Embed Size (px)
Citation preview
AMERICAN JOURNAL OF OPHTHALMOLOGY VOLUME 62 NOVEMBER, 1966 NUMBER 5
CHOROIDAL DETACHMENT AND RETINAL SURGERY
A CLINICAL AND EXPERIMENTAL STUDY
W. R. HAWKINS, M.D., AND C. L. SCHEPENS, M.D. Boston, Massachusetts
Choroidal detachment, in association with retinal surgery, results from either hemorrhagic1,2 or serous2'8 accumulation of fluid. The hemorrhagic process occurs during the operative procedure and presents as a rapidly forming elevation of the choroid. The serous effusion causes a more slowly developing detachment of the choroid that becomes clinically manifest during the postoperative period. Hemorrhagic and serous detachments of the choroid also occur in association with anterior segment surgery although the etiologic factors are somewhat different.4
The present study was undertaken to investigate the incidence, pathogenesis, and significance of choroidal detachment occurring in association with retinal detachment surgery. The report is divided into two sections, clinical and experimental.
CLINICAL STUDY
MATERIAL AND METHODS
Data were extracted from records of the Retina Associates and the Retina Service of the Massachusetts Eye and Ear Infirmary. Alphabetically consecutive records were reviewed of 1,500 patients who had undergone surgery for retinal detachment between
From the Department of Retina Research, Institute of Biological and Medical Sciences, Retina Foundation, and the Department of Ophthalmology, Massachusetts Eye and Ear Infirmary. This work was supported by a Public Health Service research grant B3489 of the National Institute of Neurological Diseases and Blindness, U. S. Public Health Service.
1961 and 1964. Only primary procedures were included. Details relating to the incidence of both hemorrhagic and serous detachment of the choroid were studied statistically. The findings were considered significant when the probability that they had occurred by chance was less than 5% ( P < 0 . 0 5 ) . Clinical features of choroidal detachment were abstracted from postoperative fundus sketches. These sketches were made by the surgeon following examination with an indirect stereoscopic ophthalmoscope. Complications resulting from detachment of the choroid, and their management, were also reviewed.
FINDINGS
Hemorrhagic detachment of the choroid. Among the 1,500 cases reviewed, subchoroi-dal hemorrhage occurred during the operative procedure in 15, an incidence of 1%. In all cases the hemorrhage followed the choroidal perforation and the acute hypotony associated with the release of subretinal fluid. The dark, convex elevation of the choroid was located in the same quadrant as the perforation site in 11 of the 15 cases (73%). However, external bleeding from the perforation site immediately following choroidal puncture was noted in three cases only (20%).
As the subchoroidal hemorrhage increased in size there was an accompanying increase in intraocular pressure. In eight cases (53%) the pressure became markedly elevated. Drainage through a sclerotomy
813

814 AMERICAN JOURNAL OF OPHTHALMOLOGY NOVEMBER, 1966
was necessary in these cases to control glaucoma. Drainage also was performed in two additional cases (14%) in which the hemorrhage was quite large. In the five other cases (33%) the hemorrhage was small and surgical drainage was not necessary.
The patients with subchoroidal hemorrhage often had high myopia. Eight of the 15 cases (53%) had refractive errors of — 8.0D or more. This differed significantly from the 7% incidence of comparable myopia in all 1,500 cases. In each of these patients with high myopia, degenerative changes of the peripheral choroid and retina had been noted during the preoperative examination.
Another common feature of the cases with hemorrhagic choroidal detachment was the posterior position of the scleral buckle. The average distance from the limbus to the posterior edge of the retinal breaks was 18 mm. In 13 of the 15 cases (87%) the retinal breaks were located posterior to the equator of the globe. The presence of vortex veins complicated the undermining of the sclera in seven cases (47%).
In the postoperative period, a progressive extension of the choroidal detachment commonly occurred before absorption began. Four cases (27%) required drainage of the subchoroidal fluid in a subsequent procedure, and at this time serosanguinous fluid was released. In all cases absorption was complete within four to six weeks.
Serous choroidal detachment. During the postoperative period, 348 cases of serous choroidal detachment were noted, an incidence of 23% for the 1,485 operations remaining after exclusion of the 15 cases with hemorrhagic choroidal detachment.
