Embed Size (px)
Citation preview

Vol. 16 No. 3 September 1998 Journal of Pain and Symptom Management 179
Original Article
Characterization of Breakthrough Pain byHospice Patients and Their CaregiversPerry G. Fine, MD, and Michael A. Busch, PhDDepartment of Anesthesiology (P.G.F.), University of Utah; National Medical Director (P.G.F.),VistaCare, Scottsdale, Arizona; and Anesta Corporation (M.A.B.), Salt Lake City, Utah, USA
AbstractThis study sought to characterize the nature of breakthrough pain experienced by 22hospice patients and to assess the perceptions of their respective caregivers. Questionnaireswere administered by trained hospice nurses to determine key elements of episodic pains inthis home-based terminally ill population. Eighty-six percent of the patients surveyedexperienced breakthrough pain, with an average of 2.9 episodes per 24-hr period and amean pain intensity of 7 on a ten-point scale, compared with average baseline pain scoresof 3.6 (daytime) and 2.6 (nighttime). Breakthrough pain episodes lasted 52 min onaverage, with a range of 1–240 min. The range of time to relief of breakthrough painswas 5–60 min, with a mean of 30 min. Caregivers’ perceptions of the pain intensities,duration, amount of relief, and time to relief were much more likely to be inaccurate, andwere usually underestimates. This study suggests that breakthrough pain is common in thehospice setting and that there is poor concordance between patients’ self-reports and theircaregivers’ perceptions of these pains. It is concluded that the pharmacodynamics ofcurrently available oral analgesics are not well-suited for breakthrough pain and thatbetter communication between patients and caregivers may lead to more optimal painmanagement. J Pain Symptom Manage 1998;16:179–183. U.S. Cancer Pain ReliefCommittee, 1998.
Key WordsBreakthrough pain, incident pain, hospice, analgesia
suffering in these patients.2,3 However, thereIntroductionare few epidemiological data concerning break-
Patients with advanced cancer and other life-through pain, either qualitatively or quantita-
limiting illnesses commonly experience moder-tively.
ate to severe pain.1 Episodes of severe pain oc-Portenoy and Hagen4 evaluated inpatients in
curring on a background of otherwise con-a major regional cancer referral center, docu-
trolled pain, known as breakthrough pain, ismenting the common occurrence and charac-
acknowledged as an important contributor toteristics of breakthrough pain. To supplementthose observations, this survey was designed toevaluate the characteristics of these episodicAddress reprint requests to: Perry G. Fine, MD, Painpains occurring in home-based hospice pa-Management Center, 546 Chipeta Way, Suite 2000,
Salt Lake City, Utah 84108, USA. tients. Because these patients are highly de-Accepted for publication: December 10, 1997. pendent upon a primary caregiver within the
U.S. Cancer Pain Relief Committee, 1998Published by Elsevier New York, New York
0885-3924/98/$19.00PII S0885-3924(98)00045-1

180 Fine and Busch Vol. 16 No. 3 September 1998
home, the perceptions of these caregivers were Interventions for treating breakthroughpains.also viewed as relevant.Amount of relief from breakthrough pain in-tervention(s).Time until meaningful relief from break-
Methods through pain.Anticipatory treatment (prevention) ofThe study was approved by the University ofbreakthrough pain.Utah Institutional Review Board. A question-
naire was developed to collect salient data re-Pain intensity/severity and relief scores weregarding breakthrough pain from interviewsassessed and reported using a 0–10 linear ana-with hospice patients with a history of persistentlogue scale. Means, modes, or both were de-pain. A similar questionnaire was worded to as-rived for numerical data but statistical signifi-sess breakthrough pain information from thecance was not reported due to the small sampleperspective of the patients’ primary caregivers.size.To accommodate the debilitated state of this
patient population, questionnaires were de-signed by field test to be administered in under Results15 min.
