-
7/29/2019 Chest Trauma Basics
1/151
CHEST TRAUMAHEST TRAUMAHEST TRAUMAHEST TRAUMAJoe Lex, MD,
FAAEMoe Lex, MD, FAAEMTemple University Hospitalemple University
Hospital
Philadelphia, PAhiladelphia, PAJuly 20uly 20 thh, 20062006
Joe Lex, MD, FAAEMoe Lex, MD, FAAEMTemple University
Hospitalemple University HospitalPhiladelphia, PAhiladelphia,
PAJuly 20uly 20 thh, 20062006
-
7/29/2019 Chest Trauma Basics
2/151
-
7/29/2019 Chest Trauma Basics
3/151
Incidence of Chest TraumaIncidence of Chest Trauma
Incidence of Chest TraumaIncidence of Chest Trauma
1/4 American trauma deaths
Contributes to another 1 of 4
Many die after reaching hospital -preventable if recognized
-
7/29/2019 Chest Trauma Basics
4/151
Pathophysiology of Chest TraumaPathophysiology of Chest
Trauma
Pathophysiology of Chest TraumaPathophysiology of Chest
Trauma
hypovolemia
ventilation-
perfusionmismatch
changes inintrathoracic
pressure
relationships
TISSUEHYPOXIA
Inadequate oxygendelivery to tissues
-
7/29/2019 Chest Trauma Basics
5/151
Pathophysiology of Chest TraumaPathophysiology of Chest
Trauma
Pathophysiology of Chest TraumaPathophysiology of Chest
Trauma
Tissue hypoxia
Hypercarbia
Respiratory acidosis: inadequate ventilation
Metabolic acidosis: tissue hypoperfusion(e.g., shock)
Tissue hypoxia
Hypercarbia
Respiratory acidosis: inadequate ventilation
Metabolic acidosis: tissue hypoperfusion(e.g., shock)
-
7/29/2019 Chest Trauma Basics
6/151
Blunt traumaBlunt trauma
Blunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
7/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
8/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
9/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
10/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
11/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
12/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
13/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
14/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
15/151
Blunt traumaBlunt traumaBlunt traumaBlunt trauma
-
7/29/2019 Chest Trauma Basics
16/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
17/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
18/151
Splinter
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
19/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
20/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
21/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
22/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
23/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
24/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
25/151
Penetrating traumaPenetrating traumaPenetrating
traumaPenetrating trauma
-
7/29/2019 Chest Trauma Basics
26/151
6 Immediate Life Threats6 Immediate Life Threats6 Immediate Life
Threats6 Immediate Life Threats
Airway obstruction
Tension pneumothorax
Open pneumothorax
sucking chest wound
Massive hemothorax Flail chest
Cardiac tamponade
Airway obstruction
Tension pneumothorax
Open pneumothorax
sucking chest wound
Massive hemothorax Flail chest
Cardiac tamponade
-
7/29/2019 Chest Trauma Basics
27/151
6 Potential Life Threats6 Potential Life Threats6 Potential Life
Threats6 Potential Life Threats
Lung contusion
Heart contusion
Aorta rupture
Diaphragm rupture
Tracheobronchial tree injury -larynx, trachea, bronchus
Esophagus trauma
Lung contusion
Heart contusion
Aorta rupture
Diaphragm rupture
Tracheobronchial tree injury -larynx, trachea, bronchus
Esophagus trauma
-
7/29/2019 Chest Trauma Basics
28/151
6 Other Frequent Injuries6 Other Frequent Injuries6 Other
Frequent Injuries6 Other Frequent Injuries
Subcutaneousemphysema
Traumatic asphyxia
Simple pneumothorax
Hemothorax
Scapula fracture
Rib fractures
Subcutaneousemphysema
Traumatic asphyxia
Simple pneumothorax
Hemothorax
Scapula fracture
Rib fractures
-
7/29/2019 Chest Trauma Basics
29/151
Primary SurveyPrimary SurveyPrimary SurveyPrimary Survey
Airway
Breathing
Circulation
Airway
Breathing
Circulation
-
7/29/2019 Chest Trauma Basics
30/151
A = AirwayA = AirwayA = AirwayA = Airway
Assess for airway patency and airexchange - listen at nose &
mouth
Assess for intercostal and supraclavicularmuscle retractions
Assess oropharynx for foreign body
obstruction
Assess for airway patency and airexchange - listen at nose &
mouth
Assess for intercostal and supraclavicularmuscle retractions
Assess oropharynx for foreign body
obstruction
-
7/29/2019 Chest Trauma Basics
31/151
B = BreathingB = BreathingB = BreathingB = Breathing
Assess respiratory movements and qualityof respirations look,
listen, feel
Shallow respirations are early indicator ofdistress cyanosis is
late
Assess respiratory movements and qualityof respirations look,
listen, feel
Shallow respirations are early indicator ofdistress cyanosis is
late
-
7/29/2019 Chest Trauma Basics
32/151
C = CirculationC = CirculationC = CirculationC = Circulation
Assess pulses for quality, rate, regularity
Assess blood pressure and pulse pressure
Skin - look and feel for color,temperature, capillary refill
Look at neck veins - flat vs. distended
Cardiac monitor
Assess pulses for quality, rate, regularity
Assess blood pressure and pulse pressure
Skin - look and feel for color,temperature, capillary refill
Look at neck veins - flat vs. distended
Cardiac monitor
-
7/29/2019 Chest Trauma Basics
33/151
Where can adults hide blood and goWhere can adults hide blood
and go
into shock?into shock?Where can adults hide blood and goWhere
can adults hide blood and go
into shock?into shock?
Chest: listen, do chest x-ray
Abdomen: do DPL or CT or US
Retroperitoneum: do CT
Thigh: physical examination
Street: ask paramedic...and in children, add
Head
Chest: listen, do chest x-ray
Abdomen: do DPL or CT or US
Retroperitoneum: do CT
Thigh: physical examination
Street: ask paramedic...and in children, add
Head
-
7/29/2019 Chest Trauma Basics
34/151
Initial assessment and managementInitial assessment and
managementInitial assessment and managementInitial assessment and
management
Primary survey
Resuscitation of vital functions Detailed secondary survey
Definitive care
Primary survey
Resuscitation of vital functions Detailed secondary survey
Definitive care
-
7/29/2019 Chest Trauma Basics
35/151
Initial assessment and managementInitial assessment and
managementInitial assessment and managementInitial assessment and
management
Hypoxia most serious problem: earlyinterventions aimed at
reversing
Immediate life-threatening injuriestreated quickly and simply,
usually withtube or a needle
Secondary survey guided by highsuspicion for specific
injuries
Hypoxia most serious problem: earlyinterventions aimed at
reversing
Immediate life-threatening injuriestreated quickly and simply,
usually withtube or a needle
Secondary survey guided by highsuspicion for specific
injuries
-
7/29/2019 Chest Trauma Basics
36/151
ThoracotomyThoracotomyThoracotomyThoracotomy
Closed heart massage is ineffective in ahypovolemic patient
Left anterior thoracotomy with cross-clamping of descending
thoracic aorta andopen-chest massage may be useful in
pulseless victim of penetrating trauma
Closed heart massage is ineffective in ahypovolemic patient
Left anterior thoracotomy with cross-clamping of descending
thoracic aorta andopen-chest massage may be useful in
pulseless victim of penetrating trauma
-
7/29/2019 Chest Trauma Basics
37/151
ThoracotomyThoracotomyThoracotomyThoracotomy
Emergency departmentthoracotomy for patientswithout cardiac
activity who
are victims of blunt thoracicinjuries is ineffective
Emergency departmentthoracotomy for patientswithout cardiac
activity who
are victims of blunt thoracicinjuries is ineffective
-
7/29/2019 Chest Trauma Basics
38/151
ThoracotomyThoracotomyThoracotomyThoracotomy
-
7/29/2019 Chest Trauma Basics
39/151
ThoracotomyThoracotomyThoracotomyThoracotomy
-
7/29/2019 Chest Trauma Basics
40/151
ThoracotomyThoracotomyThoracotomyThoracotomy
-
7/29/2019 Chest Trauma Basics
41/151
ThoracotomyThoracotomyThoracotomyThoracotomy
-
7/29/2019 Chest Trauma Basics
42/151
-
7/29/2019 Chest Trauma Basics
43/151
-
7/29/2019 Chest Trauma Basics
44/151
6 Immediate Life Threats6 Immediate Life Threats6 Immediate Life
Threats6 Immediate Life Threats
Airway obstruction
Tension pneumothorax
Open pneumothorax
sucking chest wound
Massive hemothorax Flail chest
Cardiac tamponade
Airway obstruction
Tension pneumothorax
Open pneumothorax
sucking chest wound
Massive hemothorax Flail chest
Cardiac tamponade
-
7/29/2019 Chest Trauma Basics
45/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
Airway obstruction at alveolar level:assessed and managed during
2o survey
Upper airway obstruction immediatelife threat which must be
dealt with inprimary survey
Most common cause: patients tongue
Airway obstruction at alveolar level:assessed and managed during
2o survey
Upper airway obstruction immediatelife threat which must be
dealt with inprimary survey
Most common cause: patients tongue
-
7/29/2019 Chest Trauma Basics
46/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
Chin-lift: fingersunder mandible,
lift forward sochin is anterior
Chin-lift: fingersunder mandible,
lift forward sochin is anterior
-
7/29/2019 Chest Trauma Basics
47/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
-
7/29/2019 Chest Trauma Basics
48/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
Jaw thrust: grasp angles of mandible andbring jaw forward
Jaw thrust: grasp angles of mandible andbring jaw forward
-
7/29/2019 Chest Trauma Basics
49/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
Oropharyngealairway: insert into
mouth behind tongue DO NOT push tongue
further back
Oropharyngealairway: insert into
mouth behind tongue DO NOT push tongue
further back
-
7/29/2019 Chest Trauma Basics
50/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
Nasopharyngealairway: gently
insert well-lubricated
trumpet
through nostril
Nasopharyngealairway: gently
insert well-lubricated
trumpet
through nostril
-
7/29/2019 Chest Trauma Basics
51/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
Definitive Airway
Management: tubein trachea throughvocal cords with
balloon inflated
Definitive Airway
Management: tubein trachea throughvocal cords with
balloon inflated
-
7/29/2019 Chest Trauma Basics
52/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
Orotracheal intubation
Nasotracheal intubation: in breathing
patient without major facial trauma
Surgical airways
jet insufflation
retrograde
cricothyrotomy
tracheostomy
Orotracheal intubation
Nasotracheal intubation: in breathing
patient without major facial trauma
Surgical airways
jet insufflation
retrograde
cricothyrotomy
tracheostomy
-
7/29/2019 Chest Trauma Basics
53/151
Airway ObstructionAirway ObstructionAirway ObstructionAirway
Obstruction
Jet insufflation adapters
-
7/29/2019 Chest Trauma Basics
54/151
-
7/29/2019 Chest Trauma Basics
55/151
How to perform cricothyroidotomyHow to perform
cricothyroidotomyHow to perform cricothyroidotomyHow to perform
cricothyroidotomy
-
7/29/2019 Chest Trauma Basics
56/151
-
7/29/2019 Chest Trauma Basics
57/151
-
7/29/2019 Chest Trauma Basics
58/151
-
7/29/2019 Chest Trauma Basics
59/151
-
7/29/2019 Chest Trauma Basics
60/151
-
7/29/2019 Chest Trauma Basics
61/151
-
7/29/2019 Chest Trauma Basics
62/151
-
7/29/2019 Chest Trauma Basics
63/151
-
7/29/2019 Chest Trauma Basics
64/151
-
7/29/2019 Chest Trauma Basics
65/151
-
7/29/2019 Chest Trauma Basics
66/151
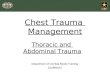
Tension pneumothoraxTension pneumothoraxTension
pneumothoraxTension pneumothorax
Air leak through lung or chest wall
One-way valve lung collapse
Mediastinum shifts to opposite side Inferior vena cava kinks on
diaphragmdecreased venous return
cardiovascular collapse
Air leak through lung or chest wall
One-way valve lung collapse
Mediastinum shifts to opposite side Inferior vena cava kinks on
diaphragmdecreased venous return
cardiovascular collapse
-
7/29/2019 Chest Trauma Basics
67/151
Inferior vena cava
-
7/29/2019 Chest Trauma Basics
68/151
Tension pneumothoraxTension pneumothoraxTension
pneumothoraxTension pneumothorax
Tension pneumothorax is not an x-raydiagnosis it MUST be
recognizedclinically
Treatment is decompression needle into2nd intercostal space of
mid-clavicular line
- followed by thoracotomy tube
Tension pneumothorax is not an x-raydiagnosis it MUST be
recognizedclinically
Treatment is decompression needle into2nd intercostal space of
mid-clavicular line
- followed by thoracotomy tube
-
7/29/2019 Chest Trauma Basics
69/151
Insert needle here
-
7/29/2019 Chest Trauma Basics
70/151
Open pneumothoraxOpen pneumothoraxOpen pneumothoraxOpen
pneumothorax
Sucking Chest Wound
Normal ventilation requires negative intra-
thoracic pressure
Large open chest-wall defectimmediate equilibration of
intra-thoracic
and atmospheric pressures If hole >2/3 tracheal diameter, air
prefers
chest defect
Sucking Chest Wound
Normal ventilation requires negative intra-
thoracic pressure
Large open chest-wall defectimmediate equilibration of
intra-thoracic
and atmospheric pressures If hole >2/3 tracheal diameter, air
prefers
chest defect
-
7/29/2019 Chest Trauma Basics
71/151
Open pneumothoraxOpen pneumothoraxOpen pneumothoraxOpen
pneumothorax
-
7/29/2019 Chest Trauma Basics
72/151
Open pneumothoraxOpen pneumothoraxOpen pneumothoraxOpen
pneumothorax
Initial treatment: seal defect and secureon three sides (total
occlusion may lead to
tension pneumothorax Definitive repair of defect in O.R.
Initial treatment: seal defect and secureon three sides (total
occlusion may lead to
tension pneumothorax Definitive repair of defect in O.R.
-
7/29/2019 Chest Trauma Basics
73/151
Massive hemothoraxMassive hemothoraxMassive hemothoraxMassive
hemothorax
Rapid accumulation of >1500 cc blood inchest cavity
Hypovolemia & hypoxemia
Neck veins may be:
Flat: from hypovolemia
Distended: intrathoracic blood
Absent breath sounds, DULL to percussion
Rapid accumulation of >1500 cc blood inchest cavity
Hypovolemia & hypoxemia
Neck veins may be:
Flat: from hypovolemia
Distended: intrathoracic blood
Absent breath sounds, DULL to percussion
-
7/29/2019 Chest Trauma Basics
74/151
-
7/29/2019 Chest Trauma Basics
75/151
-
7/29/2019 Chest Trauma Basics
76/151
-
7/29/2019 Chest Trauma Basics
77/151
Massive hemothorax: treatmentMassive hemothorax:
treatmentMassive hemothorax: treatmentMassive hemothorax:
treatment
Large-bore (32 to 36 F) tube to drainblood
If moderate sized (500 to 1500 ml) andstops bleeding, closed
drainage usuallysufficient
If initial drainage >1500 ml ORcontinuous bleeding >200 ml
/ hr, OPENTHORACOTOMY indicated
Large-bore (32 to 36 F) tube to drainblood
If moderate sized (500 to 1500 ml) andstops bleeding, closed
drainage usuallysufficient
If initial drainage >1500 ml ORcontinuous bleeding >200 ml
/ hr, OPENTHORACOTOMY indicated
-
7/29/2019 Chest Trauma Basics
78/151
Chest tube
-
7/29/2019 Chest Trauma Basics
79/151
How to place a chest tubeHow to place a chest tubeHow to place a
chest tubeHow to place a chest tube
-
7/29/2019 Chest Trauma Basics
80/151
Pleural space
-
7/29/2019 Chest Trauma Basics
81/151
-
7/29/2019 Chest Trauma Basics
82/151
-
7/29/2019 Chest Trauma Basics
83/151
-
7/29/2019 Chest Trauma Basics
84/151
-
7/29/2019 Chest Trauma Basics
85/151
-
7/29/2019 Chest Trauma Basics
86/151
l l hFl il h t
Fl il hFl il h t
-
7/29/2019 Chest Trauma Basics
87/151
Flail chestFlail chestFlail chestFlail chest
Free-floating chestsegment, usually from
multiple ribs fractures Pain and restricted
movement paradoxical
movement of chest wallwith respiration
Free-floating chestsegment, usually from
multiple ribs fractures Pain and restricted
movement paradoxical
movement of chest wallwith respiration
Fl il hFl il h t
Fl il h tFl il h t
-
7/29/2019 Chest Trauma Basics
88/151
Flail chestFlail chestFlail chestFlail chest
-
7/29/2019 Chest Trauma Basics
89/151
Fl il t t t ( ld)Fl il t t t ( ld)
Fl il t t t ( ld)Fl il t t t ( ld)
-
7/29/2019 Chest Trauma Basics
90/151
Flail treatment (old)Flail treatment (old)Flail treatment
(old)Flail treatment (old)
Fl il t t t ( ld)Fl il t t t ( ld)
Fl il t t t ( ld)Fl il t t t ( ld)
-
7/29/2019 Chest Trauma Basics
91/151
Flail treatment (old)Flail treatment (old)Flail treatment
(old)Flail treatment (old)
Fl il t t tFl il t t t
Fl il t t tFl il t t t
-
7/29/2019 Chest Trauma Basics
92/151
Flail treatmentFlail treatmentFlail treatmentFlail treatment
Ventilate well
Humidify oxygen
Resuscitate with fluids
Manage pain (!!)
Stabilize chest
Internal ventilator
External sand bags(rare)
Ventilate well
Humidify oxygen
Resuscitate with fluids
Manage pain (!!)
