Embed Size (px)
Citation preview

Cirrhosis and Cirrhosis and Associated Associated ComplicationsComplications
Luke GesselOctober 2nd, 2014

OutlineOutlineCirrhosis◦Development◦Diagnosis
Complications of Cirrhosis◦Portal Hypertension◦Ascites◦Spontaneous Bacterial Peritonitis
◦Hepatic Encephalopathy

CirrhosisCirrhosis

EpidemiologyEpidemiology30,000 deaths per year due to cirrhosis in US
10,000 deaths per year due to liver cancer largely due to cirrhotic livers in US
Hepatocellular carcinoma most rapidly increasing neoplasm in US and western Europe

CompensatedcirrhosisCompensatedcirrhosis
DecompensatedcirrhosisDecompensatedcirrhosis DeathDeath
Chronic liver diseaseChronic liver disease
Complications:
Variceal hemorrhage Ascites
Encephalopathy Jaundice
Complications:
Variceal hemorrhage Ascites
Encephalopathy Jaundice
Natural History of Chronic Natural History of Chronic Liver DiseaseLiver Disease
Viral Autoimmune Drug-induced Cholestatic
diseases Metabolic
diseases

CirrhosisCirrhosisNormalNormal
NodulesNodules
Irregular surfaceIrregular surface
Gross Liver PathologyGross Liver Pathology

CirrhosisCirrhosisNormalNormal
Regenerative Nodules surrounded by fibrous tissue
Regenerative Nodules surrounded by fibrous tissue
Liver HistologyLiver Histology
FibrosisFibrosis

Liver AnatomyLiver Anatomy

Liver AnatomyLiver Anatomy
Hepatic Lobule Sinusoid

The Road to Liver The Road to Liver InjuryInjuryHepatic fibrosis◦Accumulation of extracellular matrix, or scar, in response to acute or chronic liver injury
◦Fibrogenesis Wound healing response to injury, ultimately leading to cirrhosis
Cirrhosis◦End-stage consequence of fibrosis of hepatic parenchyma, resulting in nodule formation that may lead to altered hepatic function and blood flow

The Road to Liver The Road to Liver InjuryInjuryCirrhosis largely takes years to decades
Can be accelerated in some cases:◦Neonatal liver disease
Infants with biliary atresia may have severe fibrosis and marked parenchymal distortion at birth
◦HCV-infected patients after liver transplantation
◦HIV/HCV-coinfection◦Severe delta-hepatitis◦Some cases of drug-induced liver disease

PATHOGENESIS OF LIVER FIBROSISPATHOGENESIS OF LIVER FIBROSISPATHOGENESIS OF LIVER FIBROSISPATHOGENESIS OF LIVER FIBROSIS
HepatocytesHepatocytes
Space of DisseSpace of Disse
Sinusoidal endothelial cell
Sinusoidal endothelial cell
Hepatic stellate cellHepatic stellate cell
FenestraeFenestrae
Normal Hepatic SInusoidNormal Hepatic SInusoid
Retinoid dropletsRetinoid droplets

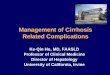
Hepatic Stellate CellsHepatic Stellate CellsThe key pathogenic feature underlying liver fibrosis and cirrhosis is hepatic stellate cell activation.
Hepatic stellate cells (also known as Ito cells or perisinusoidal cells) are located in the space of Disse
The space of Disse is located between hepatocytes and sinusoidal endothelial cells (that normally are fenestrated).
Normally, hepatic stellate cells are quiescent and serve as the main storage site for retinoids (vitamin A).

PATHOGENESIS OF LIVER FIBROSISPATHOGENESIS OF LIVER FIBROSISPATHOGENESIS OF LIVER FIBROSISPATHOGENESIS OF LIVER FIBROSIS
HepatocytesHepatocytes
Space of DisseSpace of Disse
Sinusoidal endothelial cell
Sinusoidal endothelial cell
Hepatic stellate cellHepatic stellate cell
FenestraeFenestrae
Normal Hepatic SInusoidNormal Hepatic SInusoid
Retinoid dropletsRetinoid droplets