Clinical features. Typically, serous detachment of the choroid was noted on the first or second postoperative day (table 1), and appeared as a prominent, brown-colored, smooth and immobile elevation. In many cases, however, the choroid was minimally elevated and its extent difficult to appreciate by ophthalmoscopic examination. Serous detachment of the choroid occurred
TABLE 1 DETECTABLE ONSET OF SEROUS TYPE
Postoperative Day No. Patients Percentage
First Second Third Fourth Fifth Sixth More than
TOTAL
six days
98 96 46 41 22 22 23
348
28 28 13 12 6 6 7
100%
most frequently at the level of the equator with extension anteriorly. Following scleral buckling procedures it was generally found in a meridian that was either adjacent to or opposite the area of the buckle. Less frequently serous choroidal detachment was noted in the area of the buckle. In these cases the choroidal detachment usually was noted on either the anterior or posterior aspect of the buckle. It was exceptional for a prominent elevation of the choroid to occur over the convexity of the buckle.
In approximately 10% of the 348 cases reviewed, the serous choroidal detachment became extensive and involved all quadrants. In such instances (fig. 1) the entire ora serrata was visible without scleral indentation. The rounded choroidal elevations had a scalloped contour since the vortex am-pullas maintained an attachment to the sclera. Occasionally the detachment was deeply creased along the horizontal meridian when the choroid remained adherent to the sclera along the course of the long ciliary artery and nerve.
The serous detachment of the choroid often increased in size for two to four days after onset. Then absorption began and was usually complete by the end of the second postoperative week, except in extensive cases. Following a slow absorption, a mild, but diffuse, pigmentary proliferation occasionally developed in the area of previous choroidal detachment. Sometimes faint pigment lines formed, resembling demarcation lines.
Incidence. The incidence of serous choroidal detachment increased with the pa-
VOL. 62, NO. S C H O R O I D A L D E T A C H M E N T A N D R E T I N A L SURGERY 815
tient's age (table 2) . The incidence was 3% up to the age of 20 years. It was 20% for patients between 21 and 60 years of age. For patients 61 and over, the incidence was 33%. The differences between these three percentages are significant.
Data relating to the operative procedure showed that subretinal fluid was released through a choroidal perforation in 1,314 cases, of which 26% subsequently developed a choroidal detachment. In cases which did not require perforation, the incidence was 7%, which was significantly lower (table 3) . It should be noted that the hypotony associated with release of subretinal fluid was transient. In the scleral buckling procedures the intraocular pressure was restored when the scleral sutures were pulled up. Furthermore, at the termination of the procedure, the intraocular pressure was adjusted to approximately IS mm Hg.
Vortex veins interfered with the undermining of the scleral flaps in 77 of the 1,485 cases (5%) . These were generally the most difficult cases with breaks located posterior to the equator. Several varieties of insult to the vortex veins were noted in the operative reports: (1) the intrascleral course of a vein was cut during the scleral undermining on 14 occasions; (2) 30 veins were obliterated by diathermy; (3) on 46 occasions the intrascleral course and scleral exit of a vein were encountered during the dissection of the scleral bed; and (4) thrombosis of a vortex vein was noted in two instances during the operation, apparently as a result of surgical manipulations. Among the 77 eyes in which the vortex veins were subjected to
TABLE 2 INFLUENCE OF AGE ON INCIDENCE OF SEROUS TYPE
Age Group
(yr)
0-20 21-40 41-60
61 and over
TOTALS
Cases of Cases of Retinal Choroidal
Detachment Detachment
131 157 625 572
1,485
4 29
126 189
348
Percentage
3 18 20 33
23
TABLE 3 INFLUENCE OF CHOROIDAL PERFORATION ON
INCIDENCE OF SEROUS TYPE
Cases of Cases of Retinal Choroidal
Detachment Detachment
Perforation 1,314 336 No Perforation 171 12
TOTALS 1,485 348
Percentage
26 7
23
TABLE 4 INFLUENCE OF VORTEX VEIN TRAUMA ON
INCIDENCE OF SEROUS TYPE
Vein Cases of r l . . , Involve- Retinal D e t a c h m e n t Percentage
ment Detachment U e t a c n m e n t
None One Two
1,408 62 15
314 23 11
22 37 73
TOTALS 1,485 348 23
one or more of the insults described, a single vein was involved in 62 cases (4%) and two or more in 15 (1%) . Choroidal detachment occurred after the operation in 37% of the eyes in which one vein was damaged, and in 73% of those in which two veins were involved (table 4) . The incidence of choroidal detachment associated with trauma to either one or two vortex veins was significantly higher than the incidence of 22% in operations which did not affect vortex veins.
