Embed Size (px)
Citation preview

CHAR,4CTERISTICS OF SUBJECTS EXPERIENCING RELAXATION AND RELAXATION-INDUCED ANXIETY
G. R. NORTON, LINDA RHODES and JEAN HAUCH
Unikertity of U’innipeg
and
E. A. KAPROWY
1lanitoba Department of Community Serbices and Correction
Summary-The purpose of this study was to determine the psychological characteristics of people who show a paradoxical increase in anxiety during relaxation training. Thirty-eight sub- jects who reported being anxious 50% or more of the day, were divided into two groups based on their scores on the Tellegen and Atkinson absorption scale. Half of each group was given
progressive muscle relaxation training; the other half a meditational procedure. Separate regression analyses for each group showed that during meditational procedure 32% of the change in heartrate and 42% of the change in a subjective response measured by changes in the position of an “anxiety lever”, could be predicted by the subjects’ scores on the Tellegen absorption scale, the cognitive component of the state version of the Cognitive-Somatic .Anxiety Questionnaire. and other psychological tests. Similarly, 4gv0 of the heartrate changes during progressive muscle relaxation training were predicted by these and other measures. The multiple R for anxiety lever during progressive muscle relaxation training was not significant, however. Three of 18 meditational procedure subjects and two of 20 progressive muscle relaua- tion subjects showed increased heartrates during relaxatton training. Two of the three medita-
tional procedure subjects also shoued an increase in subjective tension as measured by the anxiety lever.
Heide and Borkovec (1983) have provided evidence that relaxation training procedures can produce a paradoxical, relaxation-induced anxiety (RlA) in some people. Although their research was exploratory, it and a subsequent theoretical analysis (Heide and Borkovec, 1984) have identified several factors that might be useful in predicting who would show relax- ation-induced anxiety. Heide and Borkovec’s data suggest that variables predicting increased arousal during progressive muscle relaxation (PMR) may not be the same as those predicting increased arousal during focused relaxation (MED), a form of meditation similar to transcendental meditation. For example, the correlations between subjective measures and composite change scores during progressive
muscle relaxation training and the meditational
procedure often had different signs. Further- more, of 10 persons reporting an increase tn tension during relaxation, only one reported it during both procedures.
These data suggest that different processes may be operating during progressive muscle relaxation training and meditational procedures
to produce relaxation or its opposite, relaxation- induced anxiety. This is consistent with results reported by Norton and Johnson (1983). They found that subjects who expressed anxiety somatically (Schwartz, Davidson and Goleman, 1978) improved significantly on subjective, behavioral and physiological measures of anxiety following progressive muscle relaxation training but not Agni Yoga training. Results
Requests for reprints should be addressed to G. R. Norton. Department of Psychology. University of Winnipeg, 515 Portage Avenue. Winnipeg. lLlanitoba R3B 2E9, Canada.
21 I

212 C. R. NORTO%, LISD\ RHODES, JE-\S H.\UCH and E. .A K.\PROLV?
were similar, but less pronounced, for cogni- tively anxious subjects who benefited more from Agni I’oga. These results suggest that people who show relaxation-induced anxiety during progressive muscle relaxation may have different psychological characteristics than those showing it during meditational procedure.
The purposes of the present study were: (1) to determine if subjects selected using criteria similar to those reported in Heide and Borkovec
(1983) would show relaxation-induced anxiety following brief training in progressive muscle
relaxation or meditational procedure and; (2) if relaxation-induced anxiety produced by progressive muscle relaxation or meditational procedure could be predicted by the subject’s responses to psychological tests.
Subjects
blETHOD
Onr hundred and ninety-two Introductory Psychology students completed a brief screening questionnaire which included (I) a Likerr-type question that asked subjects what
percent of the day thry were anxious, (2) Tellegen’s Absorption Scale (TAS; Tellegen and Atkinson. 1974), (3) the CognitiLs-Somatic Anuietk Questionnaire-Trait
(CSAQ-T; Schwartz. Davidson & Goleman, 1978). the Vando Reducer-Augmentor Scale (R.A; Vando, 1974). and (5) the State-Trait .Anriety Inventory (STAI; Speilberger. Gorsuch, R: Luschene, 1970). To qualify for the stud), subjects had to report they were anxious jOro or more of the day. Of those who met this criterion, the iirst 20 males
and 20 females contacted by telephone who were able to participate served as subjects. The subjects ranged in age from IS to 25. uirh a mean of 19.9. .AII subjects received
course credit for their participation.
