Embed Size (px)
Citation preview
CISM 2018 Exam Registration Form—Department of Defense (DoD)
Final Registration: 18 September 2018 Exam Testing Window: 1 June – 23 September 2018
®
INSTRUCTIONS FOR COMPLETING THE CISM DoD EXAM REGISTRATION FORM
To register: Exam registration fees must be paid in full prior to being eligible to schedule a testing appointment. All payments must be received by no later than the final registration deadline. Complete DoD registration form. Return to [email protected].
The exam is administered via computer-based testing (CBT) at testing centers throughout the world. Registered candidates will select their exam location, date, and time through the scheduling procedure. Fully paid candidates will receive scheduling information via email once their registration is complete. A list of the locations where testing centers are available can be found at www.isaca.org/examlocations.
To avoid any delay or the possibility of the registration being canceled, it is extremely important that the registration form be completed in English carefully and correctly. Please print in block letters and black ink.
1. MEMBERSHIP ID—If you are currently a member of ISACA, please enter your member number on the line provided. Although membership in ISACA is not required to take the exam, you may wish to consider a membership at this time and begin to enjoy the cost savings and many other benefits available to you. If you are joining as an ISACA member now, please write “pending” on the line provided for your ISACA membership ID.
2. NAME—Please indicate the appropriate salutation. Your name should be entered as follows: First Name, Middle Initial, Last or Family Name. To prevent delays on the exam date, please use your legal name as it appears on your government-issued ID.
3. If you require special testing accommodations, please indicate by checking the box. Further information and the request form that must also be completed is available at www.isaca.org/specialaccom.
4. CERTIFICATIONS YOU CURRENTLY HOLD—List the certifications you currently hold.
5. RESIDENCE ADDRESS—Enter your home address. Please make sure that your home street address, city, state or province, country, and postal code are recorded in the proper fields.
6. RESIDENCE PHONE AND FAX NUMBERS—Enter your residence telephone and fax numbers, including all applicable area codes, country codes and international dialing codes.
7. BUSINESS NAME—Enter the name of your business.
8. BUSINESS ADDRESS—Enter your business address. Please make sure that your company’s street address, city, state or province, country, and postal code are recorded in the proper fields.
9. BUSINESS PHONE AND FAX NUMBERS—Enter your business telephone and fax numbers, including all applicable area codes, country codes and international dialing codes.
10. EMAIL ADDRESS—Enter your complete email address. Notification of registration, an admission ticket, pass/fail results and score will be distributed via email to all candidates who provide a valid email address.
11. SEND MAIL TO—Check (tick) the appropriate box where all CISM exam correspondence and results are to be mailed.
12. YEAR OF BIRTH
