Embed Size (px)
Citation preview

Clinical and Radiologic Findings in Progressive Facial Hemiatrophy(Parry-Romberg Syndrome)
Richard C. Cory, David A. Clayman, Walter J. Faillace, Shaun W. McKee, and Carlos H. Gama
Summary: We describe the clinical and radiologic changes re-lated to progressive facial hemiatrophy (Parry-Romberg syn-drome) occurring during a 20-month period in a child who pre-sented with unilateral neurologic deficits and facial hemiatrophy.CT and MR findings included unilateral focal infarctions in thecorpus callosum, diffuse deep and subcortical white matter sig-nal changes, mild cortical thickening, and leptomeningeal en-hancement with dense mineral deposition. Angiographic findingswere normal. We hypothesize that a noninfectious, unilateralinflammatory process, possibly associated with a chronic vaso-motor disturbance and sympathetic nerve chain inflammation,was a major factor in the pathogenesis of this syndrome.
Index terms: Face, atrophy; Children, diseases
Long after its description by Parry in 1825and Romberg in 1846, progressive facial hemi-atrophy syndrome remains a poorly understoodentity (1–3). The major features of this syn-drome, which have been reported previously,are atrophy of the soft tissues on one side of theface with hyperpigmentation of the overlyingskin and various neurologic findings, includingmigraine-type headache, trigeminal neuralgia,and focal epilepsy. Imaging features consist ofincreased signal in the white matter on protondensity– and T2-weighted magnetic resonance(MR) images, meningeal enhancement, intra-cranial calcifications, and central cerebral atro-phy.
We present serial neuroimaging findings illus-trating the progression of brain changes in acase of Parry-Romberg syndrome and specu-late on the underlying pathogenesis of this dis-order.
Case ReportWe examined a 51⁄2-year-old right-handed girl with nor-
mal developmental milestones. The mother’s pregnancy
75
was complicated by gestational diabetes and preeclamp-sia; the patient’s medical history was unremarkable fortrauma or a major illness. Intermittent frontal headachesdeveloped insidiously, without precipitating factors. Theheadaches averaged 2 hours in duration, were often ac-companied by nausea and emesis, and were assuaged byacetaminophen and sleep. There were no prodromal aurasand there was no family history of migraine headache. Theheadaches were accompanied by a mild expressive apha-sia, dysesthesia in the right hand and leg, followed bytransient hand paresis and clumsiness. Normal sensationand motor strength returned after cessation of the head-aches.
Findings at neurologic examination between episodesof neurologic dysfunction were normal. Abnormal findingsat computed tomography (CT) suggested a differentialdiagnosis of childhood hemiplegic migraine, cerebritis, orvasculitis, and prompted cerebral angiography and MRimaging.
After the first few headaches, skin atrophy and hyper-pigmentation (coup de sabre) of the left side of the fore-head below the hairline developed and progressed to in-volve the left eyelid and maxillary region lateral to the lipline (Fig 1). There was also loss of lashes around the lefteye. The progressive facial changes established the diag-nosis of progressive facial hemiatrophy.
CT and MR examinations were obtained during times ofprogressive atrophic changes in the patient’s facial ap-pearance. CT was performed without contrast enhance-ment. All MR examinations were performed on a 1.0-Tsystem and included axial and sagittal T1-weighted se-quences (733/20/2 [repetition time/echo time/excita-tions]) without and with contrast medium (0.1 mmol/kggadopentetate dimeglumine) and noncontrast spin-den-sity and T2-weighted sequences (3000/20,80/1).
The initial brain CT scan, obtained at age 5 years 7months, showed small calcifications anteriorly in the leftcingulate gyrus adjacent to the genu of the corpus callo-sum (Fig 2A). Linear sulcal and gyral calcifications werepresent in the superior lateral left frontoparietal region.Subtle low densities in the subcortical white matter of the
Received May 30, 1995; accepted after revision July 18.From the Departments of Radiology (R.C.C., D.A.C., S.W.McK.), Neurosurgery (W.J.F.), and Neurology (C.H.G.), University of Florida Health Science
Center/Jacksonville.Address reprint requests to David A. Clayman, MD, Department of Radiology, University of Florida Health Science Center/Jacksonville, University
Medical Center, 655 W 8th St, Jacksonville, FL 32209.
