Embed Size (px)
Citation preview

1586
CHAPTER 121
Anemia, Polycythemia, and White Blood Cell Disorders
Timothy G. Janz and Glenn C. Hamilton
ANEMIA
Definition
Anemia is an absolute decrease in the number of circulating red blood cells (RBCs). The diagnosis is made when laboratory mea-surements fall below accepted normal values (Table 121-1).
In emergency medicine, anemia is divided into two broad cat-egories: emergent, having immediate life-threatening complica-tions; and nonemergent, with less imminent danger to the patient. Factors other than the absolute number of circulating RBCs may place the patient in one category or another (e.g., rate of onset and underlying hemodynamic reserve of the patient). Both groups necessitate a sound diagnostic approach, but emergent anemia may require supportive therapy concomitant with or in advance of the definitive diagnosis. Although patients with nonemergent anemia are usually referred to a specialist, they are seen in the hospital often enough to make an understanding of anemia neces-sary for emergency physicians. The urgency of consultation depends predominantly on the patient’s hemodynamic tolerance of the anemia.
Pathophysiology
The major function of the RBC is oxygen transport from the lung to the tissue and carbon dioxide transport in the reverse direction. Oxygen transport is influenced by the amount of hemoglobin, its oxygen affinity, and blood flow. An alteration in any of the major components usually results in compensatory changes in the other two. For example, a decrease in hemoglobin from anemia is com-pensated by both inotropic and chronotropic cardiac changes that result in increased blood flow and decreased hemoglobin affinity at the tissue level, thereby allowing more oxygen release. These compensatory responses may collapse because of disease severity or underlying pathologic conditions. The result is tissue hypoxia and eventual cell death.
Anemia often stimulates the compensatory mechanism of erythropoiesis controlled by the hormone erythropoietin. Eryth-ropoietin is a glycoprotein produced in the kidney (90%) and the liver (10%). It regulates the production of RBCs by control-ling differentiation of the committed erythroid stem cell. It is stimulated by tissue hypoxia and products of RBC destruction during hemolysis. Erythropoietin levels are elevated in many types of anemia.
Bone marrow contains pluripotent stem cells that can differen-tiate into erythroid, myeloid, megakaryocytic, and lymphoid pro-genitors. Erythropoietin enhances the growth and differentiation of erythroid progenitors. When the late normoblast extrudes its nucleus, it still contains a ribosomal network, which identifies the
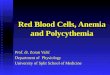
reticulocyte (Fig. 121-1). The reticulocyte retains its ribosomal network for approximately 4 days, 3 days of which are spent in bone marrow and 1 day in the peripheral circulation. The RBC matures as the reticulocyte loses its ribosomal network and circu-lates for 110 to 120 days. The erythrocyte is then removed by macrophages that detect senescent signals.
Under steady-state conditions, the rate of RBC production equals the rate of destruction. RBC mass remains constant because an equal number of reticulocytes replace the destroyed, senescent erythrocytes during the same period.
Common sites of blood loss in trauma include the pleural, peritoneal, pelvic, and retroperitoneal spaces. In nontraumatic circumstances, especially in patients receiving anticoagulants, the gastrointestinal tract, retroperitoneal space, uterus, and adnexa need to be considered.
Causes other than blood loss may be responsible for severe anemia of rapid onset. Certain rare hemolytic conditions can cause rapid intravascular destruction of RBCs (Box 121-1). More common are patients with chronic compensated hemolytic anemia (e.g., sickle cell disease), who decompensate with an acute-onset anemia as a result of decreased erythrocyte production triggered by a viral infection.
Beyond red cell destruction, the status of hemoglobin function should be considered. Impaired hemoglobin transport of oxygen is seen in cases of carbon monoxide poisoning. Methemoglobin-emia from nitrates, cyanhemoglobin from cyanide, and sulfhemo-globinemia from hydrogen sulfide may severely decrease functional hemoglobin. These patients often have fatigue, altered mental status, shortness of breath, and other manifestations of hypoxia without signs of RBC loss or volume depletion.
Diagnostic Findings in Emergent Anemia
Clinical Features
The most common cause of clinically significant anemia is blood loss. The clinical manifestation of anemia depends on how rapidly the hematocrit falls and also on the patient’s ability to compensate.
Clinical signs and symptoms include tachycardia, decreased blood pressure, postural hypotension, lightheadedness, increased heart rate, and increased respiratory rate. Complaints of thirst, altered mental status, and decreased urine output may also be present. The patient’s age, concomitant illness, and underlying hematologic, cerebral, and cardiovascular status tremendously influence the clinical findings. Children and young adults may tolerate significant blood loss with unaltered vital signs until a precipitant hypotensive episode occurs. Pediatric patients may
Section TenHEMATOLOGY AND ONCOLOGY

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1587
1. Complete blood count and peripheral smear2. Blood sample for type and crossmatch3. Prothrombin time and international normalized ratio4. Partial thromboplastin time5. Electrolyte levels6. Glucose level (especially if the patient has altered
consciousness)7. Creatinine level8. Urinalysis for free hemoglobin9. Clotting and unclotted blood samples for later testing
If possible, a blood sample is obtained for measurement of hematocrit in the emergency department. Although it may take hours before the hematocrit correctly reflects the degree of blood loss, the initial value is useful in determining a baseline. On occa-sion, this value reveals an underlying anemia with the acute blood loss superimposed. Depending on severity, a blood sample is sent for type and crossmatch. Peripheral smear interpretation is done on pretreatment blood samples.
Measurements of coagulation status, electrolytes, glucose, blood urea nitrogen, and creatinine are useful in the diagnosis of under-lying disease processes that may relate to the patient’s anemia. Values of folate, vitamin B12, iron, total iron-binding capacity, reticulocytes, and direct antiglobulin (Coombs’ test) are altered by transfusion. Therefore, pretreatment samples are best saved.
Figure 121-1. Reticulocytes with reticular material after methylene blue staining. (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:18.)
BOX 121-2
HistoryGeneralOut-of-hospital status, therapy, response to therapyBleeding diathesisPrevious blood transfusionUnderlying diseases, including allergiesCurrent medications, especially those causing platelet inhibition
TraumaNature and time of injuryBlood loss at scene
NontraumaSkin: petechiae, ecchymosesGastrointestinal: hematemesis, hematochezia, melena, peptic
ulcerGenitourinary: last menstruation, menorrhagia, metrorrhagia,
hematuria
Physical ExaminationVital Signs Measured SeriallyBlood pressure, pulse, respiratory rate, oxygen saturationOrthostatic blood pressure and pulse (contraindicated with
severe hypotension)Level and content of consciousness
SkinPallorDiaphoresisJaundiceCyanosisPurpura, ecchymoses, petechiaeEvidence of penetrating wounds
CardiovascularMurmurs, S3, S4
Quality of femoral and carotid pulses
AbdomenHepatosplenomegalyPain, guarding, rebound on palpationRectal and pelvic examinationMassesStool hemoglobin testing
History and Physical Examination for Clinically Severe Anemia
BOX 121-1
Mechanical hemolysis associated with disseminated intravascular coagulation
Massive burnsToxins (e.g., some poisonous venoms: brown recluse spider,
cobra)Infections such as malaria or Clostridium sepsisSevere glucose-6-phosphate dehydrogenase deficiency with
exposure to oxidant stressABO incompatibility transfusion reactionCold agglutinin hemolysis (e.g., Mycoplasma organisms,
infectious mononucleosis)Paroxysmal nocturnal hemoglobinuria exacerbated by
transfusionImmune complex hemolysis (e.g., quinidine)
Causes of Rapid Intravascular Red Blood Cell Destruction
AGEHEMOGLOBIN
(g/dL)HEMATOCRIT
(mL/dL)RED BLOOD CELL
COUNT (×106)
3 months 10.4-12.2 30-36 3.4-4.0
3-7 years 11.7-13.5 34-40 4.4-5.0
Adult man 14.0-18.0 40-52 4.4-5.9
Adult woman 12.0-16.0 35-47 3.8-5.2
Table 121-1 Hemogram Normal Values
become markedly tachycardic, physiologically attempting to maintain cardiac output because their ability to increase stroke volume is limited. Elderly patients commonly have underlying disease states that compromise their ability to compensate for blood loss.1
Pertinent elements of the history and physical examination of patients with acute anemia are listed in Box 121-2.
Ancillary Evaluation
Stabilization of emergent anemia commonly runs parallel to assessment. If the signs and symptoms suggest potential life-threatening conditions, intravenous lines are placed and samples for the following initial laboratory tests are drawn:

1588 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
Differential Diagnosis
The differential diagnosis of anemia is facilitated by classification of the anemia into one of three groups: decreased RBC produc-tion, increased RBC destruction, and blood loss. A complementary approach uses RBC morphology and indices. Figure 121-3 pres-ents an algorithm for the evaluation of anemia.
Diagnostic Findings in Nonemergent Anemia
Clinical Features
Nonemergent anemias are usually seen in ambulatory patients complaining of fatigue and weakness. Other voiced complaints include irritability, headache, postural dizziness, angina, decreased exercise tolerance, shortness of breath, and decreased libido. When the anemia is of slow onset, the patient may adapt until the hemo-globin is very low. Alternatively, patients with rapid blood loss may experience lightheadedness or syncope even when the measured hemoglobin is not critically low. For patients without evidence of acute bleeding or emergent condition, elements of history and physical examination may help identify the cause (Box 121-3). Most of these patients do not need immediate stabilization and can be further evaluated as outpatients.
Ancillary Evaluation
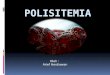
The initial laboratory evaluation includes a complete blood count with leukocyte differential, reticulocyte count, peripheral smear (Fig. 121-2), and RBC indices, including mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean cor-puscular hemoglobin concentration (MCHC).
Disposition
Criteria for the admission of patients with nonemergent anemia are shown in Box 121-4.
Figure 121-2. Normal smear. (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:22.)
BOX 121-3
HistorySymptoms of AnemiaChest pain, decreased exercise tolerance, dyspneaWeakness, fatigue, dizziness, syncope
Bleeding DiathesisBleeding after trauma, injections, tooth extractionsSpontaneous bleeding, such as epistaxis, menorrhagiaSpontaneous purpura and petechiae
Sites of Blood LossRespiratory: epistaxis, hemoptysisGastrointestinal: hematemesis, hematochezia, melenaGenitourinary: abnormal menses, pregnancies, hematuriaSkin: petechiae, ecchymoses
Intermittent Jaundice, Dark Urine
Dietary HistoryVegetarianismPoor nutrition
Drug Use and Toxin Exposure, Including Alcohol
Racial Background, Family History
Underlying DiseaseUremia, liver disease, hypothyroidismChronic disease states such as cancer, rheumatic or renal diseasePrevious surgery
MiscellaneousPrevious treatment of anemiaWeight lossBack pain
Physical ExaminationSkinPallorPurpura, petechiae, angiomasUlcerations
EyeConjunctival jaundice, pallorFunduscopic hemorrhage, petechiae
OralTongue atrophy, papillary soreness
CardiopulmonaryHeart size, murmurs, extra cardiac soundsRales, other signs of pulmonary edema
AbdomenHepatomegaly, splenomegalyAscitesMasses
Lymph Nodes
NeurologicAltered positions or vibratory sensePeripheral neuritis
Rectal and Pelvic
History and Physical Examination for Nonemergent Anemia

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1589
securing the diagnosis. The definitive diagnosis is usually made outside the emergency department and may require bone marrow examination. The emergency physician rarely initiates replace-ment therapy, except in circumstances that require transfusion. Appropriate diagnostic tests may be initiated, but replacement of iron, vitamin B12, or folate without proof of cause is generally unnecessary and unwise.
RBC indices are useful in classifying anemias caused by a pro-duction deficit. Their calculation and normal ranges are provided in Table 121-2. MCV is a measure of RBC size; decreases and increases reflect microcytosis and macrocytosis, respectively. MCH incorporates both RBC size and hemoglobin concentration. It is influenced by both and is the least helpful of the indices. The MCHC index is a measure of the concentration of hemoglobin. Low values represent hypochromia, whereas high values are noted only in patients with decreased cell membrane relative to cell volume, such as in the case of spherocytosis. An additional index is the RBC distribution width (RDW), which is a measure of the
Decreased Red Blood Cell Production
Anemias caused by decreased RBC production have a natural history of insidious onset and an associated decreased reticulocyte count. A subclassification by indices of anemias caused by decreased RBC production is listed in Box 121-5. The RBC indices and morphology manifested in a peripheral smear are useful in
Figure 121-3. Algorithm for the evaluation of anemia. AZT, azathioprine; ETOH, ethanol; fL, femtoliter; G6PD, glucose-6-phosphate dehydrogenase; Hgb, hemoglobin; LDH, lactate dehydrogenase; MCV, mean corpuscular volume; RBCs, red blood cells; TIBC, total iron-binding capacity.
Obtain B12,Folate levels
YESNO
ThalassemiaSideroblastic
anemiaChronic disease
(late)
Iron deficiency
PositiveNegative
Non-autoimmunehemolyticanemia
Autoimmunehemolyticanemia
Iron, TIBC, Ferritin
YESNO
Liver diseaseReticulocytosisMyelodysplastic
syndromesETOH abuseDrugs
B12 deficiencyFolate
deficiency
Coombs
Hemolysis
YESNO
Acute blood lossChronic diseaseChronic renal
insufficiencyHypothyroidismBone marrow
suppressionAplastic anemia
HemolysisG6PD
(bite cells)
LDH, Haptoglobin
YESNO
Peripheral blood smear:Microcytic or hypochromicRBCs
Peripheral blood smear:Schistocytes, helmet cells,spherocytes, bite cells
Peripheral blood smear:Large oval-shaped RBCs,Hypersegmented
neutrophils
MCV � 81 fL MCV 81-100 fL MCV � 100 fL
Iron deficiencyThalassemiaSideroblastic anemiaLead intoxicationChronic disease (late)
Lead intoxication Iron deficiencyThalassemiaSideroblastic anemiaChronic disease
(late)
Acute blood lossChronic diseaseChronic renal insufficiencyHypothyroidismBone marrow suppressionHemolysisG6PDAplastic anemia
B12 deficiencyFolate deficiencyLiver diseaseReticulocytosisMyelodysplastic syndromesETOH abuseDrugs (hydroxyurea, AZT,chemotherapeutic agents)
Hgb � 12 g/dL
Algorithm for the Evaluation of Anemia
BOX 121-4
Developing cardiac symptoms, such as shortness of breath or chest pain, or neurologic symptoms
Initial unexplained hemoglobin value less than 8-10 g/dL or hematocrit less than 25-30%
Major difficulty in obtaining outpatient care for patients whose hemoglobin levels are significantly low or when comorbidity is present
Admission Criteria for Nonemergent Anemia