Stabilize chest
Internal ventilator
External sand bags(rare)
C di t dC di t d
C di t dC di t d
-
7/29/2019 Chest Trauma Basics
93/151
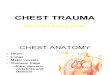
Cardiac tamponadeCardiac tamponadeCardiac tamponadeCardiac
tamponade
Usually from penetrating injuries
Classic Becks triad
elevated venous pressure - neck veins
decreased arterial pressure - BP
muffled heart sounds
Blood in sac
prevents cardiac
activity
Usually from penetrating injuries
Classic Becks triad
elevated venous pressure - neck veins
decreased arterial pressure - BP
muffled heart sounds
Blood in sac
prevents cardiac
activity
C di t dC di t d
C di t dCa diac tamponade
-
7/29/2019 Chest Trauma Basics
94/151
Cardiac tamponadeCardiac tamponadeCardiac tamponadeCardiac
tamponade
May find pulsus paradoxus - a decreaseof 10 mm Hg or greater in
systolic BP
during inspiration Systolic to diastolic gradient of less
than
30 mm Hg also suggestive
May find pulsus paradoxus - a decreaseof 10 mm Hg or greater in
systolic BP
during inspiration Systolic to diastolic gradient of less
than
30 mm Hg also suggestive
C di t dCa diac tamponade
C di t dCardiac tamponade
-
7/29/2019 Chest Trauma Basics
95/151
Cardiac tamponadeCardiac tamponadeCardiac tamponadeCardiac
tamponade
Treatment is removalof small amount of
blood 15 to 20 mlmay be sufficient from pericardial sac
Treatment is removalof small amount of
blood 15 to 20 mlmay be sufficient from pericardial sac
-
7/29/2019 Chest Trauma Basics
96/151
Pericardiocentesis
-
7/29/2019 Chest Trauma Basics
97/151
-
7/29/2019 Chest Trauma Basics
98/151
Stab wound toright ventricle
-
7/29/2019 Chest Trauma Basics
99/151
pericardium
epicardial fat
-
7/29/2019 Chest Trauma Basics
100/151
Ten-m inutebreakTen-m inutebreak
-
7/29/2019 Chest Trauma Basics
101/151
The Flock of Birds
-
7/29/2019 Chest Trauma Basics
102/151
behind the heart
Esophagoose
Azygoose v.
Vagoose n.
Thoracic duck
6 Potential Life Threats6 Potential Life Threats
6 Potential Life Threats6 Potential Life Threats
-
7/29/2019 Chest Trauma Basics
103/151
6 Potential Life Threats6 Potential Life Threats6 Potential Life
Threats6 Potential Life Threats
Pulmonary contusion
Myocardial contusion
Traumatic aortic rupture (TAR)
Traumatic diaphragmatic rupture
Tracheobronchial tree injury: larynx,trachea, bronchus
Esophageal trauma
Pulmonary contusion
Myocardial contusion
Traumatic aortic rupture (TAR)
Traumatic diaphragmatic rupture
Tracheobronchial tree injury: larynx,trachea, bronchus
Esophageal trauma
-
7/29/2019 Chest Trauma Basics
104/151
Pulmonary contusionPulmonary contusion
Pulmonary contusionPulmonary contusion
-
7/29/2019 Chest Trauma Basics
105/151
Pulmonary contusionPulmonary contusionPulmonary
contusionPulmonary contusion
Potentially life-threatening condition withinsidious onset
Parenchymal injury without laceration More than 50% will develop
pneumonia,
even with treatment
Up to 50% have only hemoptysis aspresenting symptom
Potentially life-threatening condition withinsidious onset
Parenchymal injury without laceration More than 50% will develop
pneumonia,
even with treatment
Up to 50% have only hemoptysis aspresenting symptom
-
7/29/2019 Chest Trauma Basics
106/151
-
7/29/2019 Chest Trauma Basics
107/151
Pulmonary contusionPulmonary contusion
Pulmonary contusionPulmonary contusion
-
7/29/2019 Chest Trauma Basics
108/151
Pulmonary contusionPulmonary contusionPulmonary
contusionPulmonary contusion
Patients with pre-existing conditions(emphysema, renal failure)
need early
intubation Treatment needs
to occur over time
as symptoms develop
Patients with pre-existing conditions(emphysema, renal failure)
need early
intubation Treatment needs
to occur over time
as symptoms develop
Myocardial contusionMyocardial contusion
Myocardial contusionMyocardial contusion
-
7/29/2019 Chest Trauma Basics
109/151
Myocardial contusionMyocardial contusionMyocardial
contusionMyocardial contusion
Blunt precordial chesttrauma
Difficult to diagnose Risk for dysrhythmia,
sudden death,
tamponade,pericarditis,ventricular aneurysm
Blunt precordial chesttrauma
Difficult to diagnose Risk for dysrhythmia,
sudden death,
tamponade,pericarditis,ventricular aneurysm
Myocardial contusionMyocardial contusion
Myocardial contusionMyocardial contusion
-
7/29/2019 Chest Trauma Basics
110/151
Myocardial contusionMyocardial contusionMyocardial
contusionMyocardial contusion
Myocardial contusionMyocardial contusion
Myocardial contusionMyocardial contusion
-
7/29/2019 Chest Trauma Basics
111/151
Myocardial contusionMyocardial contusionMyocardial
contusionMyocardial contusion
Also may see:
myocardial concussion stunned
myocardium with no cell death coronary artery laceration
Diagnosis by:
trans-esophageal echocardiogram (TEE)
serial cardiac enzymes / markers
Also may see:
myocardial concussion stunned
myocardium with no cell death coronary artery laceration
Diagnosis by:
trans-esophageal echocardiogram (TEE)
serial cardiac enzymes / markers
Myocardial contusionMyocardial contusion
Myocardial contusionMyocardial contusion
-
7/29/2019 Chest Trauma Basics
112/151
Myocardial contusionMyocardial contusionMyocardial
contusionMyocardial contusion
Question: Does it matter?