13. FIELD OF EMPLOYMENT—Indicate your current field of employment: 1. Financial/Banking 6. Retail and Wholesale/Distribution 10. Telecommunications/Communications 14. Health Care/Medical 2. Insurance 7. Government/Military 11. Mining/Construction/ 15. Pharmaceutical 3. Public Accounting —National/State/Local Petroleum/Agriculture 16. Advertising/Marketing/Media 4. Transportation 8. Technology Services/Consulting 12. Utilities 17. Education/Student 5. Aerospace 9. Manufacturing/Engineering 13. Legal/Law/Real Estate 99. Other
14. EDUCATIONAL LEVEL—Indicate degree or the number of equivalent years of university-level education: 1. One year or less 4. Four years 7. AS/Associates 10. Doctorate 2. Two years 5. Five years 8. BA/BS/Bachelors 99. Other 3. Three years 6. Six or more years 9. MS/MBA/Masters
15. WORK EXPERIENCE—Indicate the number of years of information security management work experience: 1. No experience 3. 4-6 years 5. 10-12 years 2. 1-3 years 4. 7-9 years 6. 13 or more years
16. CURRENT PROFESSIONAL ACTIVITY—Please select the best match if your exact title is not listed: 1. CEO, President, Owner, 5. CFO, Controller, Treasurer, 10. Compliance/Risk/Privacy 15. IT Staff General/Executive Manager Finance Executive/VP/EVP Director/Manager/ Consultant 16. IT/IS Compliance/Risk/Control Staff 2. CAE, General Auditor, Partner, 6. Chief Compliance/Risk/ Privacy Officer, VP/EVP 11. IT Senior Auditor (External/Internal) 17. Professor/Teacher Audit Head/VP/EVP 7. IT Audit Director/ Manager/Consultant 12. IT Auditor (External/ Internal Staff) 18. Student 3. CISO/CSO, Security Executive/VP/EVP 8. Security Director/Manager/Consultant 13. Non-IT Auditor (External/Internal) 99. Other 4. CIO/CTO, Info Systems/ 9. IT Director/Manager/ Consultant 14. Security Staff Technology Executive/ VP/EVP
17. SIZE OF ENTIRE ORGANIZATION—Indicate the size of your organization (number of employees) at your primary place of business: 1. Fewer than 50 employees 3. 150–499 employees 5. 1,500–4,999 employees 7. 10,000–14,999 employees 2. 50–149 employees 4. 500–1,499 employees 6. 5,000–9,999 employees 8. 15,000 or more employees
18. SIZE OF IT Audit Staff—Indicate the size of your IT audit staff (local office): 1. 0 individuals 2. 1 individual 3. 2–5 individuals 4. 6–10 individuals 5. 11–25 individuals 6. More than 25 individuals
19. SIZE OF INFORMATION SECURITY STAFF—Indicate the size of your information security staff (local office): 1. 0 individuals 2. 1 individual 3. 2–5 individuals 4. 6–10 individuals 5. 11–25 individuals 6. More than 25 individuals
20. YOUR LEVEL OF PURCHASING AUTHORITY—Indicate your level of purchasing authority: 1. Recommend products/services 2. Approve purchases 3. Recommend and approve purchases
21. EXAM LANGUAGE PREFERENCE—Indicate the language version of the exam you desire. English will be assigned if no preference is indicated.
22. HOW DID YOU HEAR ABOUT THE EXAM?—Select how you heard about the CISM exam: 1. ISACA international mailing 2. Chapter mailing 3. Event 4. Magazine 5. ISACA International Headquarters web site 6. Chapter web site 7. Supervisor 8. Colleague (co-worker) 9. Colleague (non co-worker) 10. Social Media Site 11. Other
23. AUTHORIZATION TO RELEASE CONTACT INFORMATION TO THE LOCAL ISACA CHAPTER—Enter Y for yes or N for no to indicate whether you authorize release of your name and address information to a local ISACA chapter for the purpose of promoting chapter-sponsored activities, including study courses. (This is not applicable to ISACA members, individuals joining at this time or exam passers granted provisional membership.)
