Embed Size (px)
Citation preview

660 SA MEDIESE TYDSKRIF DEEL 63 23 APRIL 1983
Ventricular septal defect due to bluntchest traumaA case report
L. R. OLlVIER, D. S. ROSSOUW,M. S. STEVENS
S. J. DE VILLlERS, W. A. VERMEULEN,
Summary
Blunt chest trauma may cause cardiac trauma, thispossibility often being overlooked. Various anatomical structures may be affected. A case of ventr'icularseptal defect due to blunt chest trauma is describedand the relevant literature is reviewed.
S Atr Med J 1983: 63: 660-662.
In cases of chest trauma, and particularly ofblunt trauma, injuryto the heart is often overlooked. I It is sometimes diagnosed at alater stage1 or only discovered post mortem.' It is our aim to drawthe attention of physicians and surgeons alike to cardiac traumaarising after blunt trauma to the chest. This commonly occurs inmotor \'ehicle accidents,~'~ but the cardiac trauma is ~ot alwayse\ident LZ because of associated injuries. The reported incidenceof heart injury following non-penetrating trauma to the chest\aries from 16% to 76%:·8 Failure to su'spect the injury, especialh' in the face of other more obvious severe injuries, probablycontributes to the relati\'e i(lfrequency of this diagnosis.2
. Jackson and Murphy' discuss the causes and mechanisms of bluntcardiac trauma in an excellent review, and also list 19 types ofinjury resulting from blunt chest trauma. We are not aware ofany South African report of a patient \\'ho has sustained aninterventricular septal defect following blunt chest trauma. Wereport a patient in whom this diagnosis \\'as made and who wassuccessfully treated.
experienced the pain while working, with improvement on rest.He also noticed shortness of breath when working or walkingbriskly.
On examination our patient was an intelligent, tall, muscularyoung man with no evidence of anaemia, jaundice or cyanosis.His pulse rate was 88/min and regular and his blood pressure120/170 mmHg. His neck veins were nor distended. The chestwall showed no sign of previous injury. A left parasternal heaveand a pansystolic thrill were palpable. The apex beat was in the5th intercostal space and well within the midclavicular line. Onauscultation a grade 4/6 pansystolic murmur, which was maximal at the 4th intercostal space to the left of the sternum andaudible over the whole anterior chest, was heard. The pulmonarycomponent of the second sound was loud. A clinical diagnosis of\'entricular septal defect (VSD) with moderate pulmonaryhypertension but without heart failure or infective endocarditiswas made.
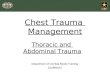
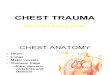
The erythrocyte sedimentation rate was 5 mm/1st h (Westergren), while a full blood count revealed no abnormality. Thehaemoglobin concentration was 17,4 g/dl and the haematocritle\'e! 0,5211/1. The blood chemical values were normal. Electrocardiography showed sinus rhythm with right axis deviation,right ventricular hypertrophy and pathological Q waves in theanterior chest leads V2 - V4, consistent with a previous anteroseptal myocardial infarction (Fig. I). Chest radiography revealedincreased vascular markings in the lungs (Fig. 2).
11111""'-1'.' ... ' ".' - ....: :~::.. ,. -.:: ;:: . -.. -.... . . - .. '~ --:=~, ;~-::.+-~ ~. ,"
. ~ . ~ , . .' ::.:, ~ ,'.- ~ ::-,:", '.,'
I II III R L F
Case report
An unmarried, well-built 25-year-old Black labourer was admitted to H. F. Verwoerd Hospital, Pretoria, on 8 September 1981.On admission his main complaint was of having had central chestpain since October 1980 when he had been caught between are\'ersing 20-ton truck and a huge waste-container, with the rearbumper at the le\'e! of his chest. During this he had experienced asensation as if his chest was cracking. Admission to a nearbyho pital was followed by a period of observation, after which hewas discharged as healthy and fit. At this time he also becamea\\'are of a vibration ·in "his chest. Since his accident he had
Departments ofMedicine and Cardiothoracic Surgery, University of Pretoria and H. F. Verwoerd Hospital, PretoriaL. R. OLIVIER, .\\ .\\ED . Principal PhysicianD. S. ROSSOUW, .\\..\\ED.. DPHIL OXO:\. ,ProfessorS. J. DE VILLIERS, .\\ .\\ED, F.es. S..-\.• Principal Surgeon\X'. A. VERMEULEN, .\\ B cH.B.. RegislrarM. S. STEVENS, .\\.B. CH.B·.. Registrar
DJh: rt:c~l\eJ: 16 :\rnl 1982
Fig. 1: ECG showing sinus rhythm with right axis deviation, rightventricular hypertrophy and pathological a waves in anteriorchest leads V2 - V4.
On echocardiography the left ventricle was seen to beenlarged, with volume overload. The size of the right ventriclewas at the upper limit of normal with hypertrophy of the anteriorwall and interventricular septum. Heart catheterization was performed on 9 September 1981 (Table I). A VSD was clearlydemonstrated. Oxygen saturation showed a rise from 70% in theright atrium to 86% in the right ventricle. The coronary arterieswere of normal distribution and patency.

SA MEDICAL JOURNAL VOLUME 63 23 APRIL 1983 661
'Shunt ratio 1,8:1.
Fig. 2. Pre-operative chest radiograph showing increased vascular markings.
On 23 November 1981 the VSD was closed with a Dacronpatch and interrupted sutures through a right ventriculotomywith the aid of total cardiopulmonary bypass and cardioplegicarrest of the heart. At operation a 3 x 5 cm area of adhesionsbetween the epicardium and pericardium in the region of themiddle third of the left anterior descending artery (LAD) wasseen. Right ventricular hypertrophy was present. A VSD of 1,5 x1,5 cm was present in the muscular septum juSt below the middlethird of the LAD. Postoperatively the right ventricular pressurewas 15/0 mmHg. The postoperative course was uneventful andthe patient was discharged on 7 December 1981. On follow-upthe patient wa found to be asymptomatic and no murmur waspresent on auscultation. A cardiac flow study performed withradio-isotopes showed no evidence of an intracardiac shunt.
cardiac trauma: (i) fractured sternum; (ii) variable cardiacrhythm; (iiz) tachycardia; (it') changing ECG; ('v) new cardiacmurmurs; (-VI) recurrent haemothorax; (z'ii) widening of themediastinum; and (zliii) haemopericardium.
Rosenthal ez al. 9 originally described the triad of chest trauma,cardiac murmur and an infarction pattern on the ECG. \X'henour patient was admitted for the econd time (to a medical ward)the diagnosis of a VSD was obvious. The question arises as towhether this VSD could have been a congenital lesion. Thepresence of fibrous tissue around the defect in the mu cularseptum suggests the recent occurrence ofan inflammatory reaction and aids in the pathological diagnosis of traumatic VSD.2
•1O
The ECG in cardiac trauma has been well described,2.5.ll 16
and acute coronary artery occlusion secondary to blunt chesttrauma is well documented. '5.16 In our patient there was electrocardiographic and macroscopic evidence ofa previou infarction.Pifarn~ el al. l ; recorded a patient with an acute occlusion of theproximal LAD. At operation 5 months later the LAD was patentand fully distended. Much the same could have happened withour patient.
Despite its seemingly protected anatomical position, theinterventricular septum appears acutely susceptible to injurysecondary to non-penetrating chest trau ma. I i Blunt trauma characteristically produces d~fects in the muscular septum, as demonstrated in this case.6
.I
'
\Xlhat actually causes the rupture of the septum? Two explanations of the mechanism of rupture of the interventricular septumhave been put forward: 18
I. The initial damage of the nutrient vessels of the septum orpapillary muscles results in infarction, which progres es to liquefaction necrosis and perforation or rupture.
2. The heart is compressed during the vulnerable period oflatediastole or early systole when the ventricular chambers are fulland the valves are closed. This elevation of ventricular tensioncauses rupture of the septum.
