Embed Size (px)
Citation preview
Chest imaging II. Interstitial lung diseases
Dávid L. Tárnoki MD, PhD
Ádám D. TárnokiMD, PhD
Department of Radiology
Semmelweis University
Topics
1. Interstitial lung diseases 2. Occupational lung diseases 3. Pleura
2
Interstitial lung diseases
3
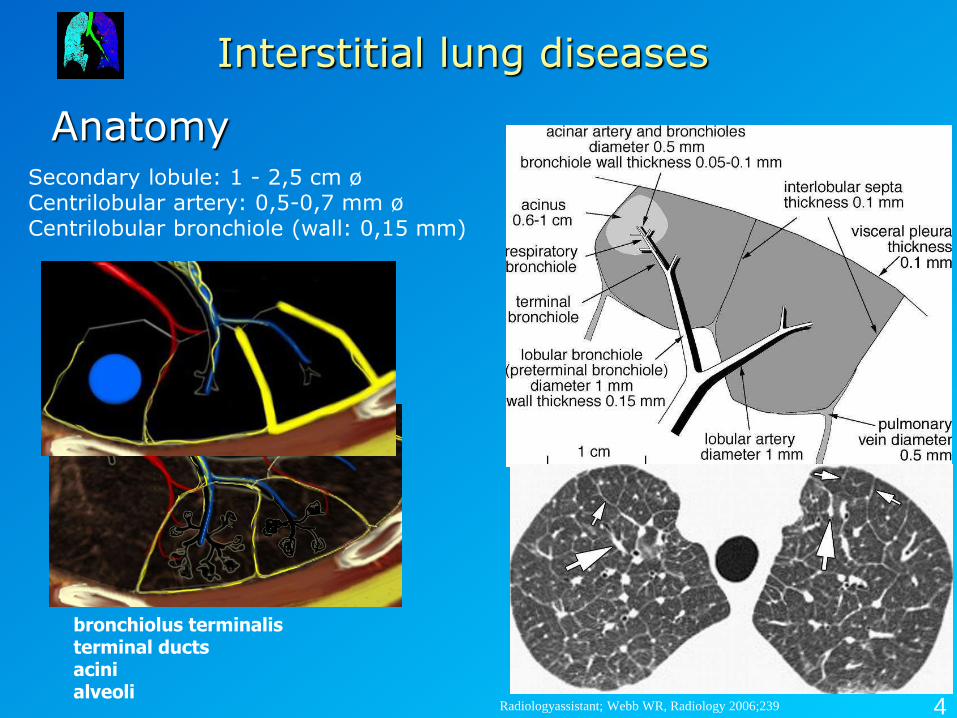
Anatomy
Interstitial lung diseases
Radiologyassistant; Webb WR, Radiology 2006;239
Secondary lobule: 1 - 2,5 cm ø Centrilobular artery: 0,5-0,7 mm ø Centrilobular bronchiole (wall: 0,15 mm)
bronchiolus terminalis terminal ducts acini alveoli
4
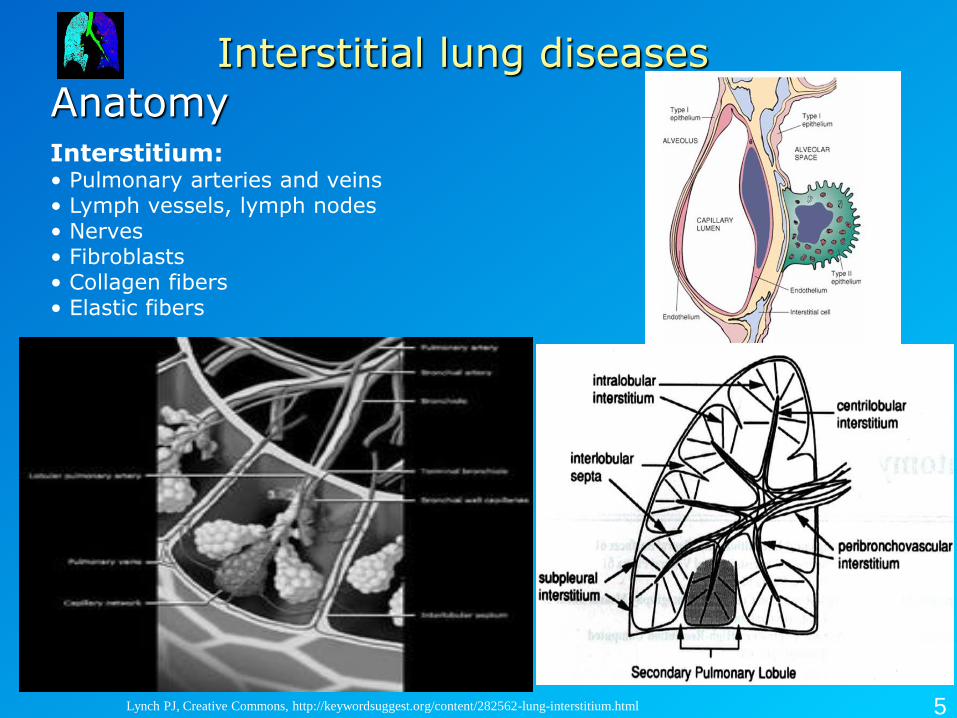
Anatomy
Interstitial lung diseases
Lynch PJ, Creative Commons, http://keywordsuggest.org/content/282562-lung-interstitium.html
Interstitium: • Pulmonary arteries and veins • Lymph vessels, lymph nodes • Nerves • Fibroblasts • Collagen fibers • Elastic fibers
5
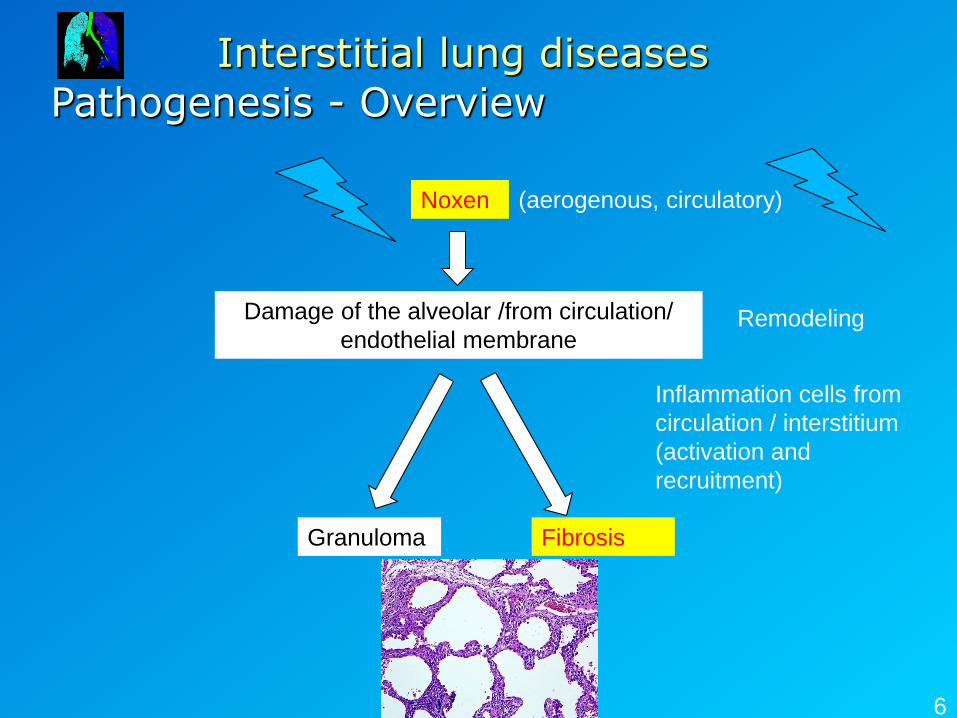
Pathogenesis - Overview
Interstitial lung diseases
6
(aerogenous, circulatory) Noxen
Damage of the alveolar /from circulation/
endothelial membrane
Granuloma
Remodeling
Fibrosis
Inflammation cells from
circulation / interstitium
(activation and
recruitment)
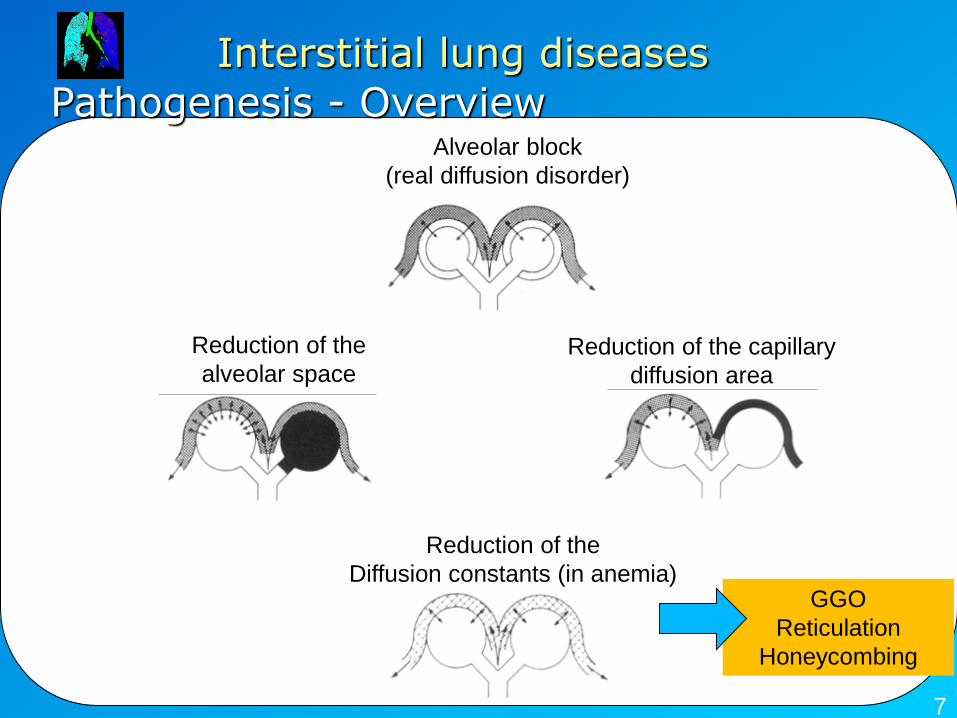
Pathogenesis - Overview
Interstitial lung diseases
7
Reduction of the
Diffusion constants (in anemia)
Alveolar block
(real diffusion disorder)
Reduction of the capillary
diffusion area
Reduction of the
alveolar space
GGO
Reticulation
Honeycombing
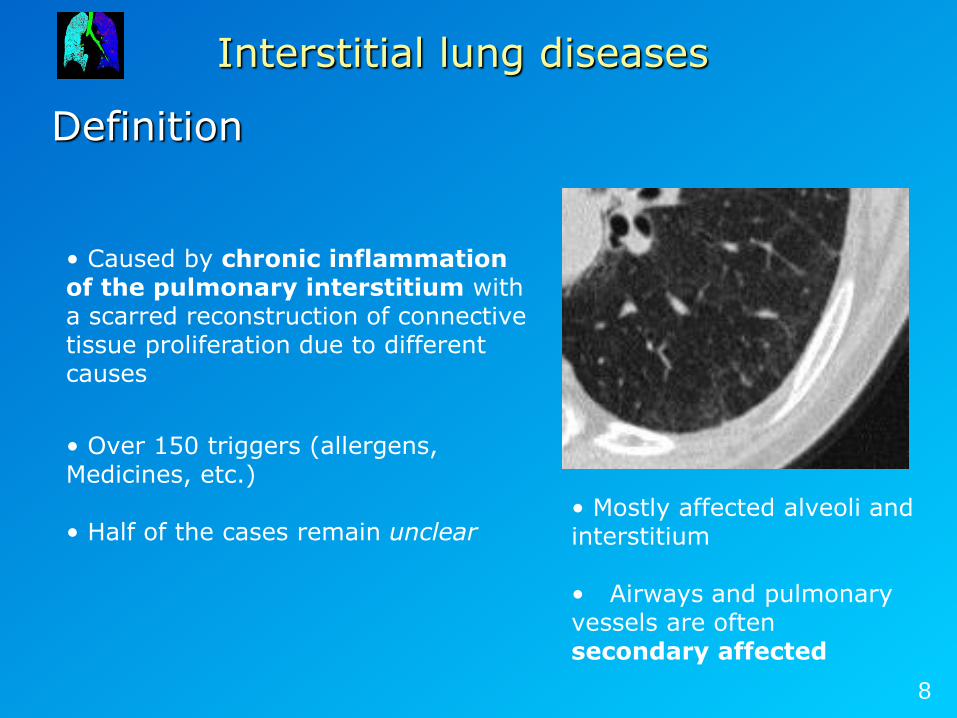
Definition
Interstitial lung diseases
• Caused by chronic inflammation of the pulmonary interstitium with a scarred reconstruction of connective tissue proliferation due to different causes