24. IS CISM CERTIFICATION REQUIRED FOR YOUR CURRENT POSITION OR FOR PROMOTION?—Enter Y for yes or N for no.
25. SIGNATURE—Be sure to sign your form. Failure to do so will result in ineligibility to sit for the exam.
2
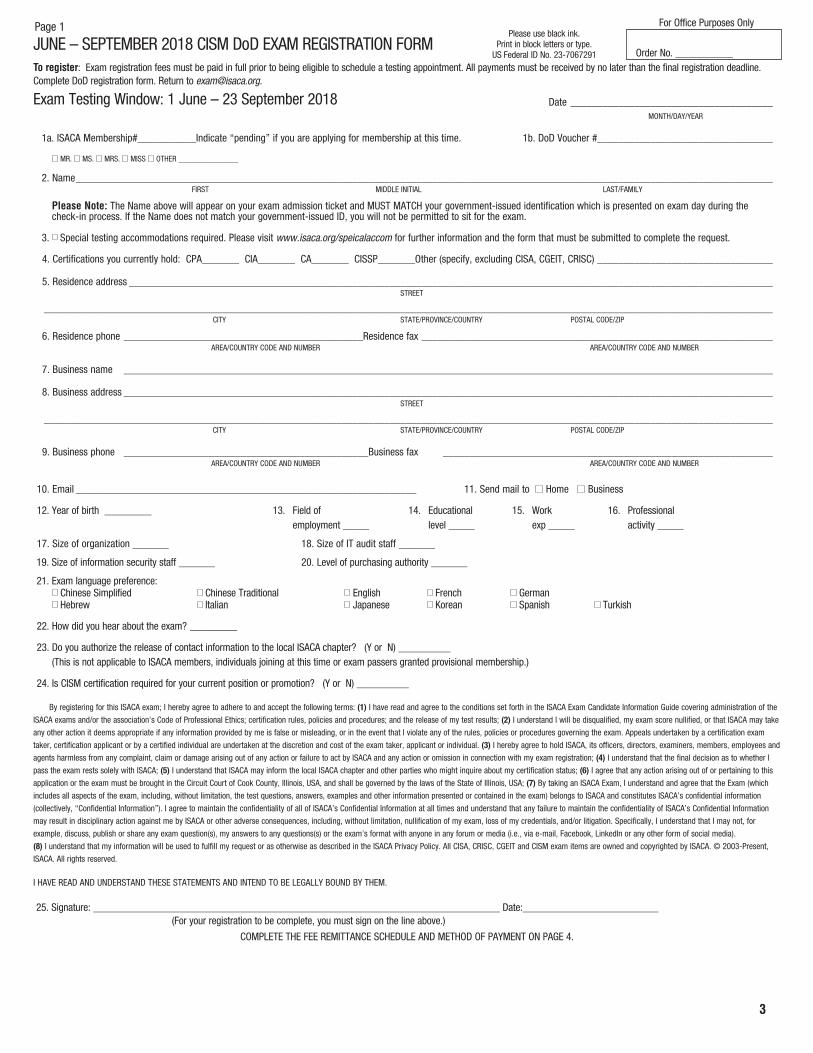
JUNE – SEPTEMBER 2018 CISM DoD EXAM REGISTRATION FORM To register: Exam registration fees must be paid in full prior to being eligible to schedule a testing appointment. All payments must be received by no later than the final registration deadline. Complete DoD registration form. Return to [email protected].
Exam Testing Window: 1 June – 23 September 2018 Date ______________________________________MONTH/DAY/YEAR
1a. ISACA Membership#___________Indicate “pending” if you are applying for membership at this time. 1b. DoD Voucher #_________________________________
MR. MS. MRS. MISS OTHER _______________
2. Name ___________________________________________________________________________________________________________________________________FIRST MIDDLE INITIAL LAST/FAMILY
Please Note: The Name above will appear on your exam admission ticket and MUST MATCH your government-issued identification which is presented on exam day during thecheck-in process. If the Name does not match your government-issued ID, you will not be permitted to sit for the exam.
3. Special testing accommodations required. Please visit www.isaca.org/speicalaccom for further information and the form that must be submitted to complete the request.
4. Certifications you currently hold: CPA_______ CIA_______ CA_______ CISSP_______Other (specify, excluding CISA, CGEIT, CRISC) _________________________________
5. Residence address _________________________________________________________________________________________________________________________STREET
_________________________________________________________________________________________________________________________________________CITY STATE/PROVINCE/COUNTRY POSTAL CODE/ZIP
6. Residence phone _____________________________________________Residence fax __________________________________________________________________AREA/COUNTRY CODE AND NUMBER AREA/COUNTRY CODE AND NUMBER
7. Business name __________________________________________________________________________________________________________________________
8. Business address __________________________________________________________________________________________________________________________STREET
_________________________________________________________________________________________________________________________________________CITY STATE/PROVINCE/COUNTRY POSTAL CODE/ZIP
9. Business phone ______________________________________________Business fax ______________________________________________________________AREA/COUNTRY CODE AND NUMBER AREA/COUNTRY CODE AND NUMBER
10. Email ________________________________________________________________ 11. Send mail to Home Business
12. Year of birth _________ 13. Field of 14. Educational 15. Work 16. Professionalemployment _____ level _____ exp _____ activity _____
17. Size of organization _______ 18. Size of IT audit staff _______
19. Size of information security staff _______ 20. Level of purchasing authority _______
21. Exam language preference:Chinese Simplified Chinese Traditional English French German
Hebrew Italian Japanese Korean Spanish Turkish
22. How did you hear about the exam? _________
23. Do you authorize the release of contact information to the local ISACA chapter? (Y or N) __________ (This is not applicable to ISACA members, individuals joining at this time or exam passers granted provisional membership.)