Other factors such as sex of the patient, refractive error, aphakia and extent of the area treated with diathermy did not significantly affect the incidence of serous choroidal detachment.
Complications. In almost all cases the choroidal detachment absorbed without complicating the postoperative course. The most frequent complication noted was secondary glaucoma which developed in four of 15 eyes (27%) with hemorrhagic detachment and in 19 of the 348 eyes (5%) with serous detachment. Corneal edema, noted on the first or second postoperative day, usually
816 AMERICAN JOURNAL OF OPHTHALMOLOGY NOVEMBER, 1966
suggested an increase of intraocular pressure. In nine of the 23 eyes (39%) with postoperative glaucoma, the anterior chamber became shallow, especially in the periphery. Four eyes were aphakic. In eight of the 23 eyes (35%) vortex veins had complicated the dissection of the scleral bed. In spite of the fact that corneal edema made visualization of the fundus unsatisfactory, the choroidal detachment was noted to involve all quadrants in 10 of the 23 eyes (43%).
The glaucoma was controlled in 17 of the 23 cases (74%) by treatment consisting of acetazolamide, 250 mg four times daily, and 1% levo-epinephrine drops, twice daily. Occasionally, 4% pilocarpine drops were used. Medical therapy was ineffective in six cases. Surgical drainage of the sub-choroidal fluid with saline injection into the anterior chamber was performed in five of these cases. In the remaining case, because of wound infection in addition to the choroidal detachment, the silicone implants and sutures were removed. These surgical procedures resulted in successful control of the glaucoma in all six cases. Following absorption of the subchoroidal fluid, it was possible to discontinue the antiglaucomatous medication in all cases.
One other postoperative complication, extensive choroidal detachment, which threatened to involve the macula, developed in two of the 15 eyes (13%) with hemorrhagic detachment and in five of the 348 eyes (1%) with serous detachment. These cases were treated with drainage of the subchoroidal fluid through a sclerotomy. In aphakic eyes, ocular volume was restored by injecting saline into the anterior chamber. But in phakic eyes saline was injected into the vitreous body in order to restore satisfactorily the ocular volume.
EXPERIMENTAL STUDY
The experimental procedures were designed to yield information relating to the pathogenesis of choroidal detachment fol
lowing retinal surgery. The effects of scleral diathermy and hypotony were studied individually in animal eyes. Then, the effects of the combination of scleral diathermy with hypotony were investigated. And, finally, the effects of diathermy, hypotony, and vortex vein occlusion were observed.
MATERIAL AND METHODS
The operative procedures were performed on the eyes of eight squirrel monkeys, weighing 480 to 640 gm. Lateral canthotomy, removal of the lateral wall of the orbit, and tenotomy of the inferior rectus muscle were performed in each case to obtain satisfactory exposure of the globe. On the fourth postoperative day the monkeys were anesthetized and the eyes were examined and then enucleated. Formalin was used for fixation. The globes were opened and examined with a dissecting microscope. The specimens were then embedded in paraffin and sections were stained with hematoxylin and eosin.
The 16 eyes used for experimentation were divided into four groups:
1. In two eyes, diathermy was applied in a 150-degree circumferential arc between the equator and the ora serrata. The intensity was similar to that used clinically in retinal detachment surgery.
2. In two other eyes, hypotony was created by needle aspiration of approximately 0.2 ml of liquid vitreous through a sclerotomy located over the pars plana ciliaris.
3. In five eyes, scleral diathermy was applied as just described and, following this, hypotony was created by aspiration of vitreous.
4. In seven eyes, the two inferior vortex veins were diathermized in addition to scleral diathermy and vitreous aspiration.
