Embed Size (px)
Citation preview
American Medical ResponseCritical Incident Stress Management Program
2014-2015 Annual Report
Serving Clark, Cowlitz, Clackamas, and Multnomah County Operations, Communications, SpecialServices Division, and Special Teams
June 1, 2015
Prepared by:Bill Lang, B.A., Paramedic, CISM Coordinator
Introduction
This First Annual Report of the Critical Incident Stress Management Program which has been in service since March 17, 2014, provides a history of the CISM Program activities which began in 2005, a statement of the mission, goals, and objectives of the program, a description of the current program,a Mock CISM Activation Scenario, an Action Log spreadsheet documenting the actions taken by those involved in the Program accompanied by a Glossary of terms and abbreviations, and a summary, as well as components for future development within the program. Pertinent guiding documents and photos are included with the report as an aid to understanding how the program functions.
Please note that any mention within this report of American Medical Response (AMR) is in reference to the Company's Operations located in Multnomah and Clackamas Counties in Oregon as well as Clark and Cowlitz Counties in Washington State. This Program currently has no formal function in any other operation within American Medical Response.
Acknowledgements
Recognizing that CISM is a community effort, developing and maintaining a meaningful program is dependent upon the support of everyone in an organization. Along the journey to this first anniversary a number of folks have been generous with their time, effort, personal skills, and moral support. Therefore, I would like to acknowledge and thank the following people: Pontine Rosteck, former Clinical and Educational Services (CES) Manager, who had the vision to include all four counties in the bargaining unit in the original CISM Program back in 2005; Randy Lauer, General Manager for AMR NW Oregon and SW Washington, who took the risk of allowing a street medic to function as coordinator of the program and secured the funds necessary to get the project off the ground; Paul Priest, Director of Operations in Multnomah and Clackamas Counties, who gave approval for providing catered lunches at team meetings, shift coverage for team meetings and pre-incident education presentations, and office work days for the coordinator; Liz Upton, Administrative Assistant for Multnomah and Clackamas County Operations, who instigated and arranged to have meals provided for the CISM Team during meetings and reserved meeting space; The folks at the International Critical Incident Stess Foundation (ICISF), who, having weathered misunderstanding of and opposition to their mission as well as a recent economic downturn, have provided a template for this program and helped locate our course instructor; Tim Dietz, Licenced Professional Counselor (LPC) and Recognized ICISF Instructor, who skillfully got the CISM Team off to a strong start with his steller course on crisis intervention and peer support, and his pointing Drew Prochniak in our direction; Drew Prochniak, LPC, who has been generous with his time and moral supportof the program without which the program would not exist. Drew has ridden with crews on his own time and even shaved his beard in order to be fit tested; Tifphany Hofstetter, Paramedic, who endured long hours sitting inthe ambulance listening to my half baked ideas and rantings, edited several defining documents for the program, and provided valuable feedback throughout the months leading up to the lauch of the program; Melody Lang, my wife and best friend, who has endured my ranting, mood swings, and interruptions and continues to believe in this project. Ultimately, the back bone and worker bees of this program are the members of the CISM Team: Jeff Beck, Lori Moorison, Nicole Beaulaurier, Alice' Hall, Julie Bolt, Mark Jones, Ed Palmer, Gary Laurent, Aaron Botteron, Mary Watson, Derek Stekhuizen, Jody Caprino, and Lewis Coleman. These are the people who face the same perplexing situations in the performance of their duties as the peers they seek to support. The peer counselors are exposed to all of the same critical incident stress, cumulative stress, and the stresses of their personal lives all the while making themselves available to their peers when the chips are down. The program exists because they said 'yes' to providing this service. These team members are among my favorite peoplein the whole world. Thank you..... and be safe.
A History of CISM at AMR
In March of 2005 Pontine Rosteck, Clinical and Educational Services (CES) Manager, was given the responsibility for establisihing a CISM Program at AMR. The motivation for this was a stipulation in the renewed Clark County, WA Ambulance Service Area (ASA) contract which required AMR to have a CISM Program in place for the Clark County Operation. Ms. Rosteck decided to establish a CISM program which would serve all Operations in the collective bargainng unit: Clark and Cowlitz Counties in Washington State, Clackamas and Multnomah Counties in Oregon.
Ms. Rosteck recruited a number of employees to take a two day course in crisis intervention and to serve as peer counselors in the program. Employees volunteered their time spent in the class as no funding was made availiable for compensation. The course was held on April 21-22,2005. A group of field employees and supervisors attended a two day course on CISM, crisis intervention, and peer support. Sam Bradley and Leslie Simmons, EMS Supervisors from AMROperations in California served as co-instructors using curriculum developed by the International Critical Incident Stress Foundation (ICISF). Those in attendance included Dale Courson, Ken Garrett, Gary Laurent, Lindsi Huff, Bill Lang, Dusty Nichols, Lori Paoli, Heather Tucker, Pontine Rostek, and Alice' Hall.
After this training event little organization or activity took place that the peer counselors were aware of. The peer counselors saw little to no utilization of their newly acquired crisis intervention skills.
On September 23, 2005 a CISM Team Meeting commenced and a Dispatch Activation Protocolwas presented as a means to provide service to the workforce. Deployment and scheduling of peer counselors was also discussed with no tangible plan resulting from the discussion.
Ms. Rosteck convened two additional team meetings to re-establish the CISM program on July 21, 2009 and January 22, 2010. Both of these meetings focused on how to best develop and maintain the CISM program as it continued to struggle to become a viable resource for the workforce. Ms. Rosteck indicated that to have an employee from the field coordinate the program may be a better option as she was finding that being in the role of both CES Manager and CISM Program Coordinator had created a perceived conflict of interest as well as an unmanageable work load. Additional discussion took place regarding the need to identify a Mental Health Professional (MHP) to partner with the program for the purposes of referral and oversight. During this time Requests For Proposals (RFP) were solicited from the Mental Health Network (MHN), the Employee Assistance Program (EAP) vendor for most of AMR operations across the country and from Public Safety EAP, the EAP Vendor for several AMR operations on the East Coast. MHN submitted a proposal for full time employees (excluding part time employees) at a cost of $12,000 to $18,750 in the first year. Public Safety EAP submitted a proposal for all employees at a cost of $6,350 to $9,150 in the first year. It was determined that neither proposal was feasible because neither vendor had a physical presence inthe local service area.
In November, 2010 Pontine Rosteck, CES Manager was laid off without notice to the CISM Team and her position was eliminated. The leadership of the program was not transferred to anyone else in the company. No information regarding the future of the CISM Program was made available and the program went into dormancy.
