Embed Size (px)
Citation preview
Chapter 15Disorders of Childhood
Ch 15
Classification Issues• Distinguishing abnormal childhood behavior requires a
knowledge from developmental psychology of what is normal for a child at a particular age or stage
• Disorders can be viewed as categories or on a continuum (dimension)
– Control represents a dimensional variable• Overcontrolled (internalizing)children show emotional inhibition
• Undercontrolled (externalizing) children show excessive behaviors (extreme aggressiveness)
Ch 15.1
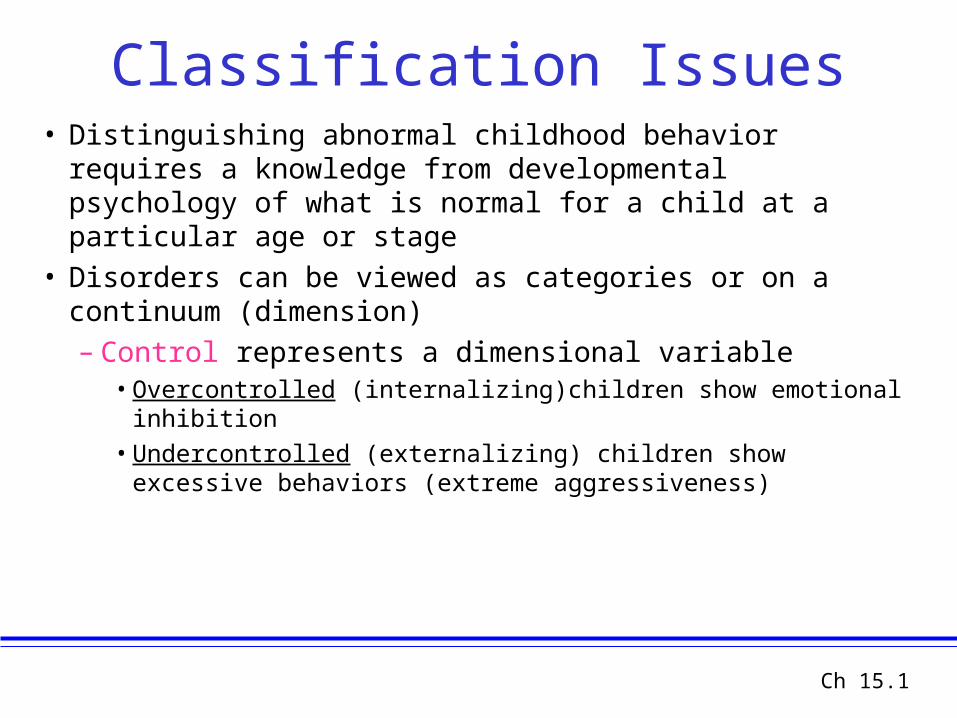
Table 15.1 Diagnoses that May be Applied to Children
Developmental Psychopathology
• Behavior genetics & neurobiological traumas• Infant / child temperaments and “the problem of the
match” with parental temperaments and expectations• Attachment theory (Bowlby, Ainsworth, Sroufe)
– Secure vs. insecure attachment– Insecure attachment category may be related to later
childhood disorders • “anxious-resistant” category - internalizing disorders• “avoidant”category - externalizing disorders
• How do temperament & attachment interact?– Evidence is inconclusive, but see Bokhorst et al. (2004)

Disorders of Undercontrolled Behavior
• Undercontrolled behavior is excessive or inappropriate for the situation
• DSM-IV recognizes two classes of undercontrolled behavior:– Attention-deficit/hyperactivity disorder (ADHD) involves
• An inability to concentrate on task for an appropriate period of time
• Difficulties in controlling motor movements in class and other situation (fidgeting, talking)
Ch 15.2
ADHD Issues• Hyperactive children have difficulties in establishing peer
