Embed Size (px)
Citation preview
HEPATOLOGY Vol. 22, No. 4, Pt. 2, 1995 AASLD ABSTRACTS 355A
993 POOR CORRELATION OF HEPATITIS ACTIVITY AND ANTI-HCV IGM IN 259 CONSECUTIVE PATIENTS, M Delle Monache. *M Micali. *E Mannetla. *A Gallo. *G M~reurth. M Santolamazza. C Berardo. R Gerardi. M Bacosi. G Bruno. RMA Masinelli and GL
GI Unit, Clinica Medica 2, Policlinian Umberto I and *Cantro Nazionale Trasfusione Sangue-CRI, Rome, Italy.
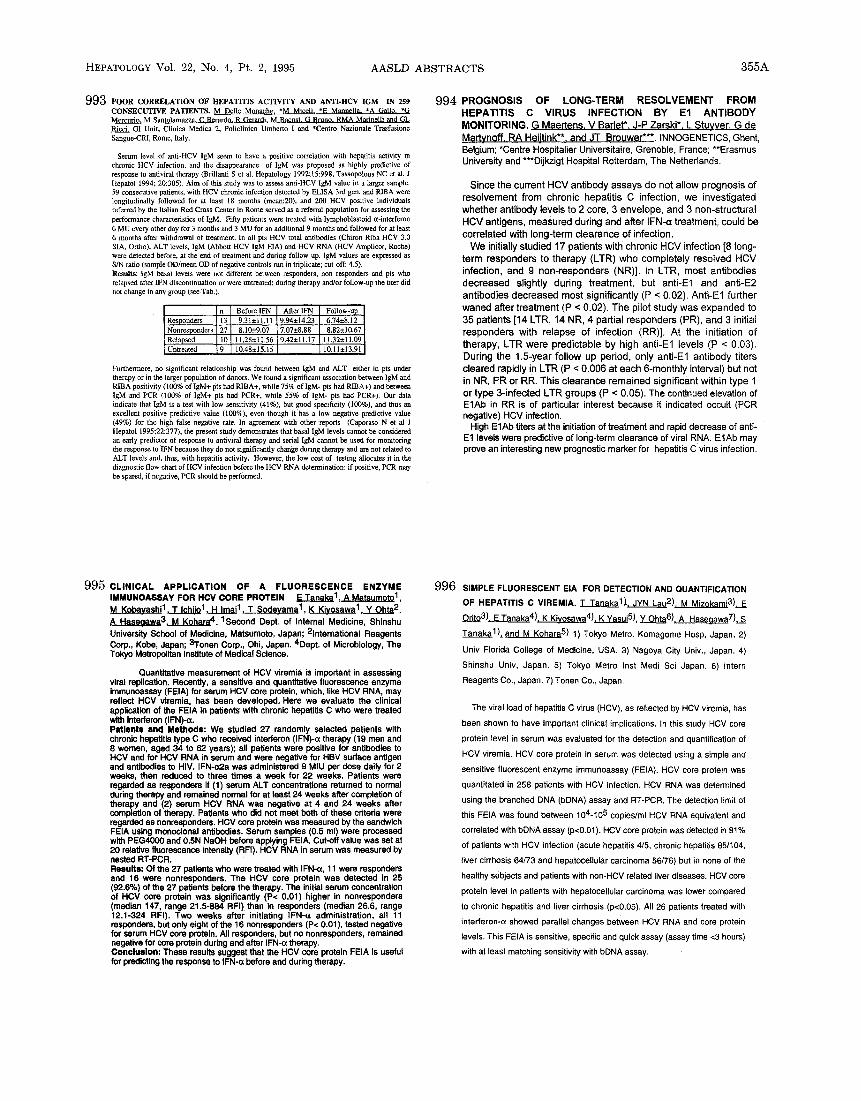
Serum level of anti-HCV lgM seem to have a positive correlation with hepatitis activity in chronic HCV infection, and the disappearance of lgM was proposed as highly predictive of response to antiviral therapy (Brillanti S et at. Hepatology 1992;15:998, Tassopolous NC et al. J Hepatol 1994; 20:305). Aim of this study was to assess anti-HCV IgM value in a larger sample: 59 consecutive patients, with HCV chronic infection detected by EL1SA 3rd gen. and RIBA were longitudinally followed for at least 18 months (mean:20), and 200 HCV positive individuals referred by the Italian Red Cross Center in Rome served as a referral population for assessing the performance characteristics of IgM. Fifty patients were treated with lymphoblastoid a-interferan 6 MU every other day for 3 months and 3 MU for an additional 9 months and followed for at least 6 months after withdrawal of treatment. In all pts HCV total antibodies (Chiron Riba HCV 3.0 SIA, Ortho), ALT levels, IgM (Abbott HCV IgM EtA) and HCV RNA (HCV Amplicor, Roche) were detected before, at the end of treatment and during follow up. IgM values are expressed as S/N ratio (sample OD/mean OD of negative controls run in triplicate; cut-off: 4.5), Results: IgM basal levels were not different between responders, non responders and pts who relapsed after IFN discontinuation or were untreated; during therapy and/or follow-up the tiler did not change in any group (see Tab.).