24. Is CISM certification required for your current position or promotion? (Y or N) __________
By registering for this ISACA exam; I hereby agree to adhere to and accept the following terms: (1) I have read and agree to the conditions set forth in the ISACA Exam Candidate Information Guide covering administration of the
ISACA exams and/or the association’s Code of Professional Ethics; certification rules, policies and procedures; and the release of my test results; (2) I understand I will be disqualified, my exam score nullified, or that ISACA may take
any other action it deems appropriate if any information provided by me is false or misleading, or in the event that I violate any of the rules, policies or procedures governing the exam. Appeals undertaken by a certification exam
taker, certification applicant or by a certified individual are undertaken at the discretion and cost of the exam taker, applicant or individual. (3) I hereby agree to hold ISACA, its officers, directors, examiners, members, employees and
agents harmless from any complaint, claim or damage arising out of any action or failure to act by ISACA and any action or omission in connection with my exam registration; (4) I understand that the final decision as to whether I
pass the exam rests solely with ISACA; (5) I understand that ISACA may inform the local ISACA chapter and other parties who might inquire about my certification status; (6) I agree that any action arising out of or pertaining to this
application or the exam must be brought in the Circuit Court of Cook County, Illinois, USA, and shall be governed by the laws of the State of Illinois, USA; (7) By taking an ISACA Exam, I understand and agree that the Exam (which
includes all aspects of the exam, including, without limitation, the test questions, answers, examples and other information presented or contained in the exam) belongs to ISACA and constitutes ISACA’s confidential information
(collectively, “Confidential Information”). I agree to maintain the confidentiality of all of ISACA’s Confidential Information at all times and understand that any failure to maintain the confidentiality of ISACA’s Confidential Information
may result in disciplinary action against me by ISACA or other adverse consequences, including, without limitation, nullification of my exam, loss of my credentials, and/or litigation. Specifically, I understand that I may not, for
example, discuss, publish or share any exam question(s), my answers to any questions(s) or the exam’s format with anyone in any forum or media (i.e., via e-mail, Facebook, LinkedIn or any other form of social media).
(8) I understand that my information will be used to fulfill my request or as otherwise as described in the ISACA Privacy Policy. All CISA, CRISC, CGEIT and CISM exam items are owned and copyrighted by ISACA. © 2003-Present,
ISACA. All rights reserved.
I HAVE READ AND UNDERSTAND THESE STATEMENTS AND INTEND TO BE LEGALLY BOUND BY THEM.
25. Signature: ______________________________________________________________________________ Date:__________________________(For your registration to be complete, you must sign on the line above.)
COMPLETE THE FEE REMITTANCE SCHEDULE AND METHOD OF PAYMENT ON PAGE 4.
Order No. ___________
Page 1 For Office Purposes Only Please use black ink.
Print in block letters or type.US Federal ID No. 23-7067291
3
CISM
Reg
istra
tion
Form
Con
tinue
d—pa
ge 2
NAM
E: _
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
___
(Ple
ase
use
blac
k in
k an
d pr
int i
n bl
ock
lette
rs o
r typ
e.)
Mem
bers
hip—
YES!