PATHOGENESIS OF LIVER FIBROSISPATHOGENESIS OF LIVER FIBROSIS
Activation of Stellate cellsLoss of Vitamin AProliferationDevelopment of Rough ER and secretion of Extracellular MatrixMatrix Deposition in Space of DisseFuthermore Stellate Cells express smooth muscle proteins and become contractile—Hepatic Myofibroblasts
Activation of Stellate cellsLoss of Vitamin AProliferationDevelopment of Rough ER and secretion of Extracellular MatrixMatrix Deposition in Space of DisseFuthermore Stellate Cells express smooth muscle proteins and become contractile—Hepatic Myofibroblasts

PATHOGENESIS OF LIVER FIBROSIS
Alterations in Microvasculature in CirrhosisAlterations in Microvasculature in Cirrhosis
Activation of stellate cells Collagen deposition in space of
Disse Constriction of sinusoids Defenestration of sinusoids
Activation of stellate cells Collagen deposition in space of
Disse Constriction of sinusoids Defenestration of sinusoids

Disease-Specific Disease-Specific MechanismsMechanismsHepatitis C Virus◦ Stellate cells directly infectable by virus
Express HCV receptors Adenovirus transduction of non-structural and core proteins induces stellate cell proliferation and release of inflammatory signals
◦ Lymphocyte recruitment◦ HCV proteins interact directly with sinusoidal endothelium
NASH◦ Leptin, adipogenic hormone proportionate to adipose mass in circulating blood activates stellate cells
◦ Downregulation of adiponectin, counterregulatory hormone amplifies fibrogenic activity of leptin Mice lacking adiponectin have enhanced fibrosis following toxic liver injury

Reversibility of Reversibility of Fibrosis/CirrhosisFibrosis/CirrhosisElimination of underlying cause critical
Other factors:◦Period of established cirrhosis
Longer periods of crosslinked collagen, less sensitive to degradative enzymes?
◦Total content of collagen and other scar molecules Large mass of scar may be inaccessible to degradative enzymes
◦Reduced expression of enzymes that degrade matrix, and prevention of apoptosis of activated stellate cells

Liver insufficiencyLiver insufficiency
Variceal hemorrhageVariceal hemorrhage
Complications of Cirrhosis Result from Portal Hypertension or Liver InsufficiencyComplications of Cirrhosis Result from Portal Hypertension or Liver Insufficiency
CirrhosisCirrhosis AscitesAscites
EncephalopathyEncephalopathy
JaundiceJaundice
Portal hypertensionPortal hypertension
Spontaneous bacterial peritonitis
Spontaneous bacterial peritonitis
Hepatorenal syndromeHepatorenal syndrome
COMPLICATIONS OF CIRRHOSIS

Development of Complications in Compensated Cirrhosis Development of Complications in Compensated Cirrhosis
AscitesAscitesJaundiceJaundiceEncephalopathyEncephalopathyGI hemorrhageGI hemorrhage
Probability of developing event
Probability of developing event
00
2020
6060
8080
100100
00 6060
4040
2020 4040 8080 100100 120120 140140 160160
MonthsMonthsGines et. al., Hepatology 1987; 7:122Gines et. al., Hepatology 1987; 7:122
NATURAL HISTORY OF CIRRHOSIS

60604040 8080 100100 120120 140140 16016000
4040
6060
8080
2020
202000
100100
MonthsMonths
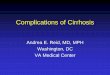
Probability of survivalProbability of survival
All patients with cirrhosisAll patients with cirrhosis
Decompensated cirrhosisDecompensated cirrhosis
180180
Decompensation Shortens SurvivalDecompensation Shortens Survival
Gines et. al., Hepatology 1987;7:122Gines et. al., Hepatology 1987;7:122
Median survival~ 9 yearsMedian survival~ 9 years
Median survival~ 1.6 yearsMedian survival~ 1.6 years
SURVIVAL TIMES IN CIRRHOSIS

Cirrhosis is a histological diagnosis
However, in patients with chronic liver disease the presence of various clinical features suggests cirrhosis
The presence of these clinical features can be followed by non-invasive testing, prior to liver biopsy
Cirrhosis - DiagnosisCirrhosis - Diagnosis

Any patient with chronic liver disease Chronic abnormal aminotransferases and/or
alkaline phosphatase
Physical exam findings Stigmata of chronic liver disease (muscle
wasting, vascular spiders, palmar erythema) Palpable left lobe of the liver Small liver span Splenomegaly Signs of decompensation (jaundice, ascites,
asterixis)
In Whom Should We Suspect In Whom Should We Suspect Cirrhosis?Cirrhosis?