The CISM Program ceased to function after the CES Manager was laid off. Between 2010 and 2013 this writer was asked by management, on occasion, to meet with field personnel for CISMdefusing after exposure to various critical incidents. This writer attempted to make it clear to management that this approach was not a CISM Program and that liability was increased by not having a partnership with a culturally competent MHP for the purpose of providing program oversight and to receive referrals.
In 2011 and 2012, casual conversations between this writer and Randy Lauer, General Managerfor AMR in NW Oregon and SW Washington, took place in which the possibility of appointing a field employee for the position of coordinator of the CISM program was discussed.
On June 25, 2012 a meeting was held as a 'CISM Program Development Focus Group.' Several members of the management team including, Phil Moyer, David Barker, Dave Fuller, (Randy Lauer was unable to attend), Frank Hiltebrand, Teamsters Shop Steward and this writer were in attendance. A discussion took place regarding whether or not the Company would compensate peer counselors for performance of duties while off duty. A few members of the management team stated that this work should be perfomed on a volunteer basis with no financial compensation. This writer maintained that peer counselors should be compensated for their time if performing peer counselor duties while off duty for the benefit of employees and the Company. No agreement was reached at that time. There was also renewed discussion regarding RFPs from Public Safety EAP and MHN to design and administer a program. NeitherRFP submission appeared to be promising as neither agency had personnel physically located in the region to effectively facilitate a program.
No further action was taken until November 29, 2012, when Randy Lauer recruited this writer to serve as coordinator with the mission of restaring the program. This writer began writing a program mission statement and goals, job descriptions for the position of coordinator and peer counselor, and began a search for possible therapists in the local community to partner with the program for MHP referral and oversight.
The ICISF provided assistance with identifying a Recognized ICISF Instructor to teach the course entiled 'Individual Crisis Intervention and Peer Support.' Tim Dietz, Licensed Professional Counselor (LPC), was contacted and plans were made for him to teach the course at AMR once the CISM Team Members were identified. Mr. Dietz suggested that peer counselors be recruited through a nomination process. Nomination forms were distributed to the work force asking each employee to name up to three coworkers whom they would want bytheir side if they were in crisis. From these nominations the top fifteen were identified. There was a commitment to having a number of peer counselors from each county Operation and Communications based roughly on the size of the Operation. Managers in each Operation and Communications were contacted and endorsements of peer counselor candidates were obtained.
This would mean that the peer counselors on the CISM Team would be nominated by peers andendorsed by management.
This writer spoke with numerous people from the mental health community in hopes of identifying a therapist who would be willing to partner with the program and be (or be willing to become) culturally competent in the realm of Emergency Medical Services (EMS). In January, 2013 Drew Prochniak, LPC, contacted this writer stating that he was new to the area and was setting up a practice specializing in first responder issues. Mr. Dietz had conveyed to Mr. Prochniak of the need for a therapist to partner with the program. After several conversations with Mr. Prochniak, an interview with Mr. Lauer, and reference checks, Mr. Prochniak agreed to serve as the MHP resource for oversight and referral for the program.
Because there was no funding provided for retaining the services of a MHP, it was decided that the therapist would be reimbursed through the current EAP vendor. At this time AMR had a national contract for EAP services with MHN (Mental Health Network). The process for establishing Mr. Prochniak on the provider network proved to be long and arduous. After six months of lengthy telephone and email conversations with representatives from MHN, Mr. Prochniak was finally added to the provider network. The program was one step closer to launch with the infrastructure in place connecting employees to professional therapy. Mr. Prochniak volunteered his time obtaining the required immunizations, fit tests, and OSHA course work in order to ride with ambulance crews in the field. Mr. Prochniak was hosted by crews in Clark, Clackamas, and Multnomah Counties for a first hand experience of a typical work day in the EMS field.
The original activation procedure, written in 2005, had been adopted as a company policy. It called for the on duty Controller and Communications Supervisor to be an integral part of the activation procedure. Several meetings were held with this writer and Kim Earls, Communications Supervisor, who was appointed for this task by Kevin Anderson, Director of the Communications Center, for the purpose of updating the policy to fit current needs. At a meeting to finalize the revised policy with Kevin Anderson, Paul Priest, Director of Multnomahand Clackamas County Operations, Chad Heidt, Chief Operations Supervisor, and this writer (Kim Earls was unavailable), Mr. Anderson stated that it would not be feasible for the Communications Center to be involved in the activation of the CISM peer counselors, after all. An alternative activation procedure was written by Chad Heidt which called for the on duty supervisor to locate and activate an on duty peer counselor. The supervisor would contact neighboring county Operations if no peer counselors were available in the county where the activation was needed. If no peer counselors were on duty anywhere in the service area, off duty peer counselors would be contacted by the supervisor.
Nominations for peer counselor were solicited from the workforce. Approximately one hundredseventy names were submitted, tabulated and ranked, based on the number of nominations eachnominee received. Supervisors of nominees were consulted for the purpose of endorsement. The top nominees were contacted and recruited to serve as peer counselors. The original goal was to assemble a team of fifteen peer counselors including the Coordinator. But one nominee withdrew from participation too close to the course date to allow for recruitment of an
additional nominee. The charter members of the CISM Team include: (Paramedics) Jeff Beck, Cowlitz; Alice'Hall, Clark; Lori Moorison, Clark; Julie Bolt, Clark; Niccole Beaulaurier, Clark;Gary Laurent, EMS Supervisor; Aaron Botteron, Multnomah; Ed Palmer, Multnomah; Mark Jones, Multnomah; Bill Lang, Coordinator; Jody Caprino, Clackamas; Lewis Coleman, Clackamas; Derek Stekhuizen, Clackamas; (Emergency Medical Dispatcher) Mary Watson, Communications; and (MHP) Drew Prochniak, LPC.
Once the CISM Team members were identified the 'Individual Crisis Intervention and Peer Support' course was scheduled. This writer spoke with Tim Dietz, LPC, Recognized ICISF Instructor, about the uniqueness of EMS personnel employed by a private sector ambulance service. Mr. Dietz designed a course which was received with great enthusiasm by those in attendance. The two day course was held in the training room at the AMR Multnomah County Operations Center on March 10-11, 2014. A catered lunch was provided by Paul Priest, Director of Multnomah and Clackamas Operations. Drew Prochniak, LPC was present for part of the course and made a presentation on the nature of his practice and his role within the program.