1590 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
and porphyrin (sideroblastic anemia and lead poisoning). Anemia of chronic disease, a secondary iron abnormality, rounds out the differential diagnosis. Not all microcytic anemias are the result of iron deficiency, and routine iron therapy for a patient with a low MCV and MCHC is inappropriate.
Iron Deficiency Anemia. Iron deficiency is a frequent cause of chronic anemia seen in the emergency department. It is the most common anemia in women of childbearing age. In older patients, occult blood loss, especially gastrointestinal, may initially appear as iron deficiency anemia. Because changes in RBC size and hemo-globin content occur only after bone marrow and cytochrome iron stores are depleted, a patient may have early symptoms of iron deficiency (e.g., fatigue) without manifesting changes in RBC structure.
The diagnosis is made by laboratory evaluation of the fasting level of serum iron, serum ferritin, and total iron-binding capacity. The laboratory interpretation and pitfalls are outlined in Table 121-3. A concentrated search for occult blood loss is vital.
Therapy consists of oral iron replacement. A cost-effective form is ferrous sulfate. The dosage is 300 mg for adults (60 mg of ele-mental iron) or 3 mg/kg/day for children. This medication is gen-erally well tolerated, although it may cause nausea, vomiting, or constipation. Patients should be warned that their stools will be blackened. The patient should also be warned that bleeding from the digestive tract can also be manifested as blackened stool. In rare patients with poor oral tolerance or absorption, parenteral iron therapy may be necessary.
The patient may experience a sense of improvement in as few as 24 hours. Reticulocytosis appears during a 3- or 4-day period in children but may take more than 1 week in adults. The hemo-globin concentration rises on a similar schedule. Explanations for response failures to iron therapy include the following: the patient is noncompliant with the iron supplementation, the blood loss may exceed the replacement, the diagnosis is incorrect, or the diagnosis is partially correct with an additional process complicat-ing the iron deficiency.2
Thalassemia. Thalassemia is a genetic autosomal defect reflected by the decreased synthesis of globin chains. The hemo-globin molecule is present as two paired globin chains. Each type of hemoglobin is made up of different globins. For example, normal adult hemoglobin (HbA) is made up of two α chains and two β chains (α2β2). HbA2 is α2δ2, and fetal hemoglobin (HbF) is α2γ2. A separate autosomal gene controls each globin chain. Dele-tions in this globin gene result in an absence or decreased function of the messenger RNA that codes for the creation of that globin. The various globins (α, β, δ, and γ) may be affected by a number of genetic combinations. The decrease in globin production in thalassemia results in decreased hemoglobin synthesis and inef-fective erythropoiesis, which is attributable to increased intramar-row hemolysis with destruction of RBCs before they are released. Normal erythropoiesis has a 10 to 20% incidence of ineffective release, with associated intramarrow RBC destruction. This inef-fective release of erythropoiesis may double or triple in patients with thalassemia. The cause is believed to be excess chains of the uninhibited globin precipitating in RBCs.3
Although many variations in thalassemia are possible, only three are commonly considered. Homozygous β-chain thalasse-mia (thalassemia major) occurs predominantly in Mediterranean populations. It represents one of the most common single-gene disorders. The disease is characterized by severe anemia, hepato-splenomegaly, jaundice, abnormal development, and premature death. Patients are transfusion dependent and die as a result of iron deposition in tissues, particularly the myocardium, or infec-tion. Treatment is supportive and consists of transfusion and iron chelation therapy.4,5
Heterozygous β-chain thalassemia (thalassemia minor) is man-ifested as a mild microcytic hypochromic anemia with target cells
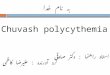
Figure 121-4. Iron deficiency anemia with hypochromic, microcytic cells and poikilocytes (abnormally shaped cells). (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:44.)
BOX 121-5
Hypochromic Microcytic Anemias (Decreased MCV and Hemoglobin Concentration)Iron deficiencyThalassemiaSideroblastic anemia or lead poisoningChronic disease (e.g., cancer, renal or inflammatory disease);
normochromic and normocytic indices often found
Macrocytic (Elevated MCV)Vitamin B12 deficiencyFolate deficiencyLiver diseaseHypothyroidism
Normocytic (Normal MCV and Hemoglobin Concentration)Primary bone marrow involvement: aplastic anemia, myeloid
metaplasia with myelofibrosis, myelophthisic anemiaResulting from underlying disease: hypoendocrine state (thyroid,
adrenal, pituitary), uremia, chronic inflammation, liver disease
Differential Diagnosis of Anemias Caused by Decreased Red Blood Cell Production: Subclassification by Red Blood Cell Indices
MCV, mean corpuscular volume.
INDEX FORMULA FOR CALCULATION NORMAL RANGE
Mean corpuscular volume
Hematocrit (%) divided by red blood cell count (106/µL)
81-100 fL
Mean corpuscular hemoglobin
Hemoglobin (g/dL) divided by red blood cell count (106/µL)
26-34 pg
Mean corpuscular hemoglobin concentration
Hemoglobin (g/dL) divided by hematocrit (%)
31-36%
fL, femtoliter.
Table 121-2Calculation of Red Blood Cell Indices and Normal Values
homogenicity of the RBCs measured. RDW is automatically cal-culated as the standard deviation of MCV divided by MCV mul-tiplied by 100. A normal RDW is 13.5 ± 1.5%. The RDW is usually elevated in anemias caused by nutritional deficiencies; however, it is not specific for any abnormality.
Microcytic Anemias. Hypochromic microcytic anemias are sub-divided into deficiencies of the three building blocks of hemoglo-bin: iron (iron deficiency anemia; Fig. 121-4), globin (thalassemia),

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1591
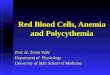
Figure 121-5. β-Thalassemia with microcytic hemochromic red cells and target cells. (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:96.)
TEST NORMAL RESULT IRON DEFICIENCY LEVEL INTERPRETATION
Fasting serum iron 60-180 µg/dL <60 µg/dL Diurnal variation (draw in morning); increased by hepatitis, hemochromatosis, hemolytic anemia, and aplastic anemia; decreased in infection
Total iron-binding capacity 250-400 µg/dL >400 µg/dL Increased in late pregnancy or hepatitis; decreased in infection
Percentage of saturation (serum iron) of total iron-binding capacity
15-45% <15%
Serum ferritin 10-10,000 mg/mL <10 mg/mL Reflects iron stores; may increase as an acute-phase reactant in infection
Bone marrow stainable iron Hemosiderin granules in reticuloendothelial cells
Absent Standard for assessment of iron stores
Table 121-3 Diagnostic Tests for Iron Deficiency Anemia
(erythrocytes with central hyperchromic bull’s-eye surrounded by pallor) seen on the peripheral smear (Fig. 121-5), an MCV com-monly more severely lowered than with iron deficiency anemia, a normal level of serum iron, and an elevated level of HbA2 (α2δ2) on hemoglobin electrophoresis (2-5%). Usually, no treatment is necessary.α-Thalassemia varies in spectrum from an asymptomatic
carrier state to prenatal death. Four gene loci control this range. In the tolerated forms, it is more commonly seen in Asians and African Americans. Microcytosis, hypochromia, target cells, and basophilic stippling are noted on the peripheral smear. The diag-nosis is made with hemoglobin electrophoresis and genetic testing.
Screening for carriers is performed by measurement of RBC indices and estimation of the HbA2 concentration. Prenatal diag-nosis can be made by analysis of fetal blood and, more recently, by fetal DNA obtained by chorionic villus sampling.
Therapy consists of blood transfusions, which are based on the clinical severity of the anemia. The goals of transfusion therapy include correction of anemia, suppression of erythropoiesis, and inhibition of increased gastrointestinal iron absorption. Iron che-lation therapy is often required to control excess iron stores. His-torically, deferoxamine, a subcutaneously administered chelator, was used; however, it has been replaced at many centers with the oral chelator deferasirox (Exjade). Deferasirox is renally cleared; thus dose adjustments may be necessary for chronic renal insuf-ficiency, and it is contraindicated in end-stage renal disease.6
Bone marrow transplantation from HLA-identical donors has resulted in disease-free survival in 60 to 90% of recipients, but its role in thalassemia has yet to be determined. Although much interest centers on permanent correction of genetic deficits in thalassemia, gene therapy does not yet exist.7
Sideroblastic Anemia. Sideroblastic anemia involves a defect in porphyrin synthesis. The resultant impaired hemoglobin pro-duction causes excess iron to be deposited in the mitochondria of the RBC precursor, but some also circulates. The result is increased
serum iron and ferritin levels, with transferrin saturation. The defective heme synthesis results in ineffective erythropoiesis, mild to moderate anemia, and a dimorphic peripheral smear with hypochromic microcytes along with normal and macrocytic cells.
Sideroblastic anemia, although found in a rare sex-linked hereditary form, is typically a disease of the elderly. Indeed, the idiopathic form is a common type of refractory anemia in elderly patients. Pallor and splenomegaly may be noted, and iron staining of the peripheral smear may demonstrate iron-containing inclu-sion bodies in RBCs. Some of these patients are deficient in pyri-doxine (vitamin B6) and respond to treatment with 100 mg of pyridoxine three times a day. Most remain anemic, but a 1- or 2-month pyridoxine trial is acceptable treatment. These patients may be susceptible to iron overload, particularly if long-term transfusion therapy is necessary, but they may respond to iron chelation therapy. Idiopathic sideroblastic anemia is considered a preleukemic state, and acute myelogenous leukemia develops in approximately 5% of these patients.
Secondary causes of sideroblastic anemia include toxins such as chloramphenicol, isoniazid, and cycloserine as well as diseases such as hemolytic and megaloblastic anemia, infection, carci-noma, leukemia, and rheumatoid arthritis. The exact mechanisms of these causative agents and diseases are unknown. Lead poison-ing is one reversible cause of sideroblastic anemia. It may be sug-gested by the appearance of RBC basophilic stippling on the peripheral smear. Elevated blood lead levels are diagnostic. Alcohol abuse may also result in disordered heme synthesis, which can be corrected by alcohol cessation or by parenteral pyridoxal phos-phate in cases of continued abuse. Oral pyridoxine may be inef-fective because of impaired conversion to the active form in alcoholic patients.
Anemia of Chronic Disease. Anemia of chronic disease is common and typically normochromic, normocytic. It is charac-terized by low serum iron levels, low total iron-binding capacity, and normal or elevated ferritin levels. Bone marrow is normal, but staining reveals an abnormality in the mobilization of iron from reticuloendothelial cells. This anemia can be differentiated from iron deficiency by total iron-binding capacity, serum ferritin level, bone marrow examination, and nonresponsiveness to a trial of iron therapy. Because the hematocrit is seldom less than 25 to 30%, therapy is not usually required. A complete search for occult blood loss is necessary during the evaluation of this diagnosis because iron deficiency may be superimposed. Dissemi-nated cancer, chronic inflammation, uremia, and infection are common causes.8
Macrocytic and Megaloblastic Anemias. In terms of the potential for a therapeutic response, the most important cause of macrocy-tosis is megaloblastic anemia. Megaloblastic anemia is the hema-tologic manifestation of a total-body alteration in DNA synthesis.