I w
ish
to b
ecom
e an
ISAC
A m
embe
r NOW
…
and
real
ize
the
bene
fits
imm
edia
tely
.IS
ACA
mem
bers
hip
offe
rs s
avin
gs a
nd m
any
bene
fits!
See
ww
w.is
aca.
org/
bene
fits
for d
etai
ls.
Mem
bers
hip
in th
e as
soci
atio
n re
quire
s yo
u to
bel
ong
to a
cha
pter
whe
n yo
u liv
e or
wor
k w
ithin
50
mile
s/80
km o
f a c
hapt
er te
rrito
ry. S
ee is
aca.
org/
chap
dues
.
Chap
ter n
umbe
r ___
____
____
Paym
ent C
alcu
latio
nAs
soci
atio
n du
es
US $
Ch
apte
r due
s (v
isit
ww
w.is
aca.
org/
chap
dues
) US
$Ne
w m
embe
r pro
cess
ing
fee
US
$
30
Tota
l Mem
bers
hip
Fees
(F)
US
$
I d
o no
t wis
h to
be
incl
uded
on
a m
ailin
g lis
t oth
er th
an fo
r ISA
CA m
ailin
gs.
Met
hod
of P
aym
ent
Plea
se n
ote:
You
r reg
istra
tion
is n
ot c
ompl
ete
unle
ss y
ou h
ave
sign
ed p
age
1 of
the
regi
stra
tion
form
.
CISM
Exa
m F
ee a
nd S
tudy
Aid
s To
tal (
E)$_
____
____
ISAC
A M
embe
rshi
p Fe
e To
tal (
if ap
plic
able
) (F)
$_
____
____
Tota
l Rem
itted
(E+F
) US
$__
____
___
Che
ck (c
hequ
e) p
ayab
le to
ISAC
A in
US
dolla
rs, d
raw
n on
a U
S ba
nk B
ank
Tran
sfer
(see
bel
ow)
D
ate
of tr
ansf
er (m
m/d
d/yy
)___
____
____
____
_ M
aste
rCar
d
VIS
A
Am
eric
an E
xpre
ss
Din
ers
Club
D
isco
ver
All p
aym
ents
by
cred
it ca
rd w
ill b
e pr
oces
sed
in U
S do
llars
.
Cred
it ca
rd n
umbe
r __
____
____
____
____
____
____
____
____
____
____
____
____
____
_
Nam
e of
car
dhol
der _
____
____
____
____
____
____
____
____
____
____
____
____
____
__
Expi
