Embed Size (px)
Citation preview

ORIGINAL REPORTS
Characterizing Information Decayin Patient Handoffs
Abbie M. Jensen, BA,* Chris Sanders, BS,† Jennifer Doty, BSN,‡ Dena Higbee, MS,† andArthur L. Rawlings, MD‡
*University of Missouri School of Medicine, Columbia, Missouri; †Russell D. and Mary B. Sheldon ClinicalSimulation Center, University of Missouri Hospitals and Clinics, Columbia, Missouri; and ‡Department ofSurgery, University of Missouri Hospitals and Clinics, Columbia, Missouri
OBJECTIVE: The purpose of this study was to analyze thedecay of information with multiple sequential patienthandoff reports given by third-year medical students whohave not had standardized patient handoff training.
METHODS: We examine the information decay of quanti-tative parameters included in 2 different simulated patienthistory and physical handoffs conducted among third-yearmedical students. Both student self-surveys and third partyobserver surveys tracked accuracy of information. A total of93 students were surveyed for the first patient scenario and103 students were surveyed for second patient scenario.Survey data were aggregated into 2 separate spreadsheets,one for each patient scenario tested. A total of 16 datapoints pertaining to the checklist were analyzed for commontrends in handoff accuracy and information decay.
RESULTS: Quantitative analysis of information passedbetween handoffs showed that between the 2 case scenarios,there was a consistent loss of information between onepresenter to the next. Overall, 33% of information was lostbetween the first and third handoffs. Within the progressionof individual handoffs, a narrative decay was demonstrated.There was a regression in handoff accuracy, trending downto an average of only 45% of information being passed onsuccessfully by the time each presenter reached the last pieceof information in their patient presentation. When examin-ing the survey data points that had greater than an 80%success rate of being included in the handoffs, thereappeared to be no correlation between their inherentqualities.
CONCLUSIONS: This study showed there is a significantdecrease in accuracy of information during sequentialpatient handoff exercises. The information decay may be aresult of time, memory, or relevance of the information to
Correspondence: Inquiries to Abbie May Jensen, BA, University of Missouri School ofMedicine, 603 Bear Valley Court, Columbia, MO 65202; e-mail: [email protected], [email protected]
Journal of Surgical Education � & 2014 Association of Program DiElsevier Inc. All rights reserved.
the student. Future studies incorporating teaching effectivehandoffs early in the clinical curriculum would be an area offuture research. ( J Surg ]:]]]-]]]. JC 2014 Association ofProgram Directors in Surgery. Published by Elsevier Inc. Allrights reserved.)
KEY WORDS: patient handoffs, information decay, med-ical student education
COMPETENCIES: Patient Care, Interpersonal and Com-munication Skills, Systems Based Practice
INTRODUCTION
Medical school is arguably the first time in an aspiringphysician’s career to learn strategies in managing patients,and more importantly, methods of communicating patientinformation efficiently and accurately to other medicalpersonnel. Reduced resident work hours confirm this notionbecause there are now more frequent changes in providerswho are switching shifts or transferring patients betweenone another. We investigated how patient information candecay in accuracy when passed among multiple providerswithout referring back to the original patient information.According to the Joint Commission’s review of 2506
sentinel events occurring between 2010 and June 30, 2012,poor communication within the medical setting and amongpractitioners is a major factor that contributes to medicalerrors.1 Even prior to this report, there was a consensualunderstanding that patient handoffs, or the transfer ofpatients care from one health care provider to another,were vulnerable to communication failures.2 More so, in2009, Riesenberg et al.3 even called patient handoffs“remarkably haphazard” and “prone to error.”Despite these findings, only 8% of U.S. medical schools
specifically teach their students how to handoff patient care ina standardized manner.4 Medical school is when aspiringphysicians begin their clinical training, yet the overwhelming
rectors in Surgery. Published by 1931-7204/$30.00http://dx.doi.org/10.1016/j.jsurg.2013.12.002
1

majority of students will begin their intern year of residencywith patient handoff skills informally learned from otherphysicians during their clinical clerkships. Sinha et al.2
reported in 2007 that 73% of residency program directorsagreed that standardized handoffs would reduce medical errors,but like medical schools, most residency programs do not havea formal policy or procedure regarding patient handoffs.5,6
It is our goal to assess patient handoff accuracy amongthird-year medical students who do not receive any formalhandoff training. This will serve as a baseline analysis forfuture studies on this topic and will likely be representativeof handoffs as they currently exist among 92% of third-yearmedical students.4 Comparison can then be made to this infuture studies of handoff accuracy in those providers whoactually do receive formal training.
METHODS
The study was conducted at the University of Missouri-Columbia School of Medicine Russell D. and Mary B.Sheldon Clinical Simulation Center. Over a period of 2years, all third-year medical students participated in asimulated patient handoff exercise at the beginning of theirsurgery clerkship.For the simulated patient handoff, 2 different general
surgery patient scenarios were written in the form of a fullhistory and physical (H&P). Patient 1 simulated a case ofacute cholecystitis, whereas patient 2 simulated a case ofappendicitis. Groups of 3 students were assigned tosequentially handoff 1 of these patients at a time fromone student to the next. The H&P for the assigned patientwas read only by the first person in each group of students.This student was allowed to read and take notes on theH&P information as needed for 7 minutes for his or herpatient presentation to the next student. Two minutes weregiven for the verbal patient handoff to take place to the nextstudent (Handoff 1), who was also allowed to take notes onthe patient being handed off to him or her. This secondstudent then relayed the information to the third and finalstudent in the group without referring back to the originalH&P (Handoff 2). This final student in the group verballypresented the information he or she had gathered back to allgroup members as a final patient checkout (Handoff 3).At the end of the handoff set, each group member was
given a checklist detailing aspects of the patient’s H&P thatwe collectively determined essential to quality patient care.There were 18 items analyzed for patient 1 and 17 items forpatient 2. Students were asked to check which of theseitems they received in the handoff, as well as whichinformation was included in the final handoff presentation.All groups of students completed this process for both casescenarios. Each handoff set was video recorded and reviewedby a standardized observer to confirm or deny the students’self-reflection.
2
After removal of incomplete survey data, 103 third-yearmedical students were surveyed for the patient 1 scenarioand 93 students were surveyed for the patient 2 scenario.Survey data were aggregated into 2 separate spreadsheets,1 for each patient scenario tested. A total of 16 data pointspertaining to the checklist were analyzed for patient1 scenario, and 15 data points were analyzed for patient2 scenario. Each data point pertained to a specific surveyquestion. The 2 data points that were not included in thefinal analysis of each scenario were the ones that were notwritten clearly enough to result in consistent interpretationby students. The discrepancy in number of data pointsbetween the 2 cases is because there was no “family history”data point for the patient 2 scenario. We then comparedcollective group accuracy of each sequential handoff basedon the number of aspects of each patient’s histories thatwere marked as included on the surveys.Three aspects of the data were considered. First, we
analyzed quantitative information decay between the 3sequential handoffs from one student to the next for eachof the 2 patients. Second, we looked at the decay inaccuracy of information within the progression of eachindividual handoff. Third, we assessed what types ofinformation were more likely to be passed on vs whichtypes were more likely to be left out of handoffs bycomparing the top one-third most likely survey questionsto be passed on with the bottom one-third.
RESULTS
Information decay of the 3 sequential handoffs was con-sistent between both patient cases. Thus, the data for the2 scenarios were aggregated into 1 data set for final analysis.A total of 16 data points were analyzed. Figure shows thefirst, second, and third handoff data, with best-fit lines foreach. The X-axis represents each survey question analyzed,numbered 1 to 16. The Y-axis represents the percentage ofstudents who passed off each piece of information point intheir handoff. Table 1 lists the survey questions thatstudents answered.Table 2 shows the survey questions in descending order