Home hospice nurses were trained in the useDemographicsof the questionnaires and recorded patient and
Twenty-two home hospice patients, 9 malescaregiver responses from a convenience sampleand 13 females, and their respective primaryof consecutive patients. Nurses were instructedcaregivers completed the survey. Four patientsto survey those patients under their care whowere between 8 and 18 years, eight patientsthey knew were experiencing some degree ofwere between 19 and 65 years, and ten pa-pain due to their disease. Only patients whotients were 65 years of age or older. Primarywere able to communicate and who had a care-diagnoses included breast cancer (three pa-giver at home were included. Each patient/tients), lung cancer (three patients), prostatecaregiver questionnaire was completed onecancer (two patients), leukemia (two patients),time with attention drawn to the previous 24-progressive neuromuscular disease (two pa-hr period of time. Breakthrough pain was de-tients), and one each of cancers originating infined as ‘‘a transitory increase in pain to greaterthe brain, liver, pancreas, kidney, stomach, andthan moderate intensity (that is, to an intensitythymus. Additionally, there was a single case ofof ‘severe’ or ‘excruciating’) which occurredmultiple myeloma and three unspecified dis-on a baseline pain of moderate intensity or lesseases. Of the primary caregivers, nine were ei-(that is, no pain or pain of ‘mild’ or ‘moderate’ther a spouse or mate, three were parents, sixintensity).’’4
were a son or daughter, two were other familyIn addition to basic demographics, the fol-relations, and, for two, the relationship was notlowing variables were recorded:identified.
Current analgesics taken on a fixed schedule.PrevalenceUsual pain intensity during most hours of the
Nineteen of the twenty-two (86%) surveyedday and night.patients with persistent pain reported experi-Number of breakthrough pain episodes perencing breakthrough pains on a regular and re-24-hr period.curring basis. About one-half of these painsUsual average severity of breakthrough painwere described as predictably occurring in asso-episodes.ciation with a specific activity, fitting the term,Usual duration of breakthrough pain epi-‘‘incident pain.’’sodes.
Predictability and causes, if identifiable, ofbreakthrough pains. Pain Locations
A wide range of discrete pain locations wasQuality of breakthrough pains (word descrip-tors from a proferred list). reported (one to nine sites) by each patient. In
order of frequency, these included the lowBody locations of breakthrough pains.

Vol. 16 No. 3 September 1998 Breakthrough Pain in Hospice Patients 181
back, abdomen, pelvis, leg(s), chest, arm(s),neck, shoulders, upper back, feet, flank, head,face, rectum or anus, and one unspecified site.The mean number of sites reported was 2.5.
Pain DescriptorsThe most common breakthrough pain de-
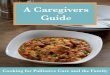
scriptors were ‘‘sharp’’ and ‘‘radiating/shoot-ing.’’ The terms ‘‘pressure/squeezing/tight,’’‘‘aching,’’ and ‘‘burning’’ were used less fre-quently, and ‘‘throbbing,’’ ‘‘crampy,’’ ‘‘stab-bing’’ and ‘‘other’’ were reported by a few pa-tients. The mean number of descriptors usedwas 1.6, with two descriptors being listed most Fig. 1. Time to relief in 19 home hospice patients
with breakthrough pain.commonly.
Diurnal Variation in Painnous methadone, or intrathecal morphine.Breakthrough pain occurred during the dayThree patients relied upon acetaminophen.in 86% of patients and during the night in 45%
Other psychological or physical modalitiesof cases. These pains were reported as oc-used were ultrasound, relaxation, reposition-curring every day in 50% of patients and everying, ice, heat, massage, bathing, or a cool clothnight in 22% of patients.compress. Two patients reported using neitheranalgesics nor other modalities to relieve theirUsual (Baseline) Pain Intensitysymptoms.Pain scores were assessed using a 0–10 ana-
A wide variation in reported time to pain re-logue scale. Average, or usual, baseline daylief was evident, ranging from 5 min to 60 mintime pain ratings were reported as a mean of(Figure 1).3.6, a mode of 5. One patient exceeded a 5/10
pain rating, reporting his ‘‘usual’’ pain to be Breakthrough Pains: Characteristics and8/10, but this actually reflected the intensity of Patient–Caregiver Concordancehis breakthrough pain, which was, indeed, hisThe frequency, intensity, and duration of ep-most ‘‘usual’’ pain, illuminating an ambiguity
isodic pains are tabulated in Table 1. Findingsassociated with communication. Of the patientscomparing patients’ reports and their caregiv-reporting night time pain, the mean intensityers’ observations are presented in Table 2.was 2.5.