• Over 150 triggers (allergens, Medicines, etc.) • Half of the cases remain unclear
• Mostly affected alveoli and interstitium
• Airways and pulmonary vessels are often secondary affected
8
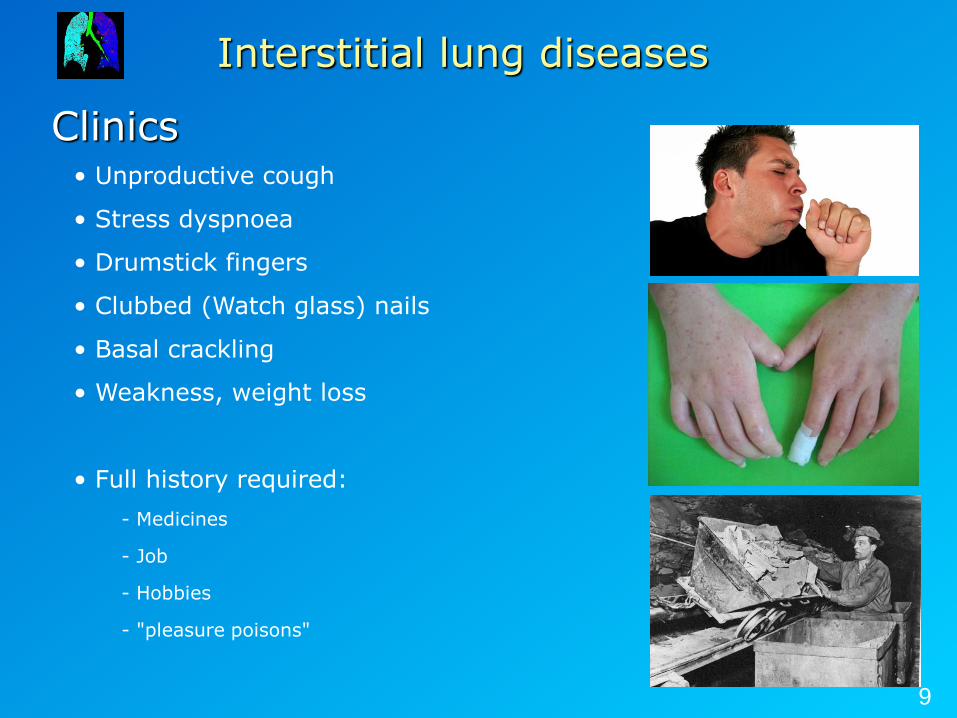
Clinics
Interstitial lung diseases
• Unproductive cough
• Stress dyspnoea
• Drumstick fingers
• Clubbed (Watch glass) nails
• Basal crackling
• Weakness, weight loss
• Full history required:
- Medicines
- Job
- Hobbies
- "pleasure poisons"
9
Diagnostics
Interstitial lung diseases
Ideally by multidisciplinary ILD board: pneumologists, rheumatologists, radiologists and pathologists • Laboratory: - Kidney functions, electrolytes, CRP - Differential blood counts - Antibodies • Lung function (Restrictive ventilation fault) • Imaging (Rö and HRCT) • Bronchoscopy with transbronchial biopsy (TBB) and bronchoalveolar lavage (BAL) • Open lung biopsy (VATS)
10
Clinics
Interstitial lung diseases
What kind of information the clinician needs from us? – Diagnosis
• UIP (Usual interstitial pneumonia) → biopsy is not necessary • Other DD? → biopsy is necessary
– Prognosis • acute / cronic • Comparison with previuos HRCT: progression / regression?
Therapeutic options - Steroids - Lung transplantation
Prognosis - Median survival after diagnosis 2.5-3.5 years
11
Typical patterns of an ILD
Ground glass opacity, consolidation
Interstitial lung diseases
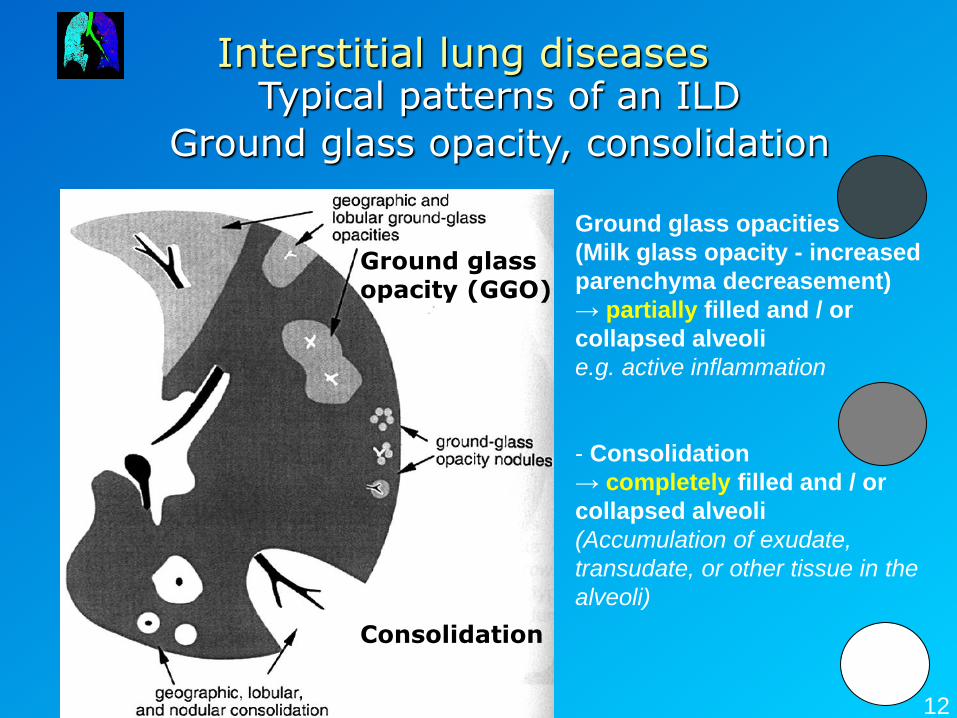
Ground glass opacities
(Milk glass opacity - increased
parenchyma decreasement)
→ partially filled and / or
collapsed alveoli
e.g. active inflammation
- Consolidation
→ completely filled and / or
collapsed alveoli
(Accumulation of exudate,
transudate, or other tissue in the
alveoli)
12
Ground glass opacity (GGO) Consolidation