of handoff accuracy. The survey questions were shaded todivide them into top, middle, and bottom thirds of correctlyhanded off information. There were 6 survey data pointsthat had greater than an 80% handoff accuracy rate at thetime of the final handoff. These data were examined forinsight into what types of information tended to beincluded vs what types were left out of student handoffpresentations.First, we studied the quantitative accuracy of the 3
progressive handoffs in each group. An average of 74% ofinformation was correctly handed off from one student tothe next. However, the chain of handoffs in each groupshowed a progressive, consistent loss of information
Journal of Surgical Education � Volume ]/Number ] � ] 2014
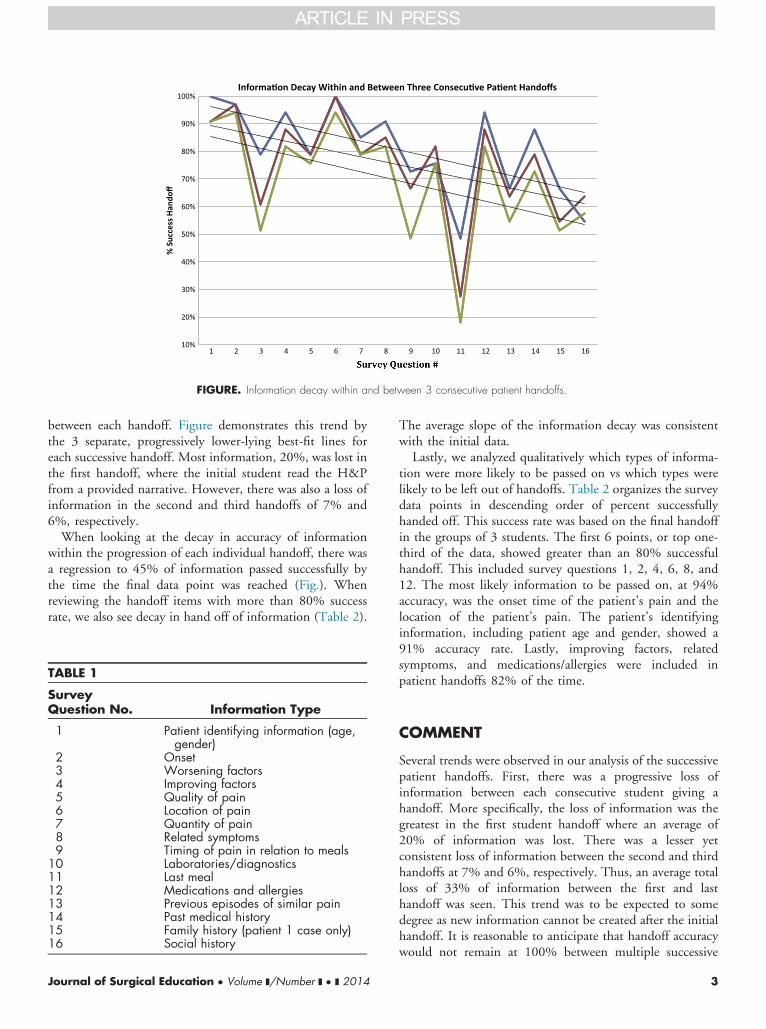
FIGURE. Information decay within and between 3 consecutive patient handoffs.
between each handoff. Figure demonstrates this trend bythe 3 separate, progressively lower-lying best-fit lines foreach successive handoff. Most information, 20%, was lost inthe first handoff, where the initial student read the H&Pfrom a provided narrative. However, there was also a loss ofinformation in the second and third handoffs of 7% and6%, respectively.When looking at the decay in accuracy of information
within the progression of each individual handoff, there wasa regression to 45% of information passed successfully bythe time the final data point was reached (Fig.). Whenreviewing the handoff items with more than 80% successrate, we also see decay in hand off of information (Table 2).
TABLE 1
SurveyQuestion No. Information Type
1 Patient identifying information (age,gender)
2 Onset3 Worsening factors4 Improving factors5 Quality of pain6 Location of pain7 Quantity of pain8 Related symptoms9 Timing of pain in relation to meals
10 Laboratories/diagnostics11 Last meal12 Medications and allergies13 Previous episodes of similar pain14 Past medical history15 Family history (patient 1 case only)16 Social history
Journal of Surgical Education � Volume ]/Number ] � ] 2014
The average slope of the information decay was consistentwith the initial data.Lastly, we analyzed qualitatively which types of informa-
tion were more likely to be passed on vs which types werelikely to be left out of handoffs. Table 2 organizes the surveydata points in descending order of percent successfullyhanded off. This success rate was based on the final handoffin the groups of 3 students. The first 6 points, or top one-third of the data, showed greater than an 80% successfulhandoff. This included survey questions 1, 2, 4, 6, 8, and12. The most likely information to be passed on, at 94%accuracy, was the onset time of the patient’s pain and thelocation of the patient’s pain. The patient’s identifyinginformation, including patient age and gender, showed a91% accuracy rate. Lastly, improving factors, relatedsymptoms, and medications/allergies were included inpatient handoffs 82% of the time.
COMMENT
Several trends were observed in our analysis of the successivepatient handoffs. First, there was a progressive loss ofinformation between each consecutive student giving ahandoff. More specifically, the loss of information was thegreatest in the first student handoff where an average of20% of information was lost. There was a lesser yetconsistent loss of information between the second and thirdhandoffs at 7% and 6%, respectively. Thus, an average totalloss of 33% of information between the first and lasthandoff was seen. This trend was to be expected to somedegree as new information cannot be created after the initialhandoff. It is reasonable to anticipate that handoff accuracywould not remain at 100% between multiple successive
3

TABLE 2. Survey Questions in Descending Order of Handoff Accuracy
Percentage Passed* Information Type Survey Question No.