n Before IFN After IFN Follow-up Responders 13 9,31±11.11 9.94±14.23 6.74±8.12
27 7.07±8.88 8.82±10.67 Nonresponders 8.10±9.07 Relapsed i 190 11,28±11.56 9.42±11,17 11.32±11.09 i Untreated 10.48± 15.15 10.11 ± 13.91
Furthermore, no significant relationship was found between IgM and ALT either in pts under therapy or in the larger population of donors. We found a significant association between lgM and RIBA positivity (100% of IgM+ pts had RIBA+, while 75% of IgM- pts had RIBA+) and between IgM and PCR (100% of IgM+ pts had PCR+, whilo 55% of IgM- pts had PCR+), Our data indicate that IgM is a test with low sensitivity (41%), but good specificity (160%), and thus an excellent positive predictive value (100%), even though it has a low negative predictive value (49%) for the high false negative rate. In agreement with other reports (Caporaso N et al J Hepatol 1995;22:377), the present study demonstrates that basal IgM levels cannot be considered an early predictor of response to antiviral therapy and serial IgM cannot be used for monitoring the response to 1FN because they do not significantly change during therapy and are not related to ALT levels and, thus, with hepatitis activity, However, the low cost of testing allocates it in the diagnostic flow chart of HCV infection before the HCV RNA determination: if positive, PCR may be spared, if negative, PCR should be performed,
994 P R O G N O S I S OF L O N G - T E R M RESOLVEMENT FROM H E P A T I T I S C V I R U S INFECTION BY E l ANTIBODY MONITORING. G Maertens. V Barlet*. J-P Zarski*. L Stuvver. G de Martynoff. RA Heiitink**. and JT Brouwer***. INNOGENETICS, Ghent, Belgium; *Centre Hospitalier Universitaire, Grenoble, France; **Erasmus University and ***Dijkzigt Hospital Rotterdam, The Netherlands.
Since the current HCV antibody assays do not allow prognosis of resolvement from chronic hepatitis C infection, we investigated whether antibody levels to 2 core, 3 envelope, and 3 non-structural HCV antigens, measured dudng and after IFN-a treatment, could be correlated with long-term clearance of infection.
We initially studied 17 patients with chronic HCV infection [8 long- term responders to therapy (LTR) who completely resolved HCV infection, and 9 non-responders (NR)]. In LTR, most antibodies decreased slightly during treatment, but anti-E1 and anti-E2 antibodies decreased most significantly (P < 0.02). Anti-E1 further waned after treatment (P < 0.02). The pilot study was expanded to 35 patients [14 LTR, 14 NR, 4 partial responders (PR), and 3 initial responders with relapse of infection (RR)]. At the initiation of therapy, LTR were predictable by high anti-E1 levels (P < 0.03). During the 1,5-year follow up period, only anti-E1 antibody titers cleared rapidly in LTR (P < 0.006 at each 6-monthly interval) but not in NR, PR or RR. This clearance remained significant within type 1 or type 3-infected LTR groups (P < 0.05). The continued elevation of E1Ab in RR is of particular interest because it indicated occult (PCR negative) HCV infection.
High E1Ab titers at the initiation of treatment and rapid decrease of anti- E1 levels were predictive of long-term clearance of viral RNA. E1Ab may prove an interesting new prognostic marker for hepatitis C virus infection.
995 CLINICAL APPLICATION OF A FLUORESCENCE ENZYME IMMUNOASSAY FOR HCV CORE PROTEIN E Tanaka 1 , A Matsumoto 1 , M Kobayashi I , T Ichiio 1 . H Imai 1 , T $odeyama 1 , K Kivosawa 1 Y Ohta 2, A Hasegawa3, M Kohara 4. 1Second Dept. of Internal Medicine, Shinshu University School of Medicine, Matsumoto, Japan; 2International Reagents Corp., Kobe, Japan; 3Tonen Corp., Ohi, Japan. 4Dept. of Microbiology, The Tokyo Metropolitan Institute of Medical Science.