In a patient with a traumatic VSD the prognosis withoutoperation depends largely on the size of the defect, the type oftrauma and associated other injuries. 19 The patient who is symptomatic requires repair sooner, occasionally within a few days ofinjury if the left-to-right shunt is ma ive. In the case of thesmall, asymptomatic VSD with a calculated shunt of less than1,5:1 and with normal right heart pres ures, closure is justifiedprimarily to avert the risk of endocarditis." In cases in which thedefect was closed using cardiopulmonary bypass the prognosIswas extremely good.
Turney el al." reported 22 case in the literature in whichsurgery was employed without a single death. The indications forsurgical repair are: 19 (i) evidence of cardiac enlargement; (ii)symptoms of congestive heart failure; and (iii) right ventricularpressure elevation.
In conclusion, we strongly recommend that in patients whohave experienced blunt trauma to the chest the diagnosis ofcardiac injury should always be entertained. I t is mandatory tonurse such patients in an intensive care unit and daily electrocardiography is essential. Early cardiac catheterization could bebeneficial to the patient, remembering that you see only whatyou look for.
9494
Mean 10
80/0-1480/30
Mean 22150/0 - 15
150/85
Pressure (mmHg)
TABLE I. CARDIAC CATHETERIZATION DATA'
Oxygensaturation
(%)
6770738686
Superior vena cavaRight atriumInferior vena cavaRight ventriclePulmonary arteryPulmonary wedgeleft ventricleAorta
Site
REFERE~CES
Discussion
In this case the diagnosis of VSD was not made at the firstadmission. The delayed onset of the typical pansystolic murmurthat is frequently noted in the literature6 is difficult to explain.Perhaps a soft murmur may have been overlooked until itbecame more obvious with improved cardiac function. Madoffand Desforges i suggest the following clinical features as significant diagnostic clues in assisting the physician in diagno ing
I. Te Ride JAM, Bru'chke A\'G, Schaepkens "an Riemp;t :\LE.\IS. Hel ,tompehanlel'e!. S"d TiJd'dzr Gm" ..,kd 1979; 123: 43-48.
2. ROlman .\1, Peter RH, Seal\' \X'C, .\Ionis JJ. Traumatic "entricular ,eptaldefect secondary to non-penetrating che;r trauma. ~III J M ..d 1970; 48:127-131.
3. Jackson DH, .\\urphy G\X'. ~onpenetrating cardiac trauma. J\fvJ COn(t'plsC"rdiO"i'<l5c Di, 1976; 45: 123-12
~. Car\' FH, Hur;t J\X', Arentzen \X'R. Acquired inten'entricular ,eptal defectsecondar,' to trauma. .\' t.'nglJ M ..d 1958; 258: 155-359.
5. Hanhorne J\X', Kantrowitz PA, Dinsmore RE, Sanders CA. Traumaticmyocardial infarction. ~ml Ill/an M ..d 1967; 66: 341-344.
6. Turney S2, .'vlathai J, Singleton R, Cowle,' RA. Traumatic \'entricular ,eptaldefect. ~ml Thor'I< S/lr~ 1972; 13: 36-43.

662 SA MEDIESE TYDSKRIF DEEL 63 23 APRIL 1983
7. Madoff IM, Desforges G. Cardiac injuries due to nonpenetrating thoracictrauma. Arm Thor<leSlIrg 1972; 14: 504-512.
8. Menzies RC. Cardiac contusion: a re,'ie\\". Med Sei L<l'" 1978; 18: 3-12.9. Rosemhal A, Parisi LF, Nadas AS. Isolated interventricular septal defect due
to nonpenetrating trauma.'" EnglJ Med 1970; 283: 338-341.10. Cleland \X'P, Ellman P, Goodwin J, Hollman A. Repair of ,'entricular septal
defect following indirect trauma. Br J Dis Chest 1961; 55: 2-22.I I. Cane RD, Schamroth L. Prolongation of the Q-T imen'al with mvocardial
contusion. Hetlrt Lung 1978; 7: 652-656.12. Chung EK, Renn J. Electrocardiographic changes in nonpenetrating trauma to
the chesr.Acra C<lrdioI1970; 25: 418-423.13. Dolara A, Morando P, Pampaloni M. Electrocardiographic findings in 98
consecUIi\"e non-penetrating chest injuries. Dis Chest 1967; 52: 50-56.