94 Time of onset 294 Location of pain 691 Patient identifying information (age, gender) 182 Improving factors 482 Related symptoms 882 Medications and allergies 1279 Quantity of pain 776 Quality of pain 576 Labs diagnostics 1076 Past medical history 1455 Previous episodes of similar pain 1352 Worsening factors 348 Timing of pain in relation to meals 945 Social history 1627 Family history (patient 1 case only) 1518 Last meal 11
*Percentage is based on the final handoff accuracy.
handoffs. Extensive cognitive psychology literature hasshown that short-term memory accuracy is a decreasingfunction of the interval between presentation and reportof an item, irrespective of report strategy.6 The findingsmay also reflect the fact that short-term memory is knownto only be able to manage 7 � 2 fragments of infor-mation at any given time, and the ability to remain focusedon a task is highly influenced by potential interferencefrom distracters that are irrelevant for the task.7,8 Althoughthe extent of the information loss seen here reflectspreviously studied trends in memory, this is the first studyof its kind to look at the unique information sets anddistracters that accompany patient handoffs. We hope thatthis information will serve as a baseline for future analysis,where patient handoffs are given without any sort ofprior handoff training, strategies to overcome our innatehuman memory limitations, or tactics to avoid cognitivedistracters.The difference between the first handoff and the last 2
was that the first member of each group obtained thepatient information by reading through a patient’s H&Pwhereas the final 2 participants in each group were givenpatient information in the form of a verbal handoff. Thisfinding is supported by the hypothesis that the workingmemory is composed of separate subcomponents forprocessing visual-spatial information vs auditory informa-tion.9 It could be suggested that a summarized, verbalhandoff is more effective at keeping a consistent amount ofinformation between students than having to extract infor-mation from a written patient note. The observed trendcould also be related to the amount of information that waspresented in the initial written patient summary. It ispossible that there was a larger falloff of information passedin the first handoff because each student only communi-cated information that he or she believed was necessary forpatient care. Whether or not the method of information
4
presentation truly affects the subsequent accuracy of patienthandoffs is a subject for further investigation.The second trend observed in this study, that there was
decay in accuracy of information within the progression ofeach individual handoff, suggests that our ability to effec-tively communicate a progression of information decreasesover a fixed period. Even though our study allowedparticipants to write down information and take notes asneeded, there was a 45% decrease in accuracy by the timethe final piece of information was handed off. It was notable to be determined whether this regression trend wasowing to delay in time of report, memory, or value ofinformation to the student. It could be suggested that thereis benefit in presenting the most important information inthe first portion of patient handoffs rather than nearer tothe end.With this study we look at the types of information that
had greater than an 80% handoff for insight into whichwere most likely to be handed off. Even though in ouranalysis of handoffs we considered all information equallyimportant to patient care, there were clearly pieces ofinformation that were more likely to be passed on thanothers. When looking at these pieces of information thatwere more likely to be handed off, we hoped to find a trendthat would tell us more about how our memory functions inthe processing of handoffs. For example, quantitativeinformation that was reported in discrete measurementssuch as pain scales, patient age, time of onset, etc. could beinferred to be passed on more effectively than informationthat was more qualitative in nature. However, no trend ofthis sort was seen. As seen in Table 2, qualitative as well asquantitative information as evenly distributed throughout.Why students chose some information to handoff couldhave been a result of time, memory, or relevance of theinformation to the student. It could also have been owing tothe significance the student put on the information in the
Journal of Surgical Education � Volume ]/Number ] � ] 2014

management of that patient’s care. The elimination of someinformation and consistent maintenance of others couldpoint toward students’ cognitive ability to remain focusedon goal-relevant stimuli in the presence of potentiallyinterfering distractors.8
This is the first study of its kind to analyze patienthandoffs as they currently exist among 92% of U.S. medicalstudents. Previous reports have focused only on the need forimproved patient handoffs, the qualitative features of hand-off errors, and the subjective accuracy of handoffs amongstudents or residents who have had some sort of formal orstandardized handoff training.2,4,5,9,11,12 The extent of theinformation loss observed here, where patient handoffs weregiven without any sort of prior standardized training ormethods to overcome inherent short-term memory limita-tions or cognitive overload, can now serve as a baseline forfuture, similar studies.There is an inherent limitation in attempting to trans-
late the qualities of a narrative into discrete pieces ofinformation. Future studies of this kind should focus oncreating information fragments that are precise and that donot allow for a significant amount of variation in interpre-tation. Each data point studied should only contain a fixed,definite amount of information that is required to beincluded in the handoff to consider it successfully handedoff from one student to the next. Also, this study onlylooked at the “handoffs” of 2 surgical patients, which weremore a model of clinical or emergency department historytaking for initial entry into care than the conveyance ofcritical patient information between residents or other careproviders between shifts. Thus, we plan to modify the“handoff” to a more traditional model in future studies tomore closely mimic the current understanding withinhandoff research.Future studies should compare the accuracy of patient
handoffs between those who have been trained to give astandardized handoff to those with no training. It has beensuggested that reducing the mental effort in the processingof task-irrelevant information results in more effectiveinformation processing.10 Accordingly, standardizing ahandoff has been suggested to optimize intellectual perform-ance and improve handoff accuracy.13 It would also bebeneficial to compare how interventions that reduce thenumber of handoffs for a given patient improve accuracy ofhandoffs and ultimately reduce negative outcomes in patientcare. Other possible future research could look at howdesigning handoffs so that the most important patientinformation is always given at the beginning of thepresentation effects accuracy. Lastly, focus could be placedon looking at how accuracy of information retention isaffected by handoffs in verbal vs written formats, howdifferent qualities of pieces of information effect theirtendency to be handed off, and hopefully provide insightinto why some pieces of information are consistently missedwhile others are not.