relations – Aggressive ADHD children have different social goals (being
disruptive) than do non-ADHD peers
• ADHD can co-occur with learning disabilities (15-30% of ADHD children have co-morbid LDs)
• ADHD shows within category differences– Some children have attention deficit, some have hyperactivity, and
some have both
• ADHD prevalence is 2-7% in US• ADHD with conduct disorder = worse prognosis
Ch 15.3
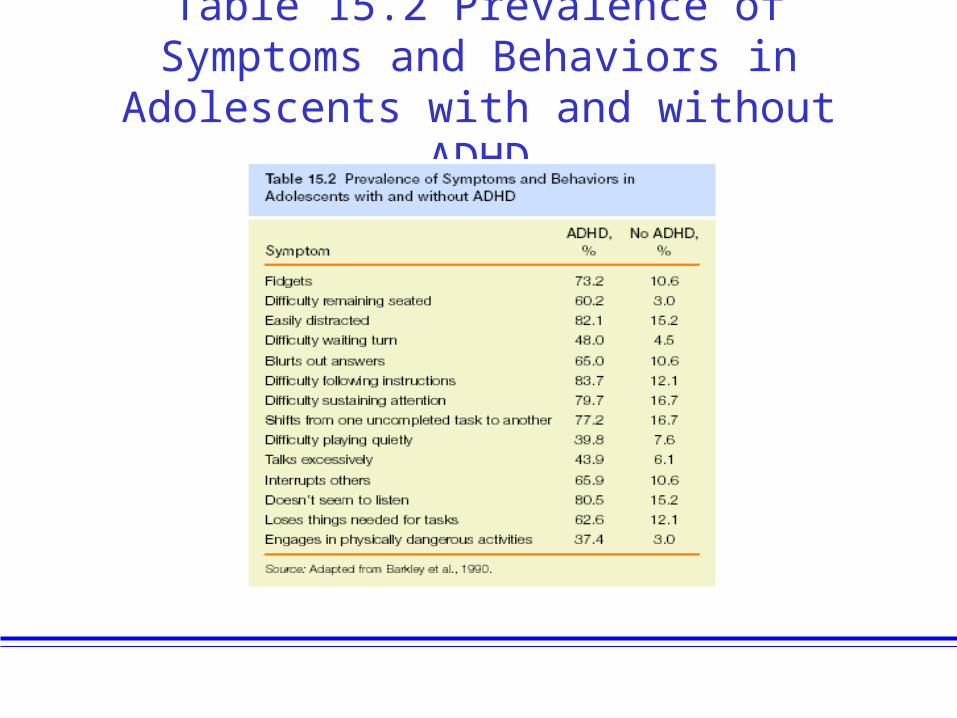
Table 15.2 Prevalence of Symptoms and Behaviors in Adolescents with and without
ADHD
ADHD: Facts and Statistics
• Prevalence (BD, 3rd. Edition)– Occurs in 4%-12% of children who are 6 to 12 years
of age– Symptoms are usually present around age 3 or 4– 68% of children with ADHD have problems as adults
• Gender Differences – Boys outnumber girls 4 to 1
• Cultural Factors • Probability of ADHD diagnosis is greatest in the
United States
Biological Theories of ADHD• Family and twin studies document a role for
genetic transmission in ADHD
• Frontal lobe function is abnormal in ADHD children– Frontal lobe is underresponsive to stimulation in ADHD
children– Frontal lobe is smaller in ADHD children– ADHD children do poorly on psychological tests that
measure the functioning of the frontal lobe
Ch 15.4
Psychological Theories of ADHD
• Bettelheim proposed a psychoanalytic view of ADHD in which hyperactivity results from stress brought on by parental personality (authoritarian, impatient, resentful)
• Learning theory suggests that hyperactivity is reinforced by the attention it elicits, thereby increasing in frequency and intensity; hyperactivity may represent modeling of older siblings or peers
