Embed Size (px)
Citation preview

Original Article : Children of Mothers in Psychiatric Hospital
Children of Mothers Admitted
to Psychiatric Hospital: Care
Arrangements and Mothers’
Perceptions
Judi Cunningham, Femi Oyebode & Panos Vostanis
This paper describes the care arrangements made for children when their
mothers are admitted to psychiatric hospital. It also describes at admission,
and at 3 months follow-up, the views and opinions of mothers and carers
with regard to the admission, its impact on the family, and the service
received. It was found that children are predominantly cared for within
their family when their mother is admitted to hospital, and that mothers
and carers are concerned about the impact of the admission and its
associated problems.
Keywords: Care arrangements; mental health problems; carers ; psychiatric admission
Introduction
It is widely accepted that the children of psychiatrically ill
parents are at greater risk of developing psychiatric, social
and educational problems themselves (e.g., Rutter &
Quinton, 1984). There are many pathways through which
mental illness may impact upon children, including
indirectly through marital discord, social adversity and
multiple changes in care-takers (Oates, 1997).
Very little is known about the care arrangements for
children when women are taken into hospital, despite the
Department of Health highlighting the ‘significance and
effect of parental mental health problems on children’
(Department of Health, 1997). Hatfield, Webster and
Mohamad (1997) report that just over half of all psy-
chiatric admission episodes involve women (Department
of Health, 1995) but information on parental status does
not seem to be routinely recorded (Stormont et al., 1997).
Once psychiatric patients are recognised as parents and
part of a family unit, it is important that the impact of
their situation is considered.
Research specifically looking at the care arrangements for
children of hospitalised parents with mental health
problems has only just begun. A study by Stormont and
her colleagues (1997) documents that 9 out of 12 inter-
viewed parents taken into psychiatric hospital had chil-
dren temporarily looked after by family members, with
the rest being taken into care. Hawes and Cottrell (1999)
showed that, in their sample, 12 out of 53 children had to
move house as a result of their mother’s psychiatric
admission.
As admission to hospital is a regular occurrence for some
who have mental health problems, it has been suggested
that the patient who is also a parent should always be
asked about the effects of their illness on the children, with
the best interests of the child a priority (Oates, 1997).
Work has recently begun in this area, with Stormont et al.
(1997) showing that hospitalised parents do not readily
accept that their children have problems. However, 14 of
the 19 parents interviewed did express concern about the
impact of their illness on their children. A recent study
by Tamarit and Yin-Har Lau (1999) has also emphasised
that the children of psychiatrically ill mothers do not
receive the attention they need.
This study intended to replicate and extend the important
work begun by these researchers. Our aims were threefold.
First, to describe the care arrangements for children when
a mother is admitted to psychiatric hospital. Second, to
investigate the views and opinions of mothers and carers
regarding the admission itself, its emotional and economic
impact on all concerned, both at the time of admission,
and 3 months afterwards. Third, to record the evaluation
Judi Cunningham
School of Psychology,
University of
Birmingham,
Edgbaston, Birmingham
B15 2TT
Femi Oyebode
Trust Headquarters,
South Birmingham
Mental Health (NHS)
Trust, Vincent Drive,
Edgbaston, Birmingham
B15 2TZ
Panos Vostanis
Greenwood Institute of
Child Health, Westcotes
House, Westcotes
Drive, Leicester
LE3 0QU
Child Psychology & Psychiatry Review Volume 5, No. 3, 2000114

Original Article : Children of Mothers in Psychiatric Hospital
of both mothers and carers with regard to the service they
had received.
Method
The study was of longitudinal design. Recruitment was
from the Queen Elizabeth Psychiatric Hospital in South
Birmingham. During a 12-month period, mothers were
identified with children aged between 2 and 12 years.
Mothers were visited as soon as possible after their
admission to hospital, and asked whether they would
participate in the study. Recruitment was on a consecutive
basis, with some exceptions. Some mothers were missed
by the recruitment because they had stayed in hospital
overnight, or just for a weekend. Other women were
judged by the ward staff to be too distressed to take part
in the study. Mothers were given the Brief Symptom
Inventory (Derogatis, 1993), and interviewed with a semi-
structured interview specifically designed for the purpose.