ratio
n da
te _
____
____
____
____
____
____
____
____
____
____
____
____
____
____
_M
ONTH
/YEA
R
Sign
atur
e __
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
Ban
k tra
nsfer
infor
matio
n:
Bank
of A
meric
a AB
A No
. 026
0-09
59-3
SW
IFT C
ode:
BOF
AUS3
N IS
ACA
Acco
unt N
o. 22
-715
7-8
(INDI
CATE
CAN
DIDA
TE’S
NAM
E IN
TRAN
SFER
INFO
RMAT
ION)
to:
ISAC
A • 1
055 P
aysp
here
Circ
le • C
hicag
o, IL
6067
4 USA
Air
Cour
ier:
ISAC
A • 3
701 A
lgonq
uin R
oad •
Suit
e 101
0 Ro
lling
Mea
dows
, IL 6
0008
USA
Fax t
o: +1
.847
.253
.144
3
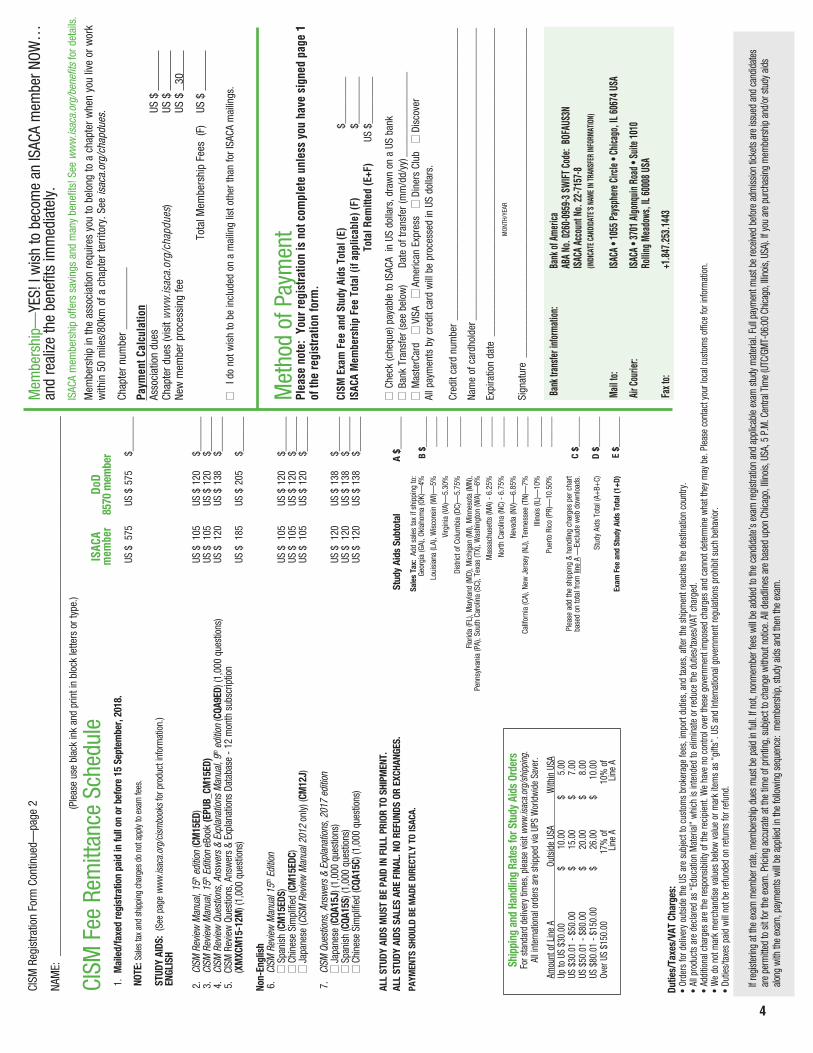
CISM
Fee
Rem
ittan
ce S
ched
ule
ISAC
A Do
Dm
embe
r 85
70 m
embe
r1.
Mai
led/
faxe
d re
gist
ratio
n pa
id in
full
on o
r bef
ore
15 S
epte
mbe
r, 20
18.
US $
575
US
$ 5
75
$___
____
NOTE
: Sale
s ta
x an
d sh
ippi
ng c
harg
es d
o no
t app
ly to
exa
m fe
es.
STUD
Y AI
DS:
(See
pag
e w
ww
.isac
a.or
g/ci
smbo
oks
for p
rodu
ct in
form
atio
n.)
ENGL
ISH
2.
CISM
Rev
iew
Man
ual,
15th e
ditio
n (C
M15
ED)
US $
105
US
$ 1
20
$___
____
3.
CISM
Rev
iew
Man
ual,
15th E
ditio
n eB
ook
(EPU
B_CM
15ED
) US
$ 1
05
US $
120
$_
____
__ 4
. CI
SM R
evie
w Q
uest
ions
, Ans
wer
s &
Expl
anat
ions
Man
ual,
9th e
ditio
n (C
QA9E
D) (1
,000
que
stio
ns)
US $
120
US
$ 1
38
$___
____
5.
CISM
Rev
iew
Que
stio
ns, A
nsw
ers
& Ex
plan
atio
ns D
atab
ase
- 12
mon
th s
ubsc
riptio
n (X
MXC
M15
-12M
) (1,
000
ques
tions
)US
$ 1
85
US $
205
$_
____
__
Non-
Engl
ish
6.