AJNR 18:751–757, Apr 1997 0195-6108/97/1804–0751 © American Society of Neuroradiology
1
752 CORY AJNR: 18, April 1997
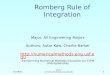
Fig 1. Left-sided facial changes in a 6-year-old girlwith progressive facial hemiatrophy: skin atrophy andhyperpigmentation of the forehead (coup de sabre);periorbital, premaxillary, and perioral soft-tissue atro-phy and hyperpigmentation; hair loss in the medialeyebrow; and loss of lashes along the medial eyelids.
Fig 2. Axial noncontrast CT scans (at age 5 years 7 months) show calci-fications and adjacent white matter decreased densities in the left frontalcingulate gyrus and corpus callosum (A) and in the superior lateral left fron-toparietal parenchyma (arrow in B).
Fig 3. Axial noncontrast T1-weighted (A) and T2-weighted (B) MR images below the genu of the corpus callosum and T2-weightedimage (C) through the level of the genu (at age 5 years 7 months) show focal low-signal abnormality in the left genu in A, becoming highsignal in B, and showing more diffuse subcortical and subependymal white matter high signal changes in C.
AJNR: 18, April 1997 FACIAL HEMIATROPHY 753
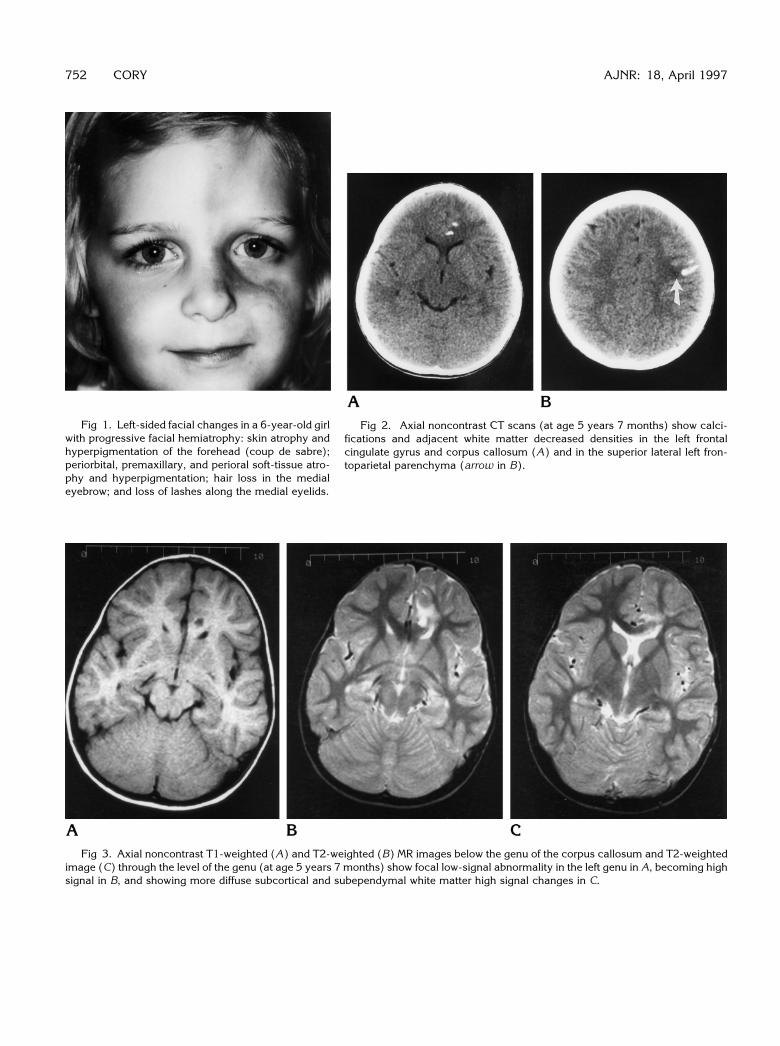
Fig 4. Serial parasagittal images of thepatient over a period of 10 months showprogression of the abnormal findings.
A, At age 5 years 7 months, a focal lowsignal abnormality is identified in the cor-pus callosal genu with a subtle area ofenhancement superiorly (arrow).
B, At age 6 years, a new area of lowsignal has formed in the body of the corpuscallosum, and enlargement of the genu ab-normality is noted.
C, At age 6 years 1 month, a new high-signal enhancing focus is seen in the ante-rior aspect of the corpus callosal body.
D, Finally, at age 6 years 5 months, thelesion in the anterior body of the corpuscallosum no longer enhances and now ishypointense.
left frontal and parietal regions were identified near thecalcifications (Fig 2B). Cerebral atrophy was not present.