Permission was asked from the mother to contact the
carer for her children. The carer was contacted and visited,
where possible, whilst the mother was still in hospital. The
carer participated in a semi-structured interview similar in
content to that conducted with the mothers, and com-
pleted the Child Behavior Checklist (Achenbach, 1991)
for each childwithin the age-range specified.Demographic
data were also collected.
Approximately 3 months after the mother was discharged
from hospital, both the mother and carer were contacted
and visited at home. Both the mother and the carer were
interviewed again; the mother completed the Brief Symp-
tom Inventory, and both mother and carer completed the
Child Behavior Checklist for each child within the age
range.
Subjects
Inclusion criteria
Mothers with children aged between 2 and 12 years
admitted to the Queen Elizabeth Psychiatric Hospital.
Mothers must have had their children resident with them
before the time of admission.
Mothers
Forty-two women fitting inclusion criteria were
approached and asked to participate in the study. Of
these, 13 women (31%) refused participation. Twenty-
nine women completed the initial part of the study.
Mothers had a mean age of 34 years (range: 20–49 years)
and had, on average, three children (range: 1–5). Women
were predominantly white (69%) and unemployed (83%),
although many of the women had young children at home.
Seventeen mothers (59%) were living with a partner at the
time of the admission. Mothers were seen, on average, 11
days after their admission to hospital (range: 0–28 days).
Seventeen of the 29 mothers (59%) completed the follow-
up. Mothers were predominantly diagnosed with a de-
pressive disorder (34%). Five women (17%) were diag-
nosed with bipolar disorders, five with schizophrenia and
other psychotic disorders, one with an alcohol related
disorder, one with an anxiety disorder, and seven (24%)
were unclassified.
Children
The cohort of 29 mothers had, between them, 76 offspring
of all ages. Only children between the ages of 2 and 12
years were included in the study, and these children
numbered 48: 24 female and 24 male. The mean age of the
children was 6 years. Children had a maximum of four
siblings. There were three children with no siblings in the
study, and two children who had adult siblings.
Carers
Of the 29 mothers involved in the study, six (29%) asked
for the carer of their children not to be contacted and six
carers could not be located. The remaining 17 carers were
asked to participate. Of these, 3 (18%) refused par-
ticipation, 14 (82%) completed the first part of the study,
and 11 (69%–one carer had died during the study)
completed the follow-up.
Measures
Mother
The Brief Symptom Inventory (Derogatis, 1993) is a 53-
item self-report questionnaire, designed to reflect current
psychological symptom patterns of psychiatric and medi-
cal patients. Each item is rated on a 5-point Likert scale
of distress from ‘not at all ’ (0) to ‘extremely’ (4).
Standardised T scores above 63 on any index indicates
‘caseness ’. The questionnaire yields nine primary symp-
tom dimensions, and three global indices. The Global
Symptom Inventory, an overall score, was used for this
study. The measure is sensitive to change and can be used
to measure patient progress. The measure is both reliable
and valid (Derogatis, 1993).
The initial qualitative interview and checklist was designed
to investigate the mother’s feelings towards her children
and her partner (if applicable) with regard to her ad-
mission to hospital. The interview also asked about the
care arrangements currently made for the children. Pre-
vious admission and demographic data were collected by
interviewing the mother, and through investigation of
hospital records.
The follow-up interview had a similar structure to the
initial interview, but emphasis was placed on the mother’s
opinion of the help and support she had received, and how
this could have been improved.
Children
The Child Behavior Checklist (CBCL) (Achenbach, 1991)
is a well-used instrument that comprises 113 behaviour
problem items that respondents score as 0 for ‘not true of
Child Psychology & Psychiatry Review Volume 5, No. 3, 2000 115
Original Article : Children of Mothers in Psychiatric Hospital
the child’, 1 for ‘somewhat or sometimes true of the
child’, and 2 for ‘very true or often true of the child’.
Scores are transferred to a behavioural profile designed to
score on syndromes derived from factor analysis. Narrow
band-like syndromes are grouped under ‘ internalising’,
‘externalising’ and ‘other ’ problems. The measure yields
a total T score, which was used for this study. Reliability
for this instrument is good (Edelbrock & Achenbach,
1980). The clinical threshold for this measure is a
standardised T score of between 60 and 63.
