Embed Size (px)
Citation preview
Click to edit Footer title style
Randomized Trial of Bead BlockTM vs EmbosphereTM for
UAE for Fibroids
Robert L Worthington-Kirsch, MD,
FSIR, FCIRSE, RVT, RPVI
Click to edit Footer title style
Disclosures
This study is supported by an unrestricted grant from Biocompatibles and Terumo
Dr Worthington-Kirsch is an active consultant to Biocompatibles, Terumo, Biosphere Medical, and Vascular Solutions
Click to edit Footer title style
Background
UAE has been established as mainstream therapy for fibroid diseaseEmbolic choice evolving
Calibrated hydrogel spheres preferredTris-acryl/gelatin most commonly usedPVA hydrogel is an emerging alternative
Click to edit Footer title style
PVA Hydrogel Spheres
Very similar to soft contact lensesPVA has been used as implanted biomaterial since the 1940sVery different properties than non-hydrogel PVA preparations
Click to edit Footer title style
Study Rationale
Clinical experience suggests that BB as effective as ES for UAE
Requires proper technique
Randomized trial needed to confirm or disprove anecdotal experience
Click to edit Footer title style
Study Design
Non-inferiority22 patients per arm gives desired power
PRCT (Level I data)Patients not informed about embolic usedMRI grader blinded for embolic used
Reviewed/approved by FDA
Click to edit Footer title style
Admission Criteria
