Embed Size (px)
Citation preview

Clinical Associations of Antiribonucleoprotein Antibodies in Patients With Systemic Lupus Erythematosus
By Evert J. ter Borg, Henk Groen. Gerda How, Pieter C. Limburg.
Aaktje A. Wouda, and Cees G.M. Kallenberg
The authors undertook a cross-sectional study
to investigate the clinical associations of antiri-
bonucleoprotein (anti-RNP) antibodies in 49
patients with systemic lupus erythematosus
(SLE) without other concomitant connective
tissue disorders. The traditional counterimmu-
noelectropheresis (CIE) and the immunoblot-
ting (IB) technique were compared. Clinically,
special attention was given to the identification
of sclerodermalike features. All patients com-
pleted a detailed questionnaire, physical exami-
nation, and additional investigations including
pulmonary function tests, chest roentgeno-
gram, radionuclide transit studies of the esoph-
agus, and nailfold capillary microscopy. Pulmo-
nary function testing and radionuclide transit
studies of the esophagus were very sensitive
for the detection of (subclinical) pulmonary and
esophageal involvement, respectively. Within
the relatively homogeneous SLE population, a
subset was recognized that was characterized
clinically by the presence of sclerodermalike
features such as Raynaud’s phenomenon, scle-
rodactyly, interstitial changes on chest roent-
genogram, and decreased numbers of nailfold
capillary loops, and serologically by the pres-
ence of anti-RNP antibodies. IB was somewhat
more sensitive than CIE for the detection of
anti-RNP (anti-Sm/anti-nRNP) antibodies but
From the Department of Internal Medicine, Divisions of Rheumatology, Clinical Immunology, Pulmonologv, and Vascular Diseases, University Hospital, Groningen. The Netherlands.
Supported by grant 87/CR/64 of the Dutch Foundation Against Rheumatism.
Evert J. ter Borg, MD: Department of Internal Medicine, Divisions of Rheumatology and Clinical Immunology; Henk Groen, MD: Department of Internal Medicine, Divisions of Clinical Immunology and Pulmonology; Gerda Horst; De- partment of Internal Medicine; Division of Clinical Immunol- ogy; Pieter C. Limburg, PhD: Department of Internal Medi- cine, Division of Rheumatology; Aaktje A. Wouda, MD:
Department of Internal Medicine, Division of Vascular Diseases; Cees G.M. Kallenberg, MD, PhD: Department of Internal Medicine, Division of Clinical Immunology.
Address reprint requests to E.J. ter Borg, MD, Rheumatol- ogist, Hospital Rijnstate DH, Lawick van Pabststraat 72, 6814 HK Arnhem, The Netherlands.
o 1990 by W.B. Saunders Company. 0049-0172/90/2003-0003$5.00/0
did not identify other clinical associations. Thus,
anti-RNP antibodies in SLE are associated with
scleroderma-associated features. For clinical
practice, CIE is the technique recommended for
their detection.
@ 1990 by W. 6. Saunders Company.
INDEX WORDS: SLE; antinuclear antibodies; antiribo- nucleoprotein antibodies; autoantibodies.
S YSTEMIC lupus erythematosus (SLE) is characterized by the occurrence of a variety
of autoantibodies directed to cellular antigens such as DNA, RNA, and RNA-protein complexes.’ Anti-double stranded DNA (anti- dsDNA) antibodies are rather specific for SLE and are observed at a high frequency (75% to 95%) in lupus patients with active disease.’ Anti-Sm antibodies are the autoantibodies most
specific for SLE, but they are found at a rela- tively low frequency (20% to 40%).lW3 Antiribonu- cleoprotein (anti-nRNP) (also referred to as anti-(Ul)RNP) antibodies are associated with mixed connective tissue disease (MCTD)4 but can also, in lower titers, be detected in SLE (30% to 40%) .‘,5 Anti-Sm antibodies almost invariably are accompanied by anti-nRNP antibodies whereas anti-nRNP antibodies may occur with- out anti-Sm.’ Antibodies to the SSA and SSB antigens are associated with Sjbgren’s syndrome primarily, but also may occur in SLE (preva-
lence 30% and 15%, respectively).’ Anti-Sm antibodies precipitate uridine-rich
(U) small nuclear (sn)RNAs, in particular Ul, U2, and U4-6, whereas anti-nRNP sera precipi- tate Ul snRNA only.6 The U snRNAs are complexed with a number of polypeptides desig- nated as 70kd and A to G proteins.’ Anti-Sm, in particular, reacts with BB’ and D, while anti- nRNP reacts with 70kd, A and C polypeptides. Anti-Sm and anti-nRNP antibodies are tