthokeratoticstratum corneum, suggesting
that the underlying spongiformpustules arise in a rhythmic fashion.
The granular layer is
absent focally, corresponding to areas producing foci of
para-keratosis. In well-developed plaques, there is regular
epider-mal acanthosis with long, bulbous rete ridges, thinning
overthe dermal papillae, and dilated capillaries within the
dermalpapillae. The last two ndings correlate with the Auspitz
sign.The stratum corneum may be entirely parakeratotic but
stillshows multiple small neutrophilic microabscesses at
varyinglevels. Spongiosis is typically scant, except in the area
imme-diately surrounding collections of neutrophils.
In pustular psoriasis, geographic tongue, and Reiter syn-drome,
intraepidermal spongiform pustules tend to be muchlarger. Grossly
pustular lesions often have little associated
acanthosis. In Reiter syndrome, the stratum corneum ismassively
thickened, with prominent foci of neutrophils parakeratosis,
alternating with orthokeratosis.
Acral lesions often demonstrate nondiagnostic featurtologically.
Spongiosis is typically prominent in these land often leads to a
differential diagnosis of psoriachronic psoriasiform spongiotic
dermatitis. Foci of neutroften contain serum and may be interpreted
as impetigcrusting.
On direct immunouorescence testing, the stratum cordemonstrates
intense uorescence with all antibodies, coment, and brin. This
uorescence may be partially indeent of the uorescent label, as it
has been noted in hematand eosin (H&E)-stained sections and
frozen unstainetions. The same phenomenon of stratum corneum
autocence has been noted in some cases of candidiasidemonstrate a
psoriasiform histology.
Psoriasis can generally be distinguished from dermatthe paucity
of edema, the relative absence of spongiostortuosity of the
capillary loops, and the presence otrophils above foci of
parakeratosis. Neutrophils in the stcorneum are commonly seen in
tinea, impetigo, candiand syphilis, but rarely are found atop
parakeratosis alting with orthokeratosis in a rhythmic fashion. In
psoriassyphilis the rete are typically long and slender, a
vainterface dermatitis is commonly present, dermal blood v
appear to have no lumen because of endothelial swellinplasma
cells are present in the dermal inltrate. Abouthird of biopsies of
syphilis lack plasma cells, but the reing characteristics still
suggest the correct diagPsoriasiform lesions of mycosis fungoides
exhibit epidtropism of large lymphocytes with little spongiosis.
Thephocytes are typically larger, darker, and more angulatethe
lymphocytes in the dermis. There is associated papdermal brosis,
and the supercial perivascular inltrasymmetrically distributed
around the postcapillary vefavoring the epidermal side (bare
underbelly sign).
Clinical differential diagnosis
Psoriasis must be differentiated from dermatomyositis,
erythematosus, seborrheic dermatitis, pityriasis rosea, planus,
eczema, and psoriasiform syphilid. The distribupsoriasis is on the
extensor surfaces, especially of the eand knees, and on the scalp;
dermatomyositis sharedistribution, whereas lupus erythematosus
generallyinvolvement of the extensor surfaces. Patients with
dermyositis may exhibit a heliotrope sign, atrophy, poikilodand
nailfold changes. Advanced lesions of discoid luputhematosus often
demonstrate follicular hyperkeratosis (tack sign). Seborrheic
dermatitis has a predilection foeyebrows, nasolabial angle, ears,
sternal region, and eThe scales in psoriasis are dry, white, and
shiny, whereasin seborrheic dermatitis are greasy and yellowish. On
reof the scales in psoriasis there is an oozing of blood
frocapillaries (Auspitz sign), whereas this does not occur i
orrheic dermatitis.In pityriasis rosea the eruption is located
on the upper
trunk, and thighs, and the duration is a matter of wLesions are
typically oval and follow skin tension Individual lesions show a
crinkling of the epidermis anlarette scaling. A herald patch is
frequently noted. Lplanus chiey affects the exor surfaces of the
wristankles. Often the violaceous color is pronounced. In dskinned
individuals, the lesions have a tendency tonounced
hyperpigmentation. The nails are not pittedpsoriasis, but
longitudinally ridged, rough, and thickPterygium formation is
characteristic of lichen planus.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmopla
Hand eczema may resemble psoriasis. In general, psoriaticlesions
tend to be more sharply marginated, but at times thelesions are
indistinguishable. Psoriasiform syphilid has inl-trated
copper-colored papules, often arranged in a guratepattern.
Serologic tests for syphilis are generally positive, butprozone
reactions may occur, and the serum may have to bediluted in order
to obtain a positive test. Generalized lymph-adenopathy and mucous
patches may be present.
Treatment
Topical therapy is generally suitable for limited
plaques.Localized treatments, such as the excimer laser or other
formsof intense pulsed light, may be suitable for limited
plaques.Phototherapy remains highly cost-effective for
widespreadpsoriasis. Cyclosporine has a rapid onset of action, but
is gen-erally not suitable for sustained therapy. Methotrexate
remainsthe systemic agent against which others are compared.
Biologicagents can produce dramatic responses at dramatic
expense.Rotating therapeutic agents that have varying toxicities
haveconceptual appeal, and combination therapy may reduce tox-icity
and reduce the incidence of neutralizing antibodies toagents such
as iniximab. Attention should be paid to comor-bidities including
metabolic syndrome, cardiac risk, and jointmanifestations.
Topical treatmentCorticosteroidsTopical application of
corticosteroids in creams, ointments,lotions, foams, and sprays is
the most frequently prescribedtherapy for psoriasis. Class I
steroids are suitable for 2-weekcourses of therapy on most body
areas. Therapy can be con-tinued with pulse applications on
weekends to reduce theincidence of local adverse effects. On the
scalp, corticosteroidsin propylene glycol, gel, foam, and spray
bases are preferredby most white patients. Black patients may nd
them drying,and may prefer oil and ointment preparations. Low to
mid-strength creams are preferred in the intertriginous areas andon
the face. To augment effectiveness of topical corticosteroidsin
areas with thick keratotic scale, the area should be hydrated
prior to application, and covered with an occlusive dressingof a
polyethylene lm (Saran wrap) or a sauna suit.Unfortunately, there
is typically a rapid recurrence of diseasewhen topical
corticosteroid therapy is discontinued. Sideeffects include
epidermal atrophy, steroid acne, miliaria, andpyoderma.
Intralesional injections of triamcinolone are helpful
forrefractory plaques. Triamcinolone acetonide (Kenalog)
sus-pension, 10 mg/mL, may be diluted with sterile saline to makea
concentration of 2.55 mg/mL. Good results are also obtainedin the
treatment of psoriatic nails by injecting triamcinoloneinto the
region of the matrix and the lateral nailfold. A digitalblock can
be performed prior to injection to provide anesthe-sia. Injections
are given once a month until the desired effectis achieved.
TarsCrude coal tar, and tar extracts such as liquor
carbonisdetergens, can be compounded into agents for topical
use.Tar bath oils and shampoos are readily available. Oil of
cade(pine tar) or birch tar in concentrations of 510% may also
beincorporated into ointments. The odor of all tars may
beoffensive.
AnthralinAnthralin is effective, but is irritating and stains
skin, clothing,and bedding. To avoid these drawbacks, short-contact
anthra-
lin treatment (SCAT) can be helpful, with anthralin washed after
1530 min. In warmer climates, SCAT is often done odoors to keep the
mess out of the house. Anthralin exertsdirect effect on
keratinocytes and leukocytes by suppressineutrophil superoxide
generation and inhibiting monocyderived IL-6, IL-8, and TNF-.
TazaroteneTazarotene is a nonisomerizable retinoic acid
receptor-speciretinoid. It appears to treat psoriasis by modulating
keratincyte differentiation and hyperproliferation, as well as by
su
pressing inammation. Combining its use with a topicorticosteroid
and weekend pulse therapy can decreairritation.
CalcipotrieneVitamin D3affects keratinocyte differentiation
partly throuits regulation of epidermal responsiveness to
calciuTreatment with the vitamin D analog calcipotriene (Dovonein
ointment, cream, or solution form has been shown to very effective
in the treatment of plaque-type and scalp priasis. Combination
therapy with calcipotriene and higpotency steroids may provide
greater response rates, fewside effects, and steroid-sparing.
Calcipotriene is unstablethe presence of many other topical agents
and degrades in tpresence of UV light. Monitoring of serum calcium
levels
adults is not required. Calcipotriene plus
betamethasodipropionate (Taclonex) is more effective than either
agealone.
Macrolactams (calcineurin inhibitors)Topical macrolactams such
as tacrolimus and pimecrolimare especially helpful for thin lesions
in areas prone to atropor steroid acne. The burning commonly
associated with theagents can be problematic, but may be avoided by
prior trement with a corticosteroid, and by application to dry
skrather than after bathing.
Salicylic acidSalicylic acid is used as a keratolytic agent in
shampo
creams, and gels. It can promote the absorption of other
topiagents. Widespread application may lead to salicylate
toxicmanifesting with tinnitus, acute confusion, and
refractohypoglycemia, especially in patients with diabetes and
thowith compromised renal function.
Ultraviolet lightPhototherapy is a cost-effective and
underutilized modalfor psoriasis. In most instances sunlight
improves psoriasHowever, severe burning of the skin may cause the
Koebnphenomenon and an exacerbation. Articial UVB lightproduced by
uorescent bulbs in broad-band or narrow-baspectrums. Maximal effect
is usually achieved at MEDAlthough suberythemogenic doses can be
effective, tresponse is slower than with erythemogenic regimens.
W
treatment, a tanning response occurs, and the dose must
increased to maintain efcacy. Maintenance UVB photothapy after
clearing contributes to the duration of remission ais justied for
many patients.
Using a monochromator, it has been shown that wavlengths of 254,
280, and 290 nm are ineffective; at 296, 300, 3and 313 nm there is
clearing. Narrow-band UVB (peak emsion around 311 nm) has been
shown to be more effectivetreating psoriasis than broad-band UVB.
Erythemogenic doare not required in order to achieve a response.
The responrates are better than 70% and close to those achievable
wPUVA therapy.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
196
SeborrheicDermatitis,
Psoriasis,
RecalcitrantPalmoplantarEruptions
10Goeckerman techniqueThe Goeckerman technique remains an
effective and cost-effective method of treatment. In its modern
form, a 25% tarpreparation is applied to the skin, and a tar bath
is taken atleast once a day. The excess tar is removed with mineral
orvegetable oil, and UV light is given. In psoriasis
daycarecenters, patients clear in an average of 18 days, and
75%remain free of disease for extended periods. The addition of
atopical corticosteroid to the Goeckerman regimen shortens thetime
required for remission. Phototoxic reactions (tar smarts)may occur
as a result of UVA generated by the predominantly
UVB bulbs.
Ingram techniqueThe Ingram technique consists of a daily coal
tar bath in asolution such as 120 mL liquor carbonis detergens to
80 L ofwarm water. This is followed by daily exposure to UV
lightfor increasing periods. An anthralin paste is then applied
toeach psoriatic plaque. Talcum powder is sprinkled over thelesions
and stockinette dressings are applied. Modern versionsof the
technique employ SCAT.
PUVA therapyHigh-intensity longwave UV radiation (UVA) given 2 h
afteringestion of 8-methoxypsoralen (Oxsoralen-Ultra), twice aweek,
is highly effective, even in severe psoriasis. Most patientsclear
in 2025 treatments, but maintenance treatment is needed.
Although PUVA therapy is highly effective, in patients withless
than 50% of the skin surface affected, UVB may be as
good.Polyethylene sheet bath PUVA is another therapeutic
alterna-tive to oral psoralen-UVA. The patient is immersed in a
psor-alen solution contained in plastic sheeting that conforms to
thepatients body.
Oral psoralen can produce cataracts, and protective eyewearmust
be used. PUVA therapy is a risk factor for skin cancer,including
squamous cell carcinoma and melanoma. Arsenicexposure is a more
signicant cofactor than prior exposure tomethotrexate, UVB, or
concomitant use of topical tar. Mentreated without genital
protection are at an increased risk ofdeveloping squamous cell
carcinomas of the penis and
scrotum. Although the risk of cancer is dose-related, there isno
denitive threshold dose of cumulative PUVA exposureabove which
carcinogenicity can be predicted.
Surgical treatmentIn patients with pharyngeal colonization by
streptococci, anexcellent response has been reported after
tonsillectomy. Moreeffective antibiotic regimens, such as a 10-day
course ofdicloxacillin combined with rifampin (600 mg/day for
anadult), have largely replaced tonsillectomy.
HyperthermiaLocal hyperthermia can clear psoriatic plaques, but
relapse isusually rapid. Microwave hyperthermia may produce
signi-cant complications, such as pain over bony prominences
andtissue destruction.
Occlusive treatmentOcclusion with surgical tape or dressings can
be effective asmonotherapy or when combined with topical drugs.
Systemic treatment
CorticosteroidsThe hazards of the injudicious use of systemic
corticosteroidsmust be emphasized. There is great risk of rebound
orinduction of pustular psoriasis when therapy is stopped.
Corticosteroid use is generally restricted to unique cistances,
such as impetigo herpetiformis when expeddelivery is not
possible.
MethotrexateThis folic acid antagonist remains the standard
against other systemic treatments are measured. Methotrexategreater
afnity for dihydrofolic acid reductase than haacid. The indications
for the use of methotrexate includriatic erythroderma, psoriatic
arthritis, acute pustular psis (von Zumbusch type), or widespread
body sinvolvement. Localized pustular psoriasis or palmoppsoriasis
that impairs normal function and employmenalso require systemic
treatment.
It is important to make sure that the patient has no hof liver
or kidney disease. Methotrexate can be toxic liver and decreased
renal clearance can enhance toxicity.important factors to consider
are alcohol abuse, cryptocirrhosis, severe illness, debility,
pregnancy, leukothrombocytopenia, active infectious disease,
immunciency, anemia, colitis, and ability to comply with
direcHepatic enzymes, bilirubin, serum albumin, creatinineline
phosphatase, complete blood count (CBC), platelet hepatitis
serology (B and C), HIV antibody, and urinshould all be evaluated
before starting treatment. Patienthypoalbuminemia have a higher
risk of developing p
nary complications.The need for liver biopsy remains
controversial. Bionot without risks and is not commonly performed
setting of methotrexate therapy for rheumatic dHowever, patients
with psoriasis have a greater risk odisease than other patient
populations. In most patientno risk factors for liver disease, the
rst liver biopsy ismonly obtained at approximately 1.01.5 g of
cumumethotrexate and repeated every subsequent 1.52.0 g utotal of
4.0 g is reached. The frequency then changes to1.01.5 g cumulative
intervals. These recommendatiolikely to change as more data are
evaluated. Weekly counts and monthly liver enzyme assessment are
rmended at the onset of therapy or when the dosage is chaMonitoring
of aminoterminal procollagen III peptide an
abolic panels that predict the risk of brosis (NASH Fibrmay
reduce the need for liver biopsy.
Numerous treatment schedules have evolved. The aurecommend
either three divided oral doses (12 h apart) wweekly single doses
orally, or single weekly subcutainjections. The weekly dose varies
from 5 mg to more50 mg, with most patients requiring 1530 mg a
week. Osingle dose exceeds 25 mg, oral absorption is unprediand
subcutaneous injections are recommended. Middoses can result in
severe toxicity and must be avoOral or cutaneous ulceration may be
a sign that the phas taken a mid-week dose. Oral folic acid has
been repto decrease side effects, especially nausea, and do14
mg/day are used. Oral folic acid is not adequathe treatment of
overdosage and leukovorin must be u
such cases.
CyclosporineThe therapeutic benet of cyclosporine in psoriatic
dmay be related to downmodulation of proinammepidermal cytokines.
The microemulsion formulation Nhas greater bioavailability and is
now standard. Do25 mg/kg/day generally produce rapid clearing of
psoUnfortunately, the lesions recur rapidly as well, and tranto
another form of therapy is required. Treatment duratiup to 6 months
are associated with a low incidence ofcomplications, but blood
pressure and serum creatinine
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
be monitored and doses adjusted accordingly. Usually, thedose is
reduced if the baseline creatinine increases byone-third.
DietThe anti-inammatory effects of sh oils rich in n-3
polyun-saturated fatty acids have been demonstrated in
rheumatoidarthritis, inammatory bowel disease, psoriasis, and
asthma.n-3 and n-6 polyunsaturated fatty acids affect a variety
ofcytokines, including IL-1, IL-6, and TNF. Herbal remedieshave
also been used with variable effects. Many of theseproducts are
unpalatable, and their efcacy does not comparefavorably to
pharmacologic agents.
Oral antimicrobial therapyThe association of streptococcal
pharyngitis with guttate pso-riasis is well established.
Staphylococcus aureusand streptococcisecrete exotoxins that act as
superantigens, producing massiveT-cell activation. Oral antibiotic
therapy for patients with pso-riasis infected with these organisms
is imperative. The efcacyof antimicrobial agents in other subsets
of psoriasis is unclear.Oral bile acid supplementation has been
shown to improvepsoriasis, presumably by affecting the microora and
endotox-ins in the gut. Oral ketoconazole, itraconazole, and other
anti-biotics have shown efcacy in a limited number of patientswith
psoriasis.
RetinoidsOral treatment with the aromatic retinoid ethylester,
etreti-nate, was effective in many patients with psoriasis,
especiallyin pustular disease. Because of its long half-life, the
drug hasbeen replaced by acitretin. Alcohol ingestion can
convertacitretin to etretinate and is strongly discouraged.
13-Cis-retinoic acid can also produce good results in some
patientswith pustular psoriasis. All of these drugs are potent
tera-togens and elevations in triglycerides may complicate
therapy.Combinations of retinoic acids with photochemotherapy canbe
effective in chronic plaque psoriasis, resulting in
loweredcumulative doses of light.
Dapsone
Dapsone use is limited largely to palmoplantar pustulosis
orother variants of pustular psoriasis. Even in this setting, it is
asecond- or third-line agent with limited efcacy.
Biologic agentsA number of biologic agents are available that
can producedramatic responses in some patients with psoriasis; all
areexpensive. Three agents block TNF-. Iniximab is a
chimericmonoclonal antibody to TNF-and requires intravenous
infu-sion; etanercept is a fusion protein of human TNF type
IIreceptor and the Fc region of IgG1; and adalimumab is
arecombinant, fully human IgG1 monoclonal antibody to TNF-.
Alefacept is a fusion protein of the external domain ofLFA-3 and
the Fc region of IgG1; it blocks T-cell activation andtriggers
apoptosis of pathogenic T cells. Efalizumab, a human-
ized monoclonal antibody to the CD11a portion of LFA-1, hasbeen
withdrawn from the market. Ustekinumab, a humanmonoclonal antibody
against IL-12 and 23, is the rst of a newclass of agents that
appear highly effective. They block theinammatory pathway at a more
proximal point than TNFagents. Neutralizing antibodies may decrease
the effectivenessof many of the biologic agents.
Percentage of patients clearing with each drugPublished data
allow for various comparisons between bio-logic agents, but as
trials are designed by the manufacturerto demonstrate the efcacy of
the agent, the endpoints of some
trials differ. In controlled trials of iniximab, the percentaof
patients reaching at least 75% improvement from baseliin the
psoriasis area and severity index (PASI 75) at weekis about 70%
with iniximab 3 mg/kg and 90% with 5 mkg, as compared to 6% with
placebo. About 35% of patienreceiving etanercept, 25 mg
subcutaneously twice a weachieve PASI 75 at 12 weeks and 45% at 24
weeks. With t50 mg induction dose administered twice a week, about
46of patients achieve PASI 75 at 12 weeks and 50% at 24 weeAbout
14% of patients receiving 12 weekly intramuscular intravenous
injections of alefacept will achieve PASI 75, aabout 38% PASI 50.