A reanalysis of Heide and Borkovec’s (1983) results showed that correlations berueen their subjects’ scores on
the Tellegen Absorption Scale (TAS) and their composite scores during progressive muscle rrla.xation and during
meditational procedure differed significantly, I (IO) = 2.81, P < 0.05, Therefore, to assure an equal distribution of subjects \<ith high and IOU TAS scores, subjects in the
present study, regardless of sex, were dibidrd into tuo groups using a median split bated on their scores. The tv.o groups of TAS subjects were then randomly assigned to either .\leditation (IIED: Carrington, 1977) or Progressike
Muscle Relaxation (PMR; Bernstein & Borkovec. 1973) training groups.
Procedure ‘vvhsn each subject arrived at the laboratory he/she was
asked to complete the Cognitive-Somatic Anuiery Question- naire-state (CS.AQ-S; Heide si Borkovec, 1983). After completing the CSAQ-S, the subject was seated in a reclin- ing chair and EKG electrodes uere attched to each leg and the left arm. The subject uas then shown ho\r to use an
“an.xltt) Ie\cr”. a moiable leper s~m~lsr to that reported
b) I\‘~ncze:. Vsndlrrl. Barlou and Xla\issakalian (1980) for msasuring ssvual arousal. Subjects v,txe told that when the l:ier. \\hich mohed rhrouah a Y°ree arc, \bas pulled
completely bath it represented “no anuiery”, mid-ua)
represented “moderate an.xiet\“. and completely foruard represented “bsr> Intense anxiety”. Heishe \has then told to use the lever throughout relaxation training to indicate
his/ her moment-to-moment changes in rslaxarion/tension. The subject icas then asked to practice using the anxiety lever \\hile imagining different levels of anxiety. EKG and anxiety lever responses !\ere recorded on a Grass 788
polygraph using iP_I-D and 7PI pre-amplifers, respectively.
.Aiter electrodes were attached and the an?tiet)- lever esplained, subjects were allowed to adapt to the room and equipment For IO min. During this time period, they were
told to relax and that they kvould soon receive taped instruc-
tions \ia headphones. Following adaptation, subjects in both the progressive
muscle relaxation and medlrational procedure conditions heard a IO-min taps providing a rationale and brief des- cription of the relavation training procedure. The brief relaxation training duration was used because, in most
cases. subjects who showed relaxation-induced anxiety in Hzids and Borkovec’s (1953) study did so within the first
two recording intervals (approx. 12 min). The tapes, which Here prepared by an advanced undergraduate student
acqualnted with both procedures, but unaware of the purpows of the study, k%ere played on a Sony model 2C-61 portable cassette recorder. Those in the progressive muscle relaxation condition were provided with instructions based on Bernstein and Borkovec (1973) to relax the feet and
calves, stomach and shoulders. Those in the meditational procedure condition heard mantra meditation instructions
baied on Carrington’s (1977) mcditatlon procedure. Sub- jects were provided with three mantras to choose from and Lrerr instructed to initially say the chosen mantra aloud,
then whispered and, finally, silently. Tapes were equated for length, number of spoken **ords and length of pauses between sets of instructions. Heart rate and an.xiety lever were monitored for I-min intervals during baseline (the last minute of the adaptation period), at 2 min. 4 min, and 6 min of relaxation training, and 1 min post-training.
RESULTS
Thirty-eight subjects completed all phases of testing and treatment. Data from two subjects, both in the meditational procedure treatment condition, were eliminated because of one sub- ject’s failure to answer items on the question- naires and because another failed to use the anxiety lever during treatment.
An all subsets multiple linear regression analysis (BMDP9R); Dixon, 1983) was com-
puted for changes in heartrate between baseline and 1 min post-treatment (e.g., X heartrate at post-treatment-,? heartrate at baseline). This
REL.4SXTION INDUCED XNNlETk 213
procedure was repeated for changes in anxiety
lever. The cognitive and somatic scales of the CSAQ-T and CSAQ-S, TAS, RA and the State and Trait scales of the STAI were included as predictor variables. Separate all subsets re- gression analyses were computed for subjects who received meditational procedures and for those who received progressive muscle relax- ation training because Heide and Borkovec (1983) had obtained different outcome measures from these two procedures. Furthermore, pre- liminary analyses of the data from the present study supported their findings. An overall multiple correlation between heartrate, anxiety lever, and the predictor variables showed that the correlations differed markedly for subjects receiving meditational procedure and those receiving progressive muscle relaxation training.