New nomenclature: Anterior Chest Wall
Syndrome
Question: Does it matter?
New nomenclature: Anterior Chest Wall
Syndrome
-
7/29/2019 Chest Trauma Basics
113/151
-
7/29/2019 Chest Trauma Basics
114/151
Traumatic aortic ruptureTraumatic aortic rupture
Traumatic aortic ruptureTraumatic aortic rupture
-
7/29/2019 Chest Trauma Basics
115/151
Traumatic aortic ruptureTraumatic aortic ruptureTraumatic aortic
ruptureTraumatic aortic rupture
90% or more dead at scene
90% mortality each undiagnosed day
Must have high index of suspicion
Disruption occurs at ligamentumarteriosum (ductus
arteriosus)
Contained hematoma of 500 to 1000 mlof blood
90% or more dead at scene
90% mortality each undiagnosed day
Must have high index of suspicion
Disruption occurs at ligamentumarteriosum (ductus
arteriosus)
Contained hematoma of 500 to 1000 mlof blood
Traumatic aortic ruptureTraumatic aortic rupture
Traumatic aortic ruptureTraumatic aortic rupture
-
7/29/2019 Chest Trauma Basics
116/151
Traumatic aortic ruptureTraumatic aortic ruptureTraumatic aortic
ruptureTraumatic aortic rupture
Radiographic signs
Wide mediastinum
(>8cm) Fractured 1st & 2nd rib
Obliterated aorticknob
Trachea deviated toright
Pleural cap
Radiographic signs
Wide mediastinum
(>8cm) Fractured 1st & 2nd rib
Obliterated aorticknob
Trachea deviated toright
Pleural cap
Elevated mainstembronchus with shift toright
Obliterated aorticwindow
Esophagus shifted to
right (NG at T4) Depressed left
mainstem bronchus
Elevated mainstembronchus with shift toright
Obliterated aorticwindow
Esophagus shifted to
right (NG at T4) Depressed left
mainstem bronchus
-
7/29/2019 Chest Trauma Basics
117/151
-
7/29/2019 Chest Trauma Basics
118/151
-
7/29/2019 Chest Trauma Basics
119/151
dye leakage
Traumatic aortic ruptureTraumatic aortic rupture
Traumatic aortic ruptureTraumatic aortic rupture
-
7/29/2019 Chest Trauma Basics
120/151
Traumatic aortic ruptureTraumatic aortic ruptureTraumatic aortic
ruptureTraumatic aortic rupture
CT becoming imaging of choice
Must know site!
NPV of normal chest x-ray (good quality,upright): 98% (CT will
find mediastinalhemorrhage in 3%, TAR in 0.4%)
78% of patients with post-traumatic widemediastinum on chest
film have normalCT
CT becoming imaging of choice
Must know site!