1592 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
Megaloblastic anemia that is not responsive to folate or vitamin B12 is commonly related to antimetabolites used in chemotherapy or rare inherited disorders of DNA synthesis.
Table 121-4 lists a number of the problems associated with megaloblastic anemia and their underlying pathologic states. A unique feature of vitamin B12 deficiency is its neurologic involve-ment. Patients may have paresthesias in their hands and feet, decreased proprioception, or decreased vibratory sense. The insid-iously developing classic neurologic complex includes loss of pro-prioception; weakness and spasticity of the lower extremities with altered reflexes; and variable mental changes, such as depression, paranoid ideation, irritability, and forgetfulness. The last two com-plaints have also been noted with folic acid deficiency. Vitamin B12–deficient patients have some of the lowest hemoglobin levels seen in any disease state.
Macrocytic anemia is suggested when the MCV is greater than 100 fL, but other criteria need to be met for megaloblastosis to be considered the cause of the macrocytic anemia. On the peripheral smear, large oval red cells (macro-ovalocytes) and hypersegmented polymorphonuclear neutrophils are believed to be diagnostic (Fig. 121-6). A bone marrow aspirate may reveal morphologic changes consistent with megaloblastic erythropoiesis. Other potentially useful laboratory tests include vitamin B12 and folate levels, red cell folate, and lactate dehydrogenase (LDH). Laboratory tech-niques, values, and interpretations are listed in Table 121-5. Once megaloblastic anemia is diagnosed and folate or vitamin B12 defi-ciency determined, standard diagnostic regimens are followed to determine the precise origin of the deficiency.
Because one deficiency may cause gastrointestinal absorption changes that beget other deficiencies, the emergency physician may be forced to initiate therapy before the final diagnosis is made. However, a caution is given to obtain necessary laboratory speci-mens before this course is pursued. The usual dosage for patients with megaloblastic anemia secondary to folate deficiency is 1 mg of oral folic acid per day. Parenteral administration is generally unnecessary because most cases are due to dietary deficiency. In contrast, malabsorption is the most common cause of vitamin B12 deficiency, and parenteral therapy is initiated at 100 µg/day intra-muscularly for the first 7 to 10 days. Thereafter, only monthly 100-µg doses are necessary. The response is often dramatic, with reticulocyte counts rising up 30 to 50% and normalization of RBC, white blood cell (WBC), and platelet counts in 6 to 8 weeks. The use of vitamin B12 or folate supplements in patients with undiagnosed anemia is to be discouraged. The routine injection of vitamin B12 in the elderly has decreased but is still a too common practice.9
Macrocytic anemias unrelated to megaloblastic changes are seen frequently. Liver disease, often associated with alcoholism, is
The defective DNA synthesis is caused by a lack of the coenzyme forms of vitamin B12 and folic acid. The deficiency appears clini-cally in tissues with rapid cell turnover, including hematopoietic cells and those of mucosal surfaces, particularly in the gastroin-testinal tract. This deficiency is characterized hematopoietically by ineffective erythropoiesis and pancytopenia. Vitamin B12 and folate deficiencies have different developmental histories, but the clinical result may be similar. Differentiation of folate and vitamin B12 deficiencies usually depends on measured levels in the laboratory.
Folic acid, absorbed in the duodenum and jejunum, is com-monly found in green vegetables, cereals, and fruit. It may be destroyed completely by cooking. The body requires approxi-mately 100 µg/day and usually stores 6 to 20 mg. Therefore, a 2- to 4-month supply is available before megaloblastic changes occur. Causes of folate deficiency are listed in Box 121-6. Most patients with folate deficiency have either an inadequate dietary intake, such as alcoholic patients, or increased use, as in pregnancy.
Vitamin B12 is found in foods of animal origin only and is not destroyed by cooking. It is absorbed in the ileum after binding to intrinsic factor. This glycoprotein factor is secreted by the parietal cells of the gastric mucosa and allows low levels of B12 to be actively absorbed. The adult requirement is 1 or 2 µg/day, with a body store of 5 mg. Therefore, megaloblastic changes may take up to 4 years to develop after cessation of vitamin B12 uptake. The various causes of vitamin B12 deficiency are listed in Box 121-7. The most common cause is chronic malabsorption.
BOX 121-7
Inadequate dietary intakeTotal vegetarianism: no eggs, milk, or cheeseChronic alcoholism (rare)
Inadequate absorptionAbsent, inadequate, or abnormal intrinsic factor, as seen in
patients with pernicious gastrectomy and anemia. In anemia, autoimmune antibodies act against gastric parietal cells and intrinsic factor.
Abnormal ileum, as can occur in sprue and inflammatory bowel disease
Inadequate useEnzyme deficiencyAbnormal vitamin B12–binding protein
Increased requirement by increased body metabolismIncreased excretion or destruction
Causes of Vitamin B12 Deficiency
BOX 121-6
Inadequate dietary intakePoor diet or overcooked or processed food dietAlcoholism
Inadequate uptakeMalabsorption with sprue and other chronic upper intestinal
tract disorders, drugs such as phenytoin and barbiturates, or blind loop syndrome
Inadequate useMetabolic block caused by drugs such as methotrexate or
trimethoprimEnzymatic deficiency, congenital or acquired
Increased requirementPregnancyIncreased RBC turnover: ineffective erythropoiesis, hemolytic
anemia, chronic blood lossMalignant disease: lymphoproliferative disorders
Increased excretion or destruction or dialysis
Causes of Folate Deficiency
CLINICAL FEATURES PATHOLOGIC CONDITION
Lemon yellow skin Combination of pallor with low-grade icterus from ineffective erythropoiesis
Petechiae, mucosal bleeding Thrombocytopenia
Infection Leukopenia
Fatigue, dyspnea on exertion, postural hypotension
Anemia
Sore mouth or tongue Megaloblastosis of mucosal surfaces
Diarrhea and weight loss Malabsorption from mucosal surface change
Paresthesias and ataxia Related to myelin abnormality in vitamin B12 deficiency only
Table 121-4Clinicopathologic Correlation of Manifestations of Megaloblastic Anemia

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1593
Figure 121-6. Megaloblastic anemia with macrocytic red cells and hypersegmented polymorphonuclear neutrophils. (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:61.)
TEST TECHNIQUE VALUE INTERPRETATION
Vitamin B12 Microbiologic or radioisotope
Normal: 300-900 µg/L Although they may overlap clinically, vitamin B12 level is usually normal in folate deficiency.Deficient: <200 µg/L
Folate Microbiologic or radioisotope
Deficient: <3 µg/L Vitamin B12 deficiency may elevate folate levels by blocking transfer of serum folate to RBCs; hemolysis may elevate folate levels.
Red cell folate Calculated Normal: 200-700 µg/L Index of tissue folate is less influenced by diet and is increased in vitamin B12 deficiency because of block.Folate deficiency: <140 µg/L
Lactate dehydrogenase Spectrophotometric Normal: 95-200 IU Normal in other macrocytic anemias; elevated two to four times normal in hemolytic anemias; isoenzymes may be helpful.
Megaloblastic anemia: 4-50 times normal
Table 121-5 Serum Tests for Diagnosis and Differentiation of Megaloblastic Anemia
the most common cause.10 Macrocytic target cells may be seen on the peripheral smear in conjunction with this disorder. Hypothy-roidism and hemolysis may also be manifested as macrocytic anemia. Screening tests to differentiate between megaloblastic anemia and macrocytic anemia of other causes include a periph-eral smear for macro-ovalocytes, hypersegmented polymorpho-nuclear neutrophils, and the LDH level.
Normochromic and Normocytic Anemias. The origin of normo-chromic and normocytic anemias secondary to decreased produc-tion is not as obvious as that of macrocytic and microcytic anemias because the latter give clues to their origin by alterations in RBC indices. One hematologic parameter that can aid in the diagnosis of normocytic anemia associated with hypoproduction is the cor-rected reticulocyte count. Reticulocytes reflect RBC production in bone marrow. They are RBCs released from bone marrow every 1 to 3 days and contain residual RNA that can be detected by supra-vital staining. Reticulocytes have an average MCV of 160 fL and in sufficient numbers can increase the MCV of the total erythro-cyte count. The reticulocyte count is expressed as a percentage of
the total RBC population and needs to be related (“corrected”) to the RBC count of the patient. Thus the corrected reticulocyte count is equal to the measured percentage of reticulocytes times the patient’s hematocrit (%) divided by 45% (taken as the normal hematocrit). The normal range is 1 to 3%.
Normocytic anemia may be classified as being due to primary bone marrow involvement or a secondary marrow response to underlying disease.
Aplastic anemia is rare but may have severe manifestations. It is suspected in anemic patients with normal indices, a low reticulocyte count, and a history of exposure to certain drugs or chemicals (Table 121-6). It is related to drug or chemical exposure in 50% of cases. Viral hepatitis, radiation, and pregnancy have been associated with aplastic anemia. Another group of patients is considered to have an “autoimmune” origin.
The aplastic state may extend to all cell lines and results from destruction by immune-stimulated lymphocytes or failure of the marrow stem cell. On occasion, only one cell line fails, as in RBC aplasia. This condition represents injury occurring at a later stage of cellular differentiation. The precise diagnosis necessitates bone marrow examination, but the causative factor may be difficult to determine.
General treatment of aplastic anemia includes removal of sus-pected marrow toxins from the environment, avoidance of aspirin, oral hygiene, and suppression of menses. Transfusions are given in life-threatening circumstances only. Bone marrow or peripheral blood stem cell transplantation from a histocompatible sibling can cure the bone marrow failure, with survival rates of 78 to 94% reported.10 However, because just 30% of patients have suit-ably matched sibling donors, only a small number undergo allo-geneic transplantation. Immunosuppression with antithymocyte globulin, antilymphocyte globulin, and other cytotoxic chemo-therapy is used in the majority of patients who are not stem cell
CAUSE RELATIVE INCIDENCE (%)
Chloramphenicol 61
Phenylbutazone 19
Anticonvulsants 4
Insecticides 4
Solvents 4
Sulfonamides 3
Gold 3
Benzene 2
From Silver BJ, Zuckerman KS: Aplastic anemia: Recent advances in pathogenesis and treatment. Med Clin North Am 64:607, 1980.
Table 121-6Aplastic Anemia Caused by Drugs or Chemicals

1594 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
rheumatoid arthritis, chronic infections such as tuberculosis and osteomyelitis, and malignant disease). Hypoendocrinism caused by hypothyroidism, hypoadrenalism, or hypopituitarism results in a hypometabolic state in which the bone marrow responds poorly to erythropoietin. Erythropoietin levels may be low. The anemia of chronic renal failure is thought to be caused by a number of factors including decreased erythropoietin production, hemolysis, suppression by dialyzable factors, and increased blood loss caused by platelet abnormalities. If necessary, it may be corrected by erythropoietin replacement therapy.13
Increased Red Blood Cell Destruction
The hemolytic anemias are defined by a shortened life span of the erythrocyte. In their acute form, hemolytic anemias can be devastating and require rapid diagnosis and intervention (see Box 121-1). Fortunately, they are relatively rare in comparison to the chronic hemolytic conditions. Chronic disorders may be related to primary blood disorders (e.g., sickle cell anemia) or may be a result of other disease states (e.g., chronic renal failure). These disorders may be manifested as acute hemolytic anemia if the tenuous balance between RBC production and destruction is upset. If the patient can be demonstrated to have a normal hema-tocrit and reticulocyte count at the same time, differentiation between acquired and inherited hemolytic anemia is possible.
Clinical Features. The clinical signs and symptoms of hemolytic anemia are, in general, caused by either intravascular or extravas-cular processes. Although it is not a precise representation of the underlying pathophysiologic condition, this division assists in the differential approach in the emergency department.
Intravascular hemolysis is usually associated with an acute process and has a dramatic appearance. Large numbers of RBCs may be lysed within the circulation. The pathologic process pri-marily involves the handling of released hemoglobin and a com-pensatory response to an acute decrease in oxygen-carrying capability. Free hemoglobin initially binds to haptoglobin and hemopexin. This complex is transported to the liver, converted to bilirubin, conjugated, and excreted. When this binding and trans-port system is overwhelmed, free hemoglobin may appear in the blood. Hemoglobin is a large molecule that remains in serum and may tint it pink.
In contrast, myoglobin is a small molecule that is rapidly cleared from serum. Examination of spun whole blood demonstrates clear serum in myoglobinemia, pink serum with free hemoglobin from intravascular hemolysis, and yellow serum from extravascular hemolysis with increased bilirubin production. In severe cases, the last mechanism may also result in free hemoglobin.
The clinical appearance of intravascular hemolysis may vary from mild chronic anemia, as seen in cases of mechanical hemo-lysis, to prostration, fever, abdominal and back pain, and mental changes, as seen with transfusion reactions. Jaundice, brown to red urine, and oliguria associated with acute renal failure induced by the hemoglobin complex can also occur.
Extravascular hemolysis is more common and usually better tolerated. Splenic blood flow slows as RBCs travel in the sinusoids close to the reticuloendothelial system, which is uniquely designed for removal of older or damaged cells. Primary splenic overactiv-ity, antibody-mediated changes, or RBC membrane abnormalities may cause this normal splenic function to increase to a pathologic degree. Hemolysis may also occur within the bone marrow. As stated previously, normal erythropoiesis is ineffective 10 to 20% of the time. This percentage increases when abnormal RBCs are produced, as in thalassemia, megaloblastic anemia, or some hemo-lytic anemias.14
After hemoglobin is disassembled in the reticuloendothelial cell, globin returns to the amino acid pool, iron is transported by transferrin to the bone marrow or iron stores, and the pyrrole ring
transplantation candidates. Unrelated donors are preferred to avoid sensitization of the patient against the non-HLA antigens that are present in bone marrow from a family donor. The disease has a wide range of severity, and the overall 5-year survival rate is 30 to 40%. Given supportive therapy, up to 80% of patients with severe aplastic anemia still die. Bone marrow transplantation before blood product sensitization has resulted in an 80% 5-year survival rate. This is usually combined with immunosuppressive therapy consisting of antilymphocyte globulin. Difficulty is still encountered in finding the correct immunologic match.11,12
Myelophthisic anemia is bone marrow failure resulting from replacement by an invading tumor, leukemia, lymphoma, or, rarely, granuloma. A more basic defect or inhibitor may compli-cate the problem because the degree of anemia cannot always be correlated with the extent of bone marrow invasion. Any patient with oncologic disease may be subject to the development of this type of anemia. Useful clues are signs of extramedullary hemato-poiesis, such as hepatosplenomegaly and a leukoerythroblastic peripheral smear that demonstrates immature WBCs, nucleated RBCs, and poikilocytosis (teardrop-shaped red cells) (Fig. 121-7). The final diagnosis is made by bone marrow examination. Therapy is directed at the underlying disorder.
Myelofibrosis of unknown origin is the usual cause of primary bone marrow failure associated with extramedullary hematopoi-esis. This myeloid metaplasia occurs in the liver and spleen and imparts a blood picture similar to that of myelophthisic anemia. The diagnosis may be made by bone marrow examination. Treat-ment is supportive, although splenectomy or the use of alkylating agents may be necessary to treat complications of extramedullary blood cell production, such as hepatosplenomegaly.
The hypoplastic anemias of secondary origin are commonly seen as mild chronic anemias with low reticulocyte counts. They have a normal MCV and RDW. Their diagnosis is made by exclu-sion. Anemia of chronic disease may have microcytic or normo-cytic indices. It is associated with chronic inflammation (e.g.,
Figure 121-7. Anisocytosis and poikilocytosis. (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:113.)