Results
Child-care arrangements
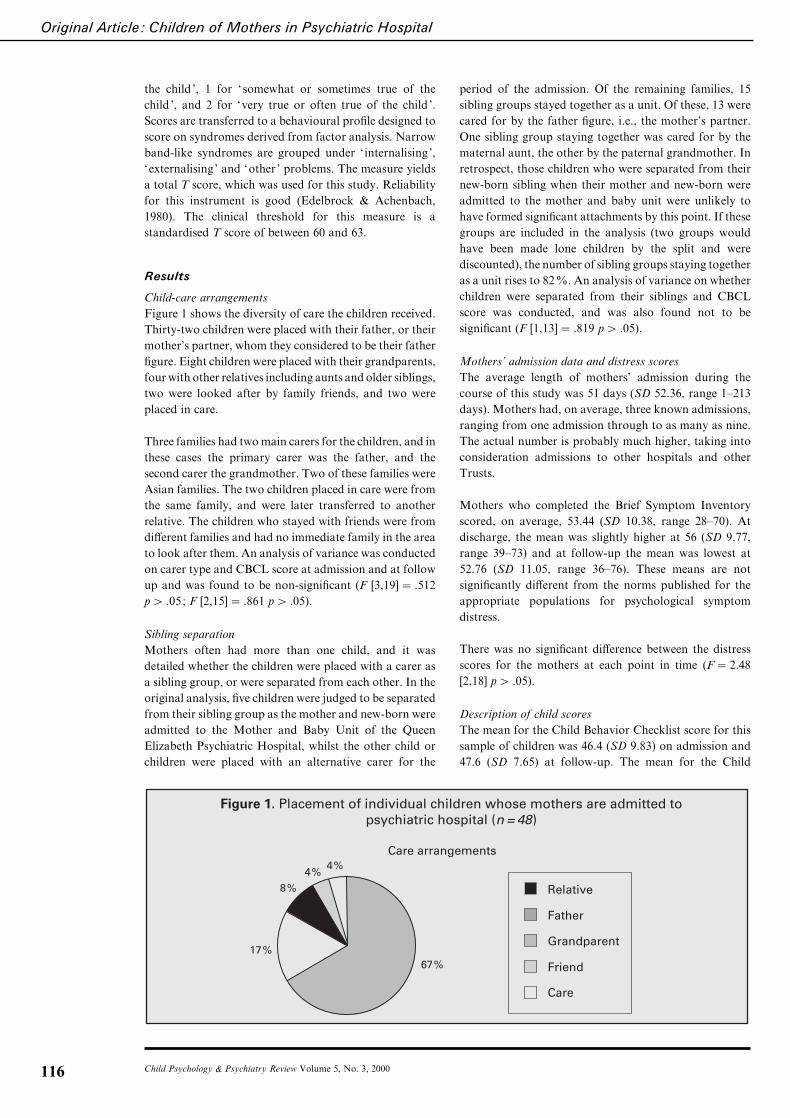
Figure 1 shows the diversity of care the children received.
Thirty-two children were placed with their father, or their
mother’s partner, whom they considered to be their father
figure. Eight children were placed with their grandparents,
fourwith other relatives including aunts and older siblings,
two were looked after by family friends, and two were
placed in care.
Three families had two main carers for the children, and in
these cases the primary carer was the father, and the
second carer the grandmother. Two of these families were
Asian families. The two children placed in care were from
the same family, and were later transferred to another
relative. The children who stayed with friends were from
different families and had no immediate family in the area
to look after them. An analysis of variance was conducted
on carer type and CBCL score at admission and at follow
up and was found to be non-significant (F [3,19]¯ .512
p" .05; F [2,15]¯ .861 p" .05).