NPV of normal chest x-ray (good quality,upright): 98% (CT will
find mediastinalhemorrhage in 3%, TAR in 0.4%)
78% of patients with post-traumatic widemediastinum on chest
film have normalCT
Traumatic aortic ruptureTraumatic aortic rupture
Traumatic aortic ruptureTraumatic aortic rupture
-
7/29/2019 Chest Trauma Basics
121/151
Traumatic aortic ruptureTraumatic aortic ruptureTraumatic aortic
ruptureTraumatic aortic rupture
Treatment -SURGICAL REPAIR
Treatment -SURGICAL REPAIR
-
7/29/2019 Chest Trauma Basics
122/151
Traumatic diaphragmatic ruptureTraumatic diaphragmatic
rupture
Traumatic diaphragmatic ruptureTraumatic diaphragmatic
rupture
-
7/29/2019 Chest Trauma Basics
123/151
Traumatic diaphragmatic ruptureTraumatic diaphragmatic
ruptureTraumatic diaphragmatic ruptureTraumatic diaphragmatic
rupture
Blunt trauma: tears leading to immediateherniation
Penetrating trauma: small tears whichmay take years to develop
herniation
Usually on left side
Blunt trauma: tears leading to immediateherniation
Penetrating trauma: small tears whichmay take years to develop
herniation
Usually on left side
-
7/29/2019 Chest Trauma Basics
124/151
Traumatic diaphragmatic ruptureTraumatic diaphragmatic
rupture
Traumatic diaphragmatic ruptureTraumatic diaphragmatic
rupture
-
7/29/2019 Chest Trauma Basics
125/151
Traumatic diaphragmatic ruptureTraumatic diaphragmatic
ruptureTraumatic diaphragmatic ruptureau at c d ap ag at c uptu
e
Treatment: surgical repair Treatment: surgical repair
Tracheobronchial tree injuryTracheobronchial tree injury
Tracheobronchial tree injuryTracheobronchial tree injury
-
7/29/2019 Chest Trauma Basics
126/151
Tracheobronchial tree injuryTracheobronchial tree
injuryTracheobronchial tree injuryTracheobronchial tree injury
Larynx - rare
Hoarseness
Subcutaneous emphysema
Palpable crepitus
Intubation may be difficult: tracheostomy
(not cricothyroidotomy) is treatment ofchoice
Larynx - rare
Hoarseness
Subcutaneous emphysema
Palpable crepitus
Intubation may be difficult: tracheostomy
(not cricothyroidotomy) is treatment ofchoice
Tracheobronchial tree injuryTracheobronchial tree injury
Tracheobronchial tree injuryTracheobronchial tree injury
-
7/29/2019 Chest Trauma Basics
127/151
Tracheobronchial tree injuryTracheobronchial tree
injuryTracheobronchial tree injuryTracheobronchial tree injury
Trachea
Blunt or penetrating
Esophagus, carotidartery and jugular
vein may be involved
Noisy breathing partial airway
obstruction
Trachea
Blunt or penetrating
Esophagus, carotidartery and jugular
vein may be involved
Noisy breathing partial airway
obstruction
Tracheobronchial tree injuryTracheobronchial tree injury
Tracheobronchial tree injuryTracheobronchial tree injury
-
7/29/2019 Chest Trauma Basics
128/151
Tracheobronchial tree injuryTracheobronchial tree
injuryTracheobronchial tree injuryTracheobronchial tree injury
Bronchus
1.5% blunt chest
trauma 80% due to
BLUNT trauma
within one inch ofcarina (tethered)
Bronchus
1.5% blunt chest
trauma 80% due to
BLUNT trauma
within one inch ofcarina (tethered)
Esophageal traumaEsophageal trauma
Esophageal traumaEsophageal trauma
-
7/29/2019 Chest Trauma Basics
129/151
Esophageal traumaEsophageal traumaEsophageal traumaEsophageal
trauma
Penetrating > blunt
Lethal if not recognized
High suspicion if
left pneumothorax and hemothoraxwithout rib fracture
shock out of proportion to apparent bluntchest trauma
particulate matter in chest tube
Penetrating > blunt
Lethal if not recognized
High suspicion if
left pneumothorax and hemothoraxwithout rib fracture
shock out of proportion to apparent bluntchest trauma
particulate matter in chest tube
Esophageal traumaEsophageal trauma
Esophageal traumaEsophageal trauma
-
7/29/2019 Chest Trauma Basics
130/151
Esophageal traumaEsophageal traumaEsophageal traumasop agea t au
a
Esophageal traumaEsophageal trauma
Esophageal traumaEsophageal trauma
-
7/29/2019 Chest Trauma Basics
131/151
Esophageal traumasop agea t au aEsophageal traumap g
Blunt trauma,most tears
superiorIf low esophagus leakage ofstomach contentsinto
mediastinum
Blunt trauma,most tears
superiorIf low esophagus leakage of
stomach contentsinto mediastinum
-
7/29/2019 Chest Trauma Basics
132/151
6 Other Frequent Injuries6 Other Frequent Injuries
6 Other Frequent Injuries6 Other Frequent Injuries
-
7/29/2019 Chest Trauma Basics
133/151
6 Other Frequent Injuriesq j6 Ot e eque t ju esq j
Subcutaneous emphysema
Traumatic asphyxia
Simple pneumothorax
Hemothorax
Scapula fracture Rib fractures
Subcutaneous emphysema
Traumatic asphyxia
Simple pneumothorax
Hemothorax
Scapula fracture Rib fractures
-