Similar to other UAE studiesWomen ages 30-50Symptomatic fibroids without other uterine diseaseUterus >250cc, <24 weeks
Click to edit Footer title style
Study DesignMRIs on designated magnet
Pre-UAE, 3-7 days post-UAE, 3 months, 6 months
Best protocol for each embolicBB – start with 700-900
ES – start with 500-700, unless Ovarian A seen
Terumo Progreat microcatheter
Consistent defined embolization endpoints
Click to edit Footer title style
Embolization Endpoints
New filling of Ovarian A or cross-uterine collateralsRetrograde flow around catheter tip“Plumping” of artery with injectionNo further filling of ascending branch
Click to edit Footer title style
Outcome Measures
MRI fibroid perfusion“immediate”, 3 months, 6 months
Uterine/dominant fibroid sizeUFS-QOL
3 months, 6 months, 1 year
Click to edit Footer title style
Study to Date2 cohorts
Site 1 – 22 patientsComplete follow-up data set 1 technical failure (anatomic basis)
Site 2 – 22 + 2 patients1 withdrawal from initial 22Follow-up complete except for 12 month QOLs
22 analyzable patients in each arm
Click to edit Footer title style
Study to Date
No serious complications
All UAEs clinically successful per patients
Including technical failure3 “failures” to discuss in more detail
Click to edit Footer title style
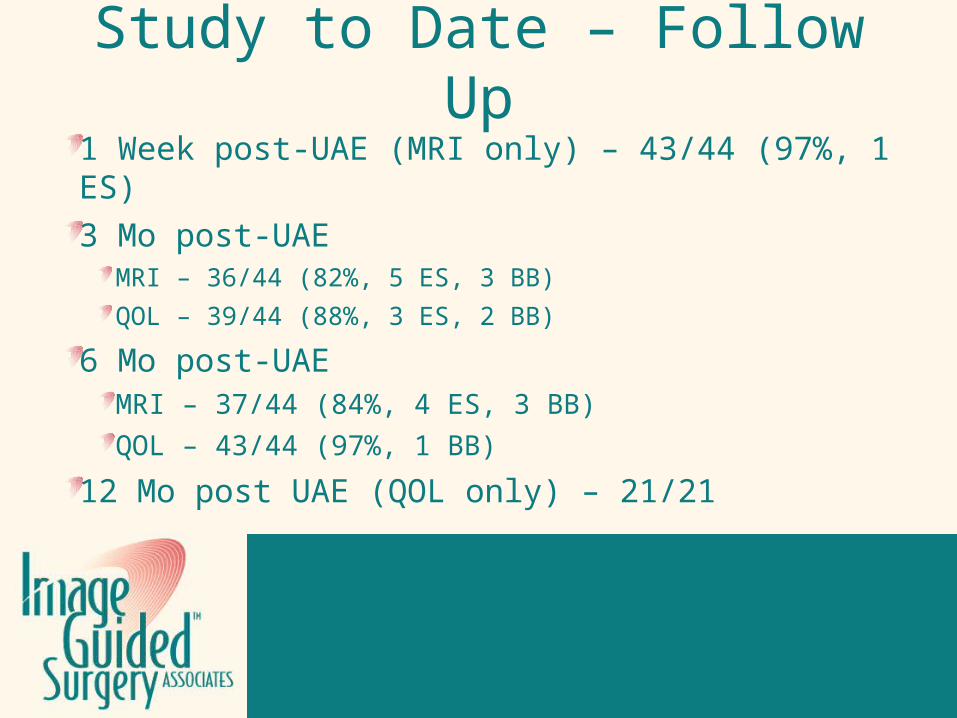
Study to Date – Follow Up1 Week post-UAE (MRI only) – 43/44 (97%, 1 ES)