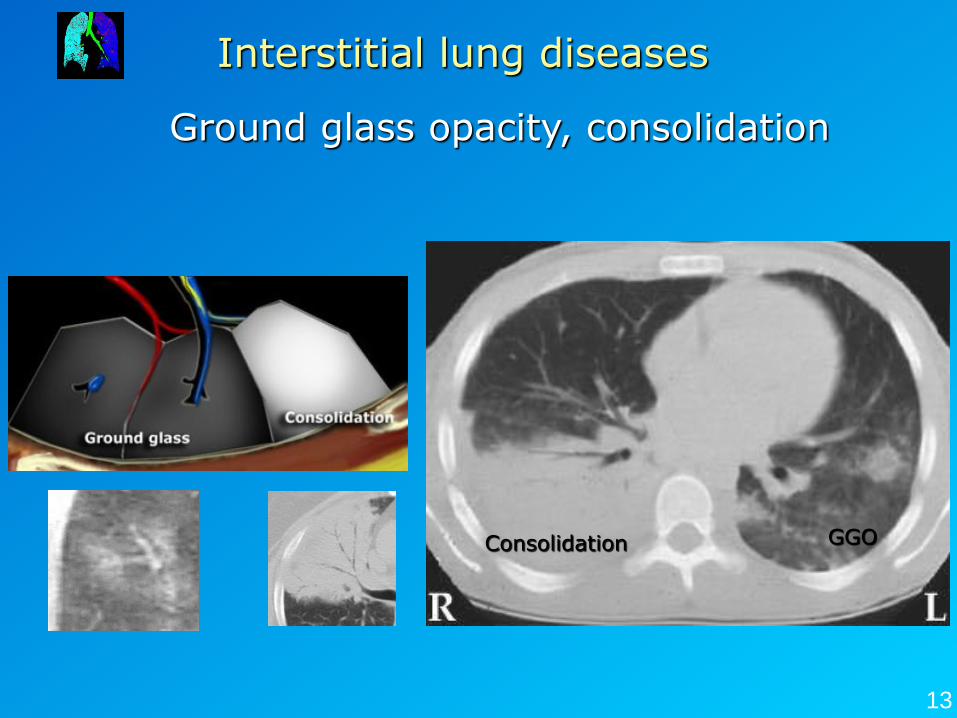
Ground glass opacity, consolidation
Interstitial lung diseases
13
Consolidation GGO
Idiopathic pulmonary fibrosis (heterogeneous entity)
Interstitial lung diseases
• AIP (acute interstitial pneumonitis)
• UIP (usual interstitial pneumonitis) 70%
• DIP (desquamative interstitial pneumonia)
• RBILD (respiratory bronchiolitis ILD)
• NSIP (non specific interstial pneumonia)
• BOOP=COP (bronchiolitis obliterans organizing pneumonia = cryptogenic organizing pneumonia)
Why do we need to subtype the idiopathic interstitial Pneumonias? Different prognosis which results different therapeutic approaches
14
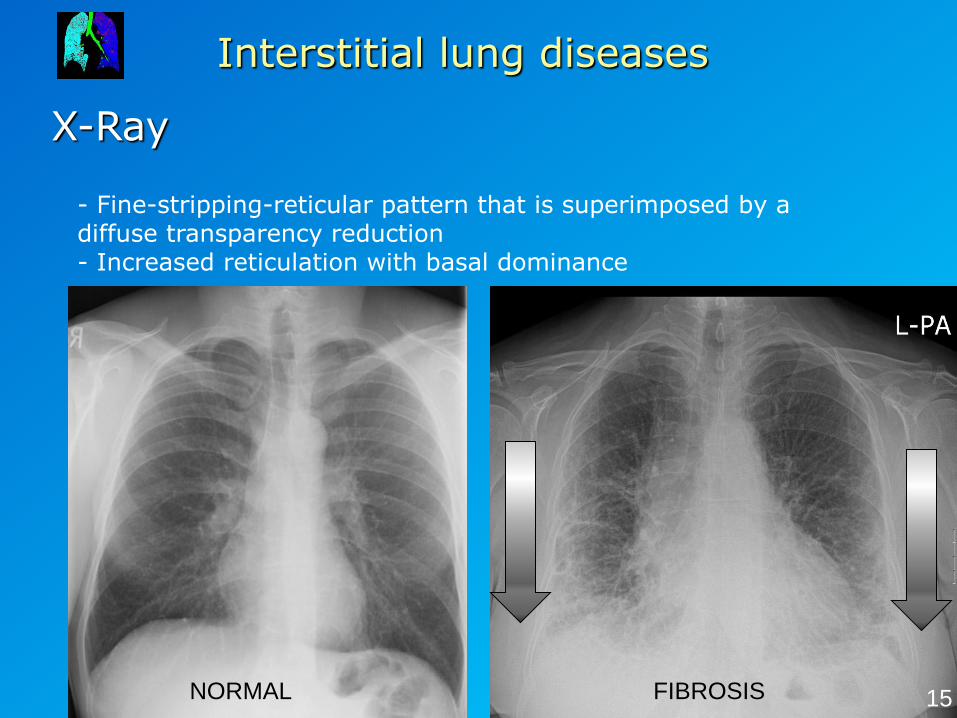
X-Ray
Interstitial lung diseases
- Fine-stripping-reticular pattern that is superimposed by a diffuse transparency reduction - Increased reticulation with basal dominance
NORMAL FIBROSIS 15
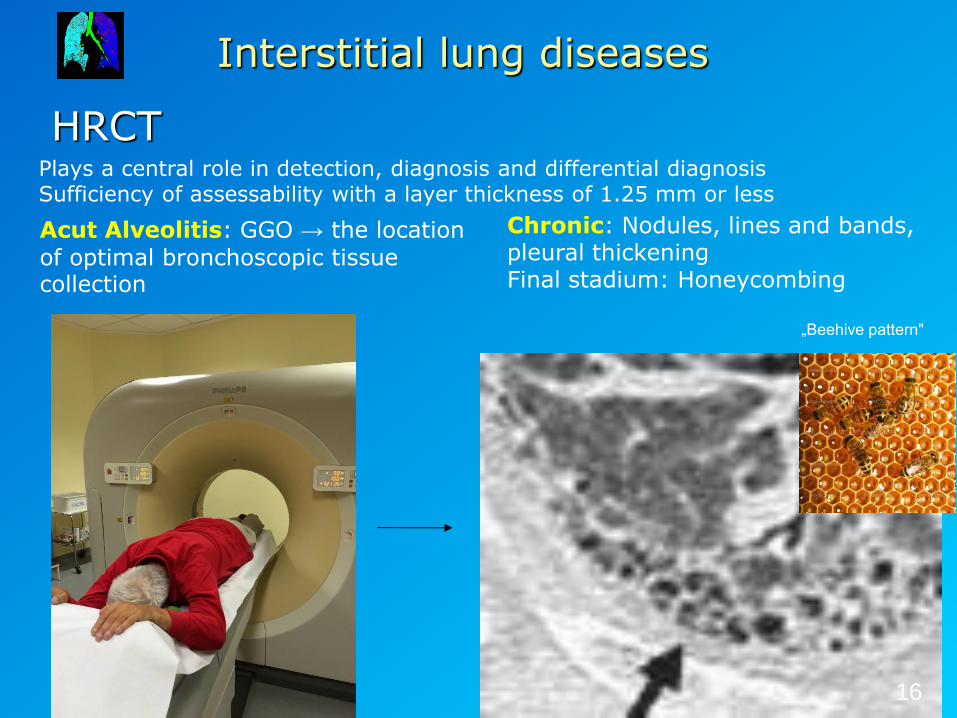
HRCT
Interstitial lung diseases
Acut Alveolitis: GGO → the location
of optimal bronchoscopic tissue collection
Chronic: Nodules, lines and bands, pleural thickening Final stadium: Honeycombing
„Beehive pattern"
16
Plays a central role in detection, diagnosis and differential diagnosis Sufficiency of assessability with a layer thickness of 1.25 mm or less
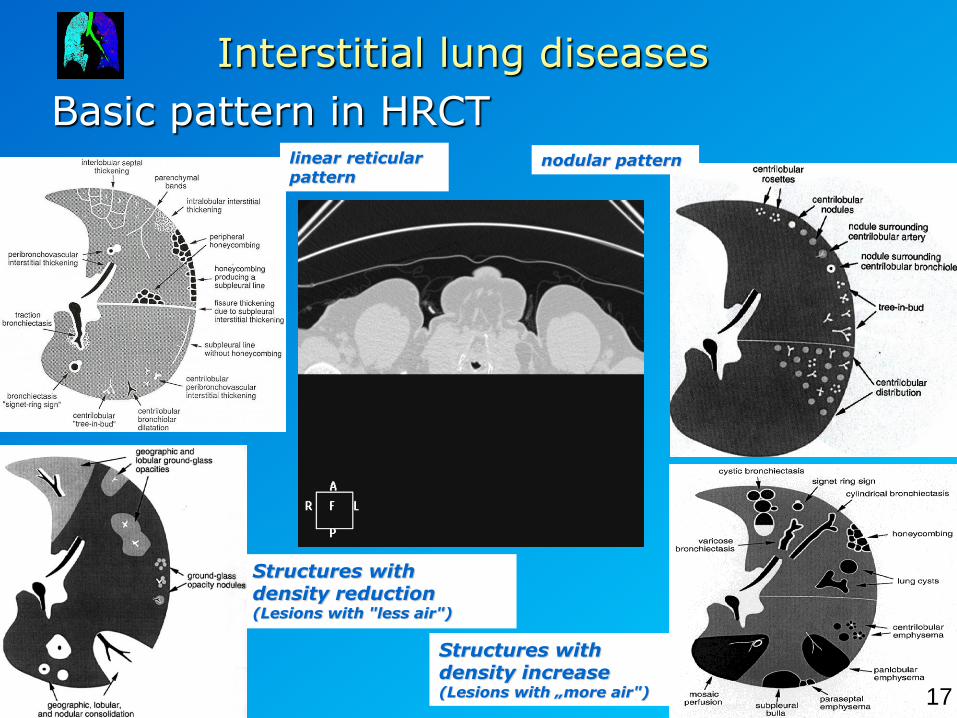
Basic pattern in HRCT
Interstitial lung diseases
linear reticular pattern
nodular pattern
Structures with density increase (Lesions with „more air")
Structures with density reduction (Lesions with "less air")
17
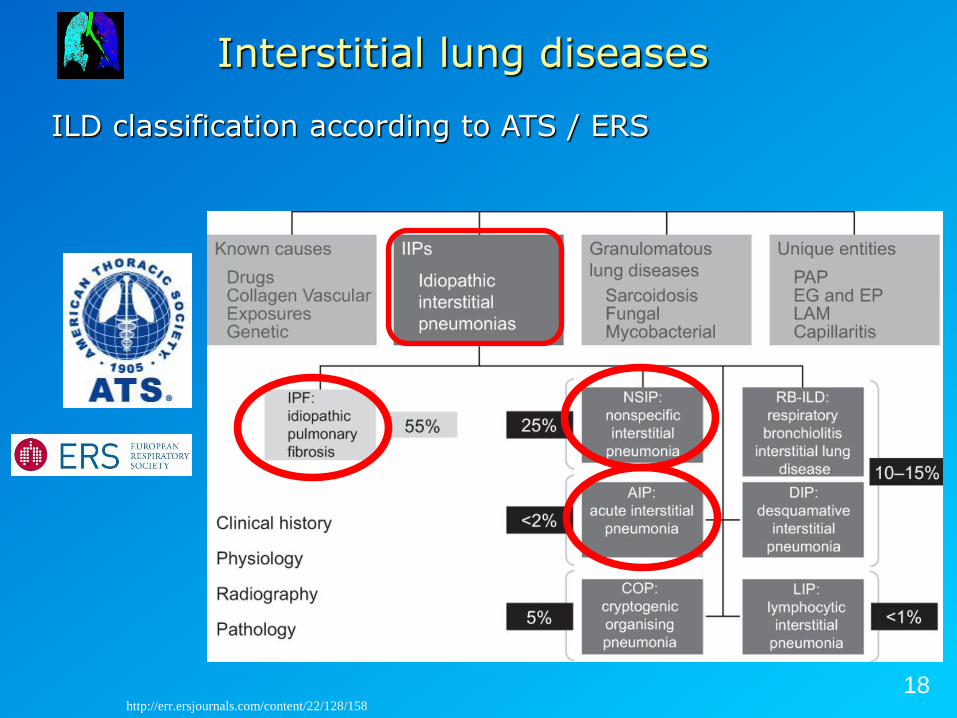
ILD classification according to ATS / ERS
Interstitial lung diseases
18 http://err.ersjournals.com/content/22/128/158