The program went live on March 17, 2014. During the first year of operation the program has enjoyed anectdotal wide spread acceptance. Peer Counselors have been activated by supervisors, have self activated when indicated, and have been contacted directly by coworkers.Peer counselors have addressed critical incident stress, cumulative job stress, and have assisted coworkers with personal problems.
Drew Prochniak, LPC obtained the required OSHA training and fit testing of personal protective equipment in order to ride with on duty crews. Mr. Prochniak rode with crews on four occasions in Clark, Clackamas, and Multnomah Counties during the first year of service. Anumber of employees have benefited from professional counseling offered by Mr. Prochniak via peer counselor referral.
Pre-incident education was provided during the first year of service in several ways. Presentations on CISM were made to new employees during New Employee Orientation and tothe River Rescue Academy by Aaron Botteron and this writer. Lucie Drum, Community Education Director and Public Information Officer for AMR, wrote articles introducing the program to the workforce. These articles were published in “The Parascope,” AMR's monthly newsletter.
In October of 2014, this writer received the 'EMS Commitment to Quality Award' from the EMS and Trauma Systems Section of the Oregon Health Authority at the Oregon EMS Conference in Salem.
In December of 2014, it was discovered that AMR had discontinued its' national contract with MHN and established a new contract with Public Safety EAP to administer the Company's EAP. This created an unexpected challenge as the process of having Mr. Prochniak accepted on the new provider network needed to be expedited so as to not have an interruption of benefits toemployees. The situation also created additional work communicating the changes in access to
EAP services to the workforce. In January of 2015, the 'EMS10 Innovation in EMS Award' was received from the Journal of Emergency Medical Services/Physio Control at the EMS Today Conference in Baltimore, MD. An article about the program was published in JEMS magazine in March, 2015. Since then, several collegues in EMS from other regions of the U. S. have contacted this writer expressing interest in the program.
On January 27, 2015, this writer made a presentation on the CISM Program and participated ona Q and A panel at the Peer Support Conference in Salem which was sponsored by the Oregon Patient Safety Commisssion.
Two team meetings were held during the first year providing continuing education, program development, and team building. This writer occasionally publishes the 'Hug Squad News,' a newsletter for the CISM Team. It is limited to one page and is distributed to the CISM team as an email attachment. It's purpose is to communicate with team members in a way which is tangible yet brief. It's byline is: 'News and continuing education for the AMR CISM Team.' A joke is included in each issue to remind team members that humor is an important part of maintaining good mental health.
The Program continues to evolve through the experience of trial and error as efforts are made todevelop, maintain, and make accessible the primary components of CISM to a large, geographically dispersed workforce functioning within several distinct operational units.
Program Mission
The mission of the CISM Program is to provide crisis intervention and peer support, access to culturally competent Professional Mental health services, and critical incident and cumulative stress education for Emergency Medical Services (EMS) field, communications, and management personnel, as well as their family members/significant others.
Program Goals
The program shall assist employees in the management and reduction of the negative effects of acute psychological stress due to exposure to critical incidents and cumulative stress due to chronic exposure to generally stressful situations encountered in the EMS work environment.
The program shall provide education for EMS field employees, Communications employees, Management, and their family members/significant others on the subject of critical incident stress, cumulative stress, symptomology of stress, and strategies to manage stress.
The program shall provide barrier free access to culturally competent professional mental health services.
Program Objectives
The program shall develop and maintain a CISM Team which includes representatives from Operations, Management, and Communications, a Program Coordinator, and a Mental Health Professional. This team shall be trained in crisis intervention and peer support using curriculum developed by the International Critical Incident Stress Foundation. Team members shall be identified by soliciting nominations from the field, communications, and management followed by endorsement from management. Team members shall be available while on duty to offer peer support and defusing of critical incidents. The CISM Team shall meet at least semiannually for the purposes of professional mental health oversight, continuing education, and mutual support.
The program shall be led by a coordinator who will provide program development and administration as well as moral and educational support for the CISM Team.
The program shall develop and maintain a formal relationship with a Licensed Mental Health Professional (MHP) in the community of service who shall be (or become) culturally competent and shall be identified as a provider in the Company's EAP for the purposes of reimbursement. The MHP shall be given the opportunity to participate in ride alongs in the field and shall have access to Company facilities.
The program shall develop and present Pre-incident Educational opportunities for employees via New Employee Orientation and other continuing education venues offered by the Company.
The program shall develop specialized support services for employees who are veterans of the military in conjunction with the Veterans Administration.
The program shall develop specialized support services and educational opportunities for family members/significant others of employees in the understanding and management of critical incident and cumulative stress.
Program Design and Features
Critical Incident Stress Management (CISM) is a program which enables EMS personnel to effectively manage acute stress and cumulative stress associated with the EMS work environment. EMS personnel encounter incidents which are out of the ordinary and generate an unusually high level of stress. How one responds may affect how well one functions as an EMS professional and in one's personal life. Historically, EMS personnel have experienced a high incidence of failed relationships, early career burnout, and changes in personality which correlates with the experience of having one's coping mechanisms overwhelmed by critical incident stress and cumulative stress. While CISM is not a cure all, it is hoped that by establishing a functioning program, EMS personnel can assist each other. Criticalincident stress and cumulative stress can be considered the byproduct of the EMS environment. It is a normal response to an abnormal circumstance. What does one do with this byproduct of managing other peoples' crisis? It is similar to the process of manufacturing which produces a toxic derivative. If the byproduct of manufacturing is not neutralized the manufacturer will end up with a hazmat incident. The same could be true of the EMS profession. Without neutralization one's coping mechanisms become overwhelmed and eventually demand one's full attention to the detriment of one's overall mental and physical health.
The following features of the CISM Program:
It is overseen by a Mental Health Professional (MHP). The MHP will participate in ride a longs, be educated in the unique environment of the EMS field and be available for further individual counseling through AMR's Employee Assistance Program. The MHP will also be present to oversee any formal critical incident stress debriefing (CISD) meetings which involve a group of responders. Drew Prochniak, Licensed Professional Counselor (LPC), has agreed to serve in this capacity. Drew specializes in treating First Responder stress and comes from a public safety family (his father is a retired police officer and his brother is a paramedic). Drew is a Wilderness First Responder and also has a background in Search and Rescue. He was a member with, and CISM resource for, the Southern Arizona Search and Rescue Association before relocating to Portland.
It is peer based. Peer Counselors (PC) are nominated by their coworkers. After completing a 16 hour training course PCs will provide initial defusing with individuals lasting approximately 30 minutes. A defusing is a more informal meeting than a debriefing which is a longer event usually involving larger groups of responders. PCs provide emotional first aid to their coworkers and may refer individuals to a MHP.
It is emotional first aid. CISM is to psychotherapy what EMS is to surgery. It is not psychotherapy and does not replace psychotherapy provided by a MHP.
It is confidential. All CISM services are confidential and are regulated by the Healthcare Information Portability and Accountability Act (HIPAA).
It is credentialed. The program model and curriculum is drawn from the International Critical Incident Stress Foundation. Related training qualifies for Continuing Medical Educational (CME) credit.
It is voluntary. There is no requirement to participate in the program in any way.
It is accessible. Peer Counselors will be available for defusing within hours of activation. During defusing, issues generated by the critical incident can be identified and information and resources can be provided by the PC. Anyone can activate CISM services by calling the on dutysupervisor or by contacting a PC directly. PCs will be utilized primarily while on duty. If no PC is on duty then an off duty PC will be contacted. Additionally, PCs can respond across county and state boundaries. This program will serve AMR personnel in Clackamas, Clark, Cowlitz, and Multnomah Counties as well as the Communications Center, Special Services Division, andSpecial Teams.
Mock CISM Activation Scenario
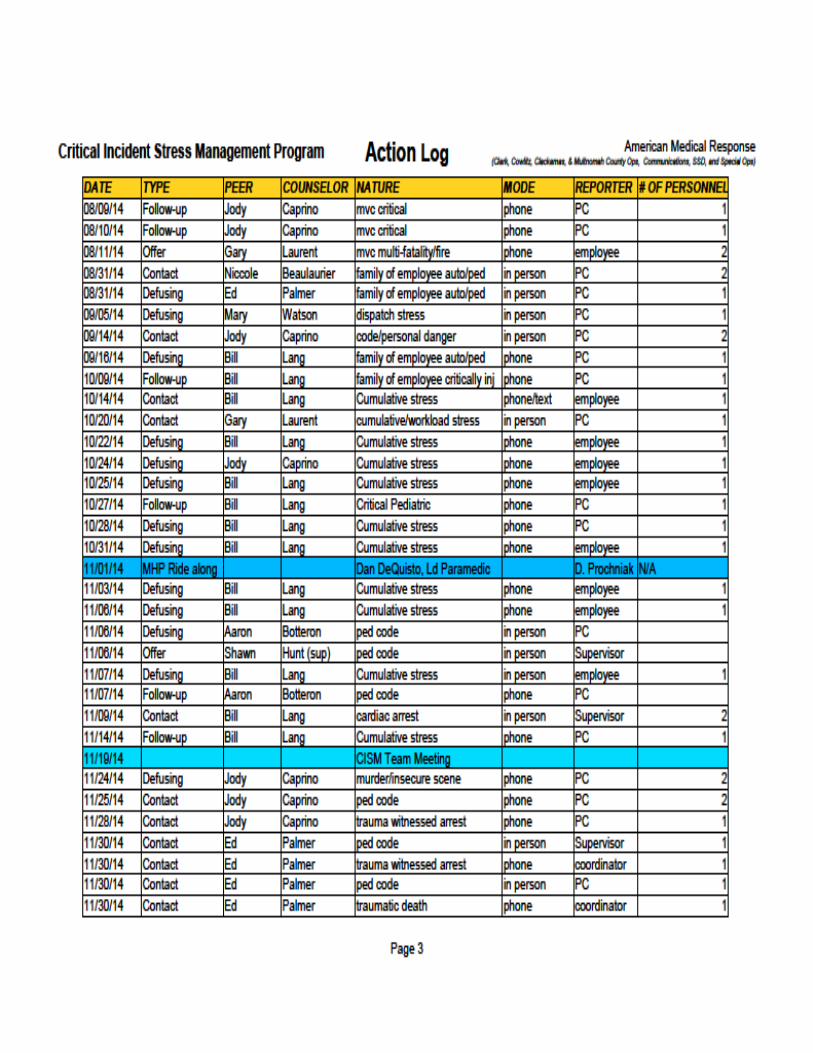
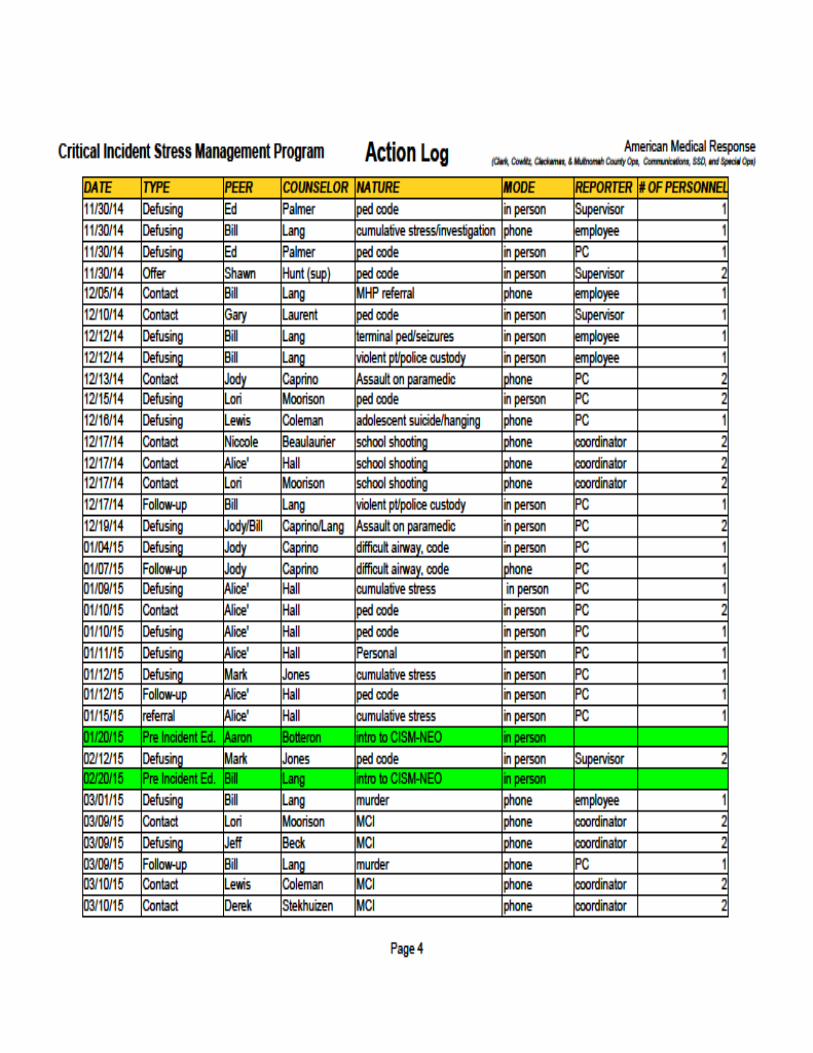
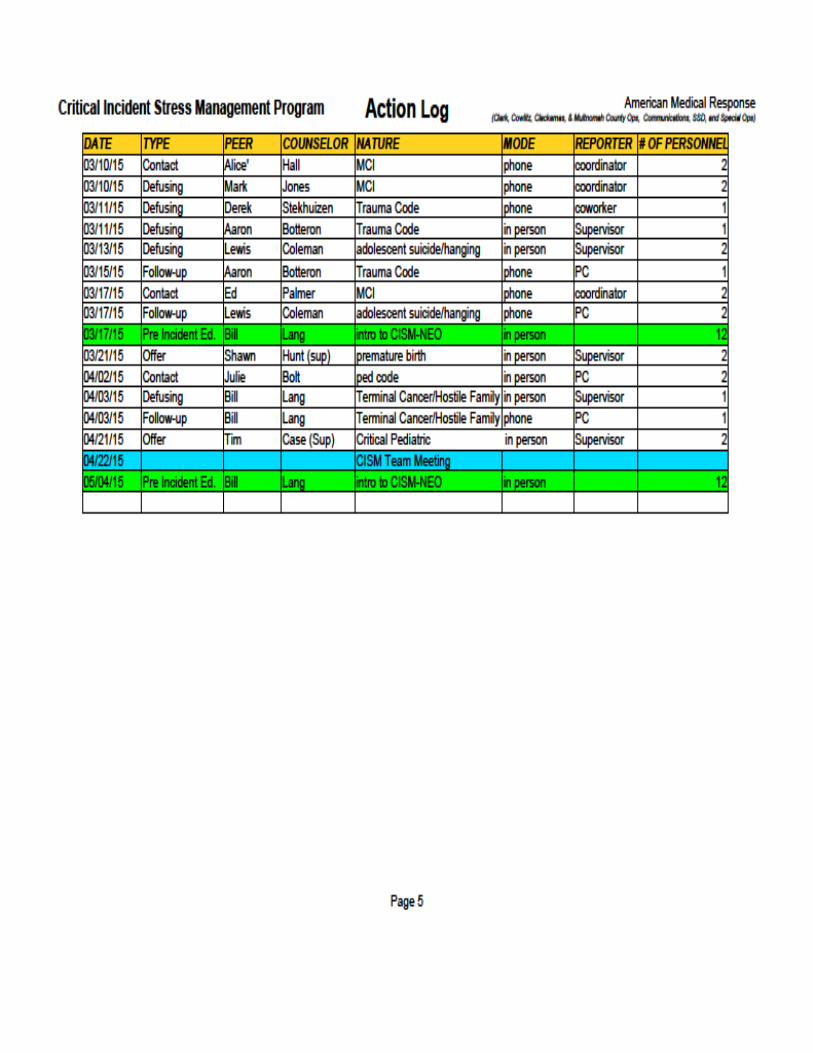
Medic 51 responds to a Murder/Suicide involving a child. The on duty supervisor hears the call dispatched (or is notified by an astute dispatcher or other personnel). The Supervisor instructs the dispatcher to keep Medic 51 out of service after the call. The supervisor contacts Medic 51 after the callto offer CISM services or simply keeps the crew out of service if critical incident exposure is obvious. If a CISM Activation is indicated the supervisor refers to the CISM Team Roster to identify a peer counselor who is on duty. The Supervisor then puts the peer counselor's unit out of service, contacts thepeer counselor and offers as much information about the incident as is available. The supervisor