3 Mo post-UAEMRI – 36/44 (82%, 5 ES, 3 BB)
QOL – 39/44 (88%, 3 ES, 2 BB)
6 Mo post-UAEMRI – 37/44 (84%, 4 ES, 3 BB)
QOL – 43/44 (97%, 1 BB)
12 Mo post UAE (QOL only) – 21/21
Click to edit Footer title style
MRI GradingPre-UAE perfusion scored at 10
Global fibroid burden, not just dominant fibroid
Follow-up perfusion scored 1-101 – Complete infarction all visible fibroids
1-2 - “Success” (10% or less residual perfusion)
3-4 – “Partial Success” (11-30% residual perfusion)
5 or higher - “Failure” (>30% residual perfusion)
Click to edit Footer title style
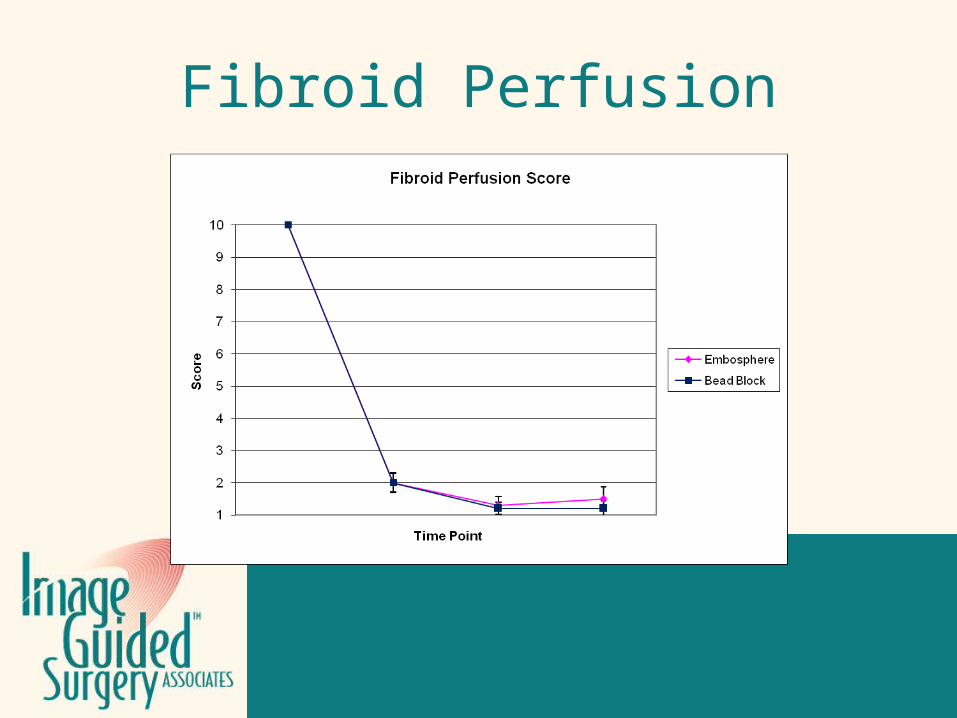
Fibroid Perfusion
Click to edit Footer title style
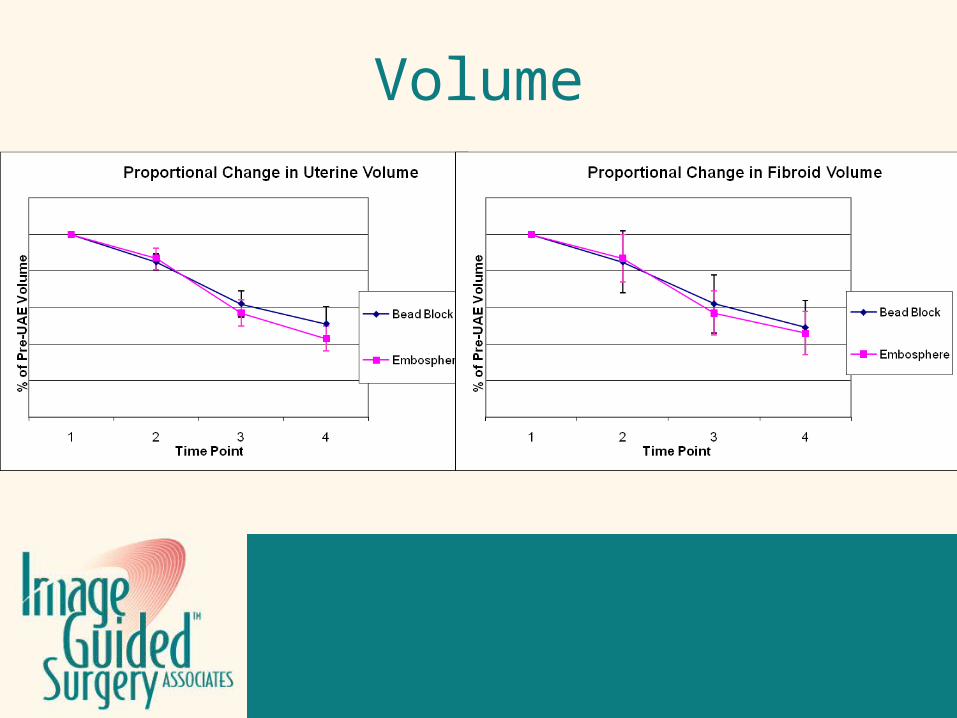
Volume
Click to edit Footer title style