Laboratory Liver insufficiency
Low albumin (< 3.8 g/dL) Prolonged prothrombin time (INR > 1.3) High bilirubin (> 1.5 mg/dL)
Portal hypertension Low platelet count (< 175 x1000/l)
AST / ALT ratio > 1
In Whom Should We Suspect In Whom Should We Suspect Cirrhosis?Cirrhosis?

Imaging studies Liver-spleen scan
Small liver, irregular uptake Splenomegaly Colloid shift to bone marrow
CAT scan / Ultrasound Nodular liver Splenomegaly Venous collaterals
In Whom Should We Suspect In Whom Should We Suspect Cirrhosis?Cirrhosis?

Small liver,irregular uptakeSmall liver,irregular uptake
SplenomegalySplenomegaly
Colloid shift to bone marrow and ribsColloid shift to bone marrow and ribs
Normal Cirrhosis
Liver-Spleen ScanLiver-Spleen Scan
DIAGNOSIS OF CIRRHOSIS – LIVER-SPLEEN SCAN

CAT Scan in CirrhosisCAT Scan in Cirrhosis
Liver with an irregular surfaceLiver with an irregular surface SplenomegalySplenomegalyCollateralsCollaterals
DIAGNOSIS OF CIRRHOSIS – CAT SCAN

Liver biopsy is not necessary in the presence of any of the following:◦Decompensated cirrhosis (variceal
hemorrhage, ascites, encephalopathy)
◦Liver-spleen and/or CAT scan diagnostic of cirrhosis
◦Liver biopsy is not necessary for pre-transplant evaluation
Confirmatory Liver Biopsy Is Not Confirmatory Liver Biopsy Is Not Always Necessary in CirrhosisAlways Necessary in Cirrhosis

• A 55-year-old asymptomatic Caucasian
man is referred to hepatology clinic for
evaluation of chronic elevation of
aminotransferases.
• He has no significant medical problems,
takes no medications and denies a family
history of liver disease.
• A 55-year-old asymptomatic Caucasian
man is referred to hepatology clinic for
evaluation of chronic elevation of
aminotransferases.
• He has no significant medical problems,
takes no medications and denies a family
history of liver disease.
Case KL
Case PresentationCase Presentation
Case KL – CASE PRESENTATION

Physical ExamPhysical Exam
• He is generally healthy appearing.
• There are no stigmata of chronic liver
disease including:
• No jaundice
• No vascular spiders or palmar
erythema
• A non-palpable liver and spleen.
• He is generally healthy appearing.
• There are no stigmata of chronic liver
disease including:
• No jaundice
• No vascular spiders or palmar
erythema
• A non-palpable liver and spleen.
Case KL
Case KL – PHYSICAL EXAM

Case KL
Laboratory ResultsLaboratory Results
Bilirubin 1.2 mg/dL
AST 80 U/L
ALT 94 U/L
Albumin 4.0 g/dL
PT 12 sec
Bilirubin 1.2 mg/dL
AST 80 U/L
ALT 94 U/L
Albumin 4.0 g/dL
PT 12 sec
WBC
4.0 x1000/uL
Hgb
17 g/dL
Platelets
175 x1000/uL
Anti-HCV
positive
HBsAg
negative
WBC
4.0 x1000/uL
Hgb
17 g/dL
Platelets
175 x1000/uL
Anti-HCV
positive
HBsAg
negative
Case KL – LAB RESULTS

Diagnostic StudiesDiagnostic Studies
Abdominal ultrasound:
mildly increased hepatic echogenicity
mild splenomegaly
Liver-spleen scan increased uptake in spleen no colloid shift to bone marrow
Abdominal ultrasound:
mildly increased hepatic echogenicity
mild splenomegaly
Liver-spleen scan increased uptake in spleen no colloid shift to bone marrow
Case KL
Case KL – DIAGNOSTIC STUDIES

Does this patient have cirrhosis?
Maybe
Does this patient need a liver biopsy?
Liver biopsy is necessary to confirm/rule out cirrhosis
Does this patient have cirrhosis?
Maybe
Does this patient need a liver biopsy?
Liver biopsy is necessary to confirm/rule out cirrhosis
Case KL
Case KL – QUESTIONCase KL – QUESTION