The first MR study, obtained the same day as the initialCT examination, showed a focal area of T1 and T2 pro-longation at the site of the cingulate calcification identifiedon the CT scan (Fig 3A and B). Subtle enhancementsuperior to this focus was seen on the contrast-enhancedsagittal T1-weighted MR image (Fig 4A). T2-weighted MRimages clearly showed abnormal hyperintensity in thesubependymal aspect of the left corpus callosal genu (Fig3C). Abnormal signal also extended anteriorly and later-ally into the subcortical white matter of the cingulate gyrusand into the deep left frontal white matter (Fig 3B and C).Abnormal high signal in the left frontoparietal subcorticalwhite matter extended into the centrum semiovale (Fig5C). T1-weighted contrast-enhanced MR images showedsulcal/pial enhancement between the left frontoparietalgyri at the site of calcification shown on the CT scan andadjacent to the signal changes in the subcortical whitematter (Fig 5B). More craniad axial T1- and T2-weightedMR images revealed a subtle thickening of the cortical gyriwith mild effacement of the sulcal spaces (Fig 6A and B).
Findings on a four-vessel cerebral arteriogram werenormal. Cerebrospinal fluid (CSF) and blood chemistries
were normal; CSF and blood cultures were without growthafter 5 days. A sleep-deprived electroencephalogram(EEG) was initially normal. Repeat EEG testing revealedintermittent slowing of posterior rhythms in the absence ofdrowsiness, without obvious epileptiform activity.
Histologic examination of a skin biopsy specimen of thehyperpigmented left side of the forehead revealed chronicinflammation with atrophy of hair follicles. Culture andspecial staining of this specimen showed no abnormality.Brain biopsy was considered but ultimately deferred owingto confidence in the clinical diagnosis.
Serial follow-up MR examinations obtained during pe-riods of worsening atrophy of the left facial structures atages 6 years, 6 years 1 month, 6 years 5 months, and 7years 3 months revealed progressive abnormal changes ofthe brain. T1-weighted images showed the development ofseveral low signal foci in the left corpus callosum over a9-month period (Fig 4B). One of these lesions, whichshowed bright contrast enhancement on T1-weighted im-ages, evolved into a well-defined hypointensity over a6-month interval (Fig 4C and D). Meningeal enhancementof the left parietal lobe persisted and did not increase overa 20-month period (Fig 7B). A modest progression of theabnormal white matter areas of hyperintensity seen on
754 CORY AJNR: 18, April 1997
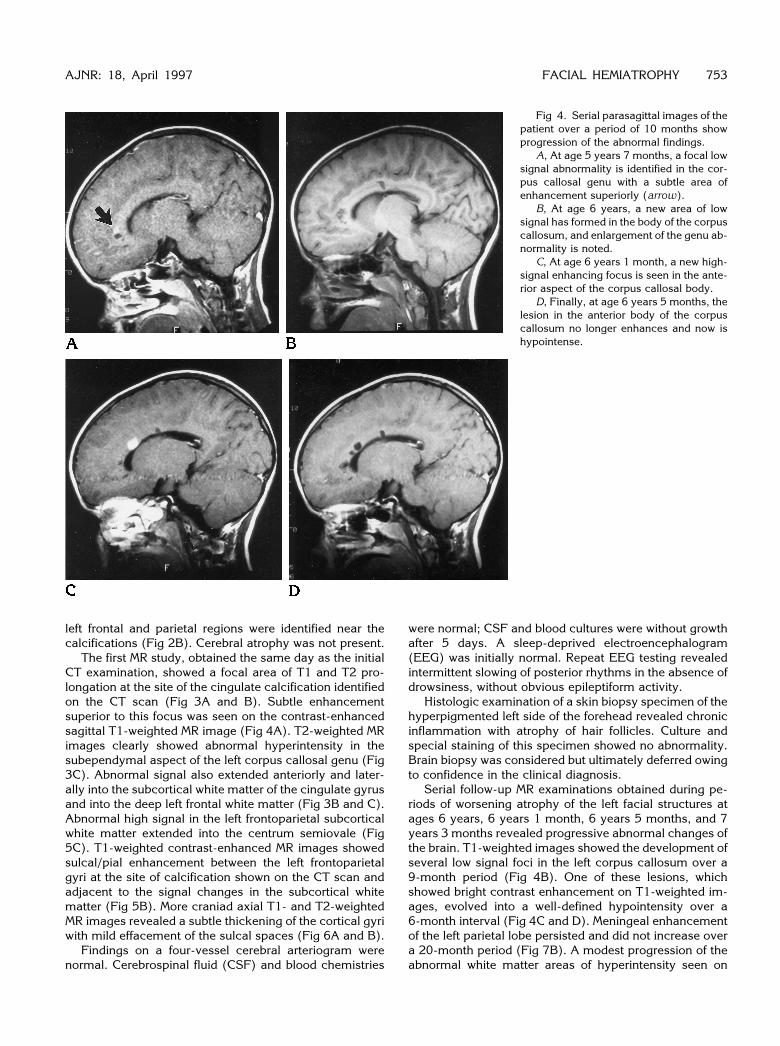
Fig 5. Axial noncontrast (A) and contrast-enhanced (B) T1-weighted MR images at the level of the centrum semiovale (at age 5years 7 months) show sulcal/pial enhancement. Axial noncontrast T2-weighted image at the same level (C) shows abnormal subcorticalhigh signal.