After two 12-injection courses, about 26of patients reach PASI 75
and 55% PASI 50. The onset of actiis somewhat slower than with
other agents, but ultimate cleing can be excellent. The data
available suggest that abo53% of patients taking 40 mg of
adalimumab every othweek achieve PASI 75 by week 12, and about 80%
of thotaking 40 mg a week achieve PASI 75. An analysis of 24
radomized controlled trials including 9384 patients suggestthat
iniximab was superior to the other agents studied, athat adalimumab
was superior to etanercept, 50 mg twweekly, and cyclosporine.
Ustekinumab was included in tstudy.
A phase III, parallel, double-blind, placebo-controlled stuof
ustekinumab for moderate to severe psoriasis (45 mg 90 mg at weeks
0 and 4, and then every 12 weeks) show
that 67.1% of those who received 45 mg and 66.4% receivi90 mg
achieved PASI 75 at week 12. In a second multicentphase III,
double-blind, placebo-controlled trial of ustekinmab in patients
with moderate to severe psoriasis, 66.7%patients receiving 45 mg
and 75.7% receiving 90 mg achievPASI 75.
Rapidity of clearing and relapseThe effects of iniximab are
rapid and similar to those achievwith cyclosporine. In contrast to
cyclosporine, clinical improvment after three intravenous infusions
of iniximab maintained for as long as 6 months in approximately
hthe patients. Adalimumab is also rapid in onset, with mapatients
demonstrating a response within the rst week treatment. About 15%
of patients treated with alefacept w
maintain benets for more than 6 months.
RisksTNF agents may induce ares of psoriasis through upregution
of plasmacytoid dendritic cells. This may be a class effeThe
biologic agents all suppress the normal immune responIniximab has
been associated with reactivation of tubercusis, demyelinating
disease, and serious systemic opportunisinfection. It may also lose
its effect because of neutraliziantibodies. Methotrexate or
azathioprine may be needed concomitant therapy to reduce the
incidence of neutraliziantibodies and infusion reactions. Even
though adalimumis a fully human antibody, it may also induce an
antiboresponse. Serious infections have been reported in patiewith
rheumatoid arthritis treated with this agent. Etanerce
has been associated with infection, onset, or
exacerbationmultiple sclerosis, vasculitis, and lupus
erythematosus-lmanifestations. All these manifestations are rare,
and may nbe statistically increased from the general population. A
sin12-week course of alefacept does not appear to impair primaor
secondary antibody responses to a neoantigen or memoresponses to a
recall antigen, but roughly 10% of patients hato interrupt therapy
because CD4 counts fall below 250/mmand CD4 counts must be
monitored with this agent. Manythe reported complications, such as
lymphoma, demyelinatidisease, and infection, are not unique to any
one bioloagent.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
198
SeborrheicDermatitis,
Psoriasis,
RecalcitrantPalmoplantarEruptions
10The National Psoriasis Foundation has endorsed a recom-
mendation that all patients be screened for latent
tuberculosisinfection prior to any immunologic therapy. They
recommenddelaying immunologic therapy until prophylaxis for
latenttuberculosis infection is completed, although they note
thatpatients with severe disease may be treated after 12 monthsof
prophylaxis. IFN- assays have greater specicity thantuberculin skin
tests and are being used along with imagingstudies to conrm
tuberculosis in patients with positive skintests.
Combination therapyIn more severe forms of psoriasis a
combination of treatmentmodalities may be employed. In treating
patients with metho-trexate, for example, concomitant topical
agents may be usedto minimize the dose. Methotrexate has been
combined withiniximab to reduce the incidence of neutralizing
antibodies,and has been used with acitretin in managing patients
withsevere, generalized pustular psoriasis. The use of PUVA
andretinoids is called Re-PUVA and has been studied
extensively.Acitretin has been combined with biologic agents to
treatrefractory psoriasis. Combination systemic therapy has
thepotential to reduce overall toxicity if the toxicities of
eachagent are different. However, new regimens should be usedwith
caution because the potential for cumulative toxicity ordrug
interaction exists.
Alternative therapiesAlternative therapies for psoriasis include
mycophenolatemofetil, sulfasalazine, paclitaxel, azathioprine,
fumaricacid esters, climatotherapy, and Grenz ray therapy.
Naildisease can respond to systemic agents, topical retinoids,
localtriamcinolone injections, and topical 5-uorouracil. The
latteragent can cause onycholysis if applied to the free edge ofthe
nail.
AkaraphanthR, et al:Efficacy of a far erythemogenic dose of
narrow-band ultraviolet B phototherapy in chronic plaque-type
psoriasis. JDermatol 2010; 37(2):140145.AsarchA, et al:Th17 cells:
a new paradigm for cutaneous inflamma-tion. J Dermatolog Treat
2008; 19(5):259266.BartlettBL, et al:Ustekinumab for chronic plaque
psoriasis. Lancet
2008; 371(9625):16391640.BenoitS, et al:Childhood psoriasis.
Clin Dermatol 2007; 25(6):555562.BerendsMA, et al:Reliability of
the Roenigk classification of liverdamage after methotrexate
treatment for psoriasis: a clinicopathologicstudy of 160 liver
biopsy specimens. Arch Dermatol 2007;143(12):15151519.BerneburgM,
et al:Phototherapy with narrowband vs. broadband UVB.Acta Derm
Venereol 2005; 85:98.BeyerV, et al:Recent trends in systemic
psoriasis treatment costs.Arch Dermatol 2010;
146(1):4654.BlauveltA:T-helper 17 cells in psoriatic plaques and
additional geneticlinks between IL-23 and psoriasis. J Invest
Dermatol 2008;128(5):10641067.BoehnckeWH, et al:Managing comorbid
disease in patients withpsoriasis. BMJ 2010 Jan 15;
340:b5666.BosJD, et al:Topical treatments in psoriasis: today and
tomorrow. ClinDermatol 2008; 26(5):432437.
BrimhallAK, et al:Safety and efficacy of alefacept,
efalizumab,etanercept and infliximab in treating moderate to severe
plaquepsoriasis: a meta-analysis of randomized controlled trials.
Br JDermatol 2008; 159(2):274285.CatherJC, et al:Combining
traditional agents and biologics for thetreatment of psoriasis.