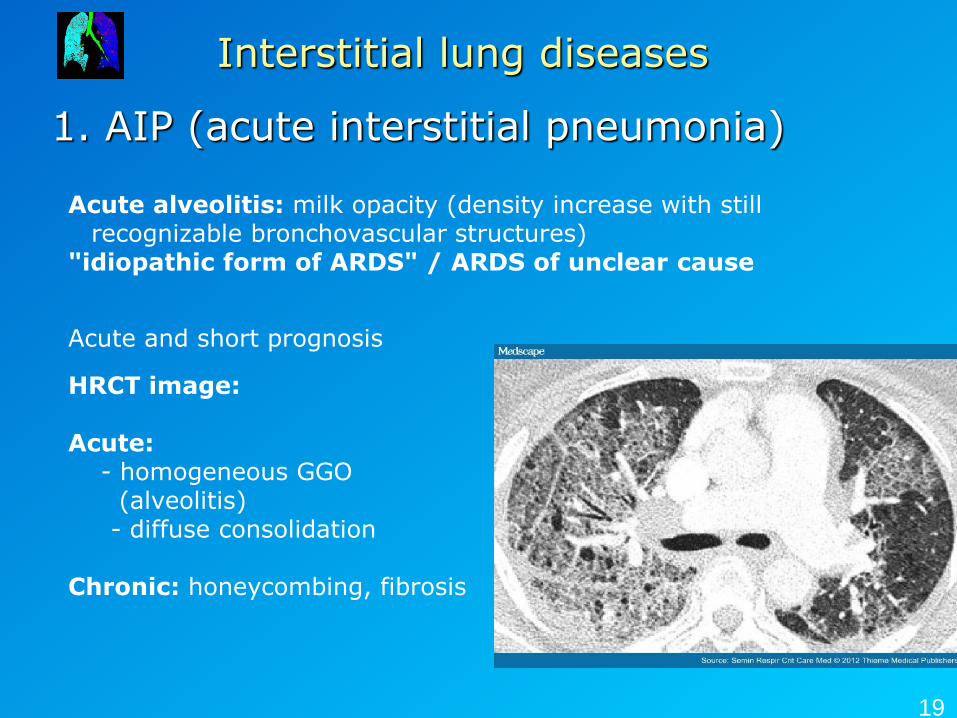
1. AIP (acute interstitial pneumonia)
Interstitial lung diseases
Acute alveolitis: milk opacity (density increase with still recognizable bronchovascular structures)
"idiopathic form of ARDS" / ARDS of unclear cause
Acute and short prognosis
HRCT image: Acute: - homogeneous GGO (alveolitis) - diffuse consolidation Chronic: honeycombing, fibrosis
19
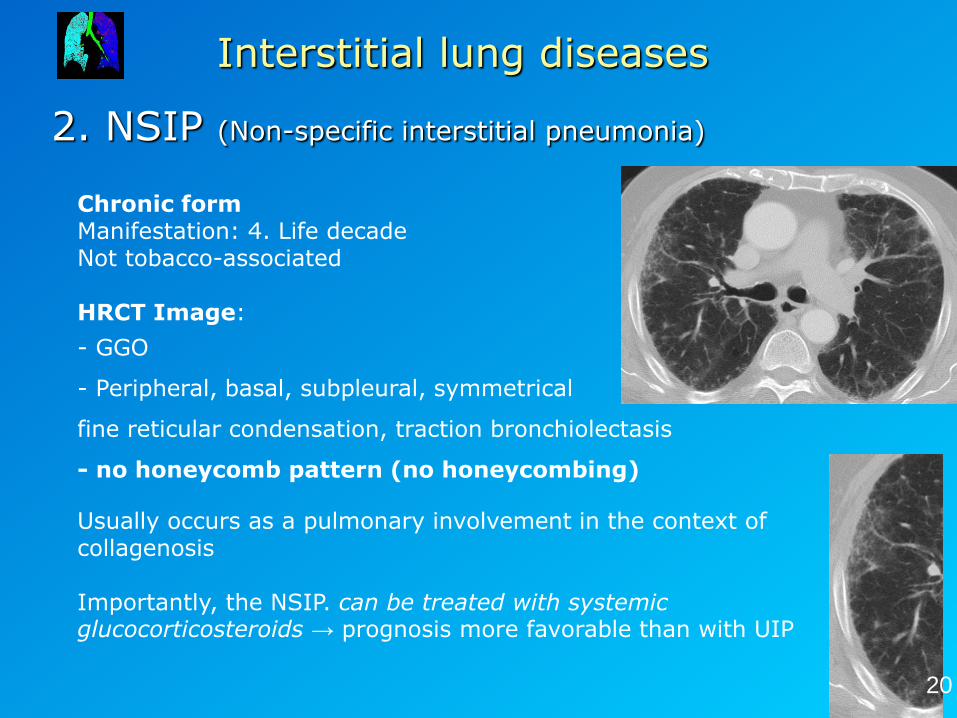
2. NSIP (Non-specific interstitial pneumonia)
Interstitial lung diseases
Chronic form Manifestation: 4. Life decade Not tobacco-associated HRCT Image:
- GGO
- Peripheral, basal, subpleural, symmetrical
fine reticular condensation, traction bronchiolectasis
- no honeycomb pattern (no honeycombing)
Usually occurs as a pulmonary involvement in the context of collagenosis Importantly, the NSIP. can be treated with systemic glucocorticosteroids → prognosis more favorable than with UIP
20
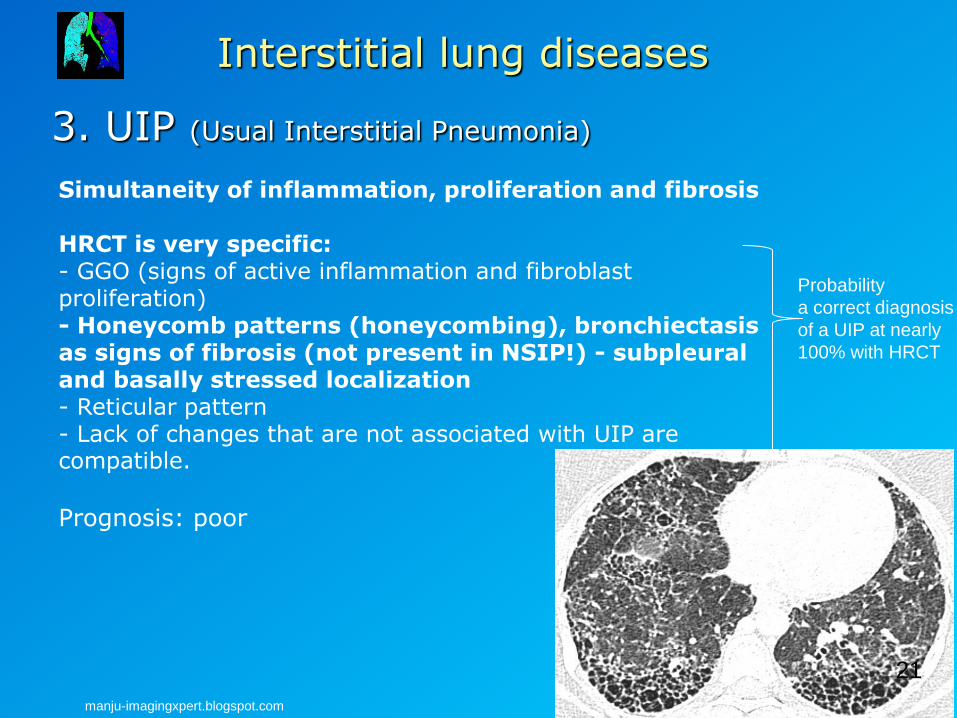
3. UIP (Usual Interstitial Pneumonia)
Interstitial lung diseases
Simultaneity of inflammation, proliferation and fibrosis HRCT is very specific: - GGO (signs of active inflammation and fibroblast proliferation) - Honeycomb patterns (honeycombing), bronchiectasis as signs of fibrosis (not present in NSIP!) - subpleural and basally stressed localization - Reticular pattern - Lack of changes that are not associated with UIP are compatible.
Prognosis: poor
manju-imagingxpert.blogspot.com
21
Probability
a correct diagnosis
of a UIP at nearly
100% with HRCT
(http://www.szote.u-szeged.hu/radio/mellk1/mellk7a.htm)
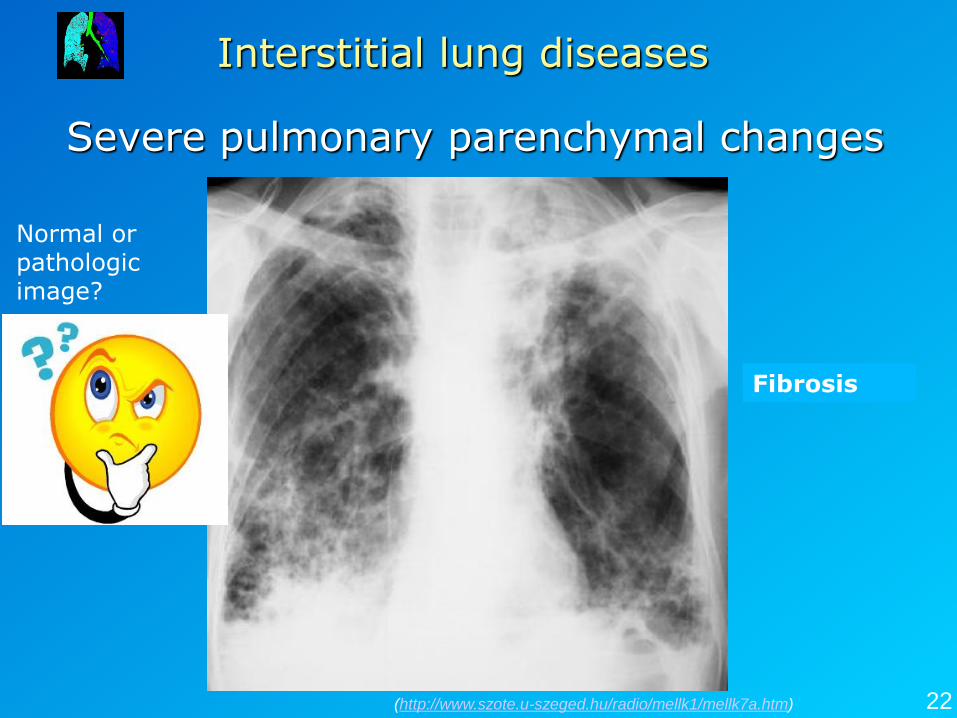
Severe pulmonary parenchymal changes
Interstitial lung diseases
22
Normal or pathologic image?