Meditation Results of evaluation of assumptions led to
transformations of some of the variables to
reduce skewness in their distributions, improve normality, linearity, and homoscedasticity of residuals. A log transformation was used for the cognitive measures of the CSAQ-S, and a square root transformation was used with the State measure of the STAI (STAI-S). All other variables were used untransformed.
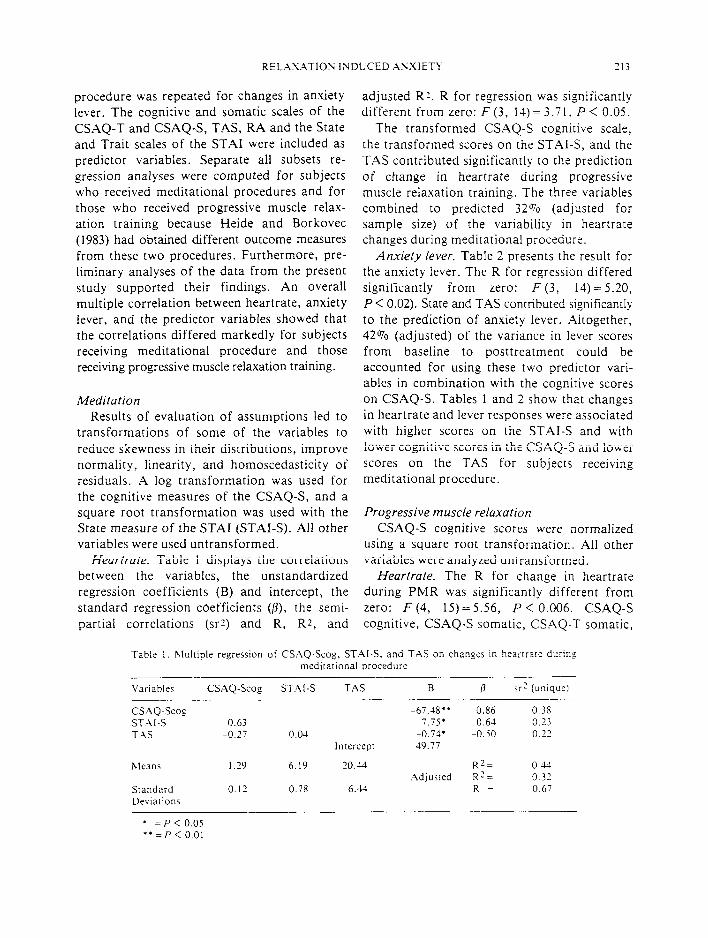
Heartrate. Table 1 displays the correlations between the variables, the unstandardized regression coefficients (B) and intercept, the standard regression coefficients (p), the semi-
partial correlations (srz) and R, Rz, and
adjusted RI. R for regression was significantly different from zero: F (3, 14) = 3.71. P < 0.05.
The transformed CSAQ-S cognitive scale,
the transformed scores on the STAI-S, and the TAS contributed significantly to the prediction of change in heartrate during progressive muscle relaxation training. The three variables combined to predicted 32oio (adjusted for sample size) of the variability in heartrate changes during meditational procedure.
Anxiety lever. Table 2 presents the result for the anxiety lever. The R for regression differed
significantly from zero: F (3, 14) =5.20, P < 0.02). State and TAS contributed significantly to the prediction of anxiety lever. Altogether, 42% (adjusted) of the variance in lever scores from baseline to posttreatment could be accounted for using these two predictor vari- ables in combination with the cognitive scores on CSAQ-S. Tables 1 and 2 show that changes in heartrate and lever responses were associated with higher scores on the STAI-S and with
lower cognitive scores in the CSAQ-S and lower scores on the TAS for subjects receiving meditational procedure.
Progressive muscle relaxation CSAQ-S cognitive scores were normalized
using a square root transformation. All other variables were analyzed untransformed.