Semin Cutan Med Surg 2005; 24:37.ConaghanPG, et al:Improving
recognition of psoriatic arthritis.Practitioner 2009;
253(1724):1518, 23.DavisMD, et al:Goeckerman treatment: neglected
in the consensusapproach for critically challenging case scenarios
in moderate tosevere psoriasis. J Am Acad Dermatol 2010;
62(3):508.DohertySD, et al:National Psoriasis Foundation consensus
statementon screening for latent tuberculosis infection in patients
with psoriasis
treated with systemic and biologic agents. J Am Acad
Dermatol59(2):209217.DuffinKC, et al:Genetics of psoriasis and
psoriatic arthritis: updafuture direction. J Rheumatol 2008;
35(7):14491453.EversAW, et al:Treatment nonadherence and long-term
effects onarrowband UV-B therapy in patients with psoriasis. Arch
Derma2010; 146(2):198199.FeuchtenbergerM, et al:Psoriatic
arthritis: therapeutic principles. Dermatol 2008;
26(5):460463.FluhrJW, et al:Emollients, moisturizers, and
keratolytic agents inpsoriasis. Clin Dermatol 2008;
26(4):380386.GoriA, et al:Unusual presentation of tuberculosis in
an infliximabtreated patientwhich is the correct TB screening
before startin
biologic? Dermatol Ther 2010 JanFeb; 23(Suppl 1):S13.GottliebA,
et al:Guidelines of care for the management of psoriaand psoriatic
arthritis: section 2. Psoriatic arthritis: overview andguidelines
of care for treatment with an emphasis on the biologiAm Acad
Dermatol 2008; 58(5):851864.GottliebAB, et al:Psoriasis and the
metabolic syndrome. J DrugsDermatol 2008; 7(6):563572.HalverstamCP,
et al:Nonstandard and off-label therapies for psoClin Dermatol
2008; 26(5):546553.HernandezC, et al:Tuberculosis in the age of
biologic therapy. J Acad Dermatol 2008; 59(3):363380.HeydendaelVM,
et al:Methotrexate versus cyclosporine in modersevere chronic
plaque psoriasis. N Engl J Med 2003; 349:658.HomeyB, et
al:Chemokines and other mediators as therapeutic in psoriasis
vulgaris. Clin Dermatol 2008; 26(5):539545.HuangW, et al:To test or
not to test? An evidence-based assess
of the value of screening and monitoring tests when using
systebiologic agents to treat psoriasis. J Am Acad Dermatol
2008;58(6):970977.LebwohlM, et al:The evolving role of topical
treatments in adjunctherapy for moderate to severe plaque
psoriasis. Cutis 2007; 80Suppl):2940.LebwohlM, et al:From the
Medical Board of the NationalPsoriasis Foundation: monitoring and
vaccinations in patientstreated with biologics for psoriasis. J Am
Acad Dermatol 2008;58(1):94105.LecluseLL, et al:Extent and clinical
consequences of antibodyformation against adalimumab in patients
with plaque psoriasis.Dermatol 2010; 146(2):127132.LeonardiCL, et
al:Efficacy and safety of ustekinumab, a humaninterleukin-12/23
monoclonal antibody, in patients with psoriasis76-week results from
a randomised, double-blind, placebo-cont
trial (PHOENIX 1). Lancet 2008; 371(9625):16651674.LiYY, et
al:Targeting leukocyte recruitment in the treatment ofpsoriasis.
Clin Dermatol 2008; 26(5):527538.MacDonaldA, et al:Psoriasis:
advances in pathophysiology andmanagement. Postgrad Med J 2007;
83(985):690697. Review.MauricePD, et al:Monitoring patients on
methotrexate: hepatic finot seen in patients with normal serum
assays of aminoterminalpeptide of type III procollagen. Br J
Dermatol 2005; 152:451.MenterA, et al:Guidelines of care for the
management of psoriapsoriatic arthritis: section 1. Overview of
psoriasis and guidelinecare for the treatment of psoriasis with
biologics. J Am Acad De2008; 58(5):826850.MssnerR, et al:Tumor
necrosis factor antagonists in the therappsoriasis. Clin Dermatol
2008; 26(5):486502.NeynsB, et al:Cetuximab treatment in a patient
with metastaticcolorectal cancer and psoriasis. Curr Oncol 2008;
15(4):196197NolanBV, et al:A review of home phototherapy for
psoriasis. DerOnline J 2010; 16(2):1.PappKA:Monitoring biologics
for the treatment of psoriasis. ClinDermatol 2008;
26(5):515521.PappKA, et al:Efficacy and safety of ustekinumab, a
humaninterleukin-12/23 monoclonal antibody, in patients with
psoriasis52-week results from a randomised, double-blind,
placebo-conttrial (PHOENIX 2). Lancet 2008;
371(9625):16751684.QureshiAA, et al:Psoriatic arthritis screening
tools. J Rheumatol 35(7):14231425.RitchlinCT:From skin to bone:
translational perspectives on psodisease. J Rheumatol 2008;
35(7):14341437.SchneiderLA, et al:Phototherapy and
photochemotherapy. ClinDermatol 2008; 26(5):464476.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
SchnMP:Treatment of psoriasis: a journey from empiricism
toevidence. Clin Dermatol 2008; 26(5):417418.SinghSK, et al:Th17
cells in the pathogenesis of psoriasis. Curr AllergyAsthma Rep
2008; 8(5):382385.TaylorWJ, et al:Drug use and toxicity in
psoriatic disease: focus onmethotrexate. J Rheumatol 2008;
35(7):14541457.TesmerLA, et al:Th17 cells in human disease. Immunol
Rev 2008;223:87113.ThaiD:Long-term data in the treatment of
psoriasis. Br J Dermatol2008; 159(Suppl 2):1824.WarrenRB, et
al:Systemic therapies for psoriasis: methotrexate,retinoids, and
cyclosporine. Clin Dermatol 2008; 26(5):438447.WeissSC, et al:An
assessment of the cost-utility of therapy for
psoriasis. Ther Clin Risk Manag 2006;
2(3):325328.WozelG:Psoriasis treatment in difficult locations:
scalp, nails, andintertriginous areas. Clin Dermatol 2008;
26(5):448459.ZellD, et al:Genetic alterations in psoriasis. J
Invest Dermatol 2008;128(7):1614.
Reactive arthritis with conjunctivitis/urethritis/diarrhea
(Reiter syndrome)
Reiter syndrome is a characteristic clinical triad of
urethritis,conjunctivitis, and arthritis. The disease occurs chiey
inyoung men of HLA-B27 genotype, generally following a boutof
urethritis or diarrheal illness. Systemic involvement caninclude
the gastrointestinal tract, kidneys, central nervoussystem, and
cardiovascular system. As few patients presentwith the classic
triad, the American College of Rheumatologyrecognizes criteria for
limited manifestations of the syndrome,including peripheral
arthritis of more than 1 months durationin association with
urethritis, cervicitis, or bilateralconjunctivitis.