Fibrosis
Interstitial lung diseases
23
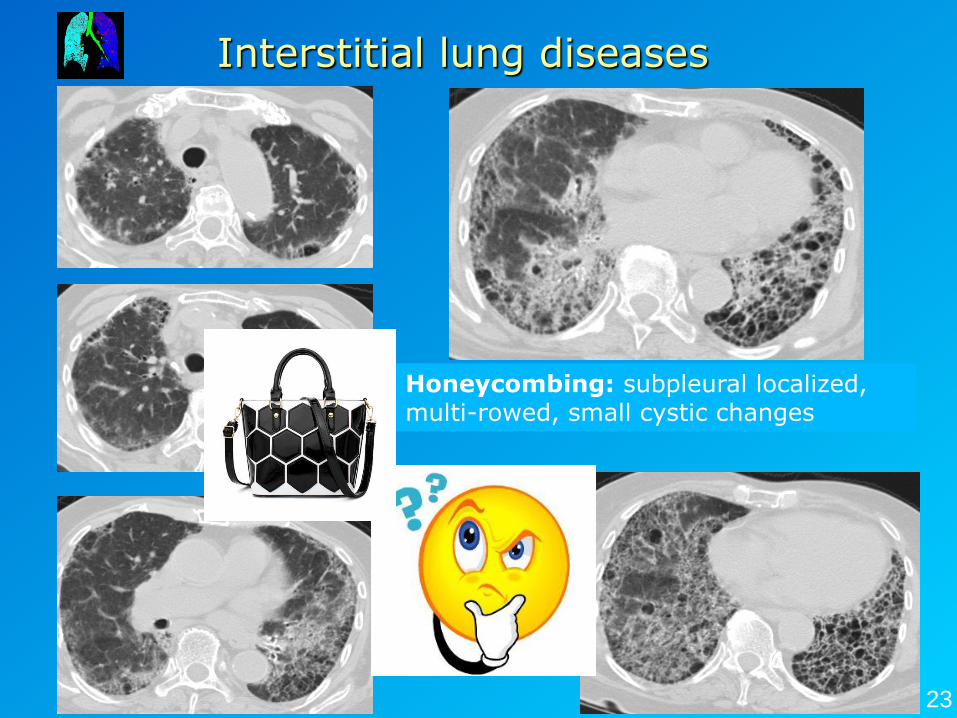
Honeycombing: subpleural localized, multi-rowed, small cystic changes
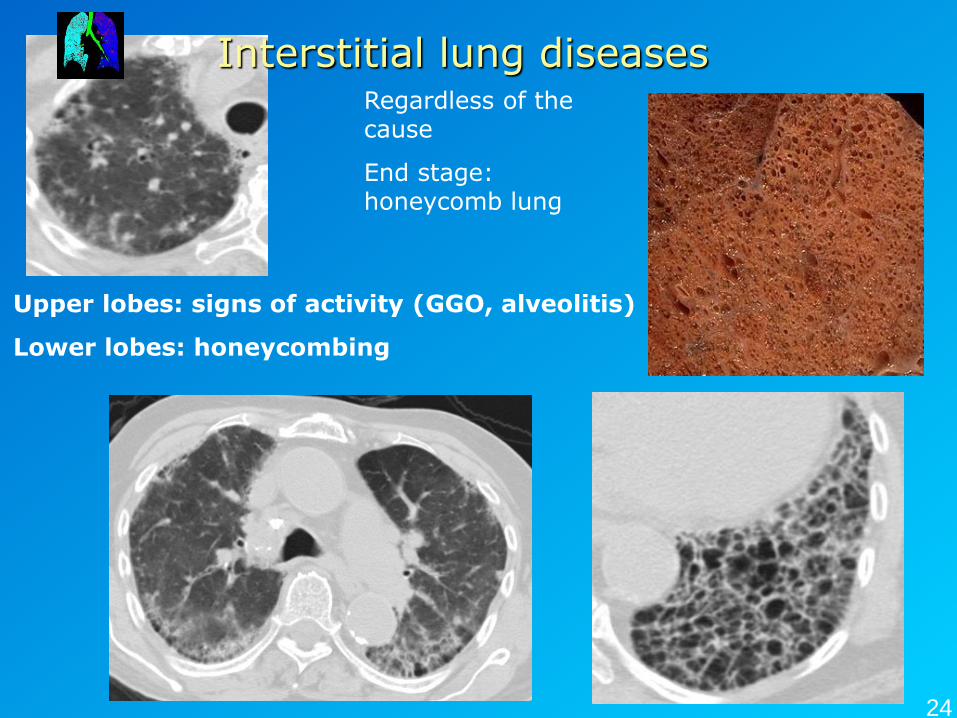
Upper lobes: signs of activity (GGO, alveolitis)
Lower lobes: honeycombing
Regardless of the cause
End stage: honeycomb lung
Interstitial lung diseases
24
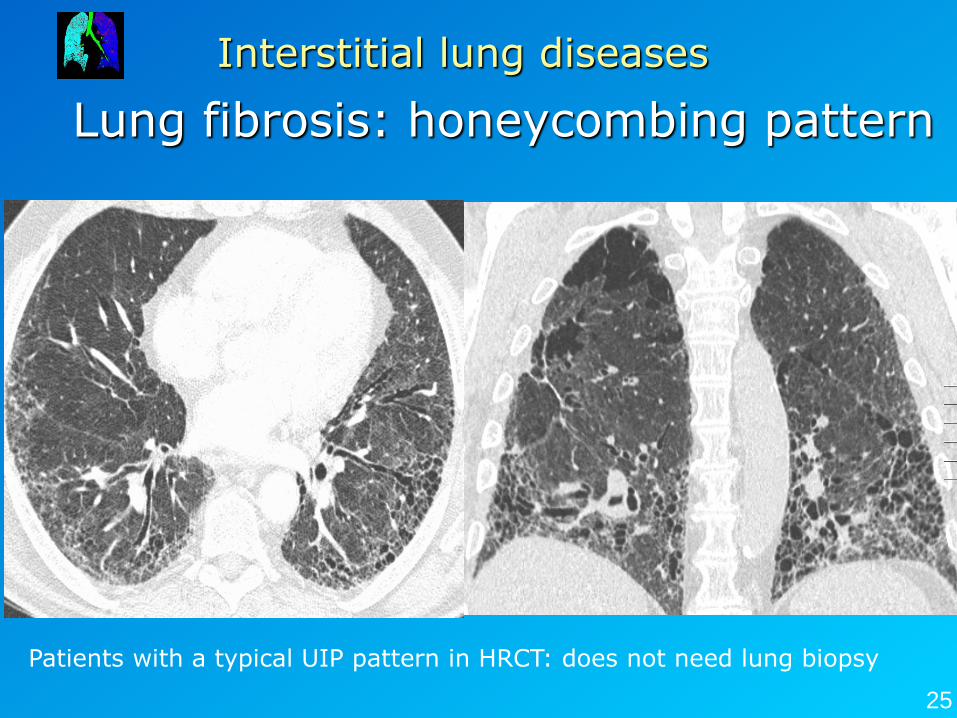
Lung fibrosis: honeycombing pattern
Interstitial lung diseases
25
Patients with a typical UIP pattern in HRCT: does not need lung biopsy
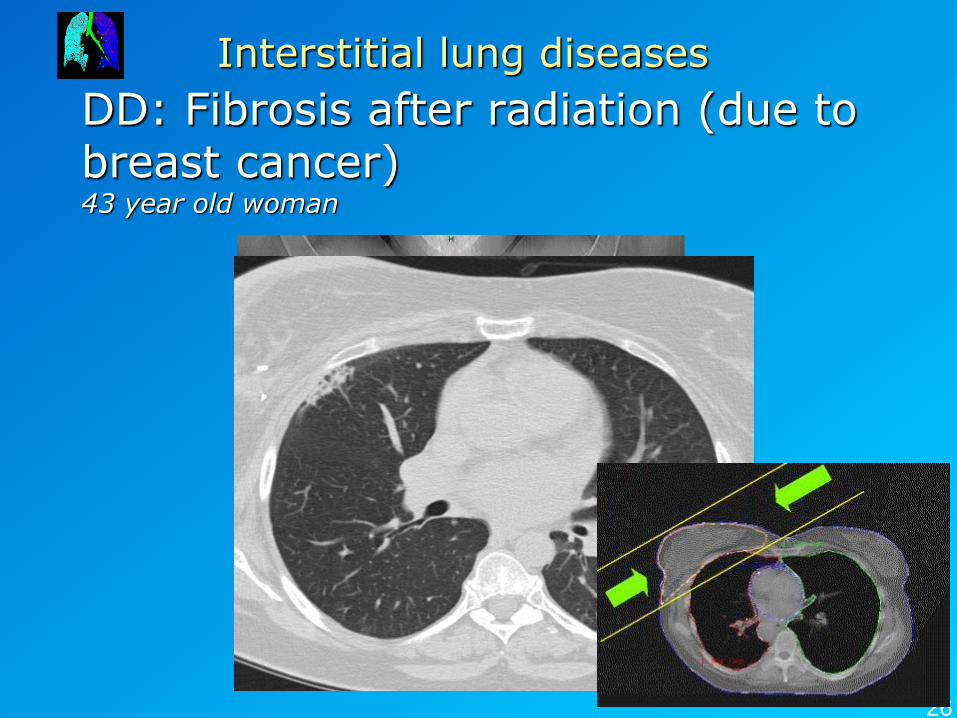
DD: Fibrosis after radiation (due to breast cancer) 43 year old woman
Interstitial lung diseases
26
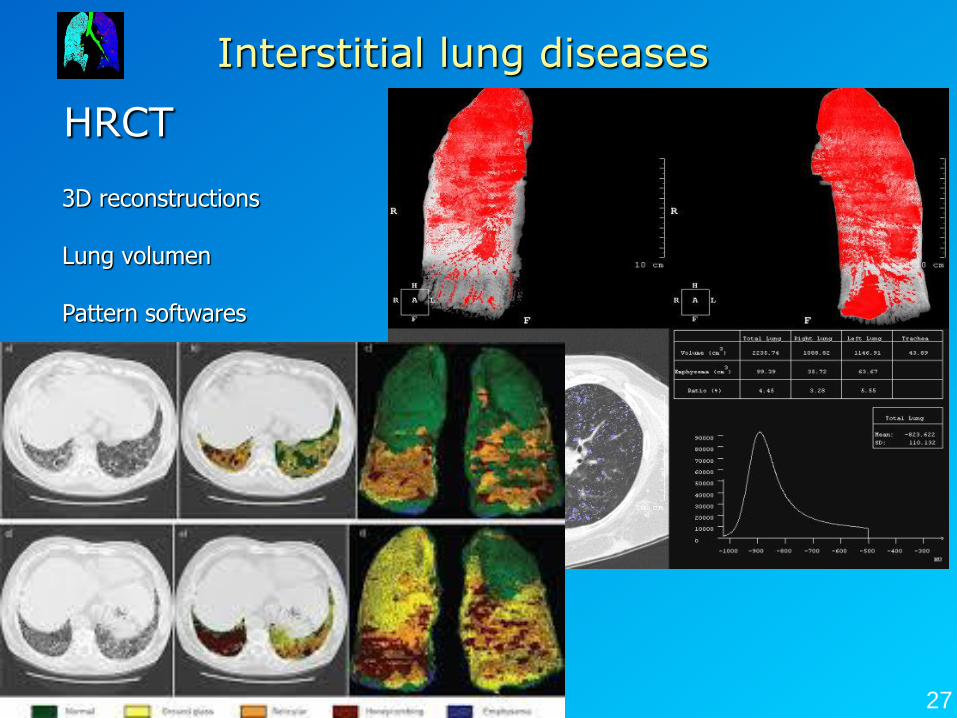
HRCT
3D reconstructions Lung volumen Pattern softwares
Interstitial lung diseases
27
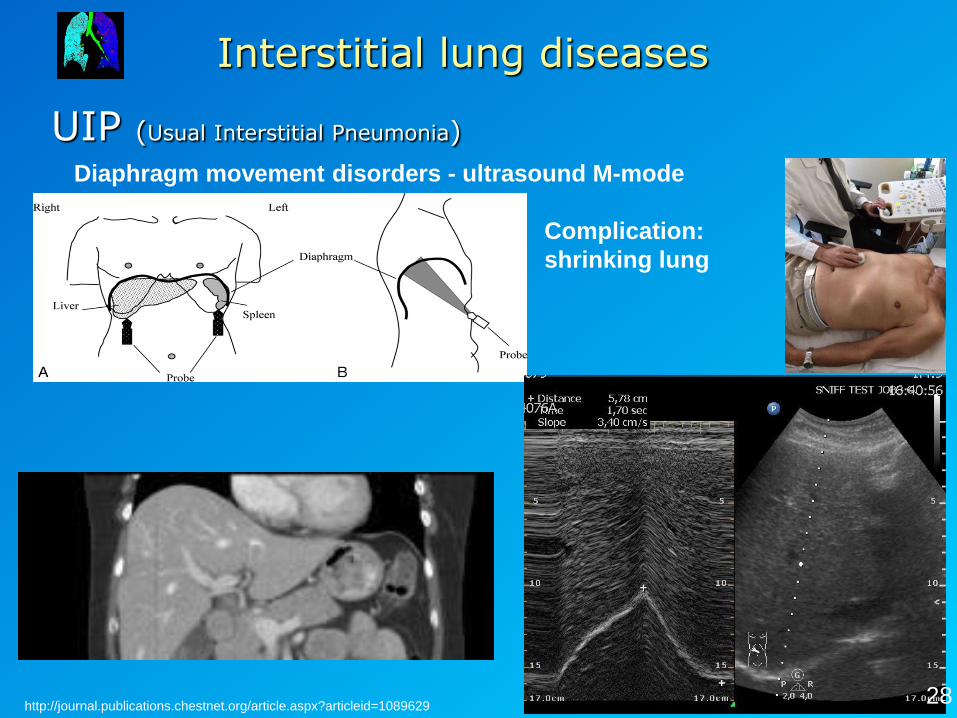
UIP (Usual Interstitial Pneumonia)
Interstitial lung diseases
Diaphragm movement disorders - ultrasound M-mode
Complication:
shrinking lung
http://journal.publications.chestnet.org/article.aspx?articleid=1089629 28
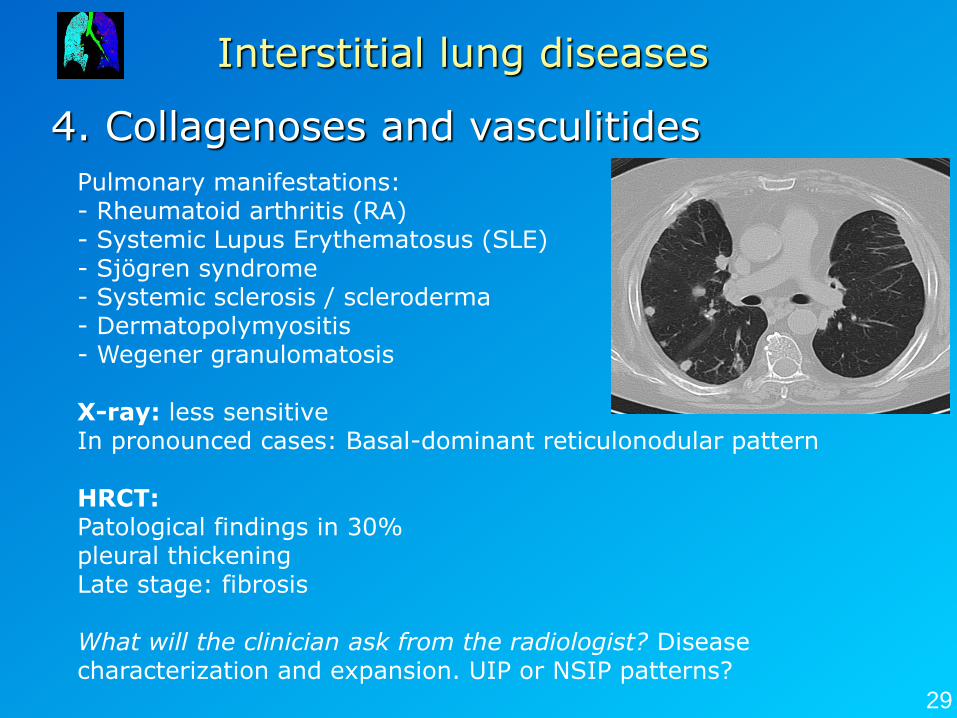
4. Collagenoses and vasculitides
Interstitial lung diseases
Pulmonary manifestations: - Rheumatoid arthritis (RA) - Systemic Lupus Erythematosus (SLE) - Sjögren syndrome - Systemic sclerosis / scleroderma - Dermatopolymyositis - Wegener granulomatosis X-ray: less sensitive In pronounced cases: Basal-dominant reticulonodular pattern HRCT: Patological findings in 30% pleural thickening Late stage: fibrosis What will the clinician ask from the radiologist? Disease characterization and expansion. UIP or NSIP patterns?