Sibling separation
Mothers often had more than one child, and it was
detailed whether the children were placed with a carer as
a sibling group, or were separated from each other. In the
original analysis, five children were judged to be separated
from their sibling group as the mother and new-born were
admitted to the Mother and Baby Unit of the Queen
Elizabeth Psychiatric Hospital, whilst the other child or
children were placed with an alternative carer for the
Father
Grandparent
Relative
Friend
Care
Figure 1. Placement of individual children whose mothers are admitted topsychiatric hospital (n = 48)
4%4%
8%
17%67%
Care arrangements
period of the admission. Of the remaining families, 15
sibling groups stayed together as a unit. Of these, 13 were
cared for by the father figure, i.e., the mother’s partner.
One sibling group staying together was cared for by the
maternal aunt, the other by the paternal grandmother. In
retrospect, those children who were separated from their
new-born sibling when their mother and new-born were
admitted to the mother and baby unit were unlikely to
have formed significant attachments by this point. If these
groups are included in the analysis (two groups would
have been made lone children by the split and were
discounted), the number of sibling groups staying together
as a unit rises to 82%. An analysis of variance on whether
children were separated from their siblings and CBCL
score was conducted, and was also found not to be
significant (F [1,13]¯ .819 p" .05).
Mothers’ admission data and distress scores
The average length of mothers’ admission during the
course of this study was 51 days (SD 52.36, range 1–213
days). Mothers had, on average, three known admissions,
ranging from one admission through to as many as nine.
The actual number is probably much higher, taking into
consideration admissions to other hospitals and other
Trusts.
Mothers who completed the Brief Symptom Inventory
scored, on average, 53.44 (SD 10.38, range 28–70). At
discharge, the mean was slightly higher at 56 (SD 9.77,
range 39–73) and at follow-up the mean was lowest at
52.76 (SD 11.05, range 36–76). These means are not
significantly different from the norms published for the
appropriate populations for psychological symptom
distress.
There was no significant difference between the distress
scores for the mothers at each point in time (F¯ 2.48
[2,18] p" .05).
Description of child scores
The mean for the Child Behavior Checklist score for this
sample of children was 46.4 (SD 9.83) on admission and
47.6 (SD 7.65) at follow-up. The mean for the Child
Child Psychology & Psychiatry Review Volume 5, No. 3, 2000116
Original Article : Children of Mothers in Psychiatric Hospital
Behavior Checklist as scored by the mothers was 52 (SD
10.77). The means for the non-referred population are 50
(SD 9.8) for boys and 50.1 (SD 9.9) for girls. This sample
does not differ significantly from the non-referred popu-
lation. Children did not score differently between ad-
mission and follow-up (t¯ .27, df¯ 13, p" .05) and
scores from the carers and the mothers also do not differ
significantly (t¯ 1.44, df¯ 36, p" .05). Mothers and
carers seem to have the same perceptions of the child’s
problem behaviours.
Factors associated with severity of children’s problems
It was hypothesised that factors such as mother’s distress,
admission length, and number of admissions may ad-
versely affect the children of mothers who are admitted to
hospital.However, children’s scores on theChild Behavior
Checklist were shown not to be associated with either the
length of the mother’s admission, nor the number of
admissions she had had in their lifetime. It seems that
children are not experiencing problems as measured by the
Child Behavior Checklist, and it could be suggested that
children being cared for by their immediate family have
attachment relationships that buffer the stress associated
with a mother’s hospital admission.
Description of children who experienced problems
Only one child was scored above the clinical threshold (T
¯ 63) by the carer on the Child Behavior Checklist whilst
the mother was in hospital. This child had reported
problems at school, with work stress and problems with
bullying, but the mother’s severity score was relatively
low (T¯ 48). At follow-up, this child’s score on the Child
Behavior Checklist had lowered to T¯ 57 from the carer
and T¯ 48 from the mother. The child’s school problems
had also significantly improved according to the parents.
One child scored T¯ 60 on the Child Behavior Checklist
whilst the mother was in hospital : a ‘borderline’ score.
During the interview, the carer of this child had also
reported problems, for example that the child was jealous
of younger siblings who were with the mother in hospital.
Unfortunately, no follow-up data are available for
this child.
At follow-up, two children from the same family were
scored by the mother well above the clinical threshold on
the Child Behavior Checklist (T¯ 76 and T¯ 75). The
mother reported in her interview that the children were
experiencing behavioural problems. The mother’s scores
were again relatively low on the Brief Symptom Inventory.
