-
Case presentationNICUPREPARED BY DR. MOHAMED DARDASAWIPediatric
resident, NPH
Supervised by Dr.Shireen Abed
-
Personal history Name: M H ALATARDate of birth : 30/11/2013 Date
of admission: 6/12/2013 (6 days)Address : Bit Lahia
-
Chief complaintPoor suckling , bluish discoloration of mucus
membranes , difficult of breathing since 2 days of age.
-
History of present illnessA 6 days male neonate presented to our
department with progressive dyspnea started at age of 2 days,
associated with cyanosis and poor suckling .
-
Perinatal history FT pregnancy, NSVDThe mother has been told 2
days before delivery that fetus has cardiac problem without
specific diagnosis.
-
Family history
healthy mother 33 years old Healthy father 34 years oldpositive
consanguinity 5 healthy siblings ( 2 sister and 3 brother )no
history of genetic , metabolic disorders or similar condition
-
PHYSICAL EXAMINATIONGeneral appearance :Lethargic , cyanosed ,in
respiratory distress
Vital sings :RR: 65 O2 Sat (room air): 65% HR: 70 -100Temp: 38 C
BP: unmeasurable ANTHROPOMETRICS: Weight: 3.5 kg , length 50 cm, HC
: 35 cm
-
Chest : RD II (tachypnea with subcostal and intercostal
retractions), decrease air entry bilateral , no added sounds
CVS: poor peripheral perfusion , weak pulses, very faint heart
sounds .
Abdomen : soft but distended with hepatomegaly (5cm below costal
margin)
CNS : lethargic, hypotonia with weak reflexes SKIN : olive green
jaundice
-
What is the diagnosis?
-
Provisional diagnosisA FT neonate with highly suspected CHD
antenatal diagnosis of cardiac problemRD and poor suckling since
2nd day of lifeEvident signs of hypoperfusion
-
laboratory investigationsABGs : PH 7.2 , PCO2 51, PO2 36 , sat
55%, HCO3 19, BE -9 CBC : Hb 15, WBC 14, PLT 63.000sugar 8 , ALT
396, AST 918, ALKP 438 , LDH 871 ,CHOL 91, TG 95, Ammonia 141
T.protein 7.3 , Albumin 3.5 , T.bil 21, D. bil 10 PT 40 ,INR 3 ,PTT
65 urea 130, CRE 0.8 , Uric acid 10 , Na 145, K 7.3 , Ca 7.4 ,Ph
7
-
Radiology Chest x ray: Cardiomegaly with bilateral lung
infiltrations.U/S Abdomen : hepatomegaly U/S brain : normal ECHO :
dilated Cardiomyopathy (secondary), normal heart structure ,
moderate contractility
-
Diagnosis
Cardiomyopathy complicated by: Heart failureHepatic failure
Acute kidney injury Suspected mitochondrial disorders
-
Management
Cardiorespiratory stabilization and support Keep on MV Dopamine
10 mic /kg/minDobutamine 10mic /kg/min monitoring blood
pressure
-
ManagementLiver support ADEK vitaminsUrsodeoxycholic acid Kept
initially NPO,TPN 1g/kg intralipid and 1g/kg aminosol Then given
pregestamil milkRandine , flagyl FFP
-
Management
Acute kidney injuryMeticulous attention to fluid
input/outputDrugs adjusted to GFR
-
ManagementOther lines of managementAntibiotics given empirically
to cover any possible sepsisRepeat blood transfusion as
neededSymptomatic management: phenobarbitone added for development
of seizures
-
Clinical course in NICUDay 2: Bad general condition HR 160 RR 50
BP 95/50 sat 95% on nasal O2Assessment :Heart failure with
cardiomyopathy( dobutamine) Liver failure AKI Convulsions add
luminal
-
Day 3: Still in bad general conditionDopamine 10 mic
/kg/minDobutamine 10 mic/kg/minPut on MCVStart TPN
-
Day 7 : CBC ; Hb 15, WBC 8, PLAT 116ABGs ; PH 7.5 , PCO2 48, PO2
37 , sat 74%, HCO3 37, BE 10 sugar 117 , ALT 46, AST 30, ALKP 438 ,
T. protein 7.3 , Albumin 3.5 , T.bil 25, D. bil 15 PT 22 ,INR 1.3
,PTT 46 urea 34, CRE 0,7 , Uric acid 2,4 , Na 145, K 4 , Ca 9 ,Ph
3,7Blood and urine culture : negative
-
Day 8 :Still in bad general condition Kidney function improved(
urea 54, crea 0,5)Still on MCV ( dopamine and dobutamine )TPNDay
18:Start weaning from MCVDopamine and dobutamine 5mic CVS :
irregular heart rate with bradycardia ECG was askedStart
pregestamil milk
-
Day 20:Stop TPN Extubation from MCVStop dopamine CBC ; Hb 13,
WBC 9,7 , PLAT 247ABGs ; PH 7,5 , PCO2 34, PO2 190 , sat 100%, HCO3
26, BE 4 (0N MCV)sugar 63 , urea 31, CRE 0,6 ,, Na 137, Cl 119, K 4