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1595
reflects the presence of younger cells associated with reticulocyto-sis. The specific diagnosis may be made by a blood smear, as with sickled cells or Heinz bodies in glucose-6-phosphate dehydroge-nase (G6PD) deficiency.
Haptoglobin binds hemoglobin on a molecule-for-molecule basis. Its absence implies saturation and degradation after binding with hemoglobin and is an early finding in hemolysis. It has a normal range of 40 to 180 mg/mL, is decreased in hepatic failure, and increases as an acute-phase reactant. After haptoglobin is bound, hemoglobin binds with hemopexin, transferrin, and albumin before circulating in its free form. Plasma free hemoglo-bin levels are determined in suspected cases of intravascular hemolysis. The result is considered positive if the level is greater than 40 to 50 mg/dL. Hemoglobin is excreted by the kidney and may be found as a smoky red pigment that is orthotoluidine posi-tive with no associated RBCs. Prussian blue–staining granules of hemosiderin may be found intracellularly in renal tubule cells excreted in urine during chronic hemolytic states.
LDH is released when the RBC is broken down peripherally or in the marrow. It is elevated in hemolytic, thalassemic, sidero-blastic, and megaloblastic anemia. It may also be seen in cases of uremia, polycythemia vera, and erythroleukemia. Normal levels of LDH range from 95 to 200 IU and may be fractionated.
In extravascular hemolysis, bilirubin is often delivered to the liver faster than the conjugating mechanism can handle it. Normal total levels are less than 1.5 mg/dL, and the indirect com-ponent amounts to less than 0.5 mg/dL. Conjugated or indirect bilirubin may rise as high as 4 or 5 mg/dL even with normal liver function. Higher levels connote some degree of underlying hepatic insufficiency.
The direct antiglobulin (Coombs’) test detects antibody or complement on human RBC membranes. It is an essential test in the evaluation of hemolysis. Approximately 90% of patients with autoimmune hemolytic anemia have a positive direct Coombs’ test result (warm agglutinin autoimmune hemolytic anemia). The indirect test measures antibody titers in serum (cold agglutinin autoimmune hemolytic anemia). The key to the direct antiglobu-lin test is the reagent. It contains an antihuman immunoglobulin (Ig) G that is produced in rabbits. This antihuman IgG in its broad-spectrum form reacts with the IgG, IgM, or C3 proteins that may coat RBCs. The reaction causes an agglutination of RBCs that is graded 0 to 4. Agglutinating properties depend on the size of the immunoglobulin. IgM is a large antibody form that can bridge the distance between cells, cause agglutination, and fix comple-ment. The direct antiglobulin test is limited in diagnosis of IgM-mediated hemolysis. It is best in determining IgG or complement on the RBC surface. IgG is not large enough to cause agglutina-tion, and the antihuman globulin attaches to RBC-bound IgG, which allows agglutination. C3 is detected in a similar manner. Both represent possible immunologic causes of hemolysis. This form of hemolysis is usually mediated extravascularly through the
Figure 121-8. Schizocytes (fragmented cell and nucleated red cells). (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:115.)
Figure 121-9. Spherocytosis. (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:115.)
BOX 121-9
Peripheral blood smearCorrected reticulocyte index or reticulocyte production indexHaptoglobin levelsPlasma free and urinary hemoglobinLactate dehydrogenase levelFractionated bilirubin levelDirect and indirect Coombs’ testRBC membrane stability (osmotic fragility)
Diagnostic Tests for Hemolysis
BOX 121-8
HistoryAlteration of color in urine or fecesAssociation with drugs, cold, sleepEarly or recent-onset anemia history with symptomsEthnic backgroundFamily history of anemia or jaundiceDrug or toxic exposureDisease states associated with hemolysis, such as systemic lupus
erythematosus, renal failure, lymphoma, infectious mononucleosis, prosthetic heart valve
Physical ExaminationJaundiceHepatosplenomegalyUlcerations, particularly in the lower extremitiesEnlarged lymph nodes
Pertinent Factors in the History and Physical Examination for Hemolytic Anemia
is converted to bilirubin. The unconjugated bilirubin circulates to the liver and is transformed. It is excreted in urine as conjugated bilirubin. The clinical picture of extravascular hemolysis is usually mild to moderate anemia, mild and intermittent jaundice, and enlargement of the spleen. The signs and symptoms vary with the severity and chronicity of the hemolysis.
Ancillary Evaluation. Once hemolysis is suspected, the history and laboratory tests have diagnostic precedence over physical examination. Important historical and physical examination points are listed in Box 121-8.
Laboratory Assessment. Important diagnostic tests for hemoly-sis are provided in Box 121-9.
The blood smear is often more diagnostic than bone marrow examination. The typical cell seen in intravascular hemolysis is the schizocyte (Fig. 121-8). The classic cell of extravascular hemolysis is the spherocyte (Fig. 121-9). It may be seen in congenital sphe-rocytosis but more commonly indicates splenic activity against an antibody-coated RBC membrane. An increase in macrocytes

1596 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
The older cells lyse at certain drug levels. The oxidant creates forms of activated oxygen, such as peroxide, that either denature the hemoglobin or destroy cell membranes. The former process produces Heinz bodies, which are clumps of denatured hemoglo-bin found in RBCs early during an episode. These cells are removed by the spleen. The diagnosis is made by enzymatic screening for G6PD, but this test cannot be performed immediately after the hemolytic episode. A 3-week delay avoids a false-negative result caused by a predominance of young cells. Treatment includes volume and RBC support as necessary. Avoidance of oxidant drugs is the only prevention.
Intrinsic Membrane Abnormality. These abnormalities are manifested in a number of ways. An altered shape is the main feature of autosomal dominant hereditary spherocytosis or ellip-tocytosis. The spleen sequesters these abnormal cells. Clinical sequelae range from compensated asymptomatic anemia to severe life-threatening acquired aplastic crises. The diagnosis is made by reviewing the family history, blood smear, and osmotic fragility testing. Splenectomy is the treatment of choice for patients requir-ing therapeutic intervention.
Paroxysmal nocturnal hemoglobinemia is a stem cell defect causing abnormal erythrocyte, neutrophil, and platelet sensitivity to complement. It is most often seen as chronic hemolysis, hemo-siderinuria, leukopenia, and thrombocytopenia. The peripheral smear is normal and the direct Coombs’ test result is negative. Its major complication is thrombosis, with a predilection for the hepatic vein. Normal activation of complement with the use of sucrose or acid hemolysis (the Ham test) is diagnostic. Transfusion can be a life-threatening hazard in patients with this disease because RBC lysis is caused by donor complement. Because of this danger, only washed packed cells should be used.
Intrinsic Hemoglobin Abnormality. More than 350 types of abnormal hemoglobin have been documented. Problems that may be seen include unstable hemoglobins that appear as Heinz body–positive anemia, M hemoglobins that fix iron in its ferric or met-hemoglobin state, and hemoglobins with increased oxygen affinity that result in tissue hypoxia and erythrocytosis.
Sickle Cell Disease. Sickle cell disease is the most important hemoglobinopathy with which the emergency physician should be familiar. In hospitals serving a large African American population, it is seen on an almost daily basis. Even experienced physicians may overlook major complications. Clinicians with less experience may fail to recognize the complexity of the disease and the many potential complications.15
Pathophysiology. Sickle cell disease is genetically determined. An abnormal allele at the gene loci for hemoglobin β chains pro-duces altered messenger RNA, which in turn results in replace-ment of glutamic acid by valine at the sixth position from the N-terminal end of the β chain. On the molecular level, this change causes an interlocking of the affected chain with adjacent hemo-globin in the deoxygenated state. This connection causes the for-mation of bundles of parallel rods called tactoids, polymers that grow to form a p-crystalline gel, and then a crystal. Gel formation is facilitated by low pH and reduced by the presence of other hemoglobins, such as HbF. The result is a sickled cell that is less
spleen because IgG is a poor initiator of the complement system. The direct antiglobulin test evaluates the RBC surface for immu-nologic markers. The indirect test assumes that IgG or C3 is in the serum and tests for serum antibody activity against RBCs. Positive test results for immunologic markers do not correlate agglutina-tion activity with the severity of hemolysis.14
Differential Diagnosis. Hemolytic anemias may be classified as congenital or acquired, Coombs’ positive or Coombs’ negative, or caused by processes intrinsic or extrinsic to the cell membrane. The last method gives a useful differential classification of hemo-lysis (Box 121-10).
Intrinsic Enzyme Defects. Eighty-five percent to 90% of the membrane-sustaining energy production of the erythrocyte is through the anaerobic glycolytic pathway. At least eight known enzyme deficiencies are associated with this pathway. The most common is pyruvate kinase deficiency, which is manifested with hemolytic jaundice and is usually diagnosed in infancy.
The remaining 10 to 15% of RBC glycolysis occurs by way of the hexose monophosphate shunt. This bypass mechanism occurs in the early stages of the glycolytic pathway and generates reduced nicotinamide adenine dinucleotide phosphate (NADPH), which is important in maintaining reduced glutathione. Glutathione is essential in the protection of hemoglobin from oxidant injury. A deficiency of the first enzyme in this pathway, G6PD, occurs in 11% of African American men. In this form, the enzyme deterio-rates with age, and older RBCs are subject to hemolysis by oxidant stress. G6PD deficiency is sex linked and has a wide range of sever-ity. The most common form in African Americans is self-limited because as the bone marrow responds, younger cells with more normal levels of G6PD predominate and can handle the oxidant stress. The variants in Sicilians, Greeks, and Arabs can be particu-larly devastating. The clinical manifestation is usually an acute hemolytic episode that may be both intravascular and extravascu-lar in appearance. It occurs 24 to 48 hours after the ingestion of an oxidant drug (Box 121-11) or after acute infections such as viral hepatitis. The anemia induced by oxidant drugs is dose related.
BOX 121-10
IntrinsicEnzyme defect
Pyruvate kinase deficiencyGlucose-6-phosphate dehydrogenase deficiency
Membrane abnormalitySpherocytosisElliptostomatocytosisParoxysmal nocturnal hemoglobinuriaSpur cell anemia
Hemoglobin abnormalityHemoglobinopathiesThalassemias (anemias)Unstable hemoglobinHemoglobin M
ExtrinsicImmunologic
AlloantibodiesAutoantibodies
MechanicalMicroangiopathic hemolytic anemiaCardiovascular, such as prosthetic heart valve disease
EnvironmentalDrugsToxinsInfectionsThermal
Abnormal sequestrations, as in hypersplenism
Classification of Hemolytic Anemia BOX 121-11
Analgesics and antipyretics: acetanilid, aspirin, phenacetinAntimalarials: primaquine, quinacrine, quinineNitrofuransSulfa drugs: sulfamethoxazole, sulfacetamide, sulfonesMiscellaneous: naphthalene, fava beans, methylene blue,
phenylhydrazine, nalidixic acid
Drugs Associated with Hemolysis in G6PD Deficiency
G6PD, glucose-6-phosphate dehydrogenase.

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1597
cause stasis, deoxygenation, and local acidosis, which promote the vicious circle of continued sickling. The pain is commonly deep and aching and is most often found in the abdomen, chest, back, and extremities. The disease may mimic an acute abdomen (e.g., cholecystitis), pulmonary embolus, renal colic, or other painful problems. A directed history that relates this pain pattern to previ-ous sickling episodes, a careful repeated physical examination, and specific organ-related laboratory tests are all the physician has to differentiate “uncomplicated” crises from a more serious patho-logic condition. Children may be seen more often with skeletal crises leading to bone deformities. In these cases, osteomyelitis and bone infarct needs to be differentiated.22
Neurologic complications can occur and include transient isch-emic attacks, cerebral infarction, spinal cord infarction, vestibular hearing problems, and hearing loss.23 Neurologic complications occur in 25% of patients with sickle cell anemia by the time they are 45 years old; 13% demonstrate infarction or ischemia in the absence of symptoms.24 Transcranial Doppler study may be useful in identifying individuals with sickle cell disease who are at risk for stroke.25 The use of exchange blood transfusions with the goal of hemoglobin S less than 30% can reduce the risk of cerebrovas-cular events by 92%.26 In the setting of an acute stroke, exchange transfusion is recommended with the goals of hemoglobin S of less than 30% and a total hemoglobin level limited to 10 g/dL.27,28 Tissue plasminogen activator (tPA) should be considered in adult sickle cell disease patients with acute nonhemorrhagic strokes. The use of tPA in this setting is the same as for acute stroke without sickle cell disease.28
Acute chest syndrome is the most common pulmonary disease associated with sickle cell disease and one of the most common causes of death.29 It is a common cause of hospitalization in sickle cell disease, second only to vaso-occlusive crisis. Patients with acute chest syndrome have fever, cough, chest pain, dyspnea, and new infiltrates on the chest radiograph. The pathophysiologic mechanism of the syndrome is not well understood, but it may be a specific form of acute lung injury. The injury is postulated to be related to pulmonary microvascular sludging, infarction of pul-monary parenchyma, and bone marrow fat embolization from infarcted bone. Macrovascular pulmonary embolism and infec-tion may also have a pathogenetic role. Although the causes of acute chest syndrome are uncertain, approximately 54% of the cases are associated with infection, including Mycoplasma and Chlamydia.30 The differential diagnosis includes pneumonia, pul-monary embolism, congestive heart failure, and adult respiratory distress syndrome. No definitive diagnostic study is available, and diagnosis is based on the presence of the clinical features and exclusion of other pulmonary causes, as mentioned in the differ-ential diagnosis. Management is primarily supportive and consists of hydration, analgesia, incentive spirometry, maintenance of adequate oxygenation and ventilation, and empirical antibiotics. Approximately 13% of patients will have respiratory failure severe enough to require mechanical ventilation. Antibiotic choice is similar to that for pneumonia in other populations. Exchange blood transfusions, as used in a similar fashion with acute stroke, are often used and have been associated with better gas exchange in acute chest syndrome.31,32 However, there are no randomized controlled studies demonstrating an improvement in outcome with the transfusions.
Although most of the diagnostic and therapeutic problems of sickle cell disease are related to vaso-occlusive crises, other serious complications should be anticipated. Sickle cell disease is a chronic hemolytic state with reasonably compensated hematocrit values in the 20 to 30% range and elevated reticulocyte counts. This compensated balance may be disrupted by a rare iron deficiency or, more commonly, by folate deficiency. A potentially life-threatening aplastic crisis may be seen as a result of suppression of erythropoiesis by an acute postinfectious condition or folate
deformable, an increase in the viscosity and sludging tendency of blood, and the sequestration of RBCs in the spleen and liver. These changes may occur when smaller amounts of polymer do not result in a sickled cell and are associated with an RBC membrane leak. The clinical complex of vaso-occlusive events, chronic hemo-lysis, thrombosis, and organ injury is derived from this pathologic process. Patients with sickle cell disease generally fall into two phenotypic groups: hemolysis phenotype and vaso-occlusion phe-notype. These groups are not genetically determined, and it is still unknown why some people fall into one group versus the other. Patients prone to hemolysis typically do not have pain, stroke, or acute chest syndrome; instead, they typically have pulmonary hypertension and leg ulcers. Their hemoglobin tends to be very low but their LDH is usually high. Patients with the vaso-occlusion phenotype typically have pain, acute chest syndrome, and stroke; they have a higher hemoglobin or high WBC level and lower LDH and indirect bilirubin concentrations.
The globin in hemoglobin is made up of two pairs of identical polypeptide globin chains. Each person has two non–sex-linked gene foci for β-globin chains, one from each parent. Normal indi-viduals express six different types of hemoglobin from varying globin chain combinations: three embryonic hemoglobins, HbA (α2β2), HbA2 (α2δ2), and HbF (α2γ2). Embryonic hemoglobins are expressed only in utero, and after 6 months of age, HbA accounts for more than 95% of hemoglobin in a normal individual. The sickle syndromes result from mutations in the β-globin gene. Instead of HbA (α2β2), an abnormal hemoglobin HbS is produced. Embryonic and fetal hemoglobins do not contain β-globin; thus there are no clinical manifestations in early infancy. As their pro-duction declines, normal HbA (α2β2) cannot be produced, and symptoms develop.
In sickle cell trait (HbAS), the patient is heterozygous and only one parent contributes the abnormal S allele. In each cell approxi-mately 40% of the hemoglobin is HbS. Sickle disease (HbSS) is homozygous, and more than 85% of the hemoglobin is HbS. Because a parent may contribute alleles other than S, a wide number of variants can exist. Two clinically important S variants are sickle cell–β-thalassemia and sickle cell–hemoglobin C disease. Therefore, not all hemoglobinopathies that cause sickling are HbS. In addition, HbSS is not limited to the African American popula-tion. Up to 10% of patients with various sickling disorders are not ethnically African American.16,17
The sickle cell trait is found in 8 to 10% of African Americans. The diagnosis is usually made after sickle cell screening (Sickledex) and a characteristic result on hemoglobin electrophoresis. Most individuals with sickle cell trait are asymptomatic but can present with spontaneous hematuria, renal papillary necrosis, splenic infarction, venous thromboembolism, traumatic hyphema, exer-tional rhabdomyolysis, and exertional sudden death.15,18,19 Recent literature suggests that pregnancy in women with sickle cell trait is not associated with an increased risk of adverse events.20 In patients with sickle cell trait who have eye trauma, serial tonometry and observation are indicated to monitor for ocular complications.
Clinical Features. Sickle cell disease can be a recurrent, painful, and frustrating problem for both patients and physicians. A study suggests that as many as 35% of a sickle cell population are recurrent emergency department users.21 Sickle cell disease is characterized by two major clinical features, hemolysis and acute vaso-occlusive events. The hallmark manifestation of sickle cell disease and the most common reason for emergency department visits is the painful vaso-occlusive crisis. Preceding infection, cold exposure, and stress such as trauma are all potential precipitating factors. Many episodes are thought to be spontaneous. The painful crisis is believed to have its origin in tissue ischemia caused by increased viscosity, sludging, and microvascular obstruction as a result of irreversibly sickled cells. Sludging and vascular blockage