One child at follow-up was scored on the borderline (T¯60) by the carer.
It is interesting to note that in cases where children were
scored above the clinical threshold, there had been a
significant domestic problem between the mother and her
partner, and it was suggested by one mother that the
children were affected by the compound stressors of
marital disharmony and hospital admission. This sugges-
tion is supported by the literature, which cites family
disruption and marital disharmony as two major risk
factors in the development of problems in children (Rutter
& Quinton, 1984).
Views and opinions of mothers
On admission, all mothers were asked a series of questions.
One of these questions was ‘do your children know where
you are? ’ Twenty-four mothers (83%) said their children
did know where they were, and three (10%) specified that
their children knew they were in hospital, but were
unaware of the reason. One mother said that some of her
children (the older children) knew that she was in hospital,
but that her younger child did not. Only one mother said
that her children did not know where she was. When asked
whether or not the mothers were worried about their
children, 17 (59%) expressed that they were. Eleven
(38%) said they were not worried about their children,
and only one mother stated that she did not feel anything
at all about her children.
Seventeen of the mothers were given a forced choice
question on how they felt about their children. The options
were that they were worried about them, that they missed
them, that they loved them, or a combination. Fourteen
(82%) of these mothers expressed that they loved their
children. Only three mothers did not take this option. The
remaining 12 mothers were given an open-ended question:
‘how do you feel about your children?’ One mother stated
that she ‘wanted her children back’, one mother expressed
sadness, and four mothers said that they felt that their
children were OK and being well looked after. Of all the
mothers, 21 (72%) expressed that they missed their
children, with somewhat melancholy overtones, such as, ‘ I
really feel that they are better off without me’.
During the follow-up interview, mothers were asked
whether they had been readmitted in the intervening
period. Eleven mothers (65%) had been readmitted and
six had not. At the time of the follow-up interview all the
mothers except one now had full-time care of their
children. When asked what problems they had en-
countered since their discharge from hospital, six women
(35%) stated that they had had no problems. Of the
others, mothers experienced problems with money, and
with medication – forgetting to take it and experiencing
unpleasant side effects. Four women had experienced
behavioural problems with their children. Some women
reported general problems: ‘It’s such a huge effort to do
anything’.
On the question of mental health support, only three
mothers (18%) said they had received no support since
leaving hospital. Five women stated that their Community
Psychiatric Nurse was their main source of support since
being discharged, three mentioned social service support,
three were attending clinics or receiving outreach support,
and two received support from their families. One mother
said that her main sources of support were her consultant
Child Psychology & Psychiatry Review Volume 5, No. 3, 2000 117

Original Article : Children of Mothers in Psychiatric Hospital
and her chaplain. When asked about the sources of
support with looking after the children, six mothers said
that their families had been extremely helpful ; four
mothers said they had received help from social workers
and health visitors ; two said they received help from
schools and nurseries, five said that they had received no
support, and two mothers stated they had not needed
any help.
Mothers were also asked about their concerns, both for
their health and for their children. On the question of
health, only one mother stated that she had no concerns.
The longevity of mental illness was a recurrent theme for
many of the mothers, with comments such as: ‘ It seems to
be taking a long time to get back to normal ’. Some
mothers were concerned that their illness was affecting the
children, not only because of their admission, but also
because of the effects of seeing their mother when she was
ill. Mothers were also concerned that they were inadequate
as parents, blaming themselves for their family’s concerns:
‘ I feel as if I’m bringing devastation on my family ’.
When asked about improving the service they had had,
mothers were generally positive about their experiences ;
in fact, six mothers (35%) said they would not change or
improve upon the service they received. Generally, treat-
ment and care within the hospital was reported favour-
ably, with problems only arising with evaluation of the
transition from hospital to home. Mothers talked of
needing help with ‘everyday things ’. A strong theme was
a feeling of isolation when returning home, needing
someone to talk to or a day centre to maintain links with
those they had met whilst in hospital : ‘ I’d like somewhere
to mix with others like me’.
Mothers also expressed that they were worried about their
children visiting them in hospital, concerned that the ward
was not a suitable environment for children. A solution
was suggested in the form of a family room staffed by
nurses, where children could visit their parents without
having to enter the ward area. Other suggestions were that
there should be a checklist on admission to record whether
or not the client has children, and what provisions are
being made for them.