Fixed Schedule Opioid Analgesics DiscussionNineteen of the twenty-two patients surveyed
The results of this study strongly suggest thatreported using one or more analgesics on a reg-breakthrough pain is a very common occur-ular schedule. Ten used continuous or sus-rence in hospice patients with otherwise well-tained release morphine, four used transder-controlled underlying continuous pain prob-mal fentanyl patches, two used oral orlems from a variety of causes. Although this isintravenous methadone, two used hydroco-a smaller sample, it appears that the incidencedone, two used continuous release oxycodone,
and one patient used intrathecal morphine.
Table 1Breakthrough Pain Interventions Characteristics of Episodic Pains
Use of short-acting oral opioid formulations Mean Mode Rangewere the most common means of relieving
Episodes/24 hr 2.9 2 1–5.5breakthrough pains. Seven patients reported Pain intensity a 7 9 3–10using hydrocodone, five used concentrated Duration (min) 52 15, 60, 240 ,1–240oral morphine solution, and four used oxyco- aPain intensity: 0 5 no pain; 10 5 pain as bad as you can
imagine.done. One each used oral methadone, intrave-

182 Fine and Busch Vol. 16 No. 3 September 1998
Table 2Concordance of Caregivers to Patients, No. (%)
Baseline pain Breakthrough pain
UPI UPI No. Duration Amount MinutesEstimates Day Night episodes (min) Severity of relief to relief
Caregiver overestimates 3 (14) 5 (24) 6 (30) 6 (32) 6 (29) 8 (38) 4 (20)Caregiver underestimates 6 (29) 4 (19) 9 (45) 9 (47) 9 (43) 5 (24) 10 (50)Concordance 12 (57) 12 (57) 5 (25) 4 (21) 6 (29) 8 (38) 6 (30)
UPI, usual pain intensity; values reported represent the number of caregivers who overestimated or underestimated patients’ scoresby at least 2 points on a 0 to 10-point analogue scale.
of breakthrough pain in hospice patients is The methodology of this study lends itself topotential errors in interpretation in two ways.higher than in the cancer population reported
by Portenoy and Hagen.4 This is probably due The data may be skewed in the direction ofoverestimation of breakthrough pain preva-to the fact that the hospice patients, by defini-
tion, are further along in their respective dis- lence by focusing only on patients who ac-knowledge persistent pain. However, becauseease trajectories.
In this study, no attempt was made to deter- previous studies1,6 have evaluated family per-ceptions of patients’ pain and have demon-mine or infer the etiologies of the pains. How-
ever, similar to the results of Portenoy and Ha- strated the prevalence of pain in patients withadvanced cancer and other life-limiting dis-gen,4 about one-half the occurrences of
breakthrough pain were precipitated (that is, eases, we are confident that these data accu-rately reflect the experiences of most termi-incident pain), and therefore predictable to
some degree. nally ill patients. Conversely, these survey datamight underestimate breakthrough pain preva-It is noteworthy that persistent pain ratings
and frequency of breakthrough pains demon- lence by overlooking patients who do not com-plain of pain.strate diurnal variation, with lessening during
nighttime hours. This observation corroborates In summary, it appears that breakthroughpain is a predictable consequence of most ad-the findings of Bruera et al.5 who documented
a similar pattern of diurnal variation in opioid vanced cancers, and perhaps many other pro-gressive, life-limiting disease processes, and itanalgesic requirements in a palliative care unit.
It would be premature to put too much stock in seems that these pains tend to become moreprevalent as patients progress toward the termi-speculation about this observation until more
studies assess this phenomenon. However, it nal phase of their respective disease. These ob-servations logically lead to the assertion that as-suggests that continuous and breakthrough
pain, as matters of awareness, are not brought sessment and treatment for breakthroughpains in this population should be the rule.to patients’ conscious attention as avidly during
sleep hours. Sleep may physiologically blunt Caregivers need to be educated in how tomatch their perceptions with what is actuallythe perceived intensity of breakthrough pains.