Journal of Surgical Education � Volume ]/Number ] � ] 2014
CONCLUSION
There is a significant decrease in accuracy of informationduring sequential patient handoff exercises both withinindividual and between successive handoffs. It is unclearwhether this information decay is a result of time, memory,or relevance of the information to the student.Despite all of the questions that this study has generated,
patient handoffs are a known, but all too often ignored,source of mistakes in the patient care setting. Accuratepatient handoffs are essential to safe and effective patientcare. More effort must be put forward into where mistakesoccur in patient handoffs, how decreasing the number ofhandoffs for a given patient improves handoff accuracy, andhow creating educational goals to standardize patient hand-offs affects their accuracy.
REFERENCES
1. Joint Commission Sentinel Event Statistics as of June30, 2012. Available at: ⟨http://www.jointcommission.org/assets/1/18/Root_Causes_Event_Type_2004_2Q2012.pdf/⟩.
2. Sinha M, Shriki J, Salness R, Blackburn PA. Need forstandardized sign-out in the emergency department: asurvey of emergency medicine residency and pediatricemergency medicine fellowship program directors.Acad Emerg Med. 2007;14:192-196.
3. Riesenberg LA, Leitzsch J, Massucci JL, et al. Residents’and attending physicians’ handoffs: a systematic reviewof the literature. Acad Med. 2009;84:1775-1787.
4. Solet DJ, Norvell JM, Rutan GH, et al. Lost intranslation: challenges-to physician communication dur-ing patient handoffs. Acad Med. 2005;80:1094-1099.
5. Arora V, Johnson J, Lovinger D, et al. Communica-tion failures in patient sign-out and suggestions forimprovement: a critical incident analysis. Qual SafHealth Care. 2005;14:401-407.
6. Wingfield A, Byrnes DL. Decay of information inshort-term memory. Science. 1972;176(4035):690-692.
7. Miller GA. The magic number seven plus or minustwo: some limits on our capacity to process informa-tion. Psychol Rev. 1956;63(2):81-97.
8. Horwitz LI, Krumholz HM, Green ML, et al. Trans-fers of patient care between house staff on internalmedicine wards: a national survey. Arch Intern Med.2006;166:1173-1177.
9. Kavic MS. Cognitive load theory and learning medi-cine. Photomed Laser Surg. 2013;31(8):1-3.
5
10. Lavi N. Distracted and confused?: selective attentionunder load. Trends Cogn Sci. 2005;9(2):75-82.
11. Donchin Y, Gopher D, Olin M, et al. A look into thenature and causes of human errors in the intensive careunit. Qual Saf Health Care. 2003;12:143-148.
12. Rabøl LI, Andersen ML, Østergaard D, Bjørn B,Lilja T, Mogensen T. Descriptions of verbal
6
communication errors between staff. An analysis of84 root cause analysis-reports from Danish hospitals.BMJ Qual Saf. 2011;20(3):268-274.
13. Sweller J, Van Merreienboer JJG, Paas FG. Cognitivearchitecture and instructional design. Educ Psychol Rev.1998;10(3):251-296.
Journal of Surgical Education � Volume ]/Number ] � ] 2014





