FINDINGS
By ophthalmoscopic examination choroidal detachment was not recognized in any of the 16 eyes. Gross examination after opening the eyes showed the presence of an ante-
VOL. 62, NO. S CHOROIDAL DETACHMENT AND RETINAL SURGERY 817
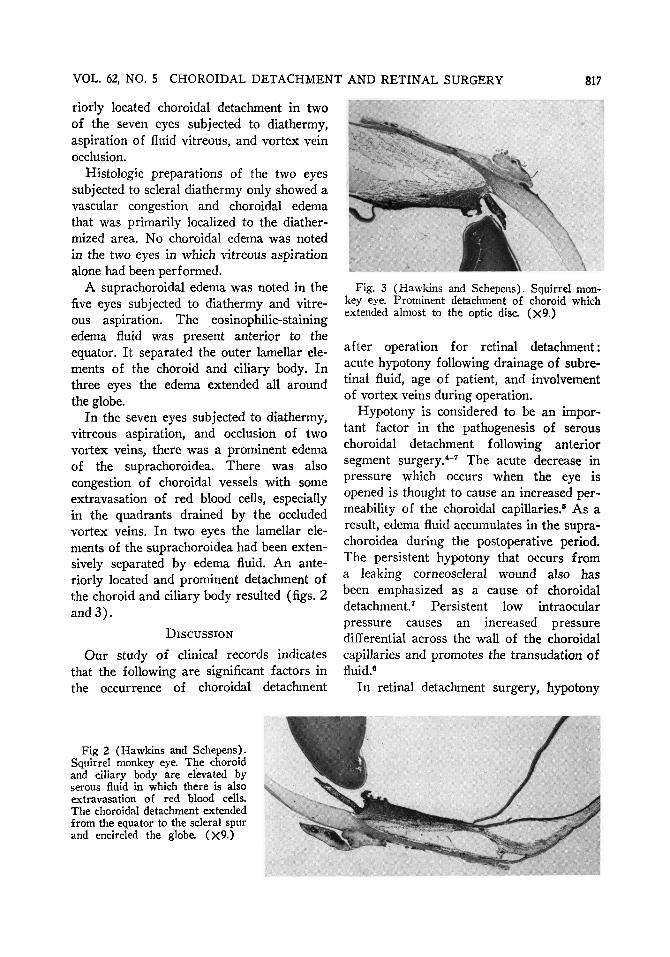
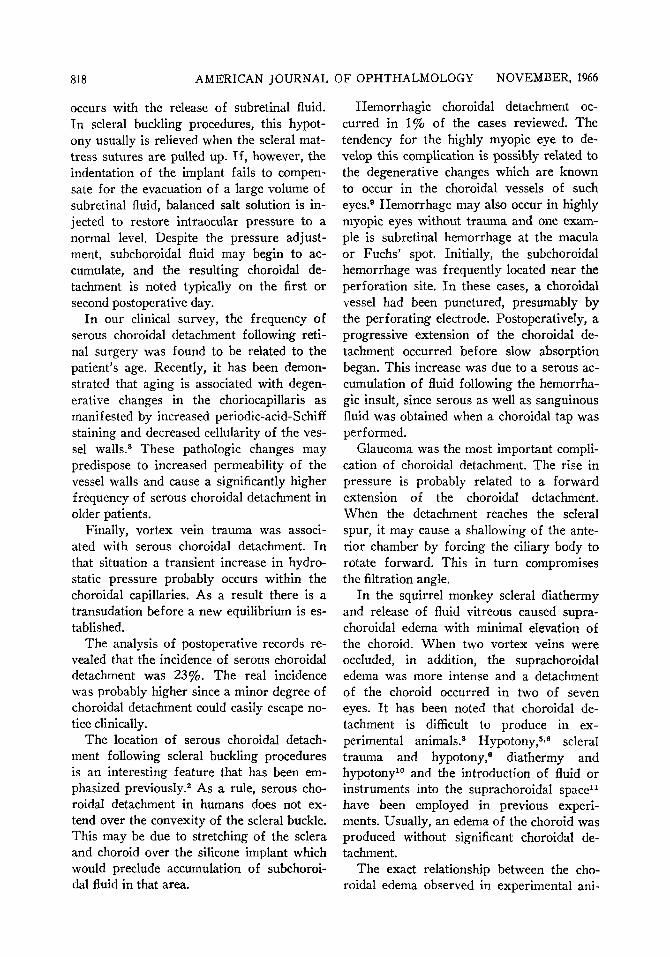
riorly located choroidal detachment in two of the seven eyes subjected to diathermy, aspiration of fluid vitreous, and vortex vein occlusion.
Histologic preparations of the two eyes subjected to scleral diathermy only showed a vascular congestion and choroidal edema that was primarily localized to the diather-mized area. No choroidal edema was noted in the two eyes in which vitreous aspiration alone had been performed.
A suprachoroidal edema was noted in the five eyes subjected to diathermy and vitreous aspiration. The eosinophilic-staining edema fluid was present anterior to the equator. It separated the outer lamellar elements of the choroid and ciliary body. In three eyes the edema extended all around the globe.