29

Occupational lung diseases
30
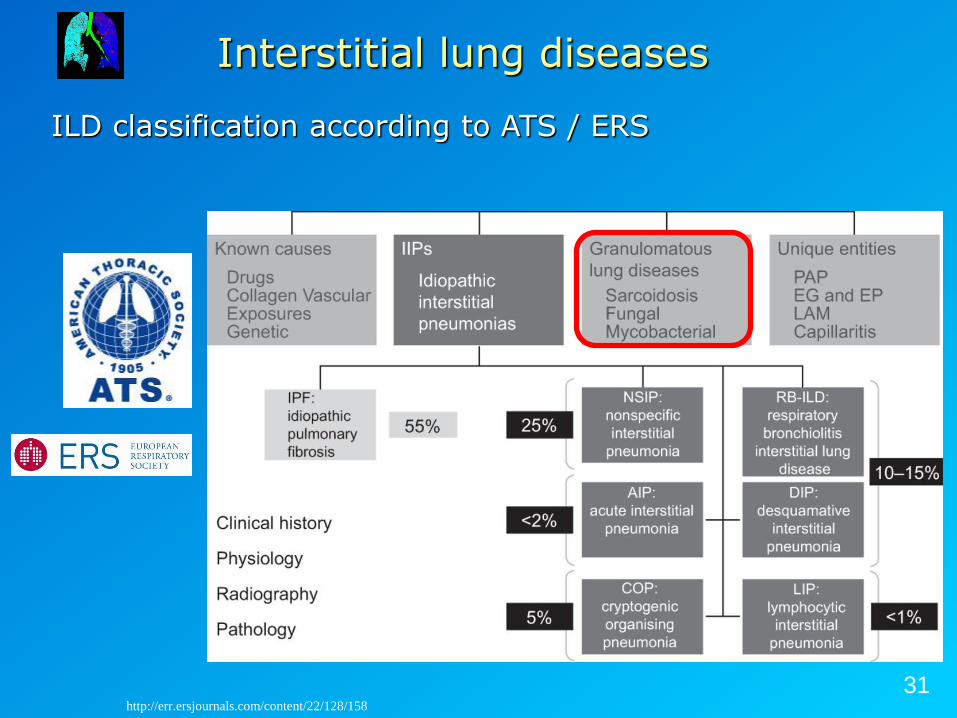
ILD classification according to ATS / ERS
Interstitial lung diseases
31 http://err.ersjournals.com/content/22/128/158
Occupational lung diseases
• New diseases due to occupational regulations • Chronic inhalation of inorganic dusts (e.g., silicate) • Long-time exposure (e.g., mineral workers) • Alveolar phagocytosis of inhaled particles and interstitial deposition
→ Interstitial reticulo-granuloma formation, sometimes massive
fibrosis • Therapy: Exposure stop
I. DISEASES OF IMMUNOLOGICAL / UNCLEAR AETIOLOGY II. PNEUMOCONIOSIS (Inhaled Particles)
• X-Ray:
• Nodular herd often with calcifications • Hilary / mediastinal lymph nodes with calcifications ("laryngeal calcification")
HRCT: • X-ray patterns + • Micronodular lesions • pulmonary fibrosis 32
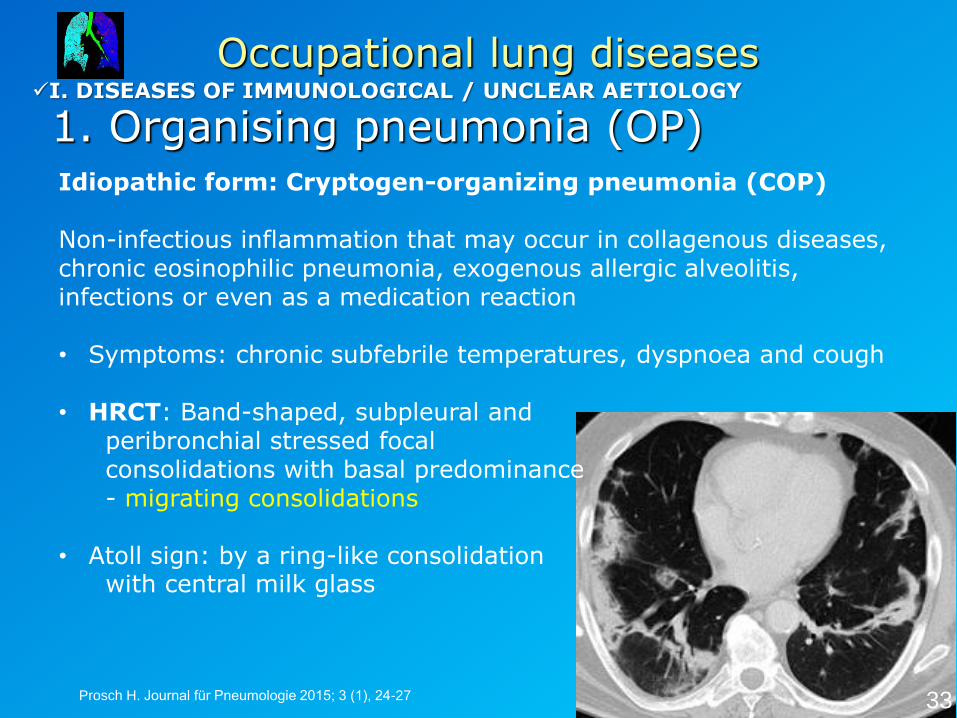
1. Organising pneumonia (OP)
Occupational lung diseases
Idiopathic form: Cryptogen-organizing pneumonia (COP) Non-infectious inflammation that may occur in collagenous diseases, chronic eosinophilic pneumonia, exogenous allergic alveolitis, infections or even as a medication reaction • Symptoms: chronic subfebrile temperatures, dyspnoea and cough
• HRCT: Band-shaped, subpleural and peribronchial stressed focal consolidations with basal predominance - migrating consolidations
• Atoll sign: by a ring-like consolidation with central milk glass
33 Prosch H. Journal für Pneumologie 2015; 3 (1), 24-27
I. DISEASES OF IMMUNOLOGICAL / UNCLEAR AETIOLOGY