Heartrate. The R for change in heartrate during PMR was significantly different from zero: F (4, 15)=5.56, P < 0.006. CSAQ-S
cognitive, CSAQ-S somatic, CSAQ-T somatic,
Table I. Multiple regression of CSAQ-Scog. STAI-S, and TAS on changes in heartrare during
meditational procedure
Variables CSAQ-Scog STXI-S TAS B P sr? (unique1
CSXQ-Scog ST.+‘.I-S TAS
hleans
Standard
Deviations
-67.18” -0.86 0.38 0.63 7.75* 0.64 0.23
-0.27 0.04 -0.74’ -0.50 0.22 Intercept 49.77
1.29 6.19 Zl3.U R2= 0.44
Adjusted R?= 0.32 0.12 0.78 6.44 R = 0.67
* = P < 0.05 **=p< 0.01
211 C. R. \ORTO\.. Li’~0.4 RHODES. JEAN HlUCH and E. 4. K-\PROL\ \(
Table 2. .XIult~ple regression of CS.-\Q-Scog. ST;\I-S. and T-\S on changs in anulst> Ir\?r dung meditationai procedure
L arlablr, CS-\Q-Scog ST\l-S T4S
CS.AQ-Scog ST.+I-S 0.63 TAS -0.27 0.04
Inrercrpr
\lean5 I .29 6.iY ‘0.4-l Standard 0.12 0.78 6.13
De\iatlons
B P ,r2 iunique)
-51.6-l -0 32 0.05 13.13’ 0.53 0. I6 -3.16” 4.7’ 0.44 15.19
l = P < 0.05 ** = P < 0.01
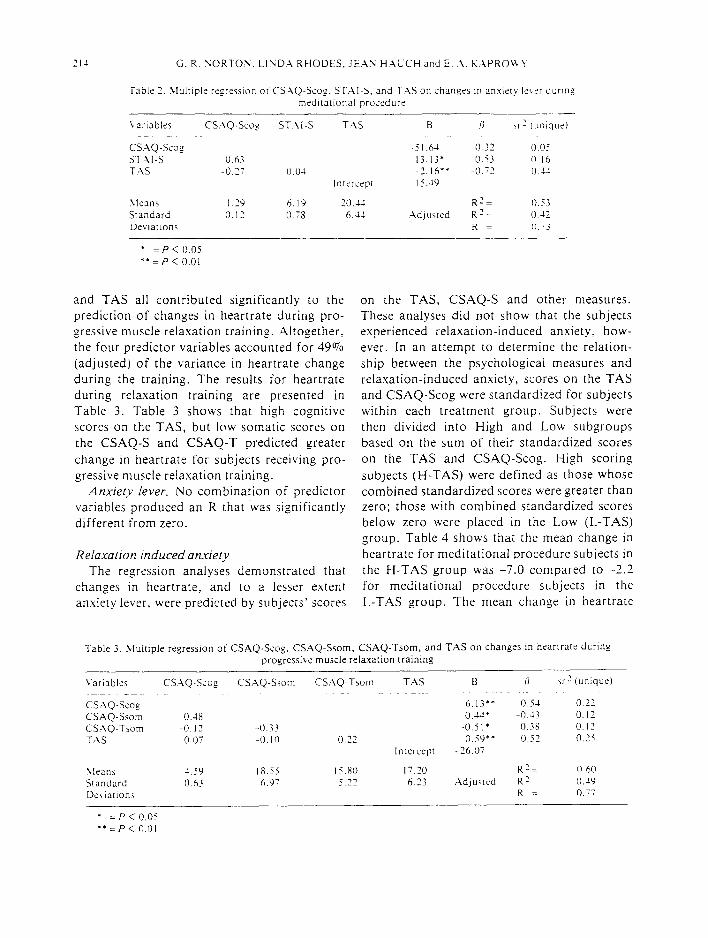
and TAS all contributed significantly to the prediction of changes in heartrate during pro- gressive muscle relaxation training. Altogether, the four predictor variables accounted for 49% (adjusted) of the variance in heartrate change during the training. The results for heartrate during relaxation training are presented in Table 3. Table 3 shows that high cognitive scores on the TAS, but low somatic scores on the CSAQ-S and CSAQ-T predicted greater
change in heartrate for subjects receiving pro- gressive muscle relaxation training.
Anxiety lever. No combination of predictor variables produced an R that ‘was significantly different from zero.