Views and opinions of carers
Carers were interviewed during the mother’s admission to
hospital, and also 3 months after the mother’s discharge.
Carers expressed a number of concerns, which ranged in
type from emotional to financial burden. Over half the
carers said that the admission had affected them econ-
omically.
The majority of carers admitted that the mother’s ad-
mission had affected them emotionally. Only one carer felt
that the mother’s admission to hospital was a relief, and
two carers said that the admission wasn’t long enough to
cause them or the children any real upset. However, it
seems those most affected are carers who are emotionally
involved with both the children and the mother, such as
parents and partners, and where the condition is chronic.
Even those who had said the admission had not affected
them emotionally expressed some concern at the follow-
up interviews. One carer stated: ‘ I didn’t think it had
(affected me) at the time, but I felt low afterwards,
drained…I couldn’t do any more’.
Eight carers also said that the admission had affected them
socially, and that they didn’t go out as much as they used
to: ‘ I don’t go out – I like to be in for the children…people
don’t come round anymore’. Seven (64%) of the carers
said they thought that the mother’s admission was
affecting the children emotionally, although only one
carer reported any school problems. Younger children
seem to be the most affected according to the carers, with
heavy emphasis on the effect the illness was having on
attachment: ‘ It’s bad, he doesn’t go to her when she calls,
and then she gets upset ’. ‘He’s not as secure – I think he
misses her ’. Even those carers who said that they thought
the children weren’t emotionally affected had reservations.
One carer said: ‘They’ve adjusted to it. They were (upset)
at the beginning, it was very traumatic. Now that’s gone
and they’re hardened to it…maybe too hard’.
During the follow-up interviews, carers were asked how
they would improve the service they and the mother had
received. Their answers reflect the pattern of answers
given by the mothers, often giving the impression that
carers feel that they are alone with the responsibilities of
looking after both mother and children. Carers also said
that they understood that help was available, but didn’t
know where or how to access it. They called for an
increase in the availability of all types of information,
including financial and emotional support and the location
of support groups.
Discussion
Our sample for this study was relatively small, especially
in the follow-up stage, and for this reason we must be
cautious in drawing firm conclusions. The voluntary
nature of the study meant that those families particularly
at risk may have been those who refused participation.
Selection criteria may have also biased results, as selection
was made on the basis of discretion by the ward staff. In a
study of this nature, it is important not to compound
existing problems, and so those who were deemed too ill to
be interviewed were either excluded from the sample, or
interviewed when their symptoms had abated. Thus, the
sample was skewed in favour of those mothers whose
symptoms were mainly of moderate degree. Drop-out
rates were also quite high: only 17 of the original 29
mothers completed the follow-up. It is the case that, in
a sample of this nature, families tend to be highly mobile,
and some had moved by the follow-up stage. Some
mothers wanted to distance themselves from their illness
once discharged, and refused any further participation.
Although much of our reported data are anecdotal, we
Child Psychology & Psychiatry Review Volume 5, No. 3, 2000118

Original Article : Children of Mothers in Psychiatric Hospital
found it important to report the feelings of those con-
cerned. Many participants we interviewed stated that not
being listened to was one of their main grievances, and this
highlights further the need for this type of research.
Having acknowledged the methodological limitations,
however, some important themes emerged from our
research. The children in our sample were cared for very
much within the bounds of immediate family when their
mothers were admitted to hospital, and this echoes the
findings in previous research (Rice, Ekdahl, & Miller,
1971; Hawes & Cottrell, 1999). It seems that the families
of mothers admitted to psychiatric hospital are very
proficient in providing child-care arrangements. We must
bear in mind, however, that this sample came only from
hospital admissions, and a different picture may emerge
when examining the children of mothers cared for in the
community. Admission to hospital may be facilitated,
especially in a voluntary admission episode, where a
mother has a carer available to look after her children.
Also, as has already been suggested, those mothers who
did not agree to be interviewed may be those less secure
with their child-care arrangements, who may not have a
partner or family members to take care of their children.
Further studies should endeavour to report on this
‘missing’ population.