Ch 15.5
Treatment of ADHD• Stimulant drugs such as methylphenidate (Ritalin) reduce disruptive
behavior and improve concentration– Improve compliance and decrease negative behaviors in many children– Medications do not affect learning and academic performance– Beneficial effects are not lasting following drug discontinuation
• Psychological therapy for ADHD involves– Parent training– Classroom management programs based on operant-conditioning techniques– Aim to increase appropriate behaviors and decrease inappropriate behaviors
• Combined Bio-Psycho-Social Treatments– Are highly recommended
Ch 15.6
Disorders of Undercontrolled Behavior
• Conduct Disorder involves behaviors that violate the rights of others – Aggression and cruelty toward people or animals– Property damage– Lying and stealing– Conduct disorder is marked by callousness and lack of
remorse
• Conduct disorder is more common in boys• Oppositional Defiant Disorder (ODD) distinction
Ch 15.7
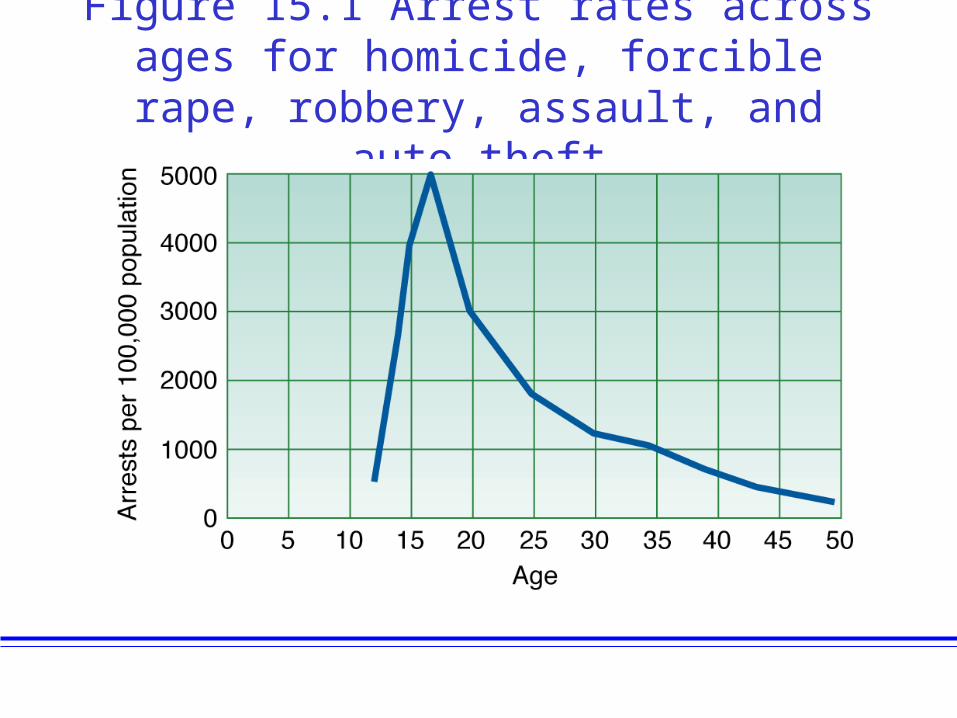
Figure 15.1 Arrest rates across ages for homicide, forcible rape, robbery, assault,
and auto theft
Etiology of Conduct Disorder• Genetic factors may play a greater role in
aggressive behavior, but a lesser role in delinquency-related behaviors – e.g. stealing, running away
• Psychological factors include – Deficiencies in moral training and awareness– Modeling of aggressive behavior (Bandura)– Cognitive distortions in which ambiguous actions are
interpreted as hostile
Ch 15.8
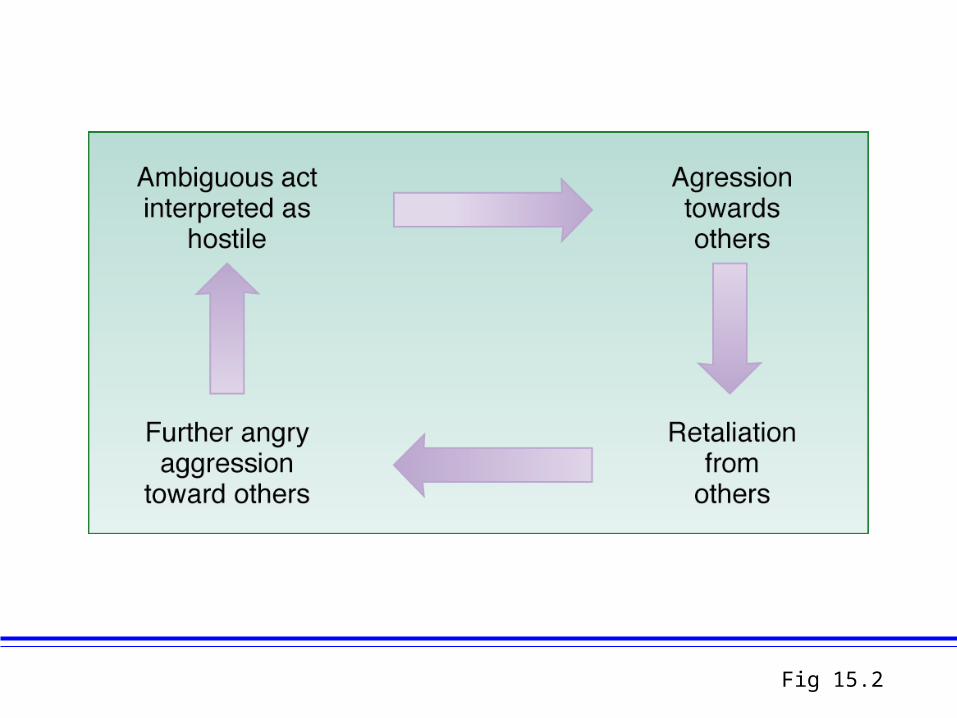
Fig 15.2
Treatment of Conduct Disorder
• Family intervention involves training parents to reward prosocial behaviors in their children