14. Jones FL. Transmural myocardial necrosis after non-penetrating cardiactrauma. Am J Cardiol 1970; 26: 419-422.
15. Pifarre R, Grieco J. Garibaldi A et al. Acute coronary artery occlusion secondary to blunt chest trauma.] Thoruc Cardicn'usc SlIrg 1982; 83: 122-125.
16. Clark TA, Corcoran FH, Baker WP er al. Early repair of traumatic vemricularseptal defec!.J TJlOr<lC Curdicn'usc SlIrg 1974; 67: 121-124.
17. Liedtke AJ, DeMuth WE. Nonpenetrating cardiac injuries: a collecti,'e review.Am Heart J 1973; 86: 687-697.Anyanwu CH. Mitral incompetence and ventricular septal defects followingnon penetrating injury. Thorax 1976; 31: 113-117.
19. Millar OR, Crocker JE, POller CA. Traumatic inten'entricular septal defect: areview and report of two cases. AfmSurg 1962; 155: 72-81.
Malignant insulinoma: The problems oftumour localization and managementA case report
L. G. SVENSSON, M. WELLSTED
Summary
A case of malignant insulinoma in a Black patient ispresented. An investigational protocol is suggestedwith a discussion of the newer techniques of pancreatic adenoma localization and the therapeuticmeasures available for the management of malignant islet cell tumours.
S A ir Med J , 983; 63: 662-<364.
Malignant insulinomas of the pancreas are rare tumours,accounting for 10% of cases of insulinoma in the Mayo Clinicseries I and 16% ofcases in the world literature,2 with a likely biastowards malignant cases. At the time of diagnosis 69% havemetasrasized, usually to the liver. Ectopic pancreatic adenomashave a higher incidence of malignancy. 3
Ne\\' investigational techniques have evolved for the localization of pancreatic adenomas, bur none is infallible. Some of thenewer techniques and avenues of research which may yieldfruitful diagnostic aid will be discussed.
Hillbrow Hospital and Department ofSurgery, University ofthe \'Vitwatersrand, JohannesburgL. G. SVENSSON, .\\.B. B.cH.,RegislrarM. WELLSTED, M.B, B.CH.. f,es. (s.A.).Principal Surgeon
Dale recened: 14 July 1982.
Case report
The patient, a 60-year-old Black man, presented at the HillbrowHospital with a history of having fainted with associated sweating, dizziness and palpitations. He had been admitted after twoprevious attacks, the only positive finding being hypertension,for which he was treated. On admission his blood sugar level wasless than I mmolll. He responded well to intravenous glucoseadministration. Apart from obesity and mild "hypertension,examination proved negative.
An oral glucose tolerance test showed a characteristic flatcurve. At the time of commencement of a 16-hour fast the insulinle\'el was 182 p U/ml; the fast was stopped when the patientdeveloped symptoms of hypoglycaemia at a blood glucose levelof 1,7 mmolll and an insulin level of33 p U/ml (normal range 626 pU/ml).
Results of the following investigations were normal: serumgastrin and cortisol estimation, liver function tests indudingalkaline phosphatase measurement, barium meal, endoscopy,liver spleen isotope scan and grey-scale ultrasound examinationof the liver. (The pancreas was not visualized.) Pro-insulin andC-peptide assays could not be obtained.
A transfemoral arteriogram was reported as showing a patentportal vein with an obstructed splenic vein with collateral drainage and associated multiple splenic varices. The pancreas waswell visualized, except for the tail. The computed tomogram(CT) was also reported as being normal. Endoscopic retrogradecholangiopancreatography also failed to localize the tumour.
Percutaneous transhepatic portal vein insulin sampling at 2cm intervals in the tributaries showed the insulin levels to be 167pU/ml in the distal stump and 159 j.LU/ml in the proximalportion of the splenic vein, 61 j.L U/ml in the superior mesentericvein, 48 pU/ml in the pancreaticoduodenal vein, 52 pU/ml inthe right gastric vein and 33 p U/ml in the portal vein (Fig. 1).