Hans Reiter was a Nazi war criminal, involved with orhaving
knowledge of involuntary sterilization, as well as astudy of an
experimental typhus vaccine that resulted in hun-dreds of deaths of
concentration camp internees. Severalauthors have suggested that he
no longer be afforded the rec-ognition of using his name to
designate the syndrome.
Clinical features
Any part of the triad may occur rst, often accompanied byfever,
weakness, and weight loss. Although the inciting ure-thritis may be
bacterial, later manifestations include a nonbac-terial urethritis
with painful urination and pyuria. Cystitis,prostatitis, and
seminal vesiculitis may be accompaniments.Vulvar ulceration has
been reported. About one-third ofpatients develop conjunctivitis,
which may be bulbar, tarsal,or angular. Keratitis is usually
supercial and extremelypainful. Iritis is common, especially in
recurrent cases.Infrequently, optic neuritis may occur. An
asymmetric arthri-tis affects peripheral joints, especially those
that are weight-bearing. Its onset is usually sudden. Pain in one
or both heelsis a frequent symptom. Sacroiliitis may develop in up
to two-thirds of patients, most of whom are of HLA-B27 type.
The skin involvement commonly begins with small,
guttate,hyperkeratotic, crusted or pustular lesions of the genitals
(Fig.10-12), palms, or soles. Involvement of the glans penis
(balani-tis circinata) occurs in 25% of patients. Lesions on the
soles andtrunk often become thickly crusted or hyperkeratotic.
Theeruption on the soles is known as keratoderma blennorrhagi-cum
(Fig. 10-13), and occurs in 10% of patients. The buccal,palatal,
and lingual mucosa may show painless, shallow, rederosions. The
nails become thick and brittle, with heavy sub-ungual keratosis.
Children are much more likely to have thepost-dysenteric form,
often with conjunctivitis and arthritis asthe most prominent
complaints.
Fig. 10-12 Genital involvement in reactive arthritis.
Fig. 10-13Keratoderma blennorrhagicum.
The syndrome generally follows an infectious urethritis
diarrheal illness. Implicated organisms include ChlamydShigella,
Salmonella, Yersinia, Campylobacter, Ureaplasma,
BorreCryptosporidium, gonococci, and bacillus CalmetteGu
(BCG). Chlamydia trachomatisand Ureaplasma urealyticumhabeen
isolated from the synovial uid of affected joints, asome patients
respond to antibiotic therapy. Reiter syndrohas also been observed
in HIV disease, but may not be direcrelated to the virus, as it
frequently occurs under treatmentthe immune response improves. The
disease has also betriggered by adalimumab and leunomide in the
setting ankylosing spondyloarthropathy and Crohn disease.
The syndrome involves both infection and the
resultiimmunologically mediated tissue injury in a
geneticapredisposed patient. HLA-B27 is present in about 80% cases.
A positive family history is often noted.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
200
SeborrheicDermatitis,
Psoriasis,
RecalcitrantPalmoplantarEruptions
10of the remaining cases. Some patients have responded to
sulfapyridine therapy. Acitretin, narrow-band UVB ptherapy,
colchicine, azithromycin, biologicals, and tetracwith niacinamide
may also be effective.
BediMKL:Successful treatment of long-standing, recalcitrant
subcorneal pustular dermatosis with etanercept. Skinmed 2007
Sep6(5):245247.BliziotisI, et al:Regression of subcorneal pustular
dermatosis tyIgA pemphigus lesions with azithromycin. J Infect
2005; 51:E31.ChengS, et al:Subcorneal pustular dermatosis: 50 years
on. ClinDermatol 2008; 33(3):229233.HowellSM, et al:Rapid response
of IgA pemphigus of the subco
pustular dermatosis subtype to treatment with adalimumab
andmycophenolate mofetil. J Am Acad Dermatol 2005; 53:541.
Eosinophilic pustular folliculitis
Eosinophilic pustular folliculitis (EPF) was rst describ1970 by
Ofuji but is also referred to as sterile eosinopustulosis. It
occurs more commonly in males, and is mreported in Asia. The mean
age of onset is 35. It is charized by pruritic, follicular
papulopustules that m12 mm. The lesions tend to be grouped and
plaquesmonly form. New lesions may form at the edges of the
plleading to peripheral extension, while central clearingplace. The
most frequent site is the face, particularly ovcheeks. The trunk
and upper extremities are comaffected, and 20% have palmoplantar
pustules. The distion is commonly asymmetrical, and the typical
couone of spontaneous remissions and exacerbations lseveral years.
The condition must be distinguishedHIV-associated eosinophilic
folliculitis, which is discin Chapter 19. A similar condition has
occurred in assocwith hepatitis C virus infection, with
allopurinol, and dpregnancy.
Histologically, there is spongiosis and vesiculation follicular
infundibulum and heavy inltration with ephils. Follicular mucinosis
may be present. There is a peral eosinophilia in half the cases,
and pulmonary eosinohas been described. The cause is unknown; but
num
studies have implicated chemotactic substances,
ICAM-cyclooxygenase-generated metabolites.
Tryptase-positivchymase-negative mast cells have also been
implicated
Indomethacin is effective in the vast majority of paTopical and
intralesional corticosteroids, clofazimine, cycline, isotretinoin,
UVB therapy, dapsone, colchcyclosporine, and cetirizine have also
been reporteffective.
Childhood cases have been described. This subset from the
typical cases in Asian males. Pediatric padevelop sterile pustules
and papules preferentially ovscalp, although scattered clusters of
pustules may occuthe trunk and extremities. Leukocytosis and
eosinoare often present. Recurrent exacerbations and remiusually
occur, with eventual spontaneous resolution.
potency topical steroids are the treatment of choice in
pepatients.
GulU, et al:Eosinophilic pustular folliculitis: the first case
associawith hepatitis C virus. J Dermatol 2007; 34(6):397399.KusS,
et al:Eosinophilic pustular folliculitis (Ofujis
disease)exacerbated with pregnancies. J Eur Acad Dermatol Venereol
2020(10):13471348.SufyanW, et al:Eosinophilic pustular
folliculitis. Arch Pathol Lab 2007; 131(10):15981601.YonedaK, et
al:Eosinophilic pustular folliculitis associated withpulmonary
eosinophilia. J Eur Acad Dermatol Venereol 2007
Se21(8):11221124.
Peripheral leukocytosis of 10 00020 000/mm3and
elevatedsedimentation rate are the most consistent ndings. There
isno specic test for Reiter syndrome.