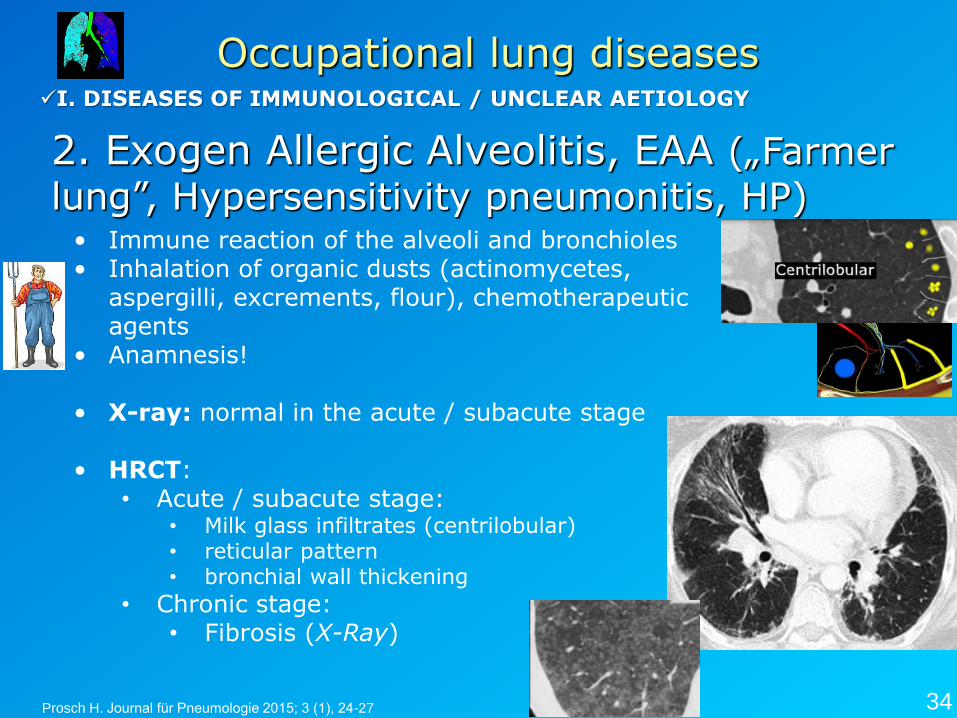
2. Exogen Allergic Alveolitis, EAA („Farmer
lung”, Hypersensitivity pneumonitis, HP)
Occupational lung diseases
• Immune reaction of the alveoli and bronchioles • Inhalation of organic dusts (actinomycetes,
aspergilli, excrements, flour), chemotherapeutic agents
• Anamnesis!
• X-ray: normal in the acute / subacute stage
• HRCT: • Acute / subacute stage:
• Milk glass infiltrates (centrilobular) • reticular pattern • bronchial wall thickening
• Chronic stage: • Fibrosis (X-Ray)
I. DISEASES OF IMMUNOLOGICAL / UNCLEAR AETIOLOGY
34 Prosch H. Journal für Pneumologie 2015; 3 (1), 24-27
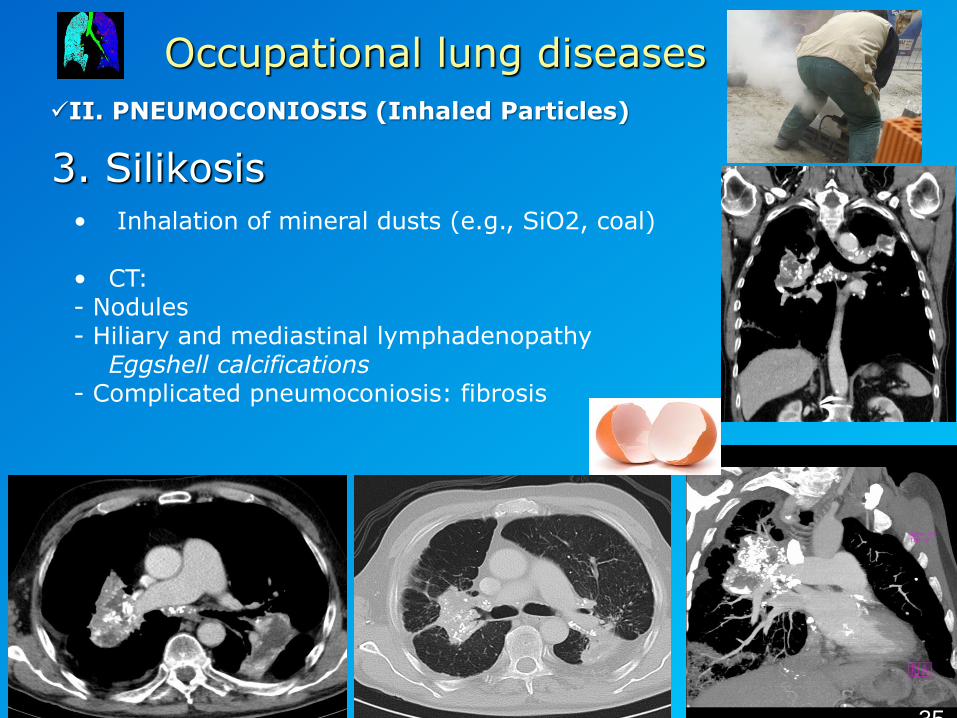
3. Silikosis
Occupational lung diseases
• Inhalation of mineral dusts (e.g., SiO2, coal) • CT: - Nodules - Hiliary and mediastinal lymphadenopathy Eggshell calcifications - Complicated pneumoconiosis: fibrosis
II. PNEUMOCONIOSIS (Inhaled Particles)
35
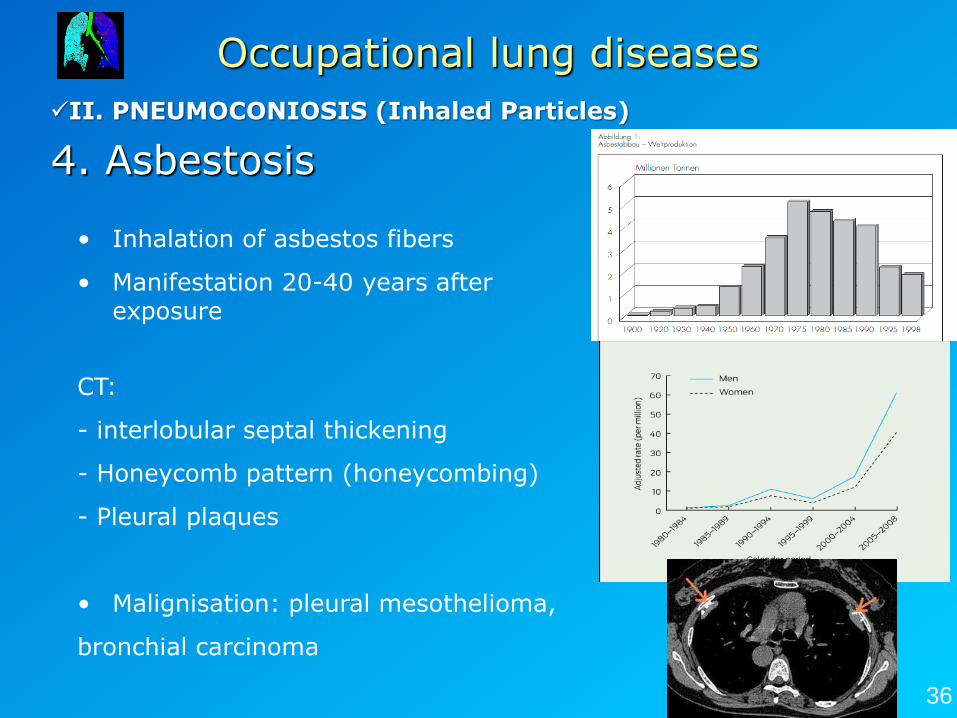
4. Asbestosis
Occupational lung diseases
• Inhalation of asbestos fibers
• Manifestation 20-40 years after exposure
CT:
- interlobular septal thickening
- Honeycomb pattern (honeycombing)
- Pleural plaques
• Malignisation: pleural mesothelioma,
bronchial carcinoma
II. PNEUMOCONIOSIS (Inhaled Particles)
36
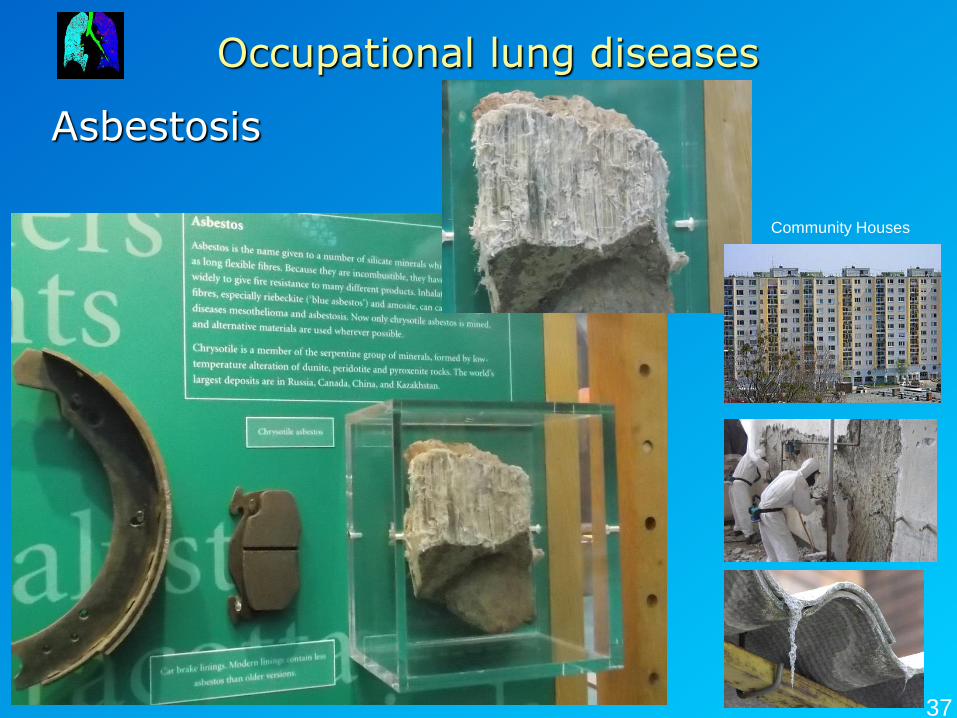
Asbestosis
Occupational lung diseases
37
Community Houses
Pleura
38
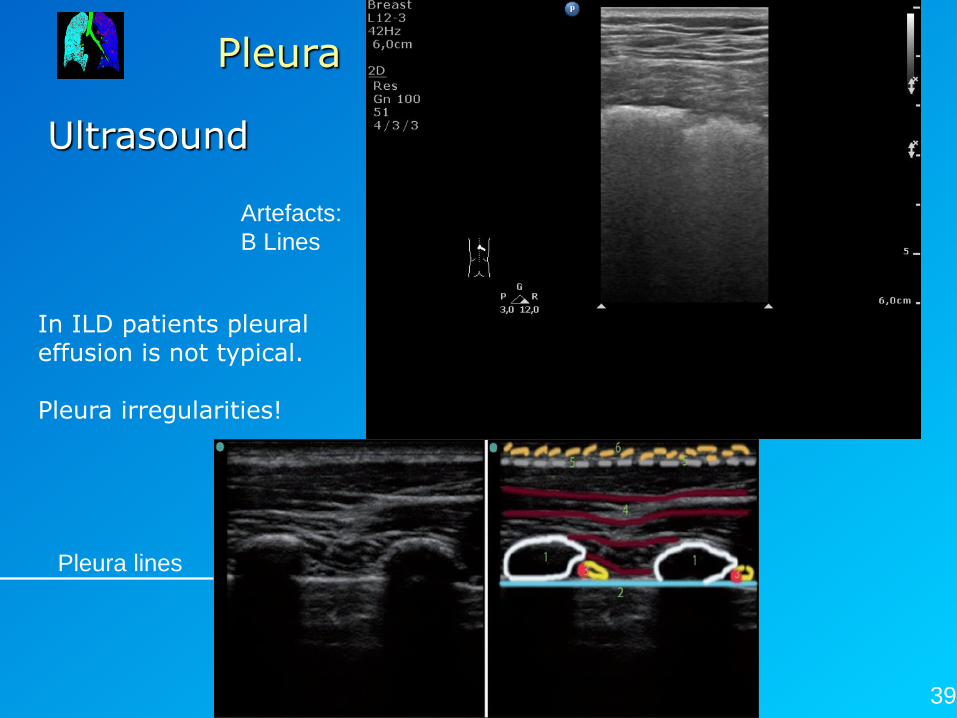
Pleura
Ultrasound
Pleura lines
39
Artefacts:
B Lines
In ILD patients pleural effusion is not typical. Pleura irregularities!