1598 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
of a slow but longer growth period caused by the delayed onset of puberty, adult patients with HbSS often have a youthful appear-ance and long, thin extremities. In a patient with suspected sickle cell disease, inquiry should be made into the family history, previ-ous pain episodes, and symptoms relative to chronic anemia, sus-ceptibility to infection, and ischemic organ damage. Table 121-7 suggests an outline to follow for the physical examination.
Most patients, other than those with mild pain crisis, should have a complete blood count performed, and current blood levels should be compared with those of previous visits. A reticulocyte count is recommended whenever the patient’s hemoglobin level has decreased by 2 g/dL from baseline. In sickle cell disease, the typical absolute reticulocyte count is three or four times the upper limit of normal. A reticulocyte count 3% or lower than the patient’s usual value may suggest an aplastic crisis. A reticulocyte count greater than 12%, particularly if it is accompanied by numerous nucleated RBCs, may indicate rapid hemolysis. Other laboratory tests are selected on the basis of potential organ complications. Unfortunately, no test is available that detects whether a patient is in a crisis. Currently, this difficult task is based on clinical grounds. In new cases, the peripheral smear may show sickled cells (Fig. 121-10), and a sickle cell screening test with Sickledex may help. Definitive diagnosis of sickle cell disease is aided by hemoglobin electrophoresis.
Management. The antisickling agent hydroxyurea reduces the frequency of painful crises in adults with a history of three or more crises annually. The beneficial effects of hydroxyurea in sickle cell disease are assumed to be due to induction of hemoglobin F, but additional mechanisms may be operative. Hydroxyurea can reduce the incidence of acute painful crisis as well as increase survival in sickle cell disease. However, the effects of hydroxyurea can take weeks to be appreciated, and it is not routinely recommended for acute episodes.35,36 Other agents, including clotrimazole, magne-sium, 5-azacitidine, erythropoietin, and butyric acid, may have a future role in therapy.37,38 Bone marrow transplantation offers the only current cure for sickle cell disease and is associated with survival rates greater than 90% and disease-free survival rates of 80 to 90%. However, the role of bone marrow transplantation in sickle cell disease remains uncertain because of the inability to predict which patients will benefit, limited patient eligibility as a result of advanced pulmonary and neurologic vasculopathies, and concerns related to transplantation mortality and treatment-induced malignant neoplasms.37,38
deficiency. This aplastic condition is suspected when the hemo-globin level falls 2 g/dL or more from previous stable levels and the reticulocyte count remains low (<2%).
Finally, children may have an acute splenic sequestration syn-drome. This syndrome involves acute splenic enlargement from increased intrasplenic sickling and obstruction. The child may demonstrate lassitude and be in shock. Each of these conditions may result in a rapidly falling RBC count and progressive symp-toms of anemia. Patients with HbSS are also subject to all other causes of anemia, such as hemolysis from G6PD deficiency. An increased susceptibility to infection is well documented with HbSS.
In infancy, an increased incidence of sudden death may be related to pneumococcal sepsis and meningitis. A WBC count and blood cultures should be performed on all febrile children with sickle cell anemia. HbSS patients who are younger than 2 years and have associated temperatures of 39.5° C or higher and WBC counts greater than 20,000/mm3 should be given intravenous anti-biotics immediately. Adults with fever require careful evaluation and laboratory assessment, including appropriate cultures. Early institution of appropriate antibiotics, such as ceftriaxone 1 to 2 g, adult dose, intravenously or intramuscularly, is necessary in patients with a discernible source of infection. In children and adults, infections with Staphylococcus and Pneumococcus species and Haemophilus influenzae are particularly common.33 An increased incidence of Salmonella osteomyelitis also occurs.34 The origin of this related immunologic deficiency is believed to be multifactorial, involving functional asplenia, poorly migrating neutrophils, and decreased opsonin production.34
Major, chronic organ damage in patients with sickle cell anemia is common. A cross section of these problems is listed in Table 121-7. These associated conditions should be quickly reviewed every time a patient with sickle cell anemia enters the emergency department. The leading causes of death in HbSS patients are cardiopulmonary disease, chronic renal failure, stroke, and infection.15
Diagnostically, most patients with HbSS seen in the emergency department are well known with defined pain patterns. Because
Figure 121-10. Sickle cells. (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:103.)
ORGAN OR SYSTEM INJURY
Skin Stasis ulcer
Central nervous system Cerebrovascular accident
Eye Retinal hemorrhage, retinopathy
Cardiac Congestive heart failure
Pulmonary Intrapulmonary shunting, embolism, infarct, infection
Vascular Occlusive phenomenon at any site
Liver Hepatic infarct, hepatitis resulting from transfusion, hepatic sequestration, intrahepatic cholestasis
Gallbladder Increased incidence of bilirubin gallstones caused by hemolysis
Spleen Acute sequestration
Urinary Hyposthenuria, hematuria
Genital Decreased fertility, impotence, priapism
Skeletal Bone infarcts, osteomyelitis, aseptic necrosis
Placenta Insufficiency with fetal wastage
Leukocytes Relative immunodeficiency
Erythrocytes Chronic hemolysis
Table 121-7 Organ Damage Seen in Sickle Cell Disease

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1599
Exchange transfusions are recommended for patients, particu-larly children, with cerebrovascular accidents. Acute symptoms may be reversed and the frequency of recurrence decreased with a regulated 3- or 4-week transfusion program. The goal is to sup-press reticulocytosis and to decrease the HbS level to less than 25%. Rarely, transfusions are given for control of bone or visceral crises. This is not an emergency department procedure and is considered only after hematologic consultation. Prophylactic transfusions to dilute HbS levels are also recommended in preg-nancy and before major surgery.40 As discussed before, for stroke in children, acute exchange transfusion is the treatment; for adults, the treatment is tPA.
A number of other therapies are being tested for both prophy-laxis and crisis management, including supplemental zinc, induced hyponatremia, gelation inhibitors, membrane-active agents, and gene manipulation. Poloxamer 188 is an artificial surfactant with hemorheologic and antithrombotic properties. Although the mechanism of action of this agent is not fully understood, it improves microvascular blood flow by reducing blood viscosity and adhesive frictional forces. In clinical trials of sickle cell patients with acute painful crisis, poloxamer reduced the total narcotic requirement, duration of pain, and pain intensity.42
Sickle Cell–β-Thalassemia. Sickle cell–β-thalassemia disease is seen most commonly in people of Mediterranean descent. The severity of the disease is related to the concentration of HbS in RBCs and the decrease in MCHC. It should be considered in a patient with a low MCV and a positive response on sickle prepara-tion. It is generally a milder form than homozygous HbSS but can be as severe as sickle cell disease. HbSC disease falls between HbSS and HbS-thalassemia in terms of severity. In addition to many of the complications of HbSS, HbSC disease has an increased inci-dence of eye hemorrhage and pregnancy complications and may cause splenomegaly. The peripheral smear demonstrates a combi-nation of sickled cells and normocytic target cells.
Extrinsic Alloantibodies. Alloantibodies are formed in re-sponse to foreign RBC antigens. In the case of the ABO system, these antibodies are preformed. The ABO system is one of the most important RBC wall antigens. ABO incompatibility resulting in donor cell destruction by the recipient’s alloantibodies can be a life-threatening reaction. These antibodies are IgM in nature and can act as a hemolysin, both agglutinating RBCs and fixing com-plement and consequently causing intravascular hemolysis.
The Rh system is another set of antigens on the RBC. This system is unique in that individuals do not have antibodies that correspond to antigens in the Rh system unless they have been sensitized by previous exposure to antigens that they lack. The antibodies produced are IgG in nature, and they accelerate extra-vascular destruction of RBCs by the spleen and liver. Most auto-immune antibodies are directed toward antigens in the Rh system.
Extrinsic Autoantibodies. Evaluation of autoimmune hemoly-sis is as complex as its origin. The major feature of autoimmune hemolysis is the production of an IgG or IgM antibody to an antigen present on the RBC membrane. Why the body responds in this manner is unknown. IgM antibodies can agglutinate, fix complement, and act as intravascular hemolysins. IgG antibodies may fix complement to the cell but do not usually complete the hemolysis process. These IgG- or C3-labeled cells undergo acceler-ated extravascular destruction. The direct antiglobulin test is useful in revealing these labeled cells.43
Autoimmune hemolytic anemias are acquired disorders, with 40 to 50% being idiopathic. The remainder are associated with a number of diseases (Box 121-12). Classification of autoim-mune hemolytic anemias is based on the optimal temperature at which the antibody reacts with the RBC membrane. Therefore, there are warm-reacting (>37° C) and cold-reacting (<37° C) antibodies.
Current therapies, including rest, adequate nutrition, hydration, oxygenation, analgesia, transfusion, and therapy for infection, are directed toward symptomatic relief and attempts to stop the cycle of deoxygenated sickling and intravascular sludging. Most patients with sickle cell anemia are mildly dehydrated because of difficulty in concentrating urine. Fluid replacement can be oral or intrave-nous, and the emergency physician should be aware of the poten-tial for congestive heart failure in patients past their second decade. A recommended starting solution is 5% dextrose in half-normal saline at a rate not to exceed 1.5 times maintenance.15,39 Oxygen through a nasal cannula at 2 to 4 L/min may help hypoxic patients and may be given to any patient with HbSS as a low-risk treatment modality with potential benefit.
Analgesia is a major benefit and essential early therapy for acute sickle cell crisis. Because a small subgroup of patients repeatedly and frequently seek care in the emergency department, emergency department caregivers may become understandably suspicious of needs and motivations. Care protocols are advised to ensure rapid appropriate treatment. Many emergency physicians caring for large populations of sickle cell patients have developed protocols to establish better physician-patient rapport and to lessen the chance of narcotic addiction and manipulation. The following is a protocol for severe pain in adults and children weighing more than 50 kg: patients are evaluated, treated with oxygen and hydration, and given intravenous morphine sulfate, 5 to 10 mg every 2 to 4 hours, or intravenous hydromorphone, 1.5 mg every 3 to 4 hours. For children weighing less than 50 kg, intravenous bolus doses of morphine sulfate, 0.1 to 0.15 mg/kg, can be given every 2 to 4 hours, or intravenous hydromorphone, 0.015 to 0.020 mg/kg, can be given every 3 to 4 hours.28 At 4 to 6 hours, the patient is allowed to decide whether inpatient or outpatient therapy is desired. Out-patient therapy includes 4 to 6 days of an effective oral analgesic. A 40-mg dose of oral morphine sulfate or equivalent is given 1 or 2 hours before the infusion is stopped. Such a protocol may bring uniformity to the patient’s expectations for care and the physician’s decisions about therapy and admission. Its major disadvantage has been a tendency to treat patients automatically rather than closely considering the potential acute complications of sickle cell disease. No standard pain management exists for sickle cell disease. A variety of analgesics (nonsteroidal anti-inflammatory drugs, mixed opioid agonist-antagonists, and opiates), dosages, and timing intervals may be chosen. Because many sickle cell disease patients can have varying degrees of hepatic or renal dysfunction, acetaminophen and nonsteroidal anti-inflammatory drugs should be used with caution.28 Because many patients with acute pain episodes are undertreated, the most important aspect of pain man-agement in these patients is a consistent, thorough, and attentive approach that offers true pain relief.39
Blood transfusion has a well-accepted role in sickle cell anemia. Selected use can decrease the chronic transfusion problems of antigen sensitization, iron overload, and hepatitis. Aplastic or splenic sequestration crises may necessitate transfusion. Serial hemoglobin values and reticulocyte counts should be obtained during hospitalization. Whereas the overall goal of simple transfu-sion therapy for symptomatic anemia is a hemoglobin level no higher than 10 g/dL, transfusion should not be used to treat asymptomatic patients, regardless of hemoglobin value.40
Priapism is a painful complication of sickle cell disease and may lead to impotence. First-line therapy for priapism lasting longer than 2 hours is aspiration of blood from the corpus cavernosum and irrigation with an alpha-adrenergic agent (e.g., phenyleph-rine). Surgical management is reserved for patients who fail to respond to aspiration and irrigation.41 Aspiration and irrigation of the corpus cavernosum can be difficult and time-consuming. This therapy is best reserved for urologic consultation. The use of exchange transfusions in the treatment of priapism is controver-sial but appears to have no current role.41