The differential diagnosis includes rheumatoid
arthritis,ankylosing spondylitis, gout, psoriatic arthritis,
gonococcalarthritis, acute rheumatic fever, chronic mucocutaneous
can-didiasis, and serum sickness. The presence of
associatedmucocutaneous lesions establishes the diagnosis. Some
casesof Lyme disease overlap with the syndrome. Individual
skinlesions may be indistinguishable from those in
psoriasis.Hyperkeratotic lesions generally have a thicker scale
crustthan most psoriatic plaques, but are otherwise identical.
Mucocutaneous lesions are generally self-limited and clearwith
topical steroids. Joint disease is managed with rest andNSAIDs.
Antibiotics, such as doxycycline, have been effectivein some cases.
Immunosuppressive agents, such as methotrex-ate, are commonly
employed for refractory joint disease.Iniximab has been successful
in treating severe disease.Refractory skin lesions are treated like
refractory psoriasis,and severely affected patients have responded
to acitretin orcyclosporine.
PanushRS, et al:Retraction of the suggestion to use the term
Reiterssyndrome sixty-five years later: the legacy of Reiter, a war
criminal,should not be eponymic honor but rather condemnation.
ArthritisRheum 2007; 56(2):693694.Sampaio-BarrosPD, et al:Frequency
of HLA-B27 and its alleles inpatients with Reiter syndrome:
comparison with the frequency in otherspondyloarthropathies and a
healthy control population. Rheumatol Int2008;
28(5):483486.ThielenAM, et al:Reiter syndrome triggered by
adalimumab(Humira) and leflunomide (Arava) in a patient with
ankylosingspondylarthropathy and Crohn disease. Br J Dermatol
2007;156(1):188189.TownesJM:Reactive arthritis after enteric
infections in the UnitedStates: the problem of definition. Clin
Infect Dis 2010; 50(2):247242.WallaceDJ, et al:The physician Hans
Reiter as prisoner of war inNuremberg: a contextual review of his
interrogations (19451947).Semin Arthritis Rheum 2003; 32:208.YuD,
et al:Role of bacteria and HLA-B27 in the pathogenesis ofreactive
arthritis. Rheum Dis Clin North Am 2003; 29:21.
Subcorneal pustular dermatosis(SneddonWilkinson disease)
In 1956, Sneddon and Wilkinson described a chronic
pustulardisease, which occurred chiey in middle-aged women.
Thepustules are supercial and arranged in annular and serpigi-nous
patterns, especially on the abdomen, axillae, and groins.Cultures
from the pustules are sterile. Oral lesions are rare.Some cases are
associated with a monoclonal gammopathy(usually IgA). The condition
is chronic, with remissions ofvariable duration.
Histologically, the pustules form below the stratum corneum,as
in impetigo. Acantholysis is absent, but spongiform pus-tules may
be noted in the upper epidermis. The histologicdifferential
diagnosis includes pustular psoriasis, and super-
cial fungal and bacterial infections. Some cases will showupper
epidermal intercellular IgA staining.
IgA pemphigus shows signicant overlap with subcornealpustular
dermatosis. Presentations of IgA pemphigus includesubcorneal
pustular dermatosis and intraepidermal neu-trophilic IgA dermatosis
types. Using immunoblotting tech-niques, Hashimoto et al have shown
that human desmocollin1 is an autoantigen for the subcorneal
pustular dermatosistype of IgA pemphigus.
Localized cases may respond well to topical
corticosteroids.Dapsone, 50200 mg/day (for an adult), is effective
for most
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
Recalcitrant palmoplantar eruptions
Dermatitis repens
Dermatitis repens, also known as acrodermatitis continua
andacrodermatitis perstans, is a chronic inammatory disease ofthe
hands and feet. It usually remains stable on the extremities,but in
rare cases generalized pustular ares may occur. Thedisease usually
begins distally on a digit, either as a pustulein the nailbed or as
a paronychia. Extension takes place byeruption of fresh pustules
with subsequent hyperkeratosis and
crusting. The disease is usually unilateral in its beginning
andasymmetrical throughout its entire course. As the
diseaseprogresses, one or more of the nails may become dystrophicor
oat away on lakes of pus. Anonychia is common in chroniccases. Some
have used the term dermatitis repens to refer tomore indolent
involvement of the distal ngers.
Involvement of the mucous membranes may occur, evenwhen the
eruption of the skin is localized. Painful, circular,white plaques
surrounded by inammatory areolae are foundon the tongue and may
form a brinous membrane. Fissuredor geographic tongue may
occur.
Histologically, intraepithelial spongiform pustules identicalto
those of psoriasis are seen in the acute stage. Later stagesshow
hyperkeratosis with parakeratosis or atrophy.
Numerous treatment options have been used, including
topical corticosteroids, calipotriene, dapsone,
sulfapyridine,methotrexate, PUVA, acitretin, cyclosporine, and
topicalmechlorethamine. The decision regarding which agent to
useshould take into consideration the severity of disease, and
thepatients age and functional impairment.
Palmoplantar pustulosis (pustular psoriasisof the
extremities)
Chronic palmoplantar pustulosis is essentially a bilateral
andsymmetrical dermatosis (Fig. 10-14). The favorite locations
arethe thenar or hypothenar eminences or the central portion ofthe
palms and soles. The patches begin as erythematous areasin which
minute intraepidermal pustules form. At the begin-
ning these are pinhead-sized; then they may enlarge and
coa-lesce to form small lakes of pus. As the lesions resolve,
denudedareas, crusts, or hyperkeratosis may persist. Palmoplantar
pus-tulosis is strongly associated with thyroid disorders and
ciga-rette smoking. Medications such as lithium, which
aggravatepsoriasis, have also been reported to induce palmoplantar
pus-tular psoriasis.
In 1968, Kato described the rst case of bilateral
clavicularosteomyelitis with palmar and plantar pustulosis. In
1974,Sonozaki described persistent palmoplantar pustulosis
andsternoclavicular hyperostosis. These conditions belong to
thespectrum of skin and joint involvement designated by Kahnas the
SAPHO syndrome (synovitis, acne, pustulosis, hyper-ostosis, and
osteitis). Common features include palmoplantarpustulosis,
acneiform eruption, and pain and swelling of a
sternoclavicular joint, or sternomanubrial or
costochondraljunctions. There is shoulder, neck, and back pain, and
limita-tion of motion of the shoulders and neck is common.
Brachialplexus neuropathy and subclavian vein occlusion may
occur.The lumbar spine and sacroiliac joints are usually
spared.Chronic multifocal osteomyelitis in children may be a
pediat-ric variant. Others have described an association
betweenpalmoplantar pustulosis and arthritis or osteitis.