• Multisystem treatment targets the child, the community, the school and the family
• Cognitive approaches involve– Anger control training– Teaching moral development reasoning
Ch 15.9
Learning Disabilities• Learning disabilities refer to inadequate
development in a specific area of academic, language or motor skills– The deficit is not due to mental retardation, autism or
reduced educational opportunities
• DSM covers 3 areas of learning disabilities– Learning disorders– Communication disorders– Motor skills involve impairment of motor coordination
Ch 15.10
• Learning Disorders refer to conditions that impair development in the classroom
• Specific learning disorders identified in DSM-IV include– Reading disorder (Dyslexia) involves difficulty in word
recognition and comprehension– Disorder of written expression involves an inability to
compose the written word– Mathematics disorder involves difficulty in recalling math
facts, errors in addition
Learning Disorders
Ch 15.11
• Communication disorders include– Expressive language disorder involves a difficulty in
speech expression• Difficulty in finding the correct word for a concept• Use of grammar is below grade level
– Phonological disorder refers to a difficulty in articulating speech sounds, but can comprehend words
– Stuttering involves a problem in verbal fluency in which words are repeated or prolonged
Communication Disorder
Ch 15.12
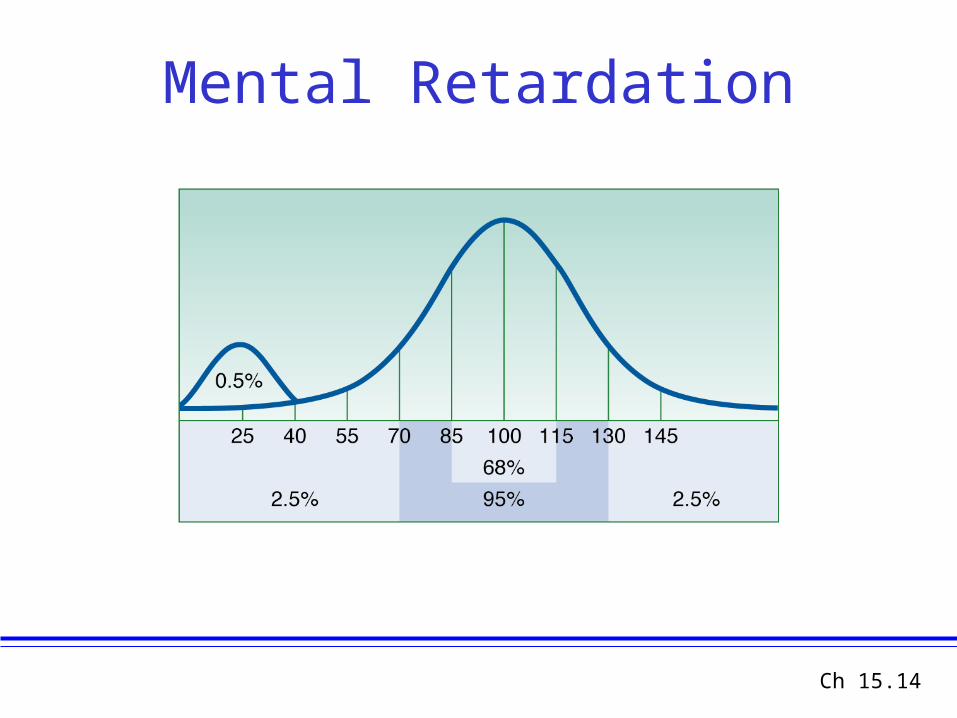
Mental Retardation• Mental retardation is defined as
– Subaverage intellectual functioning• IQ score below 70-75
– Deficits in adaptive behaviors such as dressing, use of money, use of tools and of public transportation