1600 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
schizocytes or fragmented cells, which immediately raise the sus-picion of traumatic injury (see Fig. 121-8). Microangiopathic hemolytic anemia, cardiac trauma, and exercise-induced hemo-globinemia are the most commonly encountered forms of trau-matic hemolysis.
Microangiopathic hemolytic anemia is a form of microcircula-tory fragmentation by threads of fibrin deposited in the arterioles. An underlying disease is inevitably present. It may be found in renal lesions such as malignant hypertension and preeclampsia, vasculitis, thrombotic thrombocytopenic purpura, disseminated intravascular coagulation, and vascular anomalies. The signs and symptoms are those of intravascular hemolysis. Treatment is directed at the causative disease.
Cardiac trauma to RBCs results from increased turbulence. It may be found in patients with prosthetic valves, traumatic arte-riovenous fistula, aortic stenosis, and other left-sided heart lesions. Surgical correction may be necessary. Supportive therapy with an iron supplement is usually required.
March hemoglobinemia is a form of trauma caused by breaking of intravascular RBCs by repetitive pounding. Soldiers, marathon runners, and anyone with repetitive striking against a hard surface may incur this problem. Reassurance and a change in the patient’s pattern of activity are the recommended therapy.45
Environmental Causes. Hemolysis may be seen in cases of severe burns, freshwater drowning, and hyperthermia. Toxic causes of hemolysis have been documented to be of animal origin, such as brown recluse spider and some snake bites; vegetable origin, such as castor beans and certain mushrooms; and mineral origin, such as copper. Certain infections are associated with hemolytic states, including malaria, Bartonella infection, and Clostridium sepsis.
Abnormal Sequestration. Hypersplenism may be caused by any disease that enlarges the spleen or stimulates the reticulo-endothelial system. An unfortunate cycle can be set up in which the enlarged spleen traps more blood components and grows larger. It is usually seen as splenomegaly with pancytopenia and marrow hyperactivity. Chromium-labeled RBCs may demonstrate increased trapping in the spleen. Therapy for symptomatic or severe disease is splenectomy. Adults usually tolerate splenectomy well, but children should be approached conservatively because the risk of postsplenectomy life-threatening sepsis is increased significantly.
POLYCYTHEMIA
Definition
Polycythemia is a term commonly used for erythrocytosis (i.e., increased number of RBCs). This disorder is seen occasionally in emergency medicine but rarely in a life-threatening manner that requires emergency intervention.
BOX 121-13
Hapten type with antibodies to the drugComplement-fixing antibody: quinidine, quinine, phenacetin,
ethacrynic acid, p-aminosalicylate, sulfa drugs, oral hypoglycemic agents
Non–complement-fixing antibody: penicillin dosages >20 million units/day
Autoimmune type with antibodies to the RBC membrane: D-methyldopa, L-dopa, mefenamic acid, chlordiazepoxide
Cephalosporins at dosages >4 g/day may cause hemolysis by direct membrane injury
Drugs Associated with Immune Hemolytic AnemiaBOX 121-12
NeoplasmsMalignant: chronic lymphocytic leukemia, lymphoma, myeloma,
thymoma, chronic myeloid leukemiaBenign: ovarian teratoma, dermoid cyst
Collagen Vascular DiseaseSystemic lupus erythematosusPeriarteritis nodosaRheumatoid arthritis
InfectionsMycoplasmaSyphilisMalariaBartonellaVirus: mononucleosis, hepatitis, influenza, Coxsackievirus,
cytomegalovirus
MiscellaneousThyroid disorders, ulcerative colitisDrug immune reactions
Diseases Associated with Autoimmune Hemolytic Anemia
Warm-reacting antibodies are characterized by a higher inci-dence in younger patients (30-60 years), predominance in women, variable complement fixation, and positive direct antiglobulin test result for IgG. Cold-reacting antibodies, or cold agglutinins, are seen predominantly in men and older patients (50-80 years) and with IgM complement fixation. They may also be found in patients with infectious mononucleosis, Mycoplasma infection, and lymphoma. Hemolysis may be intravascular and extra-vascular, and the direct antiglobulin test result is positive for complement.
Clinically, a patient with immune hemolytic anemia has the signs and symptoms of anemia and, often, splenomegaly. Sphero-cytosis and reticulocytosis are noted in the blood smear. The direct antiglobulin test result is positive in 90% of cases. The strength of the direct antiglobulin test result does not correlate with the sever-ity of the hemolysis because the Coombs’ reaction is an antibody function different from hemolysis or stimulation of reticuloendo-thelial sequestration. In patients with newly diagnosed, reticulo-cytopenic or severe hemolytic anemia, the emergency physician may need to institute transfusion therapy. Compatible blood may be almost impossible to find because the antibody can react with almost all donors. The most compatible donor cells in terms of the ABO and Rh systems should be transfused with the knowledge that they will be no more compatible than the patient’s own blood cells. If emergency blood transfusion is required, type-specific or type O blood (Rh-positive for men; Rh-negative for women of childbearing age) is indicated as well as prednisone or its equiva-lent in a dose of 1 mg/kg. Prednisone is believed to produce an improvement in 60% of patients with warm antibody reactions. Splenectomy and immunosuppressive therapy are also effective in treating these reactions. Cold agglutinin hemolytic anemia may be self-limited, as after infectious mononucleosis. Other forms respond well to cold avoidance, variably to immunosuppressive agents, but poorly to steroids and splenectomy. Death commonly results from uncontrolled hemolysis, the underlying primary dis-order, and pulmonary embolism.43
Drug-induced hemolytic anemia may be difficult to diagnose. The emergency physician should know the drugs most often asso-ciated with this Coombs’-positive phenomenon and realize that the result of this test is sometimes positive only in the drug’s presence. Common drugs and mechanisms of action are listed in Box 121-13.44
Extrinsic Mechanical Causes. Hemolysis may be caused by trauma to RBCs. The peripheral smear may demonstrate

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1601
confined to moderation, weight loss, and blood pressure control. The risk of vascular occlusive complications is minimal. The hematocrit is usually less than 60% and RBC mass measurements are normal.47
Primary polycythemia vera is a myeloproliferative disorder found predominantly in middle-aged or older patients. It may have all the clinical components of polycythemia. Nonspecific symptoms are reported in up to 30% of patients and include headache, weakness, dizziness, excessive sweating, and pruritus. The most serious problems are thrombotic episodes (cerebrovas-cular accident, myocardial infarction, and deep venous thrombo-sis), bleeding, and bruising. Primary polycythemia vera is a disease that involves all cell lines—hematopoietic stem, erythroid, granu-locytic, and megakaryocytic. Elevated hemoglobin or hematocrit and RBC mass is present in virtually all patients. However, a plate-let count above 400,000/µL occurs in 60% and a WBC count above 12,000/µL in 40%. Bone marrow cellularity was increased in 90% of patients, and storage iron was absent from the marrow in 94%. The diagnostic criteria used by the Polycythemia Vera Study Group are listed in Box 121-15.47
Polycythemia vera may be satisfactorily treated by phlebotomy as necessary. The reduced hematocrit improves some symptoms, but neither the leukocyte nor the platelet count is decreased. Maintenance of the hematocrit at less than 55% is recommended to decrease hypervolemia and hyperviscosity. Complications necessitating additional therapy include hyperuricemia, refractory
Pathophysiology
Erythropoiesis is controlled by the kidney-produced glycoprotein hormone erythropoietin. It is activated in the liver and regulates the committed erythropoietic stem cell. Its major stimulant is tissue hypoxia. Neoplastic dysfunction of bone marrow may also result in an elevated absolute RBC count.
The major complication of polycythemia is related to the increase in blood viscosity associated with increased RBC numbers. As the hematocrit rises past 60%, viscosity increases in an almost exponential manner. This condition increases the possibility of reduced tissue flow, thrombosis, and hemorrhage. This hazard is usually blunted to a degree by an associated increase in blood volume and some viscosity-reducing vascular dilation.46
Clinical Features
The history may range from only mild headaches to a full-blown syndrome of hypervolemia (vertigo, dizziness, blurred vision, and headache), hyperviscosity (venous thrombosis), and platelet dysfunction (epistaxis, spontaneous bruising, and gastrointestinal bleeding).
On physical examination, the skin and mucous membrane manifestations of the elevated RBC count are often readily observed. Plethora, engorgement, and venous congestion are com-monly noted (Fig. 121-11). Other systems to be examined include the fundus for venous congestion, the abdomen for evidence of splenomegaly, and the cardiopulmonary system for signs of con-gestive heart failure. Uterine, central nervous system, renal, and hepatic tumors should be sought in that these are associated with secondary polycythemia. An elevated RBC count, usually greater than the hematocrit, defines the disorder. It results in a low MCV, usually related to low serum iron and iron stores. Specific labora-tory testing is discussed in the section on differential diagnosis.
Differential Diagnosis
Polycythemia is classified as apparent, primary, or secondary (Box 121-14). Apparent polycythemia is a decrease in plasma volume such as found with dehydration. The RBC volume does not exceed the upper limit of normal. Although it is a questionable diagnostic entity, “stress” polycythemia is the tendency for an elevated hema-tocrit and is found in overweight, hypertensive, and overstressed middle-aged men. Increased cigarette smoking with its associated increased carboxyhemoglobin level is considered to be partially responsible. The symptoms are minimal, and treatment is
Figure 121-11. Polycythemia vera. Facial plethora and conjunctival suffusion in a 40-year-old woman (hemoglobin, 19.5 g/dL). (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:248.)
BOX 121-14
Appropriately increased erythropoietin caused by tissue hypoxiaCongenital heart disease with a right-to-left shuntPulmonary disease (e.g., bronchial-type chronic obstructive
pulmonary disease)CarboxyhemoglobinemiaHigh-altitude acclimatizationDecreased tissue oxygen release from hemoglobinopathies
with high oxygen affinityInappropriate autonomous erythropoietin production
Renal origin: carcinoma, hydronephrosis, cystOther lesions: uterine fibroids, hepatoma of adrenal origin,
cerebellar hemangiomaCongenital overproductionPure or essential erythrocytosisAIDS and zidovudine treatment
Causes of Apparent and Secondary Polycythemia