SAPHOsyndrome may coexist with features of Behets disease.
Theknees, spine, and ankles may be involved. Ivory vertebraehave
been described.
Fig. 10-14 A. Plantas pustulosis; B. Pustules and hyperkeratosis
atypical.
A
B
The disease is commonly resistant to treatment. Topical stoids,
retinoids, calcipotriene, or macrolactams are of sobenet. Acitretin
is generally extremely effective at a dose1 mg/kg/day, although
rebound occurs more quickly thwith etretinate. Low-dose
cyclosporine, in doses ranging fro1.25 to 5 mg/kg/day, has also
been very effective, but it is nsuitable for long-term treatment.
Dapsone, colchicine, leunmide, and mycophenolate mofetil may be
effective. O8-methoxypsoralen and high-intensity UVA irradiation
soak PUVA can both be helpful, and Grenz ray therapy cinduce
prolonged remissions in some patients. Chronic ostemyelitis in
SAPHO syndrome has been reported to respondbisphosphonates.
BlancoJF, et al:Ivory vertebra and palmoplantar pustulosis.
JRheumatol 2007 Apr; 34(4):896899.Hurtado-NedelecM, et
al:Characterization of the immune response inthe synovitis, acne,
pustulosis, hyperostosis, osteitis (SAPHO)syndrome. Rheumatology
(Oxford) 2008; 47(8):11601167.NikkelsAF, et al:Breaking the
relentless course of Hallopeausacrodermatitis by dapsone. Eur J
Dermatol 1999; 9:126.Piquero-CasalsJ, et al:Using oral tetracycline
and topical betamethasone valerate to treat acrodermatitis continua
of Hallopeau. Cutis2002; 70:106.ProenaNG:Acropustulosis repens. Int
J Dermatol 2006;45(4):389393.SkovL, et al:IL-8 as antibody
therapeutic target in inflammatorydiseases: reduction of clinical
activity in palmoplantar pustulosis. JImmunol 2008;
181(1):669679.YabeH, et al:Two cases of SAPHO syndrome accompanied
by classfeatures of Behets disease and review of the literature.
ClinRheumatol 2008; 27(1):133135.
-
5/26/2018 Chapter 10 Seborrheic Dermatitis, Psoriasis,
Recalcitrant Palmoplantar Erupt...
http:///reader/full/chapter-10-seborrheic-dermatitis-psoriasis-recalcitrant-palmoplan
202
SeborrheicDermatitis,
Psoriasis,
RecalcitrantPalmoplantarEruptions
10
Fig. 10-15 Acropustulosis of infancy. (Courtesy of Curt
SamlasMD)
Pustular bacterid
Pustular bacterid was rst described by George Andrews. It
ischaracterized by a symmetric, grouped, vesicular, or
pustulareruption on the palms and soles, marked by exacerbations
andremissions over long periods. Andrews regarded the discov-ery of
a remote focus of infection, and cure on its elimination,as crucial
to the diagnosis.
The primary lesions are pustules. Tiny hemorrhagic
punctaintermingled with the pustules are frequently seen.
Whenlesions are so numerous as to coalesce, they form a
honeycomb-like structure in the epidermis. The disease usually
begins onthe mid-portions of the palms or soles, from which it
spreadsoutwardly until it may eventually cover the entire
exoraspects of the hands and feet. There is no involvement of
thewebs of the ngers or toes, as in tinea pedis.
When the eruption is fully developed, both palms and solesare
completely covered, and the symmetry is pronounced.During fresh
outbreaks, the white blood count may show aleukocytosis that ranges
from 12 000 to 19 000/mm 3with 6580% neutrophils. As a rule,
scaling is present in fully evolvedlesions, and the scales are
adherent, tough, and dry. Duringexacerbations, crops of pustules or
vesicles make their appear-ance, and there is often severe itching
of the areas. Tendernessmay be present. Many regard this condition
as a variant ofpsoriasis, triggered by infection.
Bacharach-BuhlesM, et al:The pustular bacterid (Andrews): are
thereclinical criteria for differentiating from psoriasis pustulosa
palmaris etplantaris? Hautarzt (Germany) 1993;
44:221.WorretWI:Pustular bacterid of Andrews. Am J Dermatopathol
1985;7:200.
Infantile acropustulosis
Infantile acropustulosis is an intensely itchy
vesicopustulareruption of the hands and feet (Fig. 10-15). Most
cases beginby 10 months of age. Lesions often predominate at the
edgesof the palms and soles. Individual crops of lesions clear in
afew weeks, but recurrences may continue for months or
years.Scabies, tinea, and herpetic infection can produce
similarlesions, and must be excluded.
Histologically, a subcorneal pustule with neutrophils isnoted.
Eosinophils may be numerous. As the lesions are easilypunctured to
produce smears of the inammatory cells, biop-sies are seldom
employed.
Fig. 10-1Seborrheic dermatitis.
Fig. 10-2Seborrheic dermatitis involving the chest and
axillae.
Fig. 10-3Psoriasis.
Fig. 10-4Psoriasis plaque, red plaque with silver scale on the
kn
Fig. 10-5Inverse psoriasis.
Fig. 10-6Nail pitting and distal onycholysis in psoriasis.
Fig. 10-7Fissured and geographic tongue in a patient
withgeneralized pustular psoriasis.
Fig. 10-8Nailbed involvement in acrodermatitis continua.
Fig. 10-9Anonychia in acrodermatitis continua.
Fig. 10-10Erythrodermic psoriasis.
Fig. 10-11Hyperkeratotic lesions of the reactive arthritis
syndrom
Fig. 10-12Plantar pustulosis.
Fig. 10-13Psoriasis.
Bonus images for this chapter can be found online
http://www.expertconsult.com
Lesions often respond to topical corticosteroids. Refrlesions
may respond to dapsone at doses of 12 mg/kg
VicenteJ, et al:Are eosinophilic pustular folliculitis of
infancy andinfantile acropustulosis the same entity? Br J Dermatol
1996; 13WagnerA:Distinguishing vesicular and pustular disorders in
theneonate. Curr Opin Pediatr 1997; 9:396.














![Palmoplantar Pustulosis: Recent Advances in ...ecent Adances in Palmoplantar Pustulosis 357 patientswithPPPrangesfrom10.2–49%indierentpopu-lations[2, 5, 25, 26]andisariskfactorforischemicheart](https://img.pdfslide.net/doc/110x75/602301c9840e343f9c5d167f/palmoplantar-pustulosis-recent-advances-in-ecent-adances-in-palmoplantar-pustulosis.jpg)