Fig 6. Axial noncontrast T1-weighted (A) and T2-weighted (B) MR images through the high frontal and parietal lobes (at age 5 years7 months) show subtle cortical thickening with less definition of the gray–white border and sulcal effacement. Axial noncontrastT1-weighted MR image (C) obtained 10 months later shows mild progression of cortical changes.
spin-density and T2-weighted images occurred, which co-incided with progression of facial atrophy (Fig 7C and D).A gradual increase of the cortical gyral thickening in theleft parietal lobe was recognizable over time (Figs 6C and7A, C, and D). A follow-up CT scan showed corpus cal-losal encephalomalacia and a progression of white matterlow density in the left hemisphere (Fig 8A and B).
Discussion
Our patient had MR findings of acute, focalwhite matter enhancement with progression to
encephalomalacia, and a slowly progressivethickening of the cerebral cortex with overlyingmeningeal enhancement. The predominantfindings were intraaxial with some areas of ex-traaxial leptomeningeal enhancement. Arterio-graphic findings were normal, similar to the ex-perience of other authors (1, 3). CT and MRfindings were actively progressive at the time ofangiography.
Increased signal intensities in the cerebralwhite matter have been reported in other studies

AJNR: 18, April 1997 FACIAL HEMIATROPHY 755
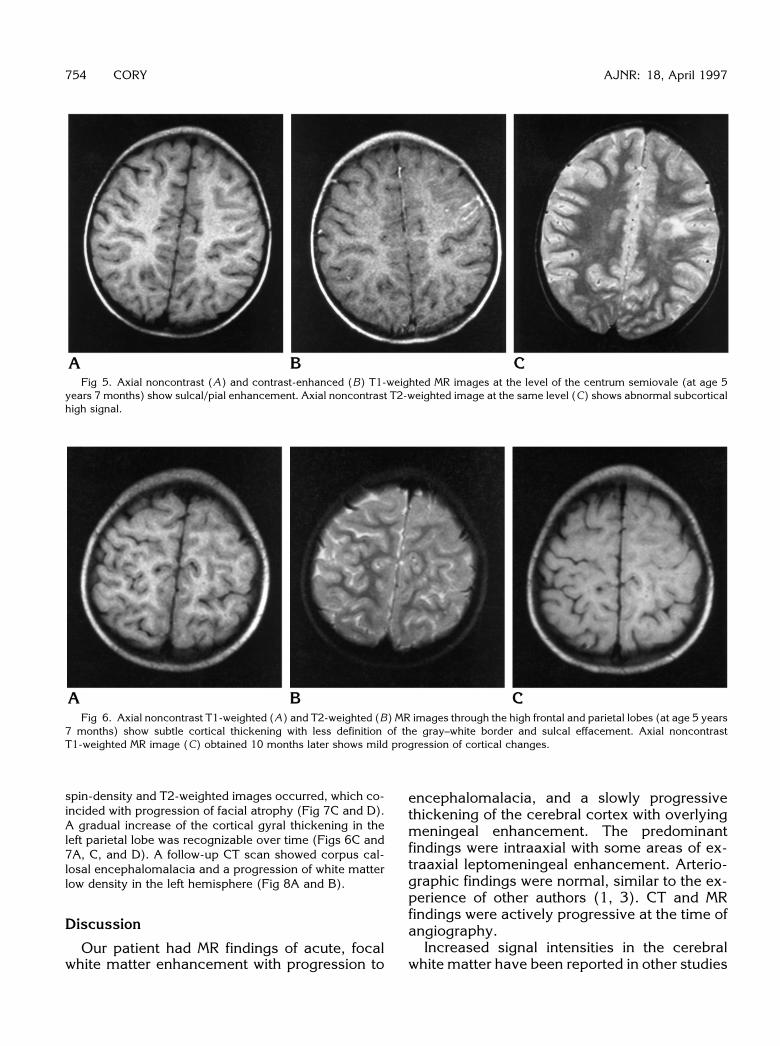
Fig 7. Axial noncontrast (A) andcontrast-enhanced (B) T1-weighted im-ages and spin-density (C) and T2-weighted (D) images through the frontaland parietal lobes above the lateral ven-tricles (at age 7 years 4 months) showmild cortical thickening involving themore frontal parenchyma. Subcorticalwhite matter high signal changes arepresent (C and D). Pial enhancement isstill present (B).