As well, it may be that nocturnal pain, regard- occurring in those for whom they are caring sothat preventative and therapeutic interventionsless of type or cause, is not recalled as vividly
as those occurring during usual waking hours, can be optimized.Based upon the prevalence, frequency, in-when pain assessment interviews are carried
out. tensity and duration of breakthrough pains, itcan further be concluded that cancer patients,Because primary caregivers are often the
ones responsible for offering or administering as well as other populations at risk for this prob-lem, require specifically tailored therapeuticanalgesics, it was viewed as important to assess
their perceptions. The data (Table 2) suggest tools.7–9 The development of analgesic formula-tions and drug delivery systems which allowthat caregivers usually underestimate patients’
self-reports of number, intensity, and duration noninvasive administration, rapid absorptionfor quick onset, individual and episodic titra-of breakthrough pain episodes, as well as
amount of time to relief from pain. tion, and have a short to moderate effective du-

Vol. 16 No. 3 September 1998 Breakthrough Pain in Hospice Patients 183
5. Bruera E, Macmillan K, Kuehn N, Miller MJ. Cir-ration should greatly contribute to the im-cadian distribution of extra doses of narcotic analge-proved well-being of these patients. Forsics in patients with cancer pain. A preliminary re-
example, a product now under review by the port. Pain 1992;49:311–314.U.S. Food and Drug Administration, oral trans-
6. Lynn J, Teno J, Phillips R, et al. Perceptions bymucosal fentanyl citrate (OTFC), with these family members of dying experience of older and se-characteristics has been tested extensively in riously ill patients. Ann Intern Med 1997;126:97–
106.both postoperative and cancer pain popula-tions, and appears to offer meaningful relief of 7. Fine PG. Advances in cancer pain management.
In: Lake CL, Rice LJ, Sperry RJ, eds. Advances in an-breakthrough pain within 5 min, equivalent toesthesia. St. Louis: Mosby, 1995:133–158.intravenous (patient controlled analgesia)
morphine.10–13 8. Ashburn MA, Fine PG, Stanley TH. Oral trans-mucosal fentanyl citrate for the treatment of break-through cancer pain. Anesthesiology 1989;71615–617.Acknowledgment
9. Fine PG, Marcus M, DeBoer AJ, Van der OordThis work was funded by a grant from Anesta B. An open label study of oral transmucosal fentanylCorp., Salt Lake City, Utah, USA. citrate (OTFC) for the treatment of breakthrough
The authors gratefully acknowledge the gen- cancer pain. Pain 1991;45:149–153.erous support of the staff at Anesta Corp. and 10. Simmonds MA. Oral transmucosal fentanyl ci-the dedicated nurses of Community Nursing trate produces pain relief faster than medication typ-
ically used for breakthrough pain in cancer patients.Service and VistaCare.American Society of Clinical Oncology (ASCO) An-nual Meeting, 1997.
11. Lyss AP. Long-term use of oral transmucosal fen-Referencestanyl citrate (OTFC) for breakthrough pain in can-
1. Bonica JJ. Cancer pain. In: Bonica JJ, ed. The cer patients. American Society of Clinical Oncologymanagement of pain. Philadelphia; Lea and Febiger, (ASCO) Annual Meeting, 1997.1990:400–434.
12. Coluzzi P. A titration study of oral transmucosal2. Portenoy RK, Hagen NA. Breakthrough pain: fentanyl citrate for breakthrough pain in cancer pa-
definition and management. Oncology 1989; tients. American Society of Clinical Oncology3(suppl):25–29. (ASCO) Annual Meeting, 1997.
3. Patt RB. Classification of cancer pain and cancer 13. Cleary JF. Double-blind randomized study of thepain syndromes. In: Patt RB, ed. Cancer pain. Phila- treatment of breakthrough pain in cancer patients:delphia: JB Lippincott Co., 1993:3–22. Oral transmucosal fentanyl citrate vs placebo. Ameri-
can Society of Clinical Oncology (ASCO) Annual4. Portenoy RK, Hagen NA. Breakthrough pain:definition, prevalence and characteristics. Pain 1990; Meeting, 1997.41:273–281.