7/29/2019 Chest Trauma Basics
134/151
Subcutaneous emphysemaSubcutaneous emphysema
Subcutaneous emphysemaSubcutaneous emphysema
-
7/29/2019 Chest Trauma Basics
135/151
ub u a ou p y ap yp yp y
Rice Krispies
May result from
airway injury lung injury
blast injury
No treatmentrequired address underlying problem
Rice Krispies
May result from
airway injury lung injury
blast injury
No treatmentrequired address underlying problem
-
7/29/2019 Chest Trauma Basics
136/151
-
7/29/2019 Chest Trauma Basics
137/151
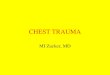
Traumatic asphyxiaTraumatic asphyxia
Traumatic asphyxiaTraumatic asphyxia
-
7/29/2019 Chest Trauma Basics
138/151
p yp yp yp y
Purple face fromextravasation of blood
(Masqueecchymotique)
Major damage is to
underlying structures Purple face fades over
time in survivors
Purple face fromextravasation of blood
(Masqueecchymotique)
Major damage is to
underlying structures Purple face fades over
time in survivors
-
7/29/2019 Chest Trauma Basics
139/151
Simple pneumothoraxSimple pneumothorax
Simple pneumothoraxSimple pneumothorax
-
7/29/2019 Chest Trauma Basics
140/151
p pp pp pp p
Air enters potential space betweenvisceral and parietal
pleura
Breath sounds down on affected side Percussion
hyper-resonance
Treatment: chest tube in 4th or 5th
intercostal space anterior to mid-axillaryline
Air enters potential space betweenvisceral and parietal
pleura
Breath sounds down on affected side Percussion
hyper-resonance
Treatment: chest tube in 4th or 5th
intercostal space anterior to mid-axillaryline
-
7/29/2019 Chest Trauma Basics
141/151
Medialpneumothorax
-
7/29/2019 Chest Trauma Basics
142/151
Pocket shooter
-
7/29/2019 Chest Trauma Basics
143/151
HemothoraxHemothorax
HemothoraxHemothorax
-
7/29/2019 Chest Trauma Basics
144/151
Lacerated lung OR disrupted intercostalartery or internal
mammary artery
Most are self-limiting Surgical consultation if
initial drainage of >20 cc/kg (~1500 cc)
continued flow of >200 cc/hr
Lacerated lung OR disrupted intercostalartery or internal
mammary artery
Most are self-limiting Surgical consultation if
initial drainage of >20 cc/kg (~1500 cc)
continued flow of >200 cc/hr
-
7/29/2019 Chest Trauma Basics
145/151
Scapula fracturesScapula fractures
Scapula fracturesScapula fractures
-
7/29/2019 Chest Trauma Basics
146/151
p
Fractured scapulaor 1st & 2nd ribs
indicates majormechanism ofinjury; consider
underlyingdamage
Fractured scapulaor 1st & 2nd ribs
indicates majormechanism ofinjury; consider
underlyingdamage
Rib fracturesRib fractures
Rib fracturesRib fractures
-
7/29/2019 Chest Trauma Basics
147/151
Most frequent thoracic cage injury
Most commonly injured: 4th 9th
If 10th/ 11th/ 12th suspect liver or spleeninjury
If 1st/ 2nd/ 3rdworry about injury to head,
neck, spinal cords, lungs, great vessels
Most frequent thoracic cage injury
Most commonly injured: 4th 9th
If 10th/ 11th/ 12th suspect liver or spleeninjury
If 1st/ 2nd/ 3rdworry about injury to head,
neck, spinal cords, lungs, great vessels
Rib fractures treatmentRib fractures treatment
Rib fractures treatmentRib fractures treatment
-
7/29/2019 Chest Trauma Basics
148/151
Intercostal blocks
Epidural anesthesia
Systemic analgesicsDo not use
taping
rib belts
external splints
Intercostal blocks
Epidural anesthesia
Systemic analgesicsDo not use
taping
rib belts
external splints
Rib fracturesRib fractures
Rib fracturesRib fractures
-
7/29/2019 Chest Trauma Basics
149/151
Ribs x-rays
are expensive
are inaccurate for diagnosis (~50%sensitivity)
add nothing to treatment
require painful positioning of the patient
are, in general, not useful
Ribs x-rays
are expensive
are inaccurate for diagnosis (~50%sensitivity)
add nothing to treatment
require painful positioning of the patient
are, in general, not useful
In conclusion...In conclusion...
In conclusion...In conclusion...
-
7/29/2019 Chest Trauma Basics
150/151
Chest trauma is common in themultiply-injured patient
Most conditions can be treated by theevaluating physician and do
notrequire emergent thoracotomy
Airway management and ajudiciously placed needle can savemany
lives
Chest trauma is common in themultiply-injured patient
Most conditions can be treated by theevaluating physician and do
notrequire emergent thoracotomy
Airway management and ajudiciously placed needle can savemany
lives
Next timeNext time
Next timeNext time
-
7/29/2019 Chest Trauma Basics
151/151
February 27th, 2004February 27th, 2004
RespiratoryRespiratoryEmergenciesEmergencies
Joe LexJoe Lex
February 27th, 2004February 27th, 2004
RespiratoryRespiratoryEmergenciesEmergencies
Joe LexJoe Lex