UFS-QOL Grading
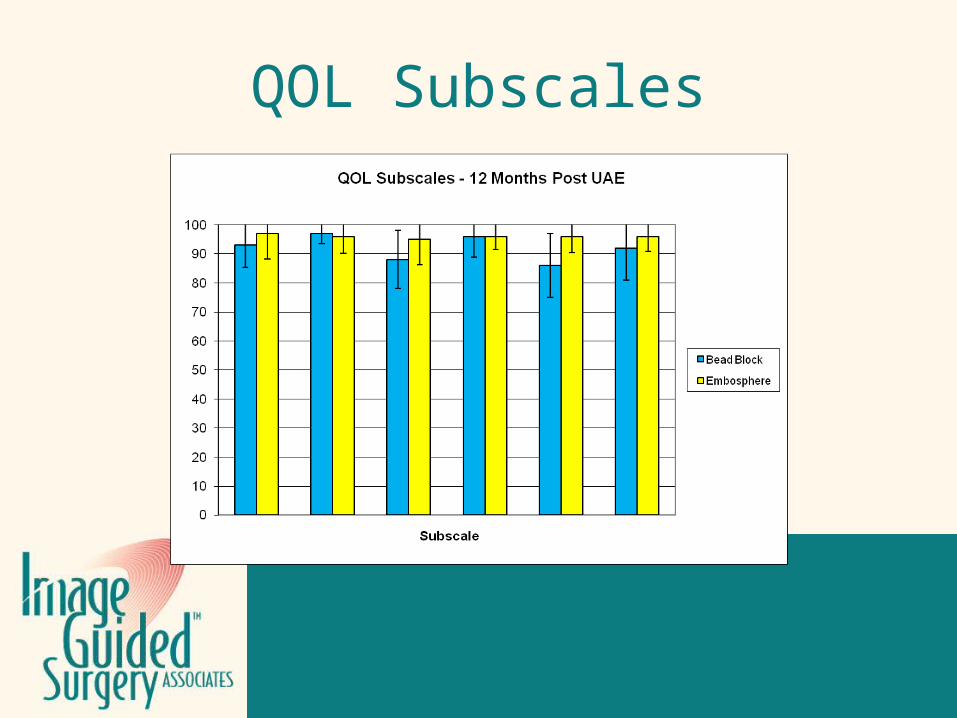
Symptom Score, QOL Score. QOL Subscales
Change of 10 points or greater significant
Click to edit Footer title style
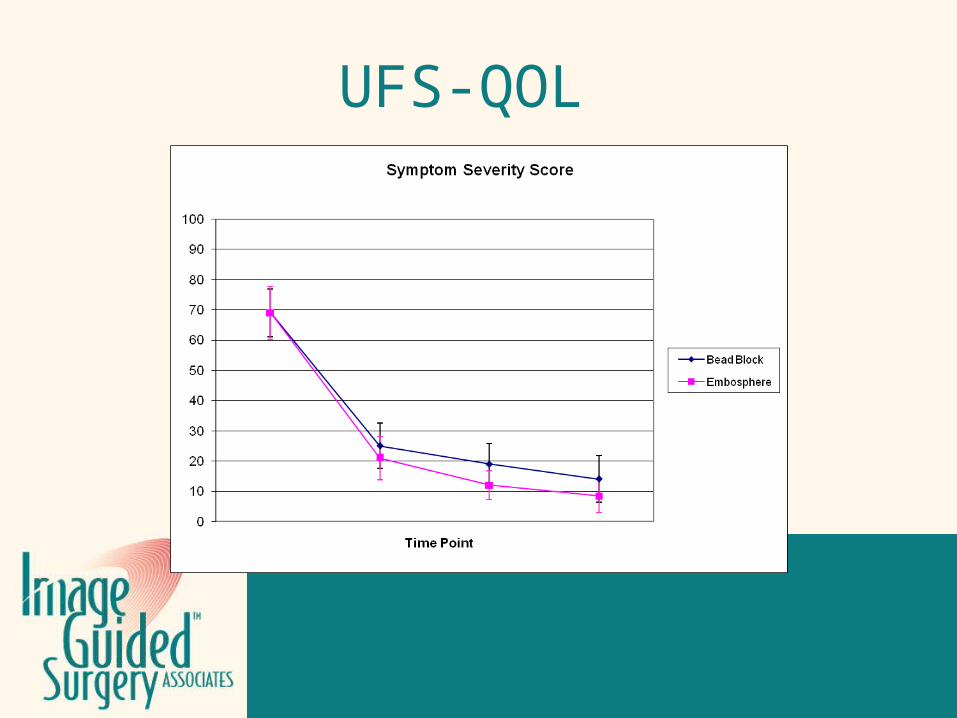
UFS-QOL
Click to edit Footer title style
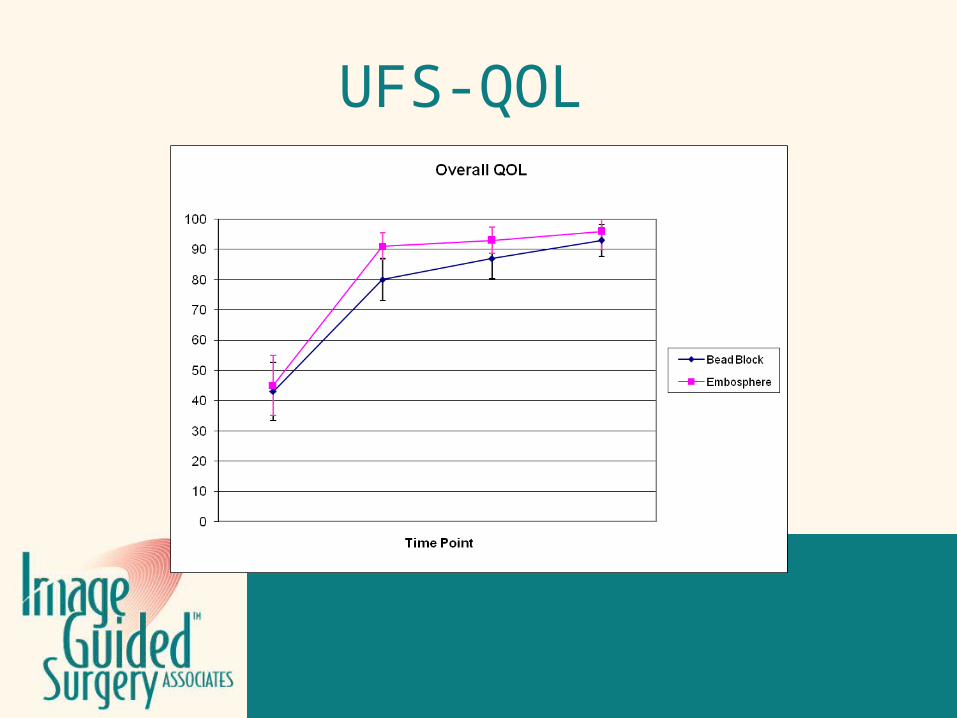
UFS-QOL
Click to edit Footer title style
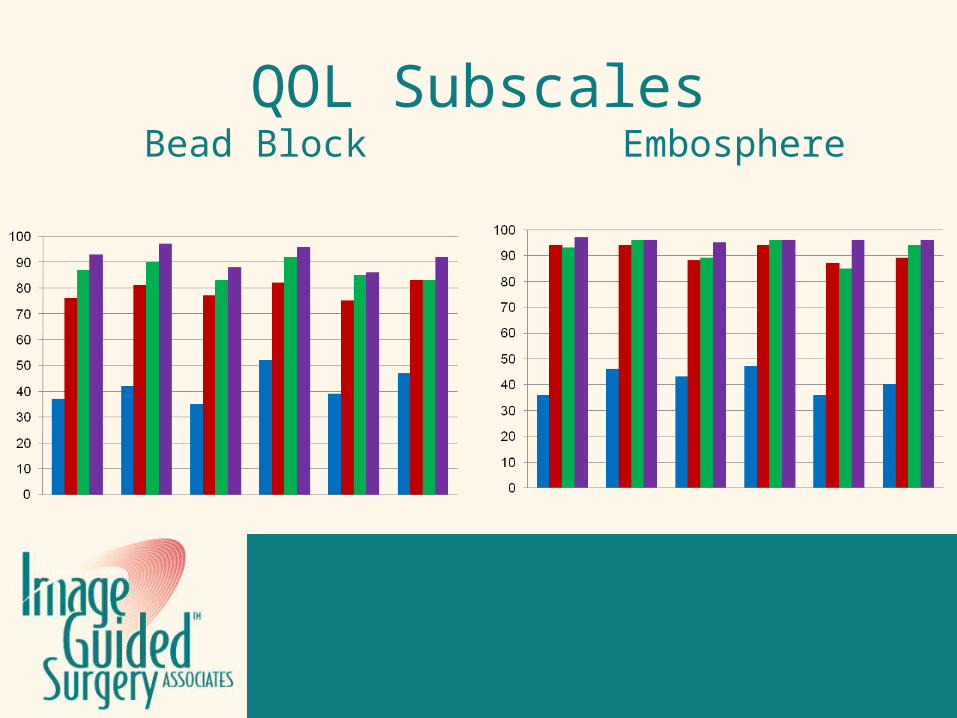
QOL SubscalesBead Block Embosphere
Click to edit Footer title style
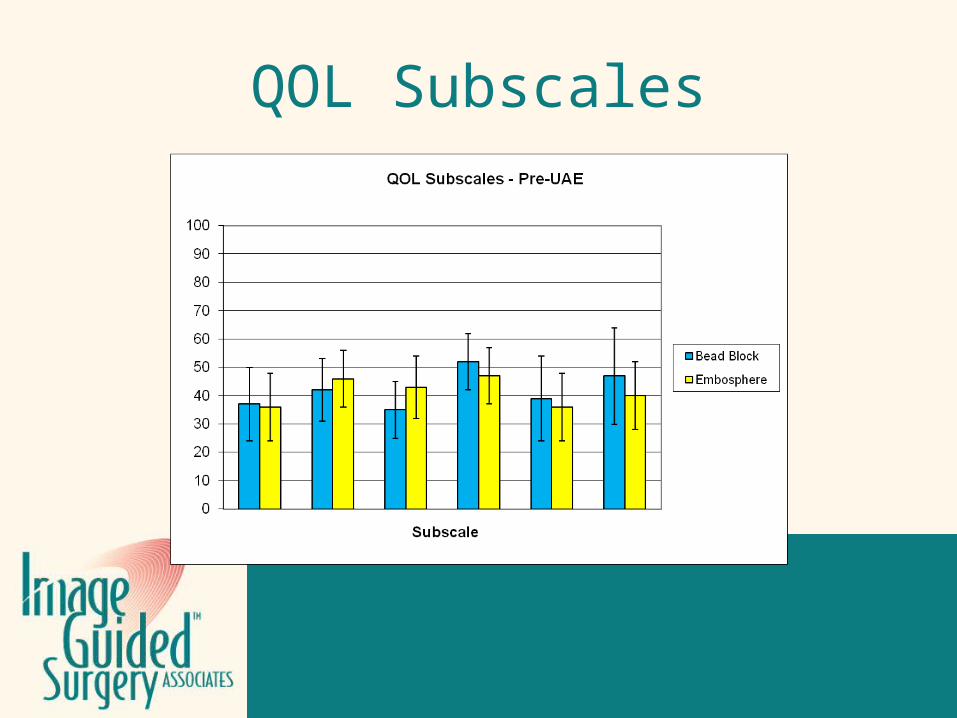
QOL Subscales
Click to edit Footer title style
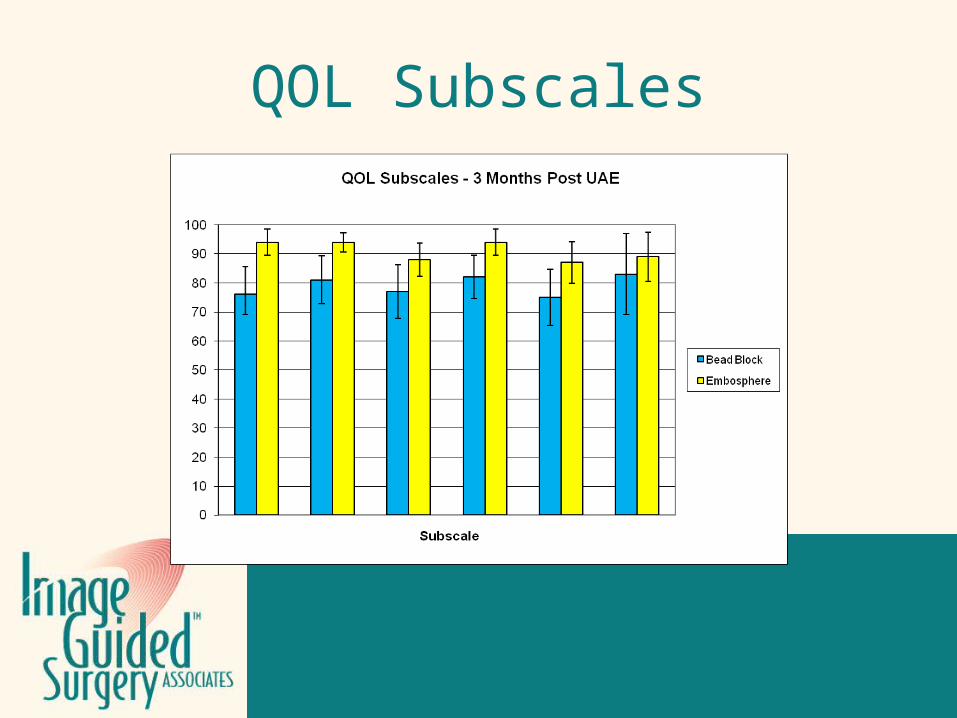
QOL Subscales
Click to edit Footer title style
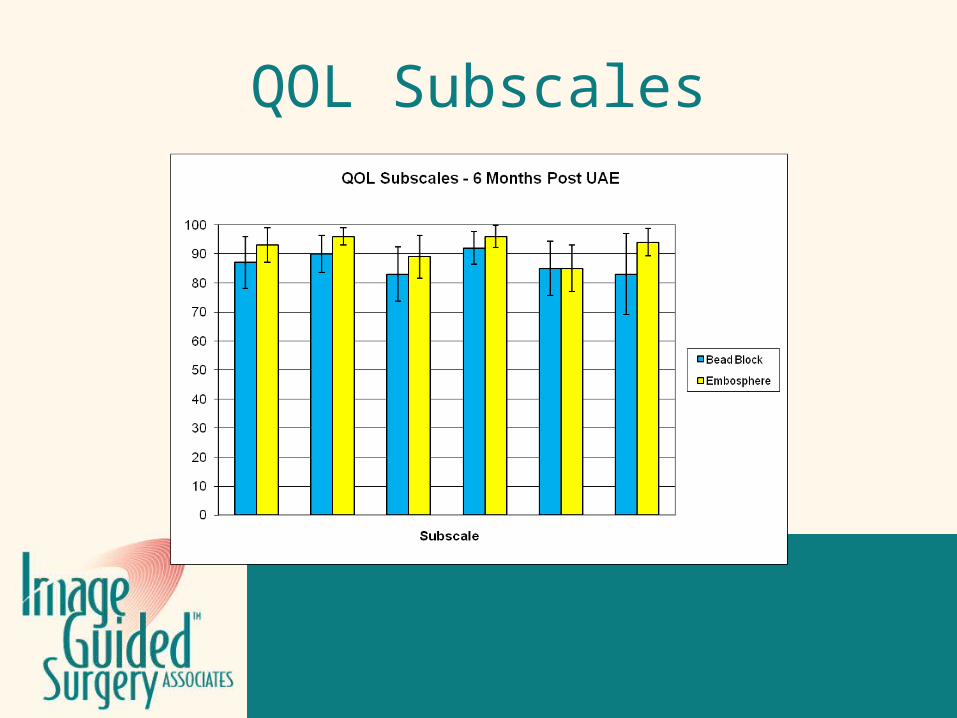
QOL Subscales
Click to edit Footer title style
QOL Subscales
Click to edit Footer title style
Treatment Failures?
Patient # 2-003Embosphere
Complete infarction at 1 week and 3 months
Significant reperfusion (4) at 6 months
SS 94>44>0
QOL 86>89>96
Will symptoms recur?
Click to edit Footer title style
Treatment Failures?
Patient # 2-016Bead Block
Almost complete infarction (2) on all f/u MRIs
SS 41>69>66 (worsening)
QOL 66>50>52 (borderline improvement)
Click to edit Footer title style
Treatment Failures?
Patient # 2-013Embosphere
Perfusion score 3 @ 1 week, then 2
SS 47>25>31
QOL 53>56>51
Click to edit Footer title style
Treatment Failures?
General consensus in literature is that UAE failure rate is ~10%.