– Onset prior to age eighteen• Not due to adult accidents or disease• Typical onset is in infancy
• American Association of Mental Retardation’s approach– Focus on remedial supports to facilitate higher functioning
Ch 15.13
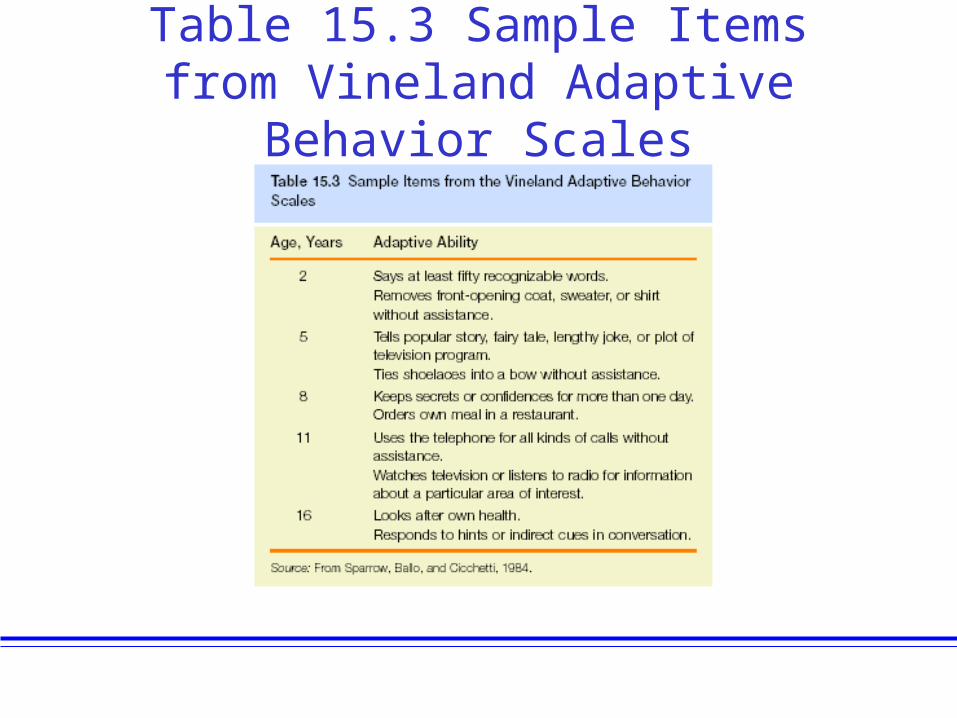
Table 15.3 Sample Items from Vineland Adaptive Behavior Scales
Mental Retardation
Ch 15.14
• No cause is evident for 75% of cases of mental retardation, the remaining 25% are often related to biological causes
• Biological causes include:– Genetic anomalies such as Down’s syndrome (Trisomy
21)– Fragile X syndrome – Abnormality on X chromosome– Recessive-gene diseases such as PKU– Infectious diseases such as Rubella and HIV– Environmental hazards such as mercury or lead poisoning
Etiology of Mental Retardation
Ch 15.15
• Autistic disorder involves children who – Prefer to be alone – Prefer to have a constant environment– Have severely limited language skills
• DSM-IV “Pervasive Developmental Disorder” distinguishes autism as a developmental disorder different from schizophrenia in adults
• Prevalence of autism is infrequent (.05 % of births)– Autism occurs more frequently (4x) in boys relative to girls
Autistic Disorder
Ch 15.16
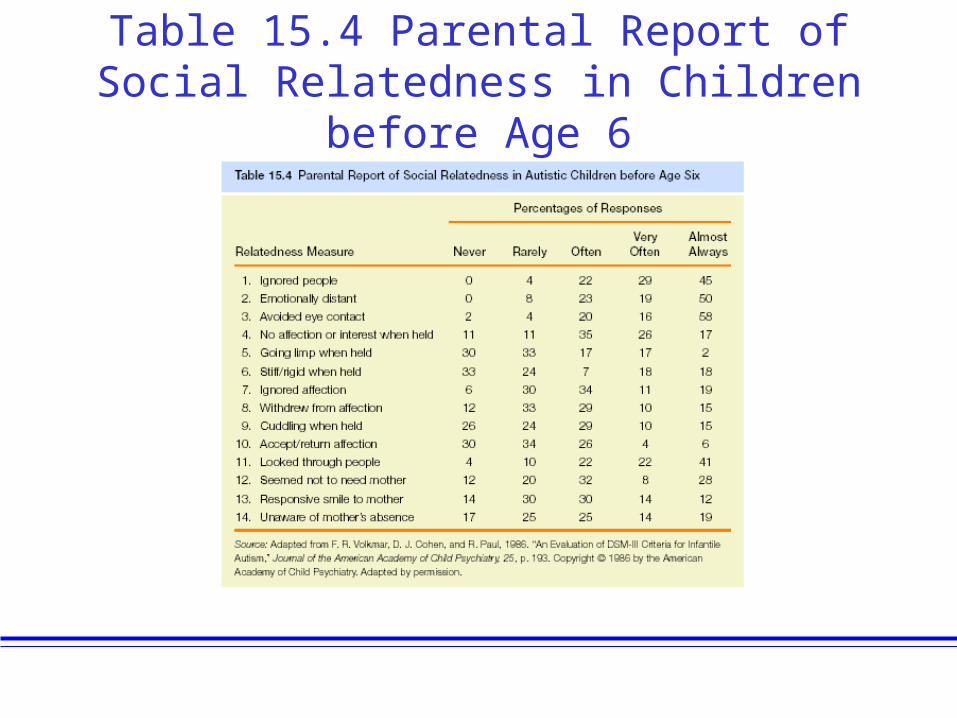
Table 15.4 Parental Report of Social Relatedness in Children before Age 6
Autistic Disorder: Facts and Statistics
• Prevalence and Features of Autism (BD, 3rd. Edition)– Rare condition – Affecting 2 to 20 persons for every 10,000 people– More prevalent in females with IQs below 35, and in males with
higher IQs– Autism occurs worldwide– Symptoms usually develop before 36 months of age