Fig 8. Noncontrast axial CT scansthrough the level of the frontal horns andcorpus callosum (A) and through the highfrontoparietal brain (B) (at age 6 years 5months) show calcifications are relativelyunchanged while white matter low densi-ties in the left hemisphere have pro-gressed.
756 CORY AJNR: 18, April 1997
of progressive facial hemiatrophy syndrome(1). Terstegge et al (2) reported meningocorti-cal dysmorphism, meningeal enhancement,and central atrophy at MR imaging and pro-posed that meningoencephalitis with vasculitiswas the mechanism underlying the morpho-logic brain changes in this disorder. The pre-dominate intraaxial, as opposed to extraaxial,manifestations in our case do not completelysupport this hypothesis. The cortical thickeningand enhancement in our patient do support me-ningocortical dysmorphism as described byTerstegge et al, but in our patient the dysmor-phism occurred without development of atro-phy. Intracranial calcifications (1, 3–5) as wellas cerebral hypodensities have also been re-ported (2, 4).
Unilateral cerebral changes ipsilateral to thefacial atrophy as seen in our case have beendescribed by others (1–4). However, our casediffers from other studies, which have reportedcontralateral cerebral involvement. Most refer-ences to contralateral intracranial disease werenonspecific and were inferred from findings onskull radiographs (6) or from the presence ofventriculomegaly seen on pneumoencephalo-grams (3, 6). In one case a CT finding of focalincreased density in the contralateral hemi-sphere was described (3). The finding was non-specific but raised the possibility of bilateraldisease in a case of progressive facial hemiat-rophy syndrome.
The pathogenesis of progressive facial hemi-atrophy has eluded investigators. Trauma hasbeen implied, but trauma is an inconsistent fea-ture (3). In 1945, Wartenberg (7) ascribedcases of scleroderma with streaklike facial atro-phy (coup de sabre) to “abortive progressivefacial hemiatrophy.” Other reports have sug-gested that the opposite is true: that progressivefacial hemiatrophy is a form of focal sclero-derma (5, 8). The diagnostic differentiating fea-ture between the two is the preservation of elas-tic tissue at histologic examination in pro-gressive facial hemiatrophy. Encephalitis, com-plicated migraine, and slow virus infection havealso been advanced as possible causes (4, 8).
Several authors have proposed that progres-sive facial hemiatrophy results from a distur-bance leading to sympathetic nervous systemhyperactivity (7, 9, 10). Wartenberg (7) statedthat trophism of the fat and subcutaneous tis-sues is under the influence of the sympatheticnervous system. Moss and Crikelair (9) pro-
duced a condition resembling progressive facialhemiatrophy by performing a unilateral sympa-thectomy in rats. More recently, Resende et al(10) ablated the superior cervical sympatheticganglion in young rabbits, cats, and dogs, andreproduced the principal clinical alterations ofParry-Romberg syndrome. In humans, no caseof progressive facial hemiatrophy has occurredafter cervical sympathectomy. The diseasemost commonly occurs during the first or sec-ond decade of life, when facial and head growthmight be most affected. We suggest that theclinical features of Parry-Romberg syndromemay not be apparent if sympathectomy occursafter facial maturation and cessation of headgrowth.