Relaxation induced anxiety The regression analyses demonstrated that
changes in heartrate, and to a lesser extent anxiety lever, were predicted by subjects’ scores
on the TAS, CSAQ-S and other measures. These analyses did not show that the subjects experienced relaxation-induced anxiety, how- ever. In an attempt to determine the relation-
ship between the psychological measures and relaxation-induced anxiety, scores on the TAS and CSAQ-Scog were standardized for subjects within each treatment group. Subjects were then divided into High and Low subgroups based on the sum of their standardized scores on the TAS and CSAQ-Scog. High scoring
subjects (H-TAS) were defined as those whose combined standardized scores were greater than zero; those with combined standardized scores below zero were placed in the Low (L-TAS) group. Table 4 shows that the mean change in heartrate for meditational procedure subjects in the H-TAS group was -7.0 compared to -2.2 for meditational procedure subjects in the L-TAS group. The mean change in heartrate
Table 3. hlultiple regression of CSAQ-S-o,, ‘ o CSAQ-Ssom, CSAQ-Tsom, and TAS on changes in heartrate dcring
progressive muscle relaxation training
Variables CS.-\Q-Scog CSAQ-Slam CSAQ-T,om TAS B ii \r? (unique) _~
CS.-\Q-Scog 6.13” 0.5-l 0.22 CSAQ-Slam 0.48 ~O.J4* -0.13 0.12 CSAQ-Trom -0.12 -0.33 -O.jl* -0.38 O.IZ T;\S 0.07 -0. IO 0.” 0.59** 0.57 0.25
Intercept -26.07
Lleani -I.SY 18.55 lS.Ril I7.20 R 2 =. 0.60 Standard 0.63 6.Y- 5.22 6.23 .AdJlJVrld n2, 0.49
De\iatronl R = 0.77
* = P < 0.05 “=P<OOl

REL.4S.4TION INDUCED ANXIETY 215
for progressive muscle relaxation training sub- DISCUSSION
jects in the H-TAS group was -1.3 compared to The results of this study provide some
-7.5 for meditational procedure subjects in the support for Heide and Borkovec’s (1983, 1984)
L-TAS group. Three of 10 subjects receiving description of relaxation induced anxiety. Using
meditationa! procedure who were in the L-TAS heartrate as a measure of anxiety, a small
group showed increased heartrates compared to number of subjects in both the meditational
none of the subjects in the H-TAS group. The three subjects showed a mean increase in heart-
rate of 12 beats/min. The number of H-TAS and L-TAS subjects who showed a decrease in heartrate were compared with those whose heartrate increased or remained the same during meditational procedure. The results showed significantly more (x2(1) =4.11, P < 0.05) L- TAS subjects did not decrease their heartrate during meditational procedure. Similar, but opposite, results occurred for subjects who received progressive muscle relaxation: two of 12 subjects in the H-TAS group, but none in the L-TAS group showed increased heartrates. The two subjects showed a mean increase of 10 beats/min. A Chi-square analysis showed that significantly (x2(1) = 4.20, P < 0.05) more H- TAS subjects than L-TAS did not decrease their heartrate during progressive muscle relaxation training.
The results for the anxiety lever are similar for the meditational procedure subjects. The subjects with high standardized TAS and
CASQ scores showed a mean change of -23.1 points compared to a mean of -10.6 for the L- TAS group. Three subjects showed an increased score on the anxiety lever, during meditation training. Two of the three subjects also showed
an increase in heartrate. Because earlier analyses had shown that TAS and CASQ did not predict changes in anxiety lever scores for progressive muscle relaxation subjects, these data were not analyzed further.
procedure and progressive muscle relaxation training groups showed a paradoxical increase in anxiety during relaxation training. Consistent
with Heide and Borkovec’s (1983) findings, the characteristics of subjects who showed rela-u- ation-induced anxiety during meditation pro- cedures, differed from those who showed it during progressive muscle relaxation training. The similarities are interesting considering that
Heide and Borkovec’s (1983) subjects were community volunteers and the subjects in this study were university students. In the present study, subjects who showed a decrease in heart- rate during meditational procedure reported high levels of cognitive anxiety (CSAQ-Scog) and openness to new experiences (TAS). The only subjects in the meditation procedure group who showed increased heartrates were those who had a low combined score on TAS and CSAQ-Scog. Similarly, those who showed a decreased heartrate during progressive muscle relaxation reported high levels of somatic anxiety (CSAQ-Ssom and CSAQ-Tsom) and scored low on the TAS measure of openness to new experiences (or the ability to become imagi- natively involved); those who showed relax- ation-induced anxiety had a high combined TAS and CSAQ-Scog score.