then arranges for private meeting space for a Defusing. The peer counselor meets with the crew and follows (as much as possible) the SAFER-R Model of Crisis Intervention (See the International Critical Incident Stress Foundation for an explanation of the SAFER-R Model, icisf.org) and assists the crew with understanding stress symptoms, making a self care plan, and referral to the MHP if indicated. The PC provides the crew with Critical Incident Stress Information Sheet (handout) and contact informationfor the MHP. The PC then offers to make a follow up call within one week. The crew and the PC decideif the crew will be relieved of duty for the remainder of the shift or go back in service. (AMR pays out the entire shift if the crew remains out of service after a critical incident so the crew does not suffer a loss in pay). The PC reports the work status of the crew to the activating supervisor and reports a CISMactivation to the CISM Program Coordinator. The coordinator documents the action in the CISM Action Log. The identities of those served are not documented in order to maintain confidentiality.
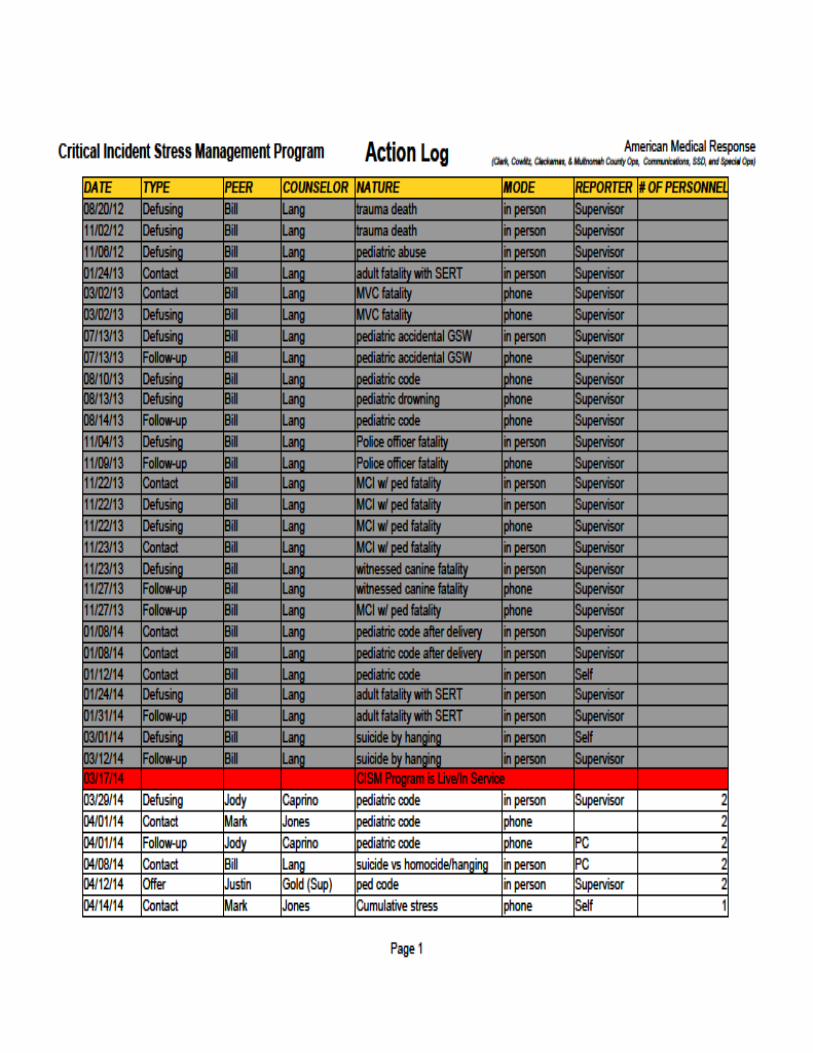
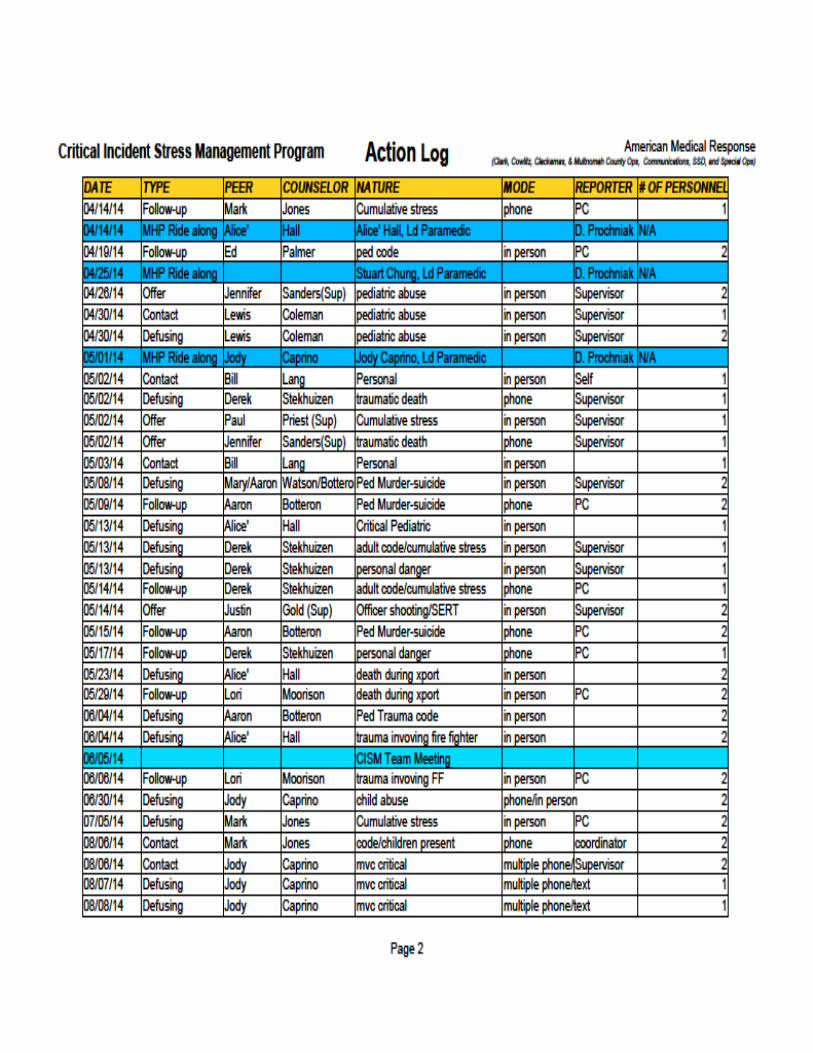
Summary of Action LogMarch 17, 2014 to March 16, 2015
Offers of Peer Support made by Supervisor: 7
Peer Counselor Contacts with Employees: 37
Defusings conducted: 46
Follow-Up Calls made by Peer Counselors: 19
Referrals to MHP by Peer Counselors: 2 (Without additional services)
MHP Ride Along: 4
Team Meetings held: 2
Pre-incident Education provided-New Employee Orientation Classes: 2 ClassesRiver Rescue Academy: 1
Glossary of Termsfor
CISM Action LogShaded fields-
Actions in Brown: MHP ride along
Actions in Grey: Actions performed before the official launch of the current Program.
Actions in Blue: Team development such as Team meetings for the purpose of mutual support, continuing education, interaction with the MHP.
Actions in Green: Actions having to do with Pre-incident Education. Includes presentations on CISM at New Employee Orientation, Continuing Education Inservices, and othervenues where education on crisis intervention, peer support, mental health therapy and information about the CISM Program are presented.