CISM
Rev
iew
Man
ual 1
5th E
ditio
nSp
anish
(CM
15ED
S)US
$ 1
05
US $
120
$_
____
__ C
hine
se S
impl
ified
(CM
15ED
C)
US $
105
US
$ 1
20
$___
____
Jap
anes
e (C
ISM
Rev
iew
Man
ual 2
012
only)
(CM
12J)
US
$ 1
05
US $
120
$_
____
__
7.
CISM
Que
stio
ns, A
nsw
ers
& Ex
plan
atio
ns, 2
017
editi
onJa
pane
se (C
QA15
J) (1
,000
que
stio
ns)
US $
120
US
$ 1
38
$___
____
Spa
nish
(CQA
15S)
(1,0
00 q
uest
ions
) US
$ 1
20
US $
138
$_
____
__ C
hine
se S
impl
ified
(CQA
15C)
(1,0
00 q
uest
ions
) US
$ 1
20
US $
138
$_
____
__
ALL
STUD
Y AI
DS M
UST
BE P
AID
IN F
ULL
PRIO
R TO
SHI
PMEN
T. AL
L ST
UDY
AIDS
SAL
ES A
RE F
INAL
. NO
REFU
NDS
OR E
XCHA
NGES
. St
udy
Aids
Sub
tota
l A
$___
____
PAYM
ENTS
SHO
ULD
BE M
ADE
DIRE
CTLY
TO
ISAC
A.
B $_
____
____
____
___
____
___
____
_
____
___
____
___
____
___
____
___
__
____
_
____
___
____
___
C $_
____
__
D $_
____
__
E
$ ___
____
4
If re
gist
erin
g at
the
exam
mem
ber r
ate,
mem
bers
hip
dues
mus
t be
paid
in fu
ll. If
not,
nonm
embe
r fee
s wi
ll be
adde
d to
the
cand
idat
e’s
exam
regi
stra
tion
and
appl
icabl
e ex
am s
tudy
mat
erial
. Ful
l pay
men
t mus
t be
rece
ived
befo
re a
dmiss
ion ti
cket
s ar
e iss
ued
and
cand
idat
es
are
perm
itted
to s
it fo
r the
exa
m. P
ricin
g ac
cura
te a
t the
tim
e of
prin
ting,
sub
ject t
o ch
ange
with
out n
otice
. All d
eadl
ines
are
bas
ed u
pon
Chica
go, I
llinois
, USA
, 5 P
.M. C
entra
l Tim
e (U
TC/G
MT-
06:0
0 Ch
icago
, Illin
ois, U
SA).
If yo
u ar
e pu
rcha
sing
mem
bers
hip
and/
or s
tudy
aid
s alo
ng w
ith th
e ex
am, p
aym
ents
will
be a
pplie
d in
the
follo
wing
seq
uenc
e: m
embe
rshi
p, s
tudy
aid
s an
d th
en th
e ex
am.
Dutie
s/Ta
xes/
VAT
Char
ges:
• Or
ders
for d
elive
ry o
utsid
e th
e US
are
sub
ject
to c
usto
ms
brok
erag
e fe
es, i
mpo
rt du
ties,
and
taxe
s, a
fter t
he s
hipm
ent r
each
es th
e de
stin
atio
n co
untry
.•
All p
rodu
cts
are
decla
red
as “
Educ
atio
n M
ater
ial”
whi
ch is
inte
nded
to e
limin
ate
or re
duce
the
dutie
s/ta
xes/
VAT
char
ged.
• Ad
ditio
nal c
harg
es a
re th
e re
spon
sibilit
y of
the
recip
ient
. We
have
no
cont
rol o
ver t
hese
gov
ernm
ent i
mpo
sed
char
ges
and
cann
ot d
eter
min
e w
hat t
hey
may
be.
Ple
ase
cont
act y
our l
ocal
cus
tom
s of
fice
for i
nfor
mat
ion.