In the seven eyes subjected to diathermy, vitreous aspiration, and occlusion of two vortex veins, there was a prominent edema of the suprachoroidea. There was also congestion of choroidal vessels with some extravasation of red blood cells, especially in the quadrants drained by the occluded vortex veins. In two eyes the lamellar elements of the suprachoroidea had been extensively separated by edema fluid. An anteriorly located and prominent detachment of the choroid and ciliary body resulted (figs. 2 and 3) .
DISCUSSION
Our study of clinical records indicates that the following are significant factors in the occurrence of choroidal detachment
Fig. 3 (Hawkins and Schepens). Squirrel monkey eye. Prominent detachment of choroid which extended almost to the optic disc. (X9.)
after operation for retinal detachment: acute hypotony following drainage of subre-tinal fluid, age of patient, and involvement of vortex veins during operation.
Hypotony is considered to be an important factor in the pathogenesis of serous choroidal detachment following anterior segment surgery.*"7 The acute decrease in pressure which occurs when the eye is opened is thought to cause an increased permeability of the choroidal capillaries.5 As a result, edema fluid accumulates in the suprachoroidea during the postoperative period. The persistent hypotony that occurs from a leaking corneoscleral wound also has been emphasized as a cause of choroidal detachment.7 Persistent low intraocular pressure causes an increased pressure differential across the wall of the choroidal capillaries and promotes the transudation of fluid.6
In retinal detachment surgery, hypotony
Fig 2 (Hawkins and Schepens). Squirrel monkey eye. The choroid and ciliary body are elevated by serous fluid in which there is also extravasation of red blood cells. The choroidal detachment extended from the equator to the scleral spur and encircled the globe. (X9.)
818 AMERICAN JOURNAL OF OPHTHALMOLOGY NOVEMBER, 1966
occurs with the release of subretinal fluid. In scleral buckling procedures, this hypot-ony usually is relieved when the scleral mattress sutures are pulled up. If, however, the indentation of the implant fails to compensate for the evacuation of a large volume of subretinal fluid, balanced salt solution is injected to restore intraocular pressure to a normal level. Despite the pressure adjustment, subchoroidal fluid may begin to accumulate, and the resulting choroidal detachment is noted typically on the first or second postoperative day.
In our clinical survey, the frequency of serous choroidal detachment following retinal surgery was found to be related to the patient's age. Recently, it has been demonstrated that aging is associated with degenerative changes in the choriocapillaris as manifested by increased periodic-acid-Schiff staining and decreased cellularity of the vessel walls.8 These pathologic changes may predispose to increased permeability of the vessel walls and cause a significantly higher frequency of serous choroidal detachment in older patients.
Finally, vortex vein trauma was associated with serous choroidal detachment. In that situation a transient increase in hydrostatic pressure probably occurs within the choroidal capillaries. As a result there is a transudation before a new equilibrium is established.
The analysis of postoperative records revealed that the incidence of serous choroidal detachment was 23%. The real incidence was probably higher since a minor degree of choroidal detachment could easily escape notice clinically.
The location of serous choroidal detachment following scleral buckling procedures is an interesting feature that has been emphasized previously.2 As a rule, serous choroidal detachment in humans does not extend over the convexity of the scleral buckle. This may be due to stretching of the sclera and choroid over the silicone implant which would preclude accumulation of subchoroidal fluid in that area.
Hemorrhagic choroidal detachment occurred in 1% of the cases reviewed. The tendency for the highly myopic eye to develop this complication is possibly related to the degenerative changes which are known to occur in the choroidal vessels of such eyes.9 Hemorrhage may also occur in highly myopic eyes without trauma and one example is subretinal hemorrhage at the macula or Fuchs' spot. Initially, the subchoroidal hemorrhage was frequently located near the perforation site. In these cases, a choroidal vessel had been punctured, presumably by the perforating electrode. Postoperatively, a progressive extension of the choroidal detachment occurred before slow absorption began. This increase was due to a serous accumulation of fluid following the hemorrhagic insult, since serous as well as sanguinous fluid was obtained when a choroidal tap was performed.
Glaucoma was the most important complication of choroidal detachment. The rise in pressure is probably related to a forward extension of the choroidal detachment. When the detachment reaches the scleral spur, it may cause a shallowing of the anterior chamber by forcing the ciliary body to rotate forward. This in turn compromises the filtration angle.