Abbreviations-
LPC: Licensed Professional Counselor. One of several credentialed Mental Health Professionals.
MHP: Mental Health Professional. Can be a LPC or other Mental Health Professional such as a Licensed Clinical Social Worker.
MVC: Motor Vehicle Crash
MCI: Mass Casualty Incident
NEO: New Employee Orientation
Sup: Supervisor. In this case, EMS Supervisor.
PC: CISM Team Peer Counselor. EMS personnel and EMS supervisors trained in crisis intervention. PCs provide psychological first aid to coworkers.
Ld: Lead. In this case Lead Paramedic
Code/ Ped Code: Cardiac arrest/ cardiac arrest involving a child
FF: Fire Fighter
+ symbol Indicates an additional, unrelated issue issue
TBGJ: Testify Before Grand Jury
Glossary of Termsfor
Action Log Continued
SERT: Special Emergency Responce Team (Law Enforcement)
Xport: Transport by ambulance.
Terms-
Contact: When a peer counselor contacts an employee in person, telephonically, via text or email, offering peer support.
Defusing: An informal meeting between a peer counselor and 1-4 employees for the purpose of providing peer support, stablization, acknowledgment of a critical
incident, facilitation of understanding of stress symptoms, management of stress, and referral to a mental health professional, if indicated.
Follow Up: Contact made by a peer counselor with an employee withing one week after a defusing with a three part question; 'How are you doing? Better, worse, or about the same?' Assessment for the need of additional services is made at this time.
MHP Ride Along: When the mental health professional rides with an ambulance crew in the field for the purpose of getting to know employees and gaining first hand knowledge of the EMS work environment. This is an opportunity for the MHP to develop cultural competency and for EMS personnel to understand the work and role of the MHP in CISM.
Offer: Offers to activate a peer counselor for defusing/peer support made by a Supervisor but the employee declines.