• W
e do
not
mar
k m
erch
andi
se v
alue
s be
low
val
ue o
r mar
k ite
ms
as “
gifts
”. U
S an
d In
tern
atio
nal g
over
nmen
t reg
ulat
ions
pro
hibi
t suc
h be
havio
r.•
Dutie
s/ta
xes
paid
will
not b
e re
fund
ed o
n re
turn
s fo
r ref
und.
Sale
s Ta
x: A
dd s
ales
tax
if sh
ippi
ng to
: Ge
orgi
a (G
A), O
klah
oma
(OK)
—4%
Loui
sian
a (L
A), W
isco
nsin
(WI)—
5%
Virg
inia
(VA)
—5.
30%
Dist
rict o
f Col
umbi
a (D
C)—
5.75
%
Flor
ida
(FL)
, Mar
ylan
d (M
D), M
ichi
gan
(MI),
Min
neso
ta (M
N),
Penn
sylv
ania
(PA)
, Sou
th C
arol
ina
(SC)
, Tex
as (T
X), W
ashi
ngto
n (W
A)—
6%
Mas
sach
uset
ts (M
A) -
6.2
5%
North
Car
olin
a (N
C) -
6.7
5%
Neva
da (N
V)—
6.85
%
Calif
orni
a (C
A), N
ew J
erse
y (N
J), T
enne
ssee
(TN)
—7%
Illin
ois
(IL)—
10%
Puer
to R
ico
(PR)
—10
.50%
Plea
se a
dd th
e sh
ippi
ng &
han
dlin
g ch
arge
s pe
r cha
rt ba
sed
on to
tal f
rom
line
A —
Excl
ude
web
dow
nloa
ds.
Stud
y Ai
ds T
otal
(A+
B+C)
Exam
Fee
and
Stu
dy A
ids
Tota
l (1+
D)
Ship
ping
and
Han
dlin
g Ra
tes
for S
tudy
Aid
s Or
ders
For s
tand
ard
deliv
ery
times
, ple
ase
visit
ww
w.is
aca.
org/
ship
ping
.Al
l int
erna
tiona
l ord
ers
are
ship
ped
via U
PS W
orld
wid
e Sa
ver.
Amou
nt o
f Lin
e A
Outs
ide
USA
With
in U
SAUp
to U
S $3
0.00
$
10.0
0 $
5.00
US $
30.0
1 - $
50.0
0 $
15.0
0 $
7.00
US $
50.0
1 - $
80.0
0 $
20.0
0 $
8.00
US $
80.0
1 - $
150.
00
$ 26
.00
$ 10
.00
Over
US
$150
.00
17%
of
10%
of
Line
A
Line
A
5
CISM Exam 2018—Important Date Information
Exam Testing Window—1 June – 23 September 2018Final registration deadline: 18 September 2018
Exam registration changes: Changes to your name, exam language, or exam type must be made prior to scheduling your exam appointment. If you have any changes after you have scheduled your appointment, please contact ISACA immediately at +1.847.660.5716 or support.isaca.org > select Certification > selectExam Questions.
Rescheduling: To reschedule your appointment, please log-in at www.isaca.org/myISACA and click on My Certifications. Rescheduling or cancelling a testing appointment must be done a least 48 hours prior to the scheduled appointment.
Deferrals: Candidates may only defer an unscheduled or cancelled eligibility. If you have scheduled a testing appointment, you must first cancel a minimum of 48 hours prior to the scheduled appointment. Deferrals can then be purchased for the $200 fee by no later than 23 September 2018.
Exam registration fees are non-refundable and non-transferable.
All deadlines are based on Chicago, Illinois, USA 5 P.M. Central Time (UTC/GMT-06:00 Chicago, Illinois, USA).
3701 Algonquin Road, Suite 1010Rolling Meadows, IL 60008 USA
Phone: +1.847.253.1545Fax: +1.847.253.1443
Questions: support.isaca.orgWeb site: www.isaca.org
DOC: June-Sept 2018 CISM DoD FormVersion: V1Update: 2018 - 0220





