1602 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
WHITE BLOOD CELL DISORDERS
The WBC count and accompanying differential are the most common laboratory tests ordered in the emergency department. It is essential that the basic physiology, pathophysiology, and clini-cal evaluation of WBCs be understood.
Physiology and Pathophysiology
The series has three morphologically indistinguishable cell types: B cells (humoral immunity), T cells (cellular immunity), and null cells. Because lymphocytes can freely leave and return to the cir-culation, the storage pools are less well defined. Only 5% of the total lymphocytes in the body are in the circulation. No marginal pool exists. Leukocytes primarily function extravascularly, and their function is closely integrated with the other types of white cells. WBCs reach their site of action through the circulation. The rate that new cells enter the circulation is usually in equilibrium with the rate of loss in tissues.
Abnormal cell counts are due to changes in production, the marginal pool, or the rate of tissue destruction. Just as in anemia or platelet count abnormalities, the differential diagnosis of increased (leukocytosis) or decreased (leukopenia) WBC counts can be organized by processes altering production, destruction, loss, and sequestration.
The granulocytic and lymphocytic series are the two cell lines of WBCs. The granulocytic series is primarily involved in phago-cytic activity. Its origin is the pluripotential stem cells located in the bone marrow. A subset of these cells differentiates and matures into the phagocytic cell lines, which include neutrophils, monocytes, basophils, and eosinophils. Granulocytes are main-tained in a series of developmental and storage pools. The most important is the postmitotic storage pool for neutrophils, which represents 15 to 20 times the circulating population. This pool contains metamyelocytes, band neutrophils, and mature neutro-phils (polymorphonuclear neutrophils). The pool can be drawn on as a ready reserve during rapid consumption of granulocytes. Circulating neutrophils are subdivided equally into the circulat-ing neutrophil pool and the marginal pool. The marginal pool consists of mature cells adherent to the blood vessel walls. These cells can rapidly enter the circulating pool and cause a substantial increase, even doubling, of the WBC count. This involvement does not alter the maturity pattern of the differential count.51 The lymphocytic series matures in lymphoid tissues located in the bone marrow, thymus, spleen, lymph nodes, and elsewhere. They are involved in the immune response against foreign substances.
Normal Values and Influences
One unique problem in WBC disorders is the wide variability in normal values and the multiple factors influencing them. WBC counts are generally performed automatically by electrical imped-ance or optical diffraction techniques. Differential counts are commonly performed by direct examination of 100 to 500 cells with the oil immersion lens of the microscope. Automated tech-niques for all differential counts are becoming more popular, however. Normal values for the WBC count are listed in Table 121-8. The “normal” count is age dependent until childhood and may be shifted upward by exercise, gender (women), smoking, and pregnancy. Decreases in the total WBC count range by 1000 to 1200 cells/mm3 have been noted in the African American population.51 Laboratory errors may be due to improper sample preparation, nucleated RBCs, or platelet clumping. The blood smear differential count may also be influenced by small sample size, improper cell identification, and age group (children). Dif-ferential ranges are listed in Table 121-9. One common but easily
BOX 121-15
Category AIncreased RBC mass
In men: hemoglobin >18.5 g/dLIn women: hemoglobin >16.5 g/dL
Normal arterial oxygen saturation (>92%)Splenomegaly
Category BThrombocytosis: platelets >400,000/mm3
Leukocytosis: WBC count >12,000/mm3 (with no fever or infection)
Leukocyte alkaline phosphatase score >100Vitamin B12 >900 pg/mL, unbound vitamin B12–binding capacity <2200 pg/mL
Diagnostic Criteria for Polycythemia Vera*
*For polycythemia vera to be diagnosed, either all three criteria in category A or the first two criteria in category A along with any two criteria in category B needs to be present.
increased RBC mass, severe pruritus, excessive splenomegaly, and thrombocytosis. Additional therapy may consist of hydroxyurea, busulfan, chlorambucil, interferon alfa, anagrelide, or radioactive phosphorus (32P). Studies suggest no improvement in long-term survival with the addition of these treatments.48 The natural history of the disease is that it burns out during a period of 15 to 20 years. However, myelofibrosis with myeloid metaplasia may develop. In 10% of cases, acute leukemia develops with a rapid and poorly responsive downhill course. The 15-year survival for polycythemia vera is 65%.49 The most common causes of death are thrombosis (29%), hematologic malignant neoplasms (23%), nonhematologic malignant neoplasms (16%), hemorrhage, and myelofibrosis with myeloid metaplasia.
Secondary polycythemia is classified first according to the appropriate erythropoietin response to abnormal tissue oxygen levels. This group of disorders may be ruled out by normal mea-sured arterial oxygen saturation. Second, inappropriate autono-mous erythropoietin production is considered. This condition can be assessed with an erythropoietin assay. Because of a strong association with renal pathologic conditions, computed tomogra-phy should be used to evaluate a patient with a suspected inap-propriate erythropoietin response. Most patients with secondary polycythemia have no central nervous system symptoms or sple-nomegaly. Because erythropoietin stimulates only the red cell pathway, these patients have normal WBC and platelet counts.
Management
The emergency treatment of any form of symptomatic polycythe-mia is phlebotomy. Usually, not more than 500 mL of blood is removed as the volume is replaced with a comparable amount of saline. No hemodynamic compromise should occur if this proce-dure is performed slowly. In true emergencies, up to 1 to 1.5 L of blood may be removed during a 24-hour period. The initial goal is to lower the hematocrit toward 60%. The final goal is a level less than 55%. Low-dose aspirin, 80 to 100 mg/day, has been shown to prevent thrombotic complications in patients with polycythe-mia vera and can be used in the acute and chronic treatment of this disorder.50
Disposition
A number of patients with known polycythemia may be managed by outpatient phlebotomies. Any newly diagnosed or symptomatic patient should be considered for admission to the hospital for full evaluation.

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1603
Modified from Miale JB: Laboratory Medicine: Hematology, 6th ed. St Louis, Mosby, 1982.
BOX 121-16
Neutrophils (absolute count >7500 cells/mm3)Inflammation: rheumatoid arthritis, goutInfection: bacterial most commonTissue necrosis: cancer, burns, infarctionsMetabolic disorders: diabetic ketoacidosis, thyrotoxicosis, uremiaRapid RBC turnover: hemorrhage, hemolysisMyeloproliferative disorders: chronic myeloid leukemia,
polycythemia veraMalignant disease (e.g., gastrointestinal cancers)Stress: exercise, pain, surgery, hypoxia, seizures, traumaDrugs: epinephrine, corticosteroids, lithium, cocainePregnancyHeredity or idiopathic diseaseLaboratory error: automated counters, platelet clumping,
precipitated cryoglobulin
Lymphocytosis (absolute count >9000/mm3, ages 1-6 years; >7000/mm3, ages 7-16 years; >4000/mm3, adults)Viral infection (primary cause): mononucleosis, rubeola, rubella,
varicella, toxoplasmosisBacterial infection: pertussis, tuberculosis, hepatitis,
cytomegalovirusLymphoproliferative: acute or chronic lymphocytic leukemiaImmunologic response: immunization, autoimmune diseases,
graft rejectionEndocrine: hypothyroidismRelative lymphocytosis associated with granulocytopenia
Causes of Leukocytosis
AGE AVERAGE95% RANGE (AVERAGE VALUE ±2 SD)
1 week 12,200 5,000-21,000
6 months 11,900 6,000-17,500
12 months 11,400 6,000-17,500
4 years 9,100 5,500-15,500
8 years 8,300 4,500-13,500
Adults 7,400 4,500-11,000
Modified from Miale JB: Laboratory Medicine: Hematology, 6th ed. St Louis, Mosby, 1982.
Table 121-8Normal Ranges for the Blood Leukocyte Count (cells/mm3)
AGE SEGMENTED NEUTROPHILS BAND NEUTROPHILS LYMPHOCYTES MONOCYTES EOSINOPHILS BASOPHILS
1 week 34 ± 15 (4100) 11.8 ± 4 (1420) 41 ± 5 (5000) 9.1 (1100) 4.1 (500) 0-4 (50)
6 months 23 ± 10 (2710) 8.8 ± 3 (1000) 61 ± 15 (7300) 4.8 (480) 2.5 (300) 0-4 (50)
12 months 23 ± 10 (2680) 8.1 ± 3 (990) 61 ± 15 (7000) 4.8 (550) 2.6 (300) 0-4 (50)
4 years 34 ± 11 (3040) 8.0 ± 3 (730) 50 ± 15 (4500) 5.0 (450) 2.8 (250) 0-6 (50)
8 years 45 ± 11 (3700) 8.0 ± 3 (660) 39 ± 15 (3300) 4.2 (350) 2.4 (200) 0-6 (50)
Adult 51 ± 15 (3800) 8.0 ± 3 (620) 34 ± 10 (2500) 4.0 (300) 2.7 (200) 0-5 (40)
Modified from Miale JB: Laboratory Medicine: Hematology, 6th ed. St Louis, Mosby, 1982.*Numbers in parentheses indicate the average number of cells per cubic millimeter.
Table 121-9 Normal Percentage Ranges for the Leukocyte Differential Count in Blood*
corrected error in laboratory reporting is to give the results in terms of the percentage of cell types. Absolute counts for each cell type are more accurate and useful in assessing the risk for infection.
Abnormal Values
Because of the wide range of normal values, all abnormal WBC counts should be interpreted in the context of the patient’s condi-tion. A careful history and physical examination, absolute cell counts, and review of the peripheral smear differential count are the starting points to determine the origins of quantitative WBC disorders.
Leukocytosis
Most cases of leukocytosis are caused by increases in the neutro-phil or lymphocyte cell lines. Neutrophil leukocytosis (neutro-philia) is an absolute neutrophil count greater than 7500 cells/mm3 and is commonly associated with infection or inflammation (Box 121-16). Because increased neutrophil destruction is associ-ated with both of these pathologic processes, bone marrow stores are drawn on, and the usual ratio of 1 band to 10 neutrophils increases. This increase is manifested as a “left shift” in the dif-ferential count and represents movement of immature neutrophils from the postmitotic pool into the circulation.
WBC counts can increase without a left shift or an increase in band forms by demarginating neutrophils from the vessel walls. It is often seen as a response to stress, exercise, or epinephrine. Severe stress can raise the WBC count to 18,000 to 20,000 cells/mm3.51
Chronic Myeloid Leukemia
One of the myeloproliferative causes of neutrophilic leukocytosis is chronic myeloid leukemia (CML). Although it is the least
common of the major leukemias (60% acute, 31% chronic lym-phocytic leukemia, and 15% CML), it should be considered in neutrophilia. Patients with CML are usually older than 40 years and have WBC counts greater than 50,000 cells/mm3. The differ-ential count shows elevated polymorphonuclear neutrophils and metamyelocytes. Less often, the basophil and eosinophil counts are also increased. CML is a stem cell disorder in which the WBC count is elevated and the differential is normal. Mature and inter-mediate granulocytes are overproduced. Platelets may also be increased, but RBC production is down, thereby resulting in anemia. The patient often complains of fatigue, anorexia, sweat-ing, and weight loss. Physical findings include pallor, sternal pain and tenderness, and splenomegaly (90% of patients; Fig. 121-12). In the laboratory, decreased leukocyte alkaline phosphatase and increased vitamin B12 levels are found, which helps differentiate CML from other causes of neutrophilia. The Philadelphia chro-mosome (Ph1) is constantly associated with the disease. The chronic phase of CML is treated with an alkylating agent (e.g., busulfan) or an antimetabolite (e.g., hydroxyurea). Selected patients may benefit from bone marrow transplantation.52

1604 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
Lymphocytic Leukocytosis
Lymphocytic leukocytosis (lymphocytosis) is an age-dependent definition: 9000 cells/mm3, ages 1 to 6 years; 7000 cells/mm3, ages 7 to 16 years; and 4000 cells/mm3, adults. It is seen in a variety of disorders, primarily infections and lymphoproliferative disease.
In the past, acute and chronic were descriptive terms applied to lymphocytic neoplasms with respect to survival time of the patient before present therapy was available. The terms acute and chronic are currently used to describe the cell maturity, rapidity of onset, and aggressiveness of therapy.
Chronic Lymphocytic Leukemia. Chronic lymphocytic leukemia is primarily a B-cell disorder and is the most common type of leukemia in the population 50 years or older. Patients initially complain of fatigue, weight loss, increased susceptibility to infec-tion, rashes, and easy bruising. The lymph nodes are nontender and smooth, and they may appear in only one or two areas. Splenic and hepatic enlargement occurs in more than 50% of patients. Laboratory support of the diagnosis is an absolute lymphocyte count greater than 5000 cells/mm3 in adults. Anemia, thrombocy-topenia, and neutropenia are often found. Autoimmune hemolytic anemia, a positive direct antiglobulin test result, and other altered immune system problems are seen. Early therapy may be directed toward complications of anemia, thrombocytopenia, impaired or accentuated immune response, or enlarged lymph nodes or spleen. Leukostasis is seldom seen in chronic lymphocytic leukemia, but therapy is considered when the total count rises to higher than 200,000/mm3.53
Acute Lymphocytic Leukemia. Acute lymphocytic leukemia is most commonly diagnosed in children younger than 10 years. It is the most frequent malignant neoplasm in children younger than 15 years. The potential for leukostasis increases in acute lympho-cytic leukemia when the blast count rises above 50,000 cells/mm3. Oncologic therapy is based on clinical staging and includes che-motherapy or radiation therapy. Aggressive therapy has improved childhood survival; current 5-year overall survival rates are esti-mated at 78 to 85%. This response to treatment has not been found to the same degree in adults.54,55
Leukopenia
In adults, leukopenia is defined as an absolute blood cell count less than 4000 cells/mm3. Leukopenia is commonly associated with a reduction in one cell type, the neutrophil, and this decrease has the greatest clinical significance. The absolute neutrophil count is calculated by multiplying the WBC count by the combined percentage of band and segmented neutrophils. The absolute neu-trophil count can be classified as mild (1000-1500 cells/mm3), moderate (500-1000 cells/mm3), or severe (<500 cells/mm3) according to the risk for infection. The last is a potentially life-threatening state because the patient is markedly susceptible to overwhelming infection. The physical signs of infection may be minimal in severe neutropenia because there are too few cells to generate a substantial inflammatory or purulent response. Neu-tropenia may be caused by decreased production, increased destruction, or movement of circulating neutrophils into marginal or tissue pools. Until recently, it was most often caused by a decrease in bone marrow production (Table 121-10). Autoim-mune neutropenia is also becoming more commonly diagnosed because it is thought to have a role in acquired immunodeficiency syndrome.56
A thorough medication history should be taken in all patients found to have neutropenia. A previous history of neutropenia, a review of recent infection, and a family history are obtained. The review of systems focuses on bleeding problems, fatigue, sweats, weight loss, and autoimmune symptoms. The physical examina-tion is directed toward sites of infection, lymphadenopathy,
The need for urgent therapy in CML is usually related to hyperuricemia and renal injury or severe anemia and subsequent angina or heart failure. Rarely, hyperleukocytosis occurs, but the more mature, “less sticky” cells in CML do not usually cause problems unless the count exceeds 500,000 cells/mm3. A higher cell count may cause leukostasis and result in deafness, visual impairment, pulmonary ventilation-perfusion abnormalities, and priapism. Treatment involves hydration, leukapheresis, transfu-sion as necessary, allopurinol to prevent severe hyperuricemia, and specific chemotherapy (hydroxyurea). Late problems in the natural history of CML involve progressive loss of cell differentia-tion and response to therapy. The term blastic crisis represents the sudden appearance of an acute form of leukemia, which is a rare substage of the evolving deterioration.52 The condition may occur in lymphoid or myeloid forms. Blast counts greater than 50,000 cells/mm3 may predispose the patient to the complications of leukostasis.
Leukemoid Reaction
A leukemoid reaction is a nonleukemic reactive granulocytic leu-kocytosis that resembles CML but has no associated Ph1 chromo-some, no absolute increase in basophils and eosinophils, and an increase in leukocyte alkaline phosphatase. It is difficult to distin-guish from CML in the emergency department, and both need to be considered a potential diagnosis in granulocytic leukocytosis. WBC counts are usually greater than 50,000 cells/mm3. A leuke-moid reaction may be seen in tuberculosis, Hodgkin’s disease, sepsis, and metastatic tumor, particularly bronchogenic, gastric, and renal carcinoma.52
Figure 121-12. Chronic myeloid leukemia. (From Hoffbrand AV, Pettite JE: Color Atlas of Clinical Hematology, 3rd ed. London, Mosby, 2000:169.)