Job Description
Job Title: Peer Counselor Reports To: Operations Supervisor
Department: Operations Location: Multnomah County
Position Status: Volunteer
POSITION SUMMARY:
The mission of the CISM Program is to provide emotional and psychological support to field and dispatch personnel as they deal with the unique critical incident and cumulative stress encountered in the Emergency Medical Services (EMS) work environment. The foundation of the program is peer based with the guidance and oversight of a Mental Health Professional (MHP). Peer Counselors (PC) are the first line providers of support to employees. PCs assess, provide emotional first aid, and referral to a MHP when appropriate, and follow up contact.
Essential Duties and Responsibilities:
1. Attend an initial company sponsored Peer Counselor Training Course (approximately 16 hours). Employees attending the course during their regularly shift will have their shift covered by the company. Employees taking the course while off duty will be paid at their applicable training pay rate. Training hours for the course are included within the 24 CE hour afforded to employees through the collective bargaining agreement.
Attend quarterly CISM Team meetings in order to address program issues, interact with the MHP, offer and receive moral support with other PCs, and obtain continuing education for PC skills development.
Adhere to the AMR confidentiality agreement understanding that any interaction with employees in the context of a CISM activation or speaking with an employee while in the role of a PC is protected by HIPAA confidentiality laws.
Be available for CISM activations while on duty. This may involve making contact with the employees in person or by phone at the PCs earliest convenience to assess the need for a Defusing. The PC may be taken out of service from regular duties by the on duty supervisor in order to meet with employees at a location identified by the on duty supervisor to provide a CISM Defusing. The Defusing gives the personnel an opportunity to explore the incident and identify stress symptoms they may be experiencing, The PC will offer emotional support, provideinformation regarding the nature of critical incident stress, information on self care while experiencing stress, and contact information for the MHP if therapy is desired.
Make contact by phone or in person with employees within one week after a Defusing for follow up.
Make a report of the CISM contact and/or Defusing and forward the report to the CISMCoordinator.
Minimum Qualifications:
Education/Licensing/Certification: Current EMT-Basic, EMT-Intermediate, EMT-IV/Airway, or EMT-Paramedic License.
Experience: Minimum 3 years experience working in the EMS field or communications center.
Knowledge and Skills: Respected among peers and and in good standing with the Company. An understandingof the unique emotional and psychological stress among EMS Personnel. Previous experience working with a CISM program desired.
DATE: October 24, 2013
TO: Communications and Operations Personnel
FROM: Bill Lang
RE: CISM Peer Counselor Nominations
Nomination Formfor
Peer Counselor
Critical Incident Stress Management Program (CISM)AMR Communications and Operations
As an AMR operations or communications employee you are invited to nominate those persons from among your co-workers to serve as peer counselors in the developing CISM Program. The peer counselor (PC) will be deployed generally while on duty to provide a defusing with personnel after encountering a critical incident. A defusing is a short, informal meeting lasting approximately 30 minutes during which personnel may talk about the incident, explore its' effects, and identify symptomsof stress. The PC may then provide information on coping skills, provide peer to peer support, and make a referral to a Mental Health Professional (MHP) if appropriate. Keep in mind, the best person for this role may not be your best friend or the most popular coworker. When making your nominationsconsider the attributes which are needed to function effectively as a peer counselor. The persons you nominate will be considered for the position of Peer Counselor based on the following skills and attributes:
- Effective listening skills - Respected among coworkers- Trustworthiness - Maintains confidentiality- Dependability - Respects privacy
You are encouraged to nominate up to 3 individuals.
My nomination for CISM Peer Counselor: 1.__________________________________ 2.__________________________________ 3.__________________________________
My county of employment:___________________________________
Hard copies of nominations can be sent via interoffice mail to Bill Lang at Multnomah County AMROperations or sent via email to [email protected] by November 25, 2013.
MEMORANDUM
CISM ProgramPeer Counselor Activation Procedure
The purpose of the CISM Program is to provide peer support and professional mental health follow up for employees experiencing critical incident and cumulative stress. The goal of the program is to restore employees to full functioning both personally and professionally.
Please utilize the following procedure when you encounter employees who are experiencing critical incident stress or cumulative stress. This procedure facilitates a private, confidential meeting with a peer counselor away from work responsibilities for the purpose of defusing critical incident and cumulative stress symptoms experienced by employees.
Place affected crew out of service. Review your county system status level and peer counselor list to determine if you will be able
to utilize an in County peer counselor.◦ If you are able to spare the resources and have a peer counselor on duty, notify the peer
counselor and give as much of the call information as you can. Determine if a follow upphone conversation is needed or if both crews need to be placed 10-7 for a defusing.
◦ If you are unable to spare a peer counselor resource or do not have one on duty, pleasecontact the duty supervisor or your sister operations to locate an available peer counselor.
◦ In the event there are no on-duty peer counselors available, please contact off dutymembers to see if they are available to assist.
If a face to face defusing is required, please arrange for a safe and private place for this tooccur.
Please e-mail your supervisor team, including Operations Chief and Manager as well as theCISM Coordinator. This e-mail should include the following.◦ Incident classification, IE: Ped Code, Homicide, MCI, etc. ◦ The affected employees.◦ The peer counselor assigned.◦ Time you were notified.
Additional Guidelines:
These matters are confidential and our crew members should be effectively treated as patients as itpertains to their protected health information.
Often those affected will not be able to return to work. You should make appropriate staffingaccommodations accordingly.
Only those directly involved in the incident and the Peer Counselor are to be present during theDefusing.