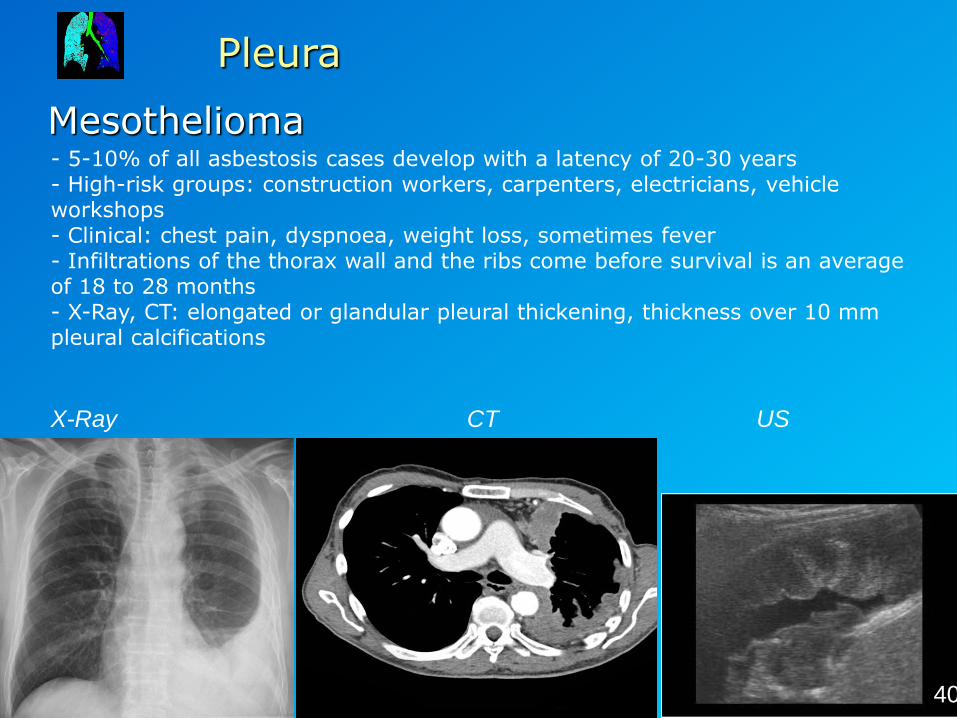
Pleura
Mesothelioma - 5-10% of all asbestosis cases develop with a latency of 20-30 years - High-risk groups: construction workers, carpenters, electricians, vehicle workshops - Clinical: chest pain, dyspnoea, weight loss, sometimes fever - Infiltrations of the thorax wall and the ribs come before survival is an average of 18 to 28 months - X-Ray, CT: elongated or glandular pleural thickening, thickness over 10 mm pleural calcifications
X-Ray CT US
40
Summary
• For the characterization of interstitial changes, the Computed tomography (HRCT) is the
method of choice • None of the samples presented is specific for a
disease (UIP only) • The suspicious diagnosis results from the
morphology, the distribution of findings, the dynamics and the clinic
→ discussion with the clinicans (!)
41
Summary
1. What kind of information needed for the clinicians?
- Diagnosis of the ILDs, biopsy, alveolitis or fibrosis patterns 2. X-Ray: Fine-striated reticular pattern, basal dominance 3. HRCT-Signs: Acute inflammation (alveolitis): GGO Chronic: Honeycombing 4. Difference between NSIP and UIP: NSIP: no honeycombing UIP is very specific: honeycombing
42
Summary
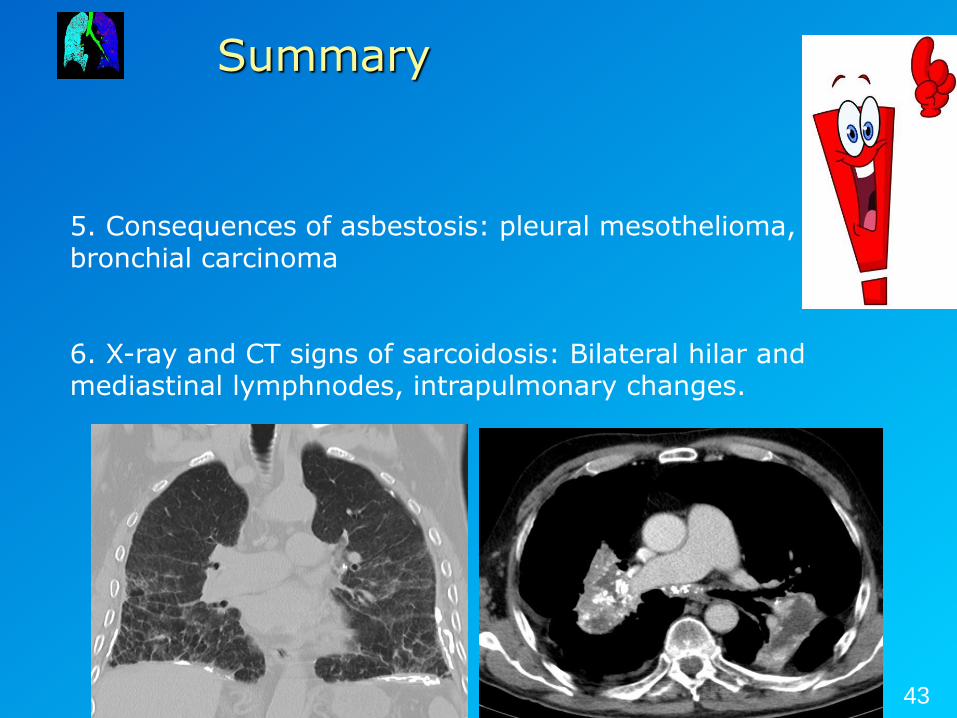
5. Consequences of asbestosis: pleural mesothelioma, bronchial carcinoma 6. X-ray and CT signs of sarcoidosis: Bilateral hilar and mediastinal lymphnodes, intrapulmonary changes.
43
Thank you!
E-mail: [email protected]
Thank you for the images: Dr.
Monostori und Dr. Judit Pápay
44
„You only see what you know“ (Johann Wolfgang von Goethe)