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1605
studies suggest some usefulness in certain clinical situations; however, the absence of leukocytosis does not exclude the presence of significant disease. For example, studies evaluating the WBC count for the diagnosis of abdominal pain have found it to be a useful confirming test or helpful in selecting patients for observa-tion.60 In evaluation of the bacterial infectious potential in febrile children, the WBC and differential counts have demonstrated limited usefulness.61 Other biomarkers, such as procalcitonin and C-reactive protein, may have more predictive value.62,63 The test should be viewed as having limited screening value in the acute care setting because multiple agents and conditions can increase the WBC count.
Although the WBC count may be nonspecific and nonsensitive, the differential count may provide helpful information. The abso-lute neutrophil count may be more helpful than the total WBC count in identifying bacterial infection.62,63
hepatosplenomegaly, and underlying disease. In patients with severe neutropenia and fever, a full radiologic and direct examina-tion of commonly involved areas, such as the chest and urine, should be performed, and sputum, urine, and blood culture speci-mens should be obtained. Basic isolation techniques, early admis-sion, and consultation with another specialist are recommended. Specific therapies may be started after cultures and consultation are completed. A number of empirical antibiotic regimens are recommended for febrile patients with neutropenia.57,58 Human granulocyte colony–stimulating factor is often used in the setting of neutropenia, but it is best done in consultation with a hema-tologist.59 Patients with a clear reversible source or without signifi-cant clinical findings and mild to moderate levels of neutropenia may have outpatient follow-up arranged, preferably after discus-sion with their physician.
RATIONALE FOR SELECTION OF WHITE BLOOD CELL AND DIFFERENTIAL COUNTS
The WBC count has not proved to be a highly sensitive or specific test for the diagnosis of a variety of disease entities. Selected
■ Anemia is caused by three basic mechanisms: bleeding, destruction of red blood cells, and decrease in production of red blood cells.
■ The use of red blood cell indices and a peripheral blood smear can help determine the mechanism of anemia.
■ One of the most important but often overlooked studies in the evaluation of suspected hemolytic anemia is the peripheral blood smear.
■ Anemia in the elderly often occurs as an exacerbation of preexisting comorbid diseases.
■ Anemia of uncertain etiology should be thoroughly evaluated. If the patient has no adverse hemodynamic consequences, the evaluation can proceed on an outpatient basis.
■ Patients with sickle cell disease should be considered to have an acute pain crisis and treated appropriately until it is proved otherwise.
■ Acute chest syndrome is one of the most common causes of death in sickle cell disease.
■ Acute transfusion therapy is most useful in sickle cell disease associated with acute stroke (in children), acute chest syndrome, and splenic sequestration.
■ The white blood cell determination in the emergency department has poor sensitivity and specificity for any specific disease.
KEY CONCEPTS
MECHANISM EXAMPLE
Proliferation in bone marrow
Aplastic anemia, leukemia, cancer chemotherapy (cyclophosphamide, azathioprine, methotrexate, chlorambucil)
Drugs: phenothiazines, phenylbutazone, indomethacin, propylthiouracil, phenytoin, cimetidine, semisynthetic penicillins, sulfonamides
Infection: viral, tuberculosis, sepsis
Maturation in bone marrow
Folate or vitamin B12 deficiency, chronic idiopathic neutropenia
Starvation
Distribution Hypersplenism: sarcoidosis, portal hypertension, malaria
Increased use Infection: viral most common (mononucleosis, rubella, rubeola), Rickettsia organisms, overwhelming bacterial infection
Autoimmune disease: systemic lupus erythematosus, AIDS, Felty’s syndrome
Laboratory error Leukocyte clumping, long delay in performing test
Table 121-10Linkage of Leukopenia to Phases of Neutrophil Maturation
The references for this chapter can be found online by accessing the accompanying Expert Consult website.

Chapter 121 / Anemia, Polycythemia, and White Blood Cell Disorders 1605.e1
References
1. Weber P, et al: Anemia in elderly an important diagnostic and therapeutic problem in geriatric medicine. Adv Gerontol 2009; 22:662-666.
2. Tefferi A: Anemia in adults: A contemporary approach to diagnosis. Mayo Clin Proc 2003; 78:1274-1280.
3. Olivieri NF: The beta-thalassemias. N Engl J Med 1999; 341:99-109.4. Borgna-Pignatti C: Modern treatment of thalassemia intermedia. Br J
Haematol 2007; 138:291-299.5. Rund D, Rachmilewitz E: Beta-thalassemia. N Engl J Med 2005;
353:1135-1139.6. Galanello R, Campus S, Origa R: Deferasirox: Pharmacokinetics
and clinical experience. Expert Opin Drug Metab Toxicol 2012; 8:123-134.
7. Lucarelli G, Gaziev G: Advances in the allogeneic transplantation for thalassemia. Blood Rev 2008; 22:53-63.
8. Weiss G, Goodnough LT: Anemia of chronic disease. N Engl J Med 2005; 352:1011.
9. Malouf R, Grimley Evans J: Folic acid with or without vitamin B12 for the prevention and treatment of healthy elderly and demented people. Cochrane Database Syst Rev 2008; 4:CD004515.
10. Locatelli F, et al: Cyclosporin A and short-term methotrexate versus cyclosporin A as graft versus host disease prophylaxis in patients with severe aplastic anemia given allogeneic bone marrow transplantation from an HLA-identical sibling: Results of a GITMO/EBMT randomized trial. Blood 2000; 96:1690-1696.
11. Young NS: Acquired aplastic anemia. Ann Intern Med 2002; 136:534-538.
12. Marsh JC, et al: Guidelines for the diagnosis and management of aplastic anaemia. Br J Haematol 2009; 147:43-50.
13. Jones M, Ibels L, Schenkel B, Zagari M: Impact of epoetin alfa on clinical end points in patients with chronic renal failure: A meta-analysis. Kidney Int 2004; 65:757-765.
14. Packman CH: Hemolytic anemia due to warm autoantibodies. Blood Rev 2008; 22:17-23.
15. Glassberg J: Evidence based management of sickle cell disease in the emergency department. Emerg Med Pract 2011; 13:1-20.
16. Quinn CT, et al: Prediction of adverse outcomes in children with sickle cell anemia: A study of the Dallas Newborn Cohort. Blood 2008; 111:544-548.
17. Yanni E, Grusse S, Yang Q, Olney R: Trends in pediatric sickle cell disease–related mortality in the United States, 1983-2002. J Pediatr 2009; 154:541-545.
18. Tsaras G, Owusu-Ansah A, Boateng FO, Amoateng-Adjepong Y: Complications associated with sickle cell trait: A brief narrative review. Am J Med 2009; 122:507-511.
19. Austin H, et al: Sickle cell trait and the risk of venous thromboembolism among blacks. Blood 2007; 110:908-912.
20. Tita AT, Biggio JR, Chapman V, Neely C, Rouse DJ: Perinatal and maternal outcomes in women with sickle cell or hemoglobin C trait. Obstet Gynecol 2007; 110:1113-1119.
21. Aisiku IP, et al: Comparisons of high versus low emergency department utilizers in sickle cell disease. Ann Emerg Med 2009; 53:587-592.
22. Dampier C, et al: Vaso-occlusion in children with sickle cell disease: Clinical characteristics and biologic correlates. J Pediatr Hematol Oncol 2004; 26:785-790.
23. Ohene-Frempong K, et al: Cerebrovascular accidents in sickle cell disease: Rates and risk factors. Blood 1998; 91:288-294.
24. Verduzco LA, Nathan DG: Sickle cell disease and stroke. Blood 2009; 114:5117-5125.
25. Krejza J, et al: Sickle cell disease and transcranial Doppler imaging. Stroke 2011; 42:81-86.
26. Adams RJ, et al: Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. N Engl J Med 1998; 339:5-11.
27. Hulbert ML, et al: Exchange blood transfusion compared with simple transfusion for first overt stroke is associated with a lower risk of subsequent stroke: A retrospective cohort study of 137 children with sickle cell anemia. J Pediatr 2006; 149:710-712.
28. The Management of Sickle Cell Disease. Bethesda, Md: National Institutes of Health, National Heart, Lung, and Blood Institute, Division of Blood Diseases and Resources; revised 2004. NIH publication 04-2117.
29. Gladwin MT, Vichinsky E: Pulmonary complications of sickle cell disease. N Engl J Med 2008; 359:2254-2259.
30. Vichinsky EP, et al: Causes and outcomes of the acute chest syndrome in sickle cell disease. N Engl J Med 2000; 342:1855-1859.
31. Turner JM, Kaplan JB, Cohen HW, Billett HH: Exchange versus simple transfusion for acute chest syndrome in sickle cell anemia adults. Transfusion 2009; 49:863-868.
32. Alhashimi D, et al: Blood transfusions for treating acute chest syndrome in people with sickle cell disease. Cochrane Database Syst Rev 2010; 20:CD007843.
33. Battersby AJ, Knox-Macaulay HH, Carrol ED: Susceptibility to invasive bacterial infections in children with sickle cell disease. Pediatr Blood Cancer 2010; 55:401-406.
34. Syrogiannopoulos GA, McCracken GH, Nelson JD: Osteoarticular infections in children with sickle cell disease. Pediatrics 1986; 78:1090-1094.
35. Brawley OW, et al: National Institute of Health consensus development conference statement: Hydroxyurea treatment for sickle cell disease. Ann Intern Med 2008; 148:932-937.
36. Steinberg MH, et al: Effect of hydroxyurea on mortality and morbidity in adult sickle cell anemia: Risks and benefits up to 9 years of treatment. JAMA 2003; 289:1645-1651.
37. Vichinsky E: New therapies of sickle cell disease. Lancet 2002; 360:629-635.
38. Amrolia PJ, Almeida A, Halsey C, Roberts IA, Davies SC: Therapeutic challenges in childhood sickle cell disease. Part 1: Current and future treatment options. Br J Haematol 2003; 120:725-736.
39. Tanabe P, et al: Emergency department management of acute pain episodes in sickle cell disease. Acad Emerg Med 2007; 14:419-425.
40. Josephson CD, Su L, Hillyer K, Hillyer C: Transfusion in the patient with sickle cell disease: A critical review of the literature and transfusion guidelines. Transfus Med Rev 2007; 21:118-133.
41. Montague DK, et al; Members of the Erectile Dysfunction Guideline Update Panel; American Urological Association: Priapism. Guidelines on the management of priapism, 2010. Available at www.auanet.org.
42. Gibbs WJ, Hagemenn TM: Purified poloxamer 188 for sickle cell vaso-occlusive crisis. Ann Pharmacother 2004; 38:320-325.
43. Gehrs BC, Friedberg RC: Autoimmune hemolytic anemia. Am J Hematol 2002; 69:258-263.
44. Arndt P, Garraty G: The changing spectrum of drug-induced immune hemolytic anemia. Semin Hematol 2005; 42:138-142.
45. Kehat I, Shupak A, Goldenberg I, Shoshani O: Long-term hematological effects in Special Forces trainees. Mil Med 2003; 168:116-119.
46. Passamonti F, et al: Polycythemia vera in young patients: A study on the long-term risk of thrombosis, myelofibrosis and leukemia. Haematologica 2003; 88:13-19.
47. Streiff MB, Smith B, Spivak JL: The diagnosis and management of polycythemia vera in the era since the Polycythemia Vera Study Group: A survey of American Society of Hematology members’ practice patterns. Blood 2002; 99:1144-1148.
48. Spivak JL: Polycythemia vera: Myths, mechanisms, and management. Blood 2002; 100:4272-4290.
49. Passamonti F, et al: Life expectancy and prognostic factors for survival in patients with polycythemia vera and essential thrombocythemia. Am J Med 2004; 117:755-761.
50. Squizzato A, Romualdi E, Middledorp S: Antiplatelet drugs for polycythaemia vera and essential thrombocythaemia. Cochrane Database Syst Rev 2008; 2:CD006503.
51. Hillman RS, et al: Normal myelopoiesis. In Hillman RS, et al, eds. Hematology in Clinical Practice, 5th ed. New York: McGraw-Hill; 2011.
52. Goldman JM, Melo JV: Chronic myeloid leukemia—advances in biology and new approaches to treatment. N Engl J Med 2003; 349:1451-1456.
53. Kipps TJ: Classification and clinical manifestations of lymphocyte and plasma cell disorders. In: Kaushansky K, et al, eds. Williams Hematology, 8th ed. New York: McGraw-Hill; 2010.
54. Ribera JM, Oriol A: Acute lymphoblastic leukemia in adolescents and young adults. Hematol Oncol Clin North Am 2009; 5:1033-1045.
55. Pui CH: Treatment of acute lymphoblastic leukemia. N Engl J Med 2006; 354:166-171.
56. Jacobson MA, Liu RC, Davies D, Cohen PT: Human immunodeficiency virus–related neutropenia and the risk of hospitalization for bacterial infection. Arch Intern Med 1997; 157:1825-1831.
57. Viscoli C, Varnier O, Machetti M: Infections in patients with febrile neutropenia: Epidemiology, microbiology, and risk stratification. Clin Infect Dis 2005; 40(Suppl 4):S240-S245.
58. Sepkowitz KA: Treatment of patients with hematologic neoplasm, fever, and neutropenia. Clin Infect Dis 2005; 40(Suppl 4):S253-S256.

1605.e2 PART III ◆ Medicine and Surgery / Section TEN • Hematology and Oncology
59. Kuderer NM: Impact of primary prophylaxis with granulocyte colony–stimulating factor on febrile neutropenia and mortality in adult cancer patients receiving chemotherapy: A systematic review. J Clin Oncol 2007; 25:3158-3162.
60. Deibener-Kaminsky J, Lesesve JF, Kaminsky P: Leukocyte differential for acute abdominal pain in adults. Lab Hematol 2011; 17:1-5.
61. Pucell K, Fergie J: Lack of usefulness of an abnormal white cell count for predicting a concurrent serious bacterial infection in infants and young
children hospitalized with respiratory syncytial virus lower respiratory tract infection. Pediatr Infect Dis 2007; 26:311-315.
62. Kuppermann N, Fleisher GR, Jaffe DM: Predictors of occult pneumococcal bacteremia in young febrile children. Ann Emerg Med 1998; 31:679-687.
63. Seigel TA, et al: Inadequacy of temperature and white blood cell count in predicting bacteremia in patients with suspected infection. J Emerg Med 2012; 42:254-259.