Heide and Borkovec (1983, 1984) suggest that several different psychological processes such as fear of losing control, fear of sensations evoked by the relaxation process and fear of
Table 3. Number of subjects showing increased, no change or decreased heartrates during medirarional procedure and progressive muscle relaxation training
hleditational Progressive \lUsCle Group Procedure Relaxation Training
N Inc. Same Dec. XChange N Inc. Same Dec. 2 Change
High CSAQ-TAS 8 0 0 8 -7.0 I2 2 5 5 -1.3
Low CSAQ-T.4S IO 3 I 6 -2.2 8 0 I 7 -7.3

216 G. R. hORT0.L. LIND.4 RHODES, JE.45 HAUCH and E. .A. KXPROI%‘F
having attention drawn to the experiencing of anxiety could lead to relaxation-induced anxiety. Davidson and Schwartz (1976) have provided a model that accommodates these
hypothesized relaxation-induced anxiety inducing processes and the results of the present study. They suggest that a person’s ability to relax is influenced by cognitive, somatic and attentional dimensions. The cognitive dimen- sion is related to what Borkovec, Robinson, Pruzinsky and DePree (1983) have described as “worry”, and somatic anxiety is related to
changes in autonomic and musculoskeletal activity. The attentional dimension, which has received the least empirical attention, is hy- pothesized to be the “self generation of behav- ior and focused attention upon the results of this resulting in restriction of awareness” at one end of the dimension and “passive receptivity and the concomitant ‘opening-up’ of aware- ness” (p. 401) at the other end.
Davidson and Schwartz’s (1976) hypothesis is directly supported by the results of the present study and those of Norton and Johnson (1983). Both of these studies show that response to relaxation training is an interaction between the characteristic ways a person experiences anxiety (cognitively or somatically) and the type of relaxation training procedure. The present study further demonstrated that relaxation- induced anxiety occurs when there is a mis- match between these variables.
REFERESCES
Berns:ein D. A. and Borkovec T. D. (1973) Pr~gressrve
Rrlaxarion Trammg. Research Press. Champaign.
Illinois.
Borkovec T. D.. Robinson E. Pruzinsky T. and Depress
J. A. (1983) Preliminary exploration of worry: some characteristics and processes. Behnv. Res. Thu. 21. P-16.
Carrlngton P. (1977) Freedom in Med~rarron. Doubleday
Xnchor. Neu York. Davidson R. J. and Schwartz G. F. (1976) The psycho-
biology oi relaxation and related states: A multi-process theory. In Behavior Conirol and lModificarion of Physio-
iogtcal Acrlrt!y (Edited by Xlostofsky D. 1.). Prentice-
Hall. New York.
Dixon %‘. J. (1983) BMDP Statisrlcai Sofiware. University of California Press, Berkeley.
Heide F. J. and Borkovec T. D. (1983) Relaxation induced anxiety: Paradoxical anxiety enhancement due to relax-
ation training. J. Consult. C/in. Psychol. 51, 171-182. Heide F. J. and Borkovec T. D. (1983) Relavation induced
anxiety: hlechanism and theoretical implications. Behav. Res. Ther. 22. I-12.
Norton G. R. and Johnson N’. E. (1983) A comparison of tHo relaxation procedures for reducing cognitive and
somatic anxiety. J. Behar. Ther. & Eh-p. Psychiai. 14, 209-2 14.
Schwartz G. E.. Davidson R. J. and Coleman D. J. (1978) Patterning of cognitive and somatic processes in the self- regulation of anxiety: Effects of meditation versus
exercise. Psychosom. ‘Wed. 40, 321-328. Speilberger C. D., Gorsuch R. L. and Luschene R. E.
(1970) STAI-jMonuaf for fhe Slale-Trail Anxiery Invenlory. Consulting Psychologists Press, Palo Alto.
Tellsgen A. and Atkmson G. (1974) Openness to absorbing and self-altering experiences (“Absorption”), a trait related to hypnotic susceptibility. J. abnorm. Psychol. 83,268-277.
Vando A. (1973) The development of the R-A scale: A
paper and pencil measure of pain tolerance. Personalify and Social Psychology Bulletin 1, 28-29.
Wincze 1. P., Venditri E., Barlow D. and blavissakalian M.
(1980) The effects of a subjective monitoring task in the measurement of genital response to erotic stimulation. Archssex. Behav. 9,533-545.
Acknow[edgemen&-This study \\as supported by grants from the Manitoba Xlental Health Research Foundation and the Universtty of (Vinnipeg. The authors express their appreciation to lnge Kirshoff for her assistance in producing the relaua- tion tapes, to Dr. T. Borkovec for his comments on an earlier version of this paper and to an anonymous reviewer for his/her helpful comments. The research reported in rhis study \vas completed by the second author in partial fulfilment of the requirements of a BA (Hons.) degree.