In the squirrel monkey scleral diathermy and release of fluid vitreous caused supra-choroidal edema with minimal elevation of the choroid. When two vortex veins were occluded, in addition, the suprachoroidal edema was more intense and a detachment of the choroid occurred in two of seven eyes. It has been noted that choroidal detachment is difficult to produce in experimental animals.3 Hypotony,5'6 scleral trauma and hypotony,6 diathermy and hypotony10 and the introduction of fluid or instruments into the suprachoroidal space11
have been employed in previous experiments. Usually, an edema of the choroid was produced without significant choroidal detachment.
The exact relationship between the choroidal edema observed in experimental ani-
VOL. 62, NO. 5 CHOROIDAL DETACHMENT AND RETINAL SURGERY 819
mals and the choroidal detachment that occurs in humans is difficult to determine. In this regard, a factor not previously considered is the age disparity. Since most laboratory animals are young, it may be that only a minimal accumulation of suprachoroidal edema fluid is to be expected.
A final consideration is the role of scleral diathermy in the pathogenesis of choroidal detachment accompanying retinal surgery. In our clinical survey the circumferential extent of the diathermized area did not affect the incidence of choroidal detachment. However, 12 cases of choroidal detachment occurred when no perforation was done to release the subretinal fluid. Thus, the diathermy reaction obviously participated in the mechanism of the edema formation. Furthermore, in the animal experiments it was noted that edema and detachment of the choroid occurred only when diathermy was also used in the procedure. It would seem, therefore, that the choroidal injury produced by diathermy is another factor that influences the incidence of choroidal detachment in association with retinal surgery.
SUMMARY
Choroidal detachment is a common sequel of retinal surgery. It may occur as either a hemorrhagic or a serous accumulation of fluid. In a series of 1,500 cases, hemorrhagic and serous choroidal detachments were observed in 1% and 23% of cases, respective-
Hemorrhagic choroidal detachment occurred following perforation and the acute hypotony associated with drainage of subretinal fluid. It was most common in highly myopic eyes. The development of serous choroidal detachment was associated with drainage of subretinal fluid, age of patient, vortex vein involvement, and scleral diathermy. The clinical features of serous detachments were described.
Glaucoma was the most serious complication of choroidal detachment; it disappeared following absorption of the choroidal detachment.
In the squirrel monkey choroidal detachment was produced following the combination of scleral diathermy, vitreous aspiration, and destruction of two vortex veins. Scleral diathermy with vitreous aspiration produced suprachoroidal edema of a lesser degree.
20 Stamford Street (02114)
ACKNOWLEDGMENT
We wish to acknowledge the assistance of Taylor Smith, M.D., and Richard Donovan, V.M.D., in the pathologic studies. The fundus painting is by William J. Stenstrom.
REFERENCES
1. Tolentino, F. I., and Brockhurst, R. J.: Unilateral scleral icterus due to choroidal hemorrhage. Arch. Ophth. 70:3S8, 1963.
2. Schepens, C. L.: Importance of choroidal detachment in fundus diagnosis. (Society Proceedings.) Am. J. Ophth. 51:333, 1961.
3. Bernard, P.: Le decollement de la choroide: Bull. Soc. Ophtal. France. Suppl. 1963, p. 77.
4. Spaeth, E. B., and DeLong, P.: Detachment of the choroid: A clinical and histopathologic analysis. Arch. Ophth. 32 :217, 1944.
5. O'Brien, C. S.: Detachment of the choroid after cataract extraction: Clinical and experimental studies, with report of 75 cases. Arch. Ophth. 14 :S27, 1935.
6. Capper, S. A., and Leopold, I. H.: Mechanism of serous choroidal detachment. Arch. Ophth. 55:101, 1956.
7. Verhoeff, F. H., and Waite, J. H.: Separation of the choroid, with report of a spontaneous case. Arch. Ophth. 55:38, 1925.
8. Friedman, E., Smith, T. A., and Kuwabara, T.: Senile choroidal vascular patterns and drusen. Arch. Ophth. 69 :220, 1963.
9. Hogan, M. J., and Zimmerman, L. E.: Ophthalmic Pathology: An Atlas and Textbook. Philadelphia, Saunders, 1962, p. 114.
10. Swan, K. C, Christensen, L., and Weisel, J. T.: Choroidal detachment in the surgical treatment of retinal separation. Arch. Ophth. 55:240, 1956.
11. Pau, V. H.: Ueber die Amotio Chorioidae (Spongiosis Chorioidae), Klin. Mbl. Augenh. 130:347, 1957.