In contrast, many authors have reasoned thata pathologic state of sympathetic irritation leadsto the facial hemiatrophy and, as a result, peri-arterial sympathectomy has been performedwith some success in order to halt the progres-sion of facial atrophy (8). Tebloev and Kalash-nikov (11) reported 19 patients in whom facialhemiatrophy developed after the onset of gan-glionitis of the superior cervical sympatheticganglion, brain stem encephalitis, trigeminalneuralgia, tumors of the gasserian ganglion,and syringobulbia. These authors proposed apathologic relationship between the develop-ment of symptomatic facial hemiatrophy andlesions of the mesencephalotruncal and supe-rior cervical sympathetic ganglion structures. Ifthe sympathetic nervous system is responsible,it remains unclear whether facial atrophy resultsfrom postinflammatory hypofunctioning of thesympathetic nerves or from sympathetic hyper-activity in the presence of active inflammation.
Anatomically, the internal carotid nervesarise from the superior cervical ganglia and giverise to the medial and lateral internal carotidplexus. The lateral plexus communicates withlower cranial and deep facial nerves and gan-glia, while the medial plexus communicateswith upper cranial nerves. Terminal filamentsfrom the internal carotid plexus course aroundthe cerebral arteries (12).
We postulate that the CT and MR imagingfindings in progressive facial hemiatrophy rep-resent a diffuse, slowly progressive and self-limited inflammatory process. We suggest thatthe more focal changes represent an ac-celerated and local manifestation of the samepathologic process. Our case reveals the initialdynamic evolution of progressive facial hemiat-

AJNR: 18, April 1997 FACIAL HEMIATROPHY 757
rophy and demonstrates the first phases of achronic, progressive disease course that ispunctuated by acute exacerbations. We dis-agree with Fry et al (1), who discounted thetheory of a trigeminal or sympathetic innerva-tion abnormality. Instead, we favor the hypoth-esis of hyperactivity of the sympathetic nervoussystem, specifically, inflammation of the supe-rior cervical ganglion in a young patient, as thecause of progressive facial hemiatrophy. Thedivision of the sympathetic nervous system intoright and left and the distribution of medial andlateral internal carotid nerve branches providean anatomic basis for the unilateral facial andintracranial manifestations of the disease. Thehyperactive vasomotor tone of the intracranialvasculature might explain migraine symptom-atology and normal cerebral angiography. Last,recent animal studies and clinical series lendsupport to the hyperactive sympathetic nervoussystem hypothesis as the etiologic mechanismresponsible for progressive hemifacial atrophysyndrome (8–11).
AcknowledgmentsWe thank Dorothy Shumate for her kind assistance in
searching the literature and preparing the manuscript andL. Habelson Wilf and Robert P. Booth for their assistance inediting the manuscript.
References1. Fry JA, Alvarellos A, Fink CW, Blaw ME, Roach ES. Intracranial
findings in progressive facial hemiatrophy. J Rheum 1992;19:956–958
2. Terstegge K, Kunath B, Felber S, Speciali JG, Henkes H, HostenN. MR of brain involvement in progressive hemifacial atrophy(Romberg disease): reconsideration of a syndrome. AJNR Am JNeuroradiol 1994;15:145–150
3. Aher SW, Berg BO. Progressive hemifacial atrophy: report of3cases, including one observed over 43 years, and CT findings.Arch Neurol 1992;39:44–46
4. Sagild J, Alving J. Hemiplegic migraine and progressive hemifa-cial atrophy. Ann Neurol 1985;17:620
5. Merritt KK, Faber HK, Bruch H. Progressive facial hemiatrophy:report of two cases with cerebral calcifications. J Pediatr 1937;10:374–395
6. Eadie MJ, Sutherland JM, Tyrer JH. The clinical features of hemi-facial atrophy. Med J Austr 1963;50:177–180
7. Wartenberg R. Progressive facial hemiatrophy. Arch Neurol Psy-chiatry 1945;54:75–97
8. Rogers BO. Progressive facial hemiatrophy: Romberg’s disease: areview of 772 cases. International Congress Series 66. Washing-ton, DC: Excerpta Medica Foundation; 1963:681–689
9. Moss ML, Crikelair GF. Progressive facial hemiatrophy followingcervical sympathectomy in the rat. Arch Oral Biol 1959;1:254–258
10. Resende LA, Pai DV, Alves A. Experimental study of progressivefacial hemiatrophy: effects of cervical sympathectomy in animals[in French]. Rev Neurol (Paris) 1991;147:609–611
11. Tebloev IK, Kalashnikov IuD. Pathogenesis of symptomatic facialhemiatrophy [in Russian]. Zh Nevropatol Psikhiatr Im S S Korsa-kova 1979;79:413–416
12. Gray H; Goss CM, ed. Gray’s Anatomy of the Human Body. 29thed. Philadelphia, Pa: Lea & Febiger; 1973:1013–1014