• Autism and Intellectual Functioning– 50% have IQs in the severe-to-profound range of mental retardation– 25% test in the mild-to-moderate IQ range (i.e., IQ of 50 to 70)– Remaining people display abilities in the borderline-to-average IQ
range– Better language skills and IQ test performance predicts better
lifetime prognosis (50% never acquire useful speech)
Etiology of Autism: Psychological Theories
• Bettelheim argued that parental rejection induces autistic disorder
• Behavioral theory suggests that autism results from inattentive parents, especially the mother
• Follow-up studies have found little support for psychological explanations of autism
Ch 15.17
• Genetic factors play a strong role in transmission of autistic disorder – Siblings of a person with autistic disorder have a 75 fold
increase in risk – Twin studies show greater concordance for autism in
MZ twins (60-91% than in DZ twins (0-20%)
• Neurological studies consistently find structural abnormalities in the cerebellum of autistic children (e.g., substantially reduced sized)
Biological Etiology of Autism
Ch 15.18
Treatment of Autistic Disorder • Drug treatment often involves the administration of haloperidol
– Reduces social withdrawal and odd motor behaviors– Haloperidol does not alter the abnormal interpersonal relations or
language impairments of autism
• Efficacy of psychodynamic therapy is unknown• Behavior therapy approach (Lovaas)
– Uses modeling and operant conditioning to reinforce language and prosocial behaviors
– Parent education training increases treatment generalization beyond hospital settings
Ch 15.19