Case DW
A 55 year-old, previously healthy man, complains of fatigue for several months.
He denies excessive alcohol use, but admits to using IV drugs when he was a teenager.
A 55 year-old, previously healthy man, complains of fatigue for several months.
He denies excessive alcohol use, but admits to using IV drugs when he was a teenager.
Case DW – CASE PRESENTATIONCase DW – CASE PRESENTATION

Physical ExamPhysical Exam
Exam shows vascular spiders on his back.
Abdominal exam reveals a firm liver edge, and an easily palpated left lobe, 2 cm below the xyphoid.
The spleen tip is palpable.
There is no shifting dullness on abdominal percussion.
Exam shows vascular spiders on his back.
Abdominal exam reveals a firm liver edge, and an easily palpated left lobe, 2 cm below the xyphoid.
The spleen tip is palpable.
There is no shifting dullness on abdominal percussion.
Case DW
Case DW – PHYSICAL EXAMCase DW – PHYSICAL EXAM

Case DW
Laboratory ResultsLaboratory Results
Bilirubin 1.1 mg/dL
AST 110 U/L
ALT 92 U/L
Albumin 3.5 g/dL
PT 12.5 sec
Bilirubin 1.1 mg/dL
AST 110 U/L
ALT 92 U/L
Albumin 3.5 g/dL
PT 12.5 sec
WBC 4.0 x1000/uL
Hgb 12 g/dL
Platelets 95 x1000/uL
Anti-HCV positive
HBsAg negative
WBC 4.0 x1000/uL
Hgb 12 g/dL
Platelets 95 x1000/uL
Anti-HCV positive
HBsAg negative
Case DW – LAB RESULTSCase DW – LAB RESULTS

Diagnostic StudiesDiagnostic Studies
Abdominal ultrasound: Echogenic, heterogeneous liver
parenchyma Enlarged caudate lobe Enlarged spleen (15.5 cm)
Liver-spleen scan: Colloid shift to bone marrow Increased uptake by spleen
Abdominal ultrasound: Echogenic, heterogeneous liver
parenchyma Enlarged caudate lobe Enlarged spleen (15.5 cm)
Liver-spleen scan: Colloid shift to bone marrow Increased uptake by spleen
Case DW
Case DW – DIAGNOSTIC STUDIESCase DW – DIAGNOSTIC STUDIES

Does this patient have cirrhosis?
Yes
Does this patient need a liver biopsy?
Liver biopsy is NOT necessary to establish the diagnosis of cirrhosis
Does this patient have cirrhosis?
Yes
Does this patient need a liver biopsy?
Liver biopsy is NOT necessary to establish the diagnosis of cirrhosis
Case DW
Case DW – QUESTIONS

Portal HypertensionPortal Hypertension

Hepatic Blood FlowHepatic Blood Flow

Portal Hypertension
Cirrhotic Liver
Portal Blood Flow
Systemic Blood Flow

Portal HypertensionPortal HypertensionDefined by pathological increase in portal venous pressure
Complications arise when portal pressure gradient exceed 10-12 mm Hg (normal <6 mm Hg)
Cirrhosis is the most common cause of portal hypertension
The site of increased resistance in cirrhosis is sinusoidal
Cirrhosis is the most common cause of portal hypertension

Portal HypertensionPortal Hypertension
Architectural disturbances(fibrosis, scarring, vascular thrombosis, etc.)
Functional alterations(contraction of vascular smooth muscle and stellate cells)
Cirrhotic liver
Increased hepatic resistance
Portal hypertension
Splanchnic vasodilatation
Collaterals and PSS
Increased portalblood inflow
Effective hypovolemia
Activation of endogenousvasoactive systems
Na retentionHypervolemia
Increased cardiac index

Increased Intrahepatic Increased Intrahepatic ResistanceResistance1. Architectural distortion of the
liver◦ Fibrous tissue and regenerative nodules◦ Thrombosis of portal and hepatic veins
2. Dynamic reversible contractile elements

Normal Liver
Hepatic vein
Hepatic vein
SinusoidSinusoid
Portal vein
Portal vein
LiverLiver
Splenic veinSplenic vein
Coronary veinCoronary vein

Portal systemic collaterals
Portal systemic collaterals
Distorted sinusoidal
architectureleads to
increased resistance
Distorted sinusoidal
architectureleads to
increased resistance
Portal vein
Portal vein
Cirrhotic Liver
SplenomegalySplenomegaly