3 Failures out of 44 patients is not unexpected.
Click to edit Footer title style
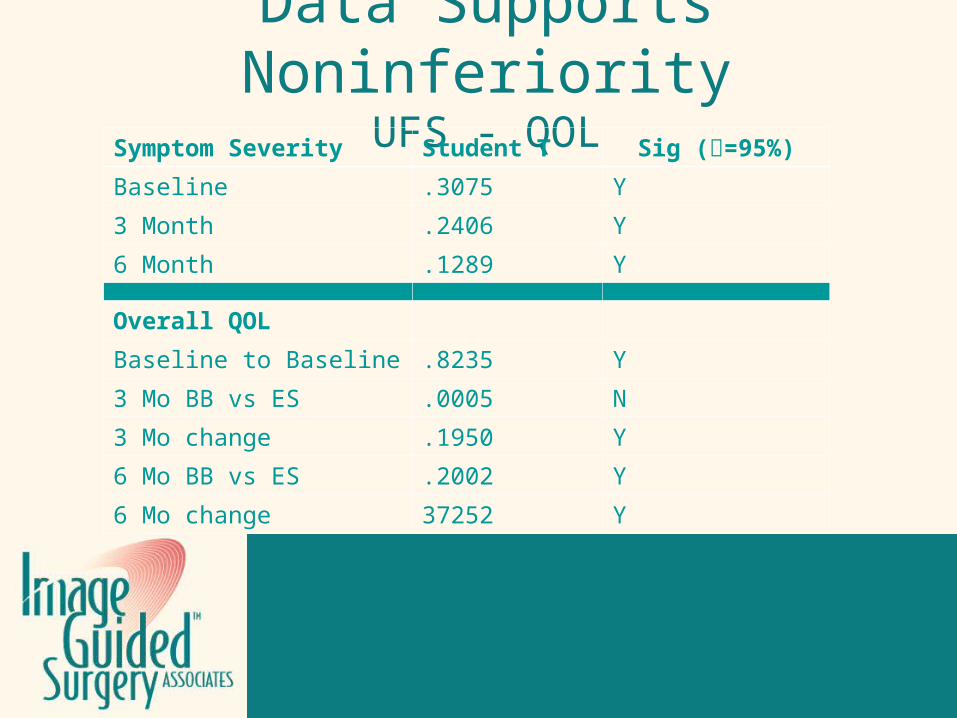
Data Supports Noninferiority
UFS - QOLSymptom Severity Student T Sig (=95%)
Baseline .3075 Y
3 Month .2406 Y
6 Month .1289 Y
Overall QOL
Baseline to Baseline .8235 Y
3 Mo BB vs ES .0005 N
3 Mo change .1950 Y
6 Mo BB vs ES .2002 Y
6 Mo change 37252 Y
Click to edit Footer title style
Data Supports Noninferiority
Perfusion
Click to edit Footer title style
Data Supports NoninferiorityVolume Reduction
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteriaAdequate sample size/power analysisRandomization by independent third partyDouble-blindingIdentical care and follow-up
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteriaAdequate sample size/power analysisRandomization by independent third partyDouble-blindingIdentical care and follow-up
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteriaAdequate sample size/power analysisRandomization by independent third partyDouble-blindingIdentical care and follow-up
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteriaAdequate sample size/power analysisRandomization by independent third partyDouble-blindingIdentical care and follow-up
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteriaAdequate sample size/power analysisRandomization by independent third partyDouble-blindingIdentical care and follow-up
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteriaAdequate sample size/power analysisRandomization by independent third partyDouble-blindingIdentical care and follow-up
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Intention to treat analysisBlinded imaging assessmentClear endpoint assessmentUFS-QOL, Enhanced MRIReporting
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Intention to treat analysisBlinded imaging assessmentClear endpoint assessmentUFS-QOL, Enhanced MRIReporting
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Intention to treat analysisBlinded imaging assessmentClear endpoint assessmentUFS-QOL, Enhanced MRIReporting
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Intention to treat analysisBlinded imaging assessmentClear endpoint assessmentUFS-QOL, Enhanced MRIReporting
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Intention to treat analysisBlinded imaging assessmentClear endpoint assessmentUFS-QOL, Enhanced MRIReporting
Click to edit Footer title style
Spies – “How to Evaluate New Embolics”
Intention to treat analysisBlinded imaging assessmentClear endpoint assessmentUFS-QOL, Enhanced MRIReporting

Click to edit Footer title style
Questions?