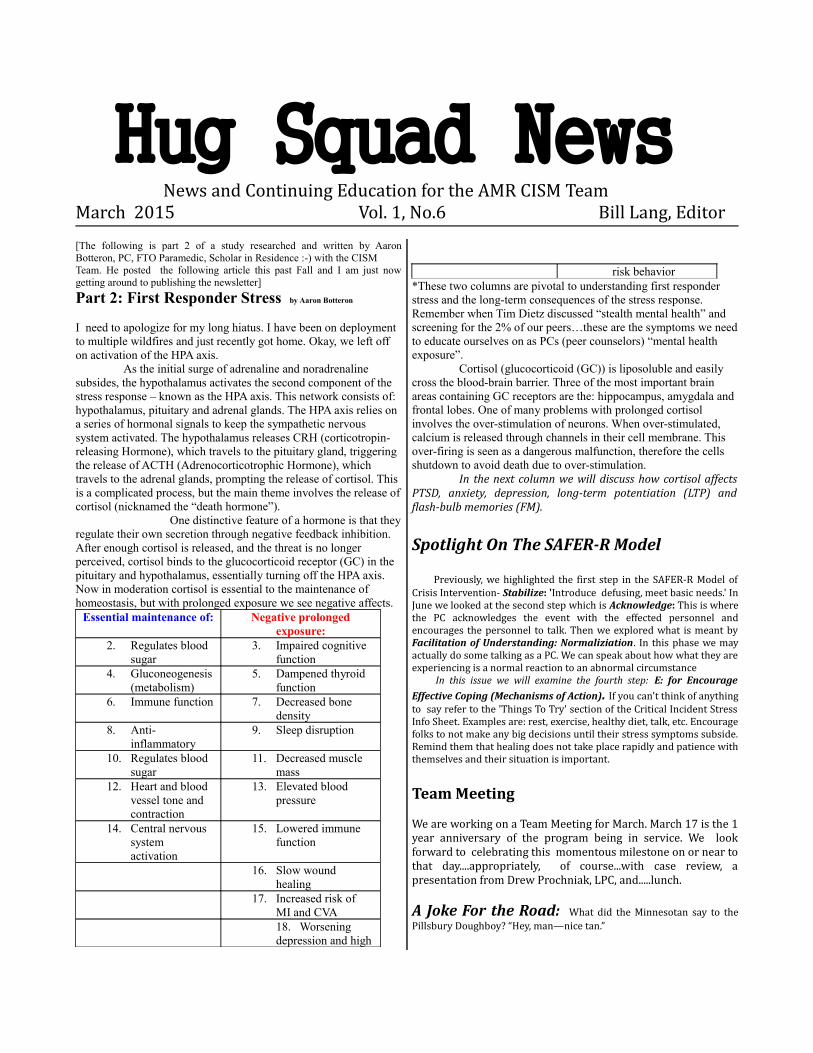
Hug Squad NewsNews and Continuing Education for the AMR CISM Team
March 2015 Vol. 1, No.6 Bill Lang, Editor [The following is part 2 of a study researched and written by AaronBotteron, PC, FTO Paramedic, Scholar in Residence :-) with the CISM Team. He posted the following article this past Fall and I am just nowgetting around to publishing the newsletter]
Part 2: First Responder Stress by Aaron Botteron
I need to apologize for my long hiatus. I have been on deployment to multiple wildfires and just recently got home. Okay, we left off on activation of the HPA axis.
As the initial surge of adrenaline and noradrenaline subsides, the hypothalamus activates the second component of the stress response – known as the HPA axis. This network consists of: hypothalamus, pituitary and adrenal glands. The HPA axis relies on a series of hormonal signals to keep the sympathetic nervous system activated. The hypothalamus releases CRH (corticotropin-releasing Hormone), which travels to the pituitary gland, triggering the release of ACTH (Adrenocorticotrophic Hormone), which travels to the adrenal glands, prompting the release of cortisol. This is a complicated process, but the main theme involves the release ofcortisol (nicknamed the “death hormone”).
One distinctive feature of a hormone is that theyregulate their own secretion through negative feedback inhibition. After enough cortisol is released, and the threat is no longer perceived, cortisol binds to the glucocorticoid receptor (GC) in the pituitary and hypothalamus, essentially turning off the HPA axis. Now in moderation cortisol is essential to the maintenance of homeostasis, but with prolonged exposure we see negative affects.
Essential maintenance of: Negative prolongedexposure:
2. Regulates blood sugar
3. Impaired cognitive function
4. Gluconeogenesis(metabolism)
5. Dampened thyroid function
6. Immune function 7. Decreased bone density
8. Anti-inflammatory
9. Sleep disruption
10. Regulates blood sugar
11. Decreased muscle mass
12. Heart and blood vessel tone and contraction
13. Elevated blood pressure
14. Central nervous system activation
15. Lowered immune function
16. Slow wound healing
17. Increased risk of MI and CVA18. Worsening depression and high
risk behavior*These two columns are pivotal to understanding first responder stress and the long-term consequences of the stress response. Remember when Tim Dietz discussed “stealth mental health” and screening for the 2% of our peers…these are the symptoms we needto educate ourselves on as PCs (peer counselors) “mental health exposure”.
Cortisol (glucocorticoid (GC)) is liposoluble and easily cross the blood-brain barrier. Three of the most important brain areas containing GC receptors are the: hippocampus, amygdala and frontal lobes. One of many problems with prolonged cortisol involves the over-stimulation of neurons. When over-stimulated, calcium is released through channels in their cell membrane. This over-firing is seen as a dangerous malfunction, therefore the cells shutdown to avoid death due to over-stimulation.
In the next column we will discuss how cortisol affectsPTSD, anxiety, depression, long-term potentiation (LTP) andflash-bulb memories (FM).
Spotlight On The SAFER-R Model
Previously, we highlighted the first step in the SAFER-R Model ofCrisis Intervention- Stabilize: 'Introduce defusing, meet basic needs.' InJune we looked at the second step which is Acknowledge: This is wherethe PC acknowledges the event with the effected personnel andencourages the personnel to talk. Then we explored what is meant byFacilitation of Understanding: Normaliziation. In this phase we mayactually do some talking as a PC. We can speak about how what they areexperiencing is a normal reaction to an abnormal circumstance In this issue we will examine the fourth step: E: for Encourage
Effective Coping (Mechanisms of Action). If you can't think of anythingto say refer to the 'Things To Try' section of the Critical Incident StressInfo Sheet. Examples are: rest, exercise, healthy diet, talk, etc. Encouragefolks to not make any big decisions until their stress symptoms subside.Remind them that healing does not take place rapidly and patience withthemselves and their situation is important.
Team Meeting
We are working on a Team Meeting for March. March 17 is the 1year anniversary of the program being in service. We lookforward to celebrating this momentous milestone on or near tothat day....appropriately, of course...with case review, apresentation from Drew Prochniak, LPC, and.....lunch.
A Joke For the Road: What did the Minnesotan say to thePillsbury Doughboy? “Hey, man—nice tan.”


“Happy Birthday Peer Support”Drew Prochniak, LPC, presents a cake to the CISM Team at the team meeting on
April 22, 2015 celebrating the first year of service.
This photo was taken on the second day of the Individual Crisis Interventionand Peer Support Class held at Multnomah County Operations on April 11,2014. The term 'Hug Squad' was originally coined by Carl Lemmon,Paramedic, during a light hearted conversation about the Program. Can EMSpersonnel more comfortably 'embrace' CISM/Peer Support using a humorousterm such as 'EMS Hug Squad?' Time will tell.