Increased Intrahepatic Increased Intrahepatic ResistanceResistance1. Architectural distortion of the liver
2. Dynamic reversible contractile elements◦ 40% of increased intrahepatic vascular
resistance◦ Involves:
Vascular smooth muscle cells Activated hepatic stellate cells that contract around
sinusoids reducing caliber Hepatic myofibroblasts that compress cirrhotic nodules Vasoactive mediators that modulate intrahepatic
resistance

Increased Intrahepatic Increased Intrahepatic ResistanceResistance
◦ Increased production of vasoconstrictors with exaggerated response by hepatic vascular bed
◦ Insufficient release of vasodilators and insufficient response by hepatic vascular bed
Vasoconstrictors
EndothelinAngiotensin
NorepinephrineVasopressinLeukotrienesThromboxaneOthers?
Vasodilators
Nitric OxideCarbon Monoxide
Others?

Variceal HemorrhageVariceal Hemorrhage

Prevalence of Esophageal Varices in Cirrhosis
Prevalence of Esophageal Varices in Cirrhosis
%%
100100
6060
4040
2020
00OverallOverall Child AChild A Child BChild B
8080
Child CChild C
Pagliaro et al., In: Portal Hypertension: Pathophysiology and Management, 1994: 72Pagliaro et al., In: Portal Hypertension: Pathophysiology and Management, 1994: 72
PREVALENCE OF ESOPHAGEAL VARICES IN CIRRHOSIS

Lowest Rebleeding Rates are Obtained in HVPG Responders and With Ligation + -
Blockers
Lowest Rebleeding Rates are Obtained in HVPG Responders and With Ligation + -
Blockers
(19 trials)(19 trials)(26 trials)(26 trials) (54 trials)(54 trials)
%%RebleedingRebleeding
8080
6060
4040
2020
00UntreatedUntreated -
blockers-
blockersSclero-therapySclero-therapy
(18 trials)(18 trials)
LigationLigation
(6 trials)(6 trials)
HVPG-Responders
*
HVPG-Responders
*(6 trials)(6 trials)
-blockers+ ISMN
-blockers+ ISMN
(2 trials)(2 trials)
Ligation +
-blockers
Ligation +
-blockers
Bosch and García-Pagán, Lancet 2003; 361:952Bosch and García-Pagán, Lancet 2003; 361:952 * HVPG <12 mmHg
or >20% from baseline
* HVPG <12 mmHg or >20% from
baseline
LOWEST REBLEEDING RATES ARE OBTAINED IN HVPG RESPONDERS AND IN PATIENTS TREATED WITH VARICEAL BAND LIGATION + BETA-BLOCKERS

AscitesAscites

AscitesAscitesMost common cause of decompensation in patients with cirrhosis
Occurs at rate of 7-10% per year
5% of patients with ascites can develop right sided pleural effusions—hepatic hydrothorax◦Develops through diaphragmatic defects


AscitesAscitesDiagnosis◦Physical Exam◦Ultrasonography◦Diagnostic Paracentesis

Peritoneal pathology- Malignancy- Tuberculosis
Peritoneal pathology- Malignancy- Tuberculosis
Sinusoidal hypertension-Cirrhosis-Late Budd-Chiari
Sinusoidal hypertension-Cirrhosis-Late Budd-Chiari
Source of ascites
Source of ascites
Hepatic sinusoidsSAAG > 1.1
Hepatic sinusoidsSAAG > 1.1
PeritoneumSAAG < 1.1 PeritoneumSAAG < 1.1
“Capillarized” sinusoidAscites protein < 2.5
“Capillarized” sinusoidAscites protein < 2.5
Peritoneal lymphAscites protein > 2.5
Peritoneal lymphAscites protein > 2.5
Post-sinusoidal hypertension
- Cardiac ascites- Early Budd-Chiari - Veno-occlusive disease
Post-sinusoidal hypertension
- Cardiac ascites- Early Budd-Chiari - Veno-occlusive disease
Normal “leaky” sinusoidAscites protein > 2.5
Normal “leaky” sinusoidAscites protein > 2.5
Ascites Can Be Characterized by Serum-Ascites Albumin Gradient (SAAG) and Ascites Protein
ASCITES CAN BE CHARACTERIZED BY SERUM-ASCITES ALBUMIN GRADIENT (SAAG) AND ASCITES PROTEIN