, Ca 10 , T.bil 12,5 D. bil 7,5
-
Day 22 :Stop dobutamine Start captoprilDay 25:Cholastasis
improved (T. bil 6 , D bil 4 )Lasix DigoxinStop phenobarbitoneDay
29:sugar 73 , urea 19, CRE 0,4 , T.bil 5 , D. bil 3,5T. protein 5 ,
Albumin 3
-
Further investigationsanti-SSA/Ro, anti-SSB/La were
negativeTORCH: was asked but not done
-
Our final diagnosisDilated
cardiomyopathyArrhythmiaCholestasis
Highly suspected IEM (Mitochondrial disorder)
-
Discharged to Rantisi Hospital after 31 days of admission On
moderate general condition HR 100 RR 59 BP 97/60 SAT 99% ( room
air)Digoxin 20 mic /12h poLasix 4mg /8h poCaptopril 1,5 mg /8h
Ursodeoxycholic acid 40mg /8h poAdol 2 drop /24 poVit k 2mg /24
po
-
What has been done in the referral hospital?Severe
cardiomyopathy AV block Sebrrhic dermatitis RSV
bronchiolitisAcintobacter central line colonization
-
Pacemaker insertionLasix 3 mg /24h Captopril 1.5 mg /12h
Spironolactone 12.5 mg /24h Carvedilol 1mg /24h Aquacream
emollitionOintment polycutan
-
Diagnosis CARDIOMYOPATHY COMPLICATED BY AV BLOCk , AKI and
CHOLESTASIS
-
NEONATAL CHOLESTASIS
-
DEFINITIONConjugated hyperbilirubinemia is defined as a
conjugated bilirubin concentration greater than 2 mg/dL or more
than 20% of total bilirubinProlonged elevation of the serum levels
of conjugated bilirubin beyond the 1st 14 days of life
-
ETIOLOGIESBasic distinction is between:Extrahepatic
etiologiesIntrahepatic etiologies
-
EXTRAHEPATIC ETIOLOGIESExtrahepatic biliary atresiaCholedochal
cystBile duct stenosisSpontaneous perforation of the bile
ductCholelithiasisInspissated bile/mucus plugExtrinsic compression
of the bile duct
-
INTRAHEPATIC
ETIOLOGIESIdiopathicToxicGenetic/ChromosomalInfectiousMetabolicMiscellaneous
-
INTRAHEPATIC ETIOLOGIESIdiopathic Neonatal
HepatitisToxicTPN-associated cholestasisDrug-induced
cholestasisGenetic/ChromosomalTrisomy 18Trisomy 21
-
INTRAHEPATIC ETIOLOGIESInfectiousBacterial sepsis (E. coli,
Listeriosis, Staph. aureus)TORCHSHepatitis B and
CVaricellaCoxsackie virusEcho virusTuberculosis
-
INTRAHEPATIC ETIOLOGIESMetabolicDisorders of Carbohydrate
MetabolismGalactosemiaFructosemiaGlycogen Storage Disease Type
IVDisorders of Amino Acid
MetabolismTyrosinemiaHypermethioninemia
-
INTRAHEPATIC ETIOLOGIESMetabolic (cont.)Disorders of Lipid
MetabolismNiemann-Pick diseaseWolman diseaseGaucher
diseaseCholesterol ester storage diseaseDisorders of Bile Acid
Metabolism3B-hydroxysteroid
dehydrogenase/isomeraseTrihydroxycoprostanic acidemia
-
INTRAHEPATIC ETIOLOGIESMetabolic (cont.)Peroxisomal
DisordersZellweger syndromeAdrenoleukodystrophyEndocrine
DisordersHypothyroidismIdiopathic hypopituitarism
-
INTRAHEPATIC ETIOLOGIESMetabolic (cont.)Miscellaneous Metabolic
DisordersAlpha-1-antitrypsin deficiencyCystic fibrosisNeonatal iron
storage diseaseNorth American Indian cholestasis
-
INTRAHEPATIC ETIOLOGIESMiscellaneousAlagille
syndromeNonsyndromic paucity of intrahepatic bile ductsCarolis
diseaseBylers diseaseCongenital hepatic fibrosis
-
COMMON ETIOLOGIESIdiopathic neonatal hepatitis
35-40%Extrahepatic biliary atresia 30%Alpha-1-antitrypsin
deficiency 5-10%Intrahepatic cholestasis syndromesPremature
infantsTPN-associatedSepsisDrug-induced
-
Treatable causes of cholestasisSepsisHypothyroidism or
hypopituitarism GalactosemiaExtrahepatic biliary atresia
-
Is there association between arrhythmia and cholestasis??
-
Neonatal cholestasis associated with arrhythmia
-
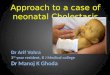
ECG showing third degree heart block with atrioventricular
dissociation and slow ventricular rate (atrial rate is 150,
ventricular rate is 85 bpm).
-
Congenital heart block Congenital heart block is a rare
disorder.It has an incidence of about 1 in 22,000 live births.
neonatal lupusstructural heart disease(L TGA, AV canal defects
)Many times, no clear etiology is determined for isolated CAVBThe
prognosis for congenital complete heart block is usually
favorable
-
THANK YOUIF YOU HAVE A PHOTO OF YOUR PATIENT, PUT IT HERE