Quantitative measurement of HCV viremia is important in assessing viral replication. Recently, a sensitive and quantitative fluorescence enzyme immunoassay (FEIA) for serum HCV core protein, which, like HCV RNA, may reflect HCV viremia, has been developed. Here we evaluate the clinical application of the FEIA in patients with chronic hepatitis C who were treated with interferon (IFN)-¢¢. Patients and Methods: We studied 27 randomly selected patients with chronic hepatitis type C who received interferon (IFN)-a therapy (19 men and 8 women, aged 34 to 62 years); all patients were positive for antibodies to HCV and for HCV RNA in serum and were negative for HBV surface antigen and antibodies to HIV. IFN-cc2.a was administered 9 MIU per dose daily for 2 weeks, then reduced to three times a week for 22 weeks. Patients were regarded as responders if (1) serum ALT concentrations returned to normal during therapy and remained normal for at least 24 weeks after completion of therapy and (2) serum HCV RNA was negative at 4 and 24 weeks after completion of therapy. Patients who did not meet both of these criteria were regarded as nonresponders. HCV core protein was measured by the sandwich FEIA using monoclonal antibodies. Serum samples (0.5 ml) were processed with PEG4000 and 0.5N NaOH before applying FEIA. Cut-off value was set at 20 relative fluorescence intensity (RFI). HCV RNA in serum was measured by nested RT-PCR. Results: Of the 27 patients who were treated with IFN-~, 11 were responders and 16 were nonresponders. The HCV core protein was detected in 25 (92.6%) of the 27 patients before the therapy. The initial serum concentration of HCV core protein was significantly (P< 0,01) higher in nonresponders (median 147, range 21.5-884 RFI) than in responders (median 26.6, range 12.1-324 RFI). Two weeks after initiating IFN-o~ administration, all 11 responders, but only eight of the 16 nonresponders (P< 0.01), tested negative for serum HCV core protein. All responders, but no nonresponders, remained negative for core protein during and after IFN-a therapy. Conclu$1onl These results suggest that the HCV core protein FEIA is useful for predicting the response to IFN-a before and during therapy.
996 SIMPLE FLUORESCENT EIA FOR DETECTION AND QUANTIFICATION
OF HEPATITIS C VIREMIA. T Tanaka1.).. JYN Lau2). M Mizokami3),__E.E
Orit03). E Tanaka4). K Kivosawa4). K Yasui5), Y Ohta6). A Hasegawa7). S
Tanaka 1), ~nd M Kohara 5) 1) Tokyo Metro. Komagome Hosp, Japan. 2)
Univ Florida College of Medicine, USA. 3) Nagoya City Univ., Japan. 4)
Shinshu Univ, Japan. 5) Tokyo Metro Inst Medi Sci Japan. 6) Intern
Reagents Co., Japan. 7) Tonen Co., Japan.
The viral load of hepatitis C virus (HCV), as reflected by HCV viremia, has
been shown to have important clinical implications, in this study HCV core
protein level in serum was evaluated for the detection and quantification of
HCV viremia. HCV core protein in serum was detected using a simple and
sensitive fluorescent enzyme immunoassay (FEtA). HCV core protein was
quantitated in 258 patients with HCV infection. HCV RNA was determined
using the branched DNA (bDNA) assay and RT-PCR. The detection limit of
this FEIA was found between 104-105 copies/ml HCV RNA equivalent and
correlated with bDNA assay (p<O.01). FICV core protein was detected in 81%
of patients with HCV infection (acute hepatitis 4/5, chronic hepatitis 85/104,
liver cirrhosis 64/73 and hepatocellular carcinoma 86/76) but in none of the
healthy subjects and patients with non-HCV related liver diseases. HCV core
protein level in patients with hepatocellular carcinoma was lower compared
to chronic hepatitis and liver cirrhosis (p<0.05). All 26 patients treated with
interferon-(x showed parallel changes between HCV RNA and core protein
levels. This FEIA is sensitive, specific and quick assay (assay time <3 hours)
with at least matching sensitivity with bDNA assay.






















![1877.] Medicine. 241 MEDICINE](https://img.pdfslide.net/doc/110x75/6248decce7f255195063a334/1877-medicine-241-medicine.jpg)