Ascites: ManagementAscites: ManagementSodium restriction—2 grams dailyOral diuretics◦Spironolactone (more effective than loop diuretics) Started at dose of 50-100 mg/daily Adjust 13-4 days to maximal effective dose of 400 mg/day
◦Furosemide can be added as well 5:2 ratio
Fluid restriction not required unless there is hyponatremia—Na<130

Ascites: ManagementAscites: ManagementWeight loss goal◦1 kg in first week◦2 kg/wk subsequently
Excessive loss of weight (>1 lb./day)◦Can lead to intravascular depletion◦Can lead to Pre-Renal Kidney Injury
Avoid ASA and NSAIDs◦Can reduce diuretic induced natriuresis
◦May precipitate Renal Failure

Ascites: ManagementAscites: ManagementLarge Volume Paracentesis (LVP)◦For patients with tense ascites◦Albumin is to be given at rate of 6-8 gram/liter, particularly with removal of >5 liters
10% of patients with cirrhosis and ascites may become diuretic resistant◦Recurrent LVP plus albumin ◦TIPS
Encephalopathy

Spontaneous Bacterial Spontaneous Bacterial PeritonitisPeritonitis

Spontaneous Bacterial Spontaneous Bacterial PeritonitisPeritonitisThe most life-threatening complication of ascites
~1/3 of hospitalized patients with cirrhosis are diagnosed as having a bacterial infection—most common is SBP
All Patients with cirrhosis and ascites who are hospitalized emergently should undergo a diagnostic paracentesis
Diagnosis is established with ascitic fluid neutrophil count greater than 250/mm3
Bacteria are isolated in only 40-50% of casees

Spontaneous Bacterial Spontaneous Bacterial PeritonitisPeritonitisOnce diagnosis established◦Empiric antibiotic therapy with IV 3rd generation cephalosporin
◦Success rates for 3rd generation cephalosporins have been as low as 40% in nosocomial SBP
◦In this case use Pip/Tazo or a Carbapenem
Avoid Aminoglycosides—High Incidence of Renal Toxicity in Patients with Cirrhosis
For prevention of progressive renal dysfunction administer albumin◦1.5 g/kg day 1 and 1g/kg on day 3

Spontaneous Bacterial Spontaneous Bacterial PeritonitisPeritonitis~70% Risk of RecurrenceProphylactic Antibiotic◦Recommended Antibiotic is Norfloxacin 400 mg daily
Per UpToDate:◦In settings where norfloxacin is unavailable Ciprofloxacin 500 mg daily Trimethoprim-Sulfamethoxazole one double strength tablet daily

All SBPsAll SBPs SBP caused by gram-negative bacteria
SBP caused by gram-negative bacteria
Probability of SBP
recurrence
Probability of SBP
recurrence
MonthsMonths
p=0.0063p=0.0063
PlaceboPlacebo
NorfloxacinNorfloxacin
PlaceboPlacebo
p=0.0013p=0.0013
NorfloxacinNorfloxacin
00
1.01.0
.8.8
.4.4
.2.2
.6.6
44 88 1212 2020
00
1616 00 44 88 1212 20201616
MonthsMonths
Norfloxacin Reduces Recurrence of Spontaneous Bacterial Peritonitis
Norfloxacin Reduces Recurrence of Spontaneous Bacterial Peritonitis
Gines et al., Hepatology 1990; 12:716Gines et al., Hepatology 1990; 12:716
NORFLOXACIN REDUCES RECURRENCE OF SPONTANEOUS BACTERIAL PERITONITIS (SBP)

Hepatic Hepatic EncephalopathyEncephalopathy

Hepatic EncephalopathyHepatic EncephalopathyReversible syndrome caused by astrocyte swelling
Ammonia and other toxins play key role in pathogenesis
Ammonia accumulates due to shunting of blood through portosystemic collaterals and decreased liver metabolism

Hepatic EncephalopathyHepatic Encephalopathy HE associated with cirrhosis is of gradual onset and rarely fatal
Distinguished from encephalopathy from acute liver failure and portosystemic bypass in absence of cirrhosis
Stage 1: Forgetfulness and Inversion of Sleep/Wake Pattern
Stage 2: Confusion, Bizarre behavior and Disorientation
Stage 3: Lethargy and Profound Disorientation
Stage 4: Coma