Despite the areas highlighted for concern, we feel that this
research has yielded positive results with regard to the
placement of children in a secure environment whilst their
mother is in hospital. The large proportion of children
staying with close relatives has implications for their
attachment status, with the traumatic effects of the
mother’s illness and its associated psychosocial problems
possibly being buffered by a secure attachment to an
alternative care-giver. Work is currently underway to
investigate the attachment status of these children.
Although children were cared for mostly within the family,
it remains clear from those we interviewed that mothers,
even at the peak of their own mental illness, are concerned
about their children’s welfare. Both mothers and carers
expressed anxiety about the effect illness and admission
may have on the children, and although complimentary
about the service provided by the hospital during the
admission, areas of concern arise with regard to the
transition from hospital to home, and the availability of
support information.
Although our sample was small, our investigation mirrors
other research in this area in that it highlights the need for
a formal set of guidelines to be implemented, making
practitioners and agencies aware of the larger sphere of
responsibility when a mother is admitted to hospital (e.g.,
Tamarit & Yin-Har Lau, 1999). Child and adult mental
health services are currently fragmented in many areas,
and this research shows that there is a need for joint
training within these services, with liaison between them a
priority. A multi-agency approach is called for to include
mothers, carers and children in achieving a care plan for
the family as an integrated unit, the whole of which is
affected by an admission to hospital.
Acknowledgements
The authors would like to thank the mothers and families
who participated in the study for their invaluable contri-
butions. We also would like to thank the staff of the Queen
Elizabeth Psychiatric Hospital, the Research and De-
velopment Unit, and particularly Mandy Dixon and
Emma Robertson for their help and support, as well as
peer reviewers for their comments on an earlier draft of
this paper. Lastly, we gratefully acknowledge the South
Birmingham Mental Health (NHS) Trust for providing
the funding for this research.
References
Achenbach, T. M. (1991). Manual for the Child Behavior
Checklist. Centre for Children, Youth and Families, University
of Vermont.
Department of Health Statistics Division (1995). Mental health in
England. London: Department of Health.
Department of Health (1997). Briefing paper for managers (23
January 1997). London: Department of Health.
Derogatis, L. R. (1993). Brief symptom inventory: Administration,
scoring and procedures manual. National Computers Systems
Inc.
Edelbrock, C., & Achenbach, T. M. (1980). A typology of child
behavior profile patterns: Distribution and correlates for
disturbed children aged 6–16. Journal of Abnormal Child
Psychology, 8, 441–470.
Hatfield, B., Webster, J., & Mohamad, H. (1997) Psychiatric
emergencies : Assessing parents of dependent children.
Psychiatric Bulletin, 21, 19–22.
Hawes, V., & Cottrell, D. (1999). Disruption of children’s lives by
maternal psychiatric admission. Psychiatric Bulletin, 23,
153–156.
Oates, M. (1997). Patients as parents : The risk to children. British
Journal of Psychiatry, 170 (suppl.32), 22–27.
Rice, E.P., Ekdahl, M.C., & Miller, L. (1971). Children of
mentally ill parents : Problems in child care. New York:
Behavioral Publications.
Rutter, M., & Quinton, D. (1984). Parental psychiatric disorder :
Effects on children. Psychological Medicine, 14, 853–880.
Stormont, F., Craig, T., Atakan, Z., Loader, P., & Williams, C.
(1997). Concerns about the children of psychiatric in-patients :
What the parents say. Psychiatric Bulletin, 21, 495–497.
Tamarit, L.M., & Yin-Har Lau, A. (1999). Children’s needs when
their mothers are admitted to psychiatric units. Psychiatric
Bulletin, 23, 214–217.
Child Psychology & Psychiatry Review Volume 5, No. 3, 2000 119
![MOTHERS WHO KILL: THE FORENSIC USE ... - Melbourne Law … · 2013] Mothers Who Kill: Evidence of Psychiatric Disorders 299 ally, it has been estimated that at least one in seven](https://img.pdfslide.net/doc/110x75/5f048c4a7e708231d40e838e/mothers-who-kill-the-forensic-use-melbourne-law-2013-mothers-who-kill-evidence.jpg)