Hepatic EncephalopathyHepatic EncephalopathyOn Exam◦Asterixis◦Fetor Hepaticus (sweet smelling odor to breath)
Diagnosis◦Made Clinically◦Serum Ammonia levels are unreliable/correlate poorly with stage
◦Number connection test and EEG are used in research but not routinely in clinical setting

Ong et al., Am J Med 2003; 114:188Ong et al., Am J Med 2003; 114:188
Poor Correlation of Ammonia Levels With Presence or Severity of
Encephalopathy
Venous total
ammoniamol/L
Venous total
ammoniamol/L
00
400400
350350
300300
250250
200200
150150
100100
5050
Grade 0Grade 0 Grade 1Grade 1 Grade 2Grade 2 Grade 3Grade 3 Grade 4Grade 4
Severity of Hepatic EncephalopathySeverity of Hepatic Encephalopathy
POOR CORRELATION OF AMMONIA LEVELS WITH PRESENCE OR SEVERITY OF HEPATIC ENCEPHALOPATHY

Hepatic EncephalopathyHepatic EncephalopathyMainstay of therapy is identification and treatment of precipitating factors◦Dehydration◦Infections◦Overdiuresis◦GI bleeding◦High Oral Protein Load◦Constipation◦Use of Narcotics◦TIPS

Hepatic EncephalopathyHepatic EncephalopathyTreatment:◦Lactulose and Rifaxamin◦Consider change in dietary protein from animal to vegetable source
◦Strict protein restriction is not necessary and is discouraged long-term

Hepatocellular Hepatocellular CarcinomaCarcinoma

Hepatocellular Hepatocellular CarcinomaCarcinomaHCC can occur in both compensated and decompensated cirrhotics and can be the event that leads to decompensation
5th most common cause of cancer worldwide
3rd most common cause of cancer related mortality worldwide
In the United States there ahs been a twofold increase in assess of HCC over the past two decades◦ Relates to the increase in prevalence of chronic hepatitis C

Hepatocellular Hepatocellular CarcinomaCarcinomaEntertains in patients with compensated cirrhosis who:◦Suddenly decompensate◦Develop Portal Vein Thrombosis
Diagnosis◦Dynamic Radiologic Imaging (CT or MRI with contrast)
◦Elevated AFP may support diagnosis◦In some instances liver biopsy may be needed to conform

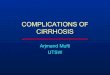
Cabibbo G et al. (2009) Multimodal approaches to the treatment of hepatocellular carcinomaNat Clin Pract Gastroenterol Hepatol doi:10.1038/ncpgasthep1357
Figure 1 Algorithm for staging and treating patients diagnosed as having hepatocellular carcinoma

ConclusionConclusion Cirrhosis is the result of a common pathway from numerous causes of liver inflammation
Decompensated cirrhosis carries a significant mortality and complications should be closely monitored in the inpatient and outpatient setting
Ascites should always be sampled with emergent hospitalization
Hepatic Encephalopathy severity does not directly correlate with ammonia level and should prompt evaluation of inciting cause
Patients with HCC should undergo timely evaluation and triage into the appropriate management arm so as to maximize survival potential

ReferencesReferences Bosch J, D’Amico G, Garcia-Pagan JC. Portal Hypertension and
Nonsurgical Management. In: Schiff ER, Sorrell MF, Maddrey WC, editors. Tenth edition. Schiff’s Diseases of the Liver, Vol. 1. Philadelphia: Lippincott Williams & Wilkins; p. 419-483
Friedman SL. Hepatic fibrosis. In: Schiff ER, Sorrell MF, Maddrey WC, editors. Tenth edition. Schiff’s Diseases of the Liver, Vol. 1. Philadelphia: Lippincott Williams & Wilkins; p. 395-418
Friedman SL. Pathogenesis of hepatic fibrosis. Up-to-Date. May 2010.
Rockey DC, Friedman SL(2006). Hepatic fibrosis and cirrhosis. In: Boyer TD, Wright TL, Manns MP, editors. 5th edition. Zakim and Boyer’s hepatology, vol.1. New York: Elsevier;. p. 87–109.
Rodriguez-Vilarrupla et al (2007). Current concepts on the pathophysiology of portal hypertension. Annals of Hepatology; 6(1): Jan-March: 28-36.
Vorobioff J; Bredfeldt JE; Groszmann RJ. Increased blood flow through the portal system in cirrhotic rats. Gastroenterology 1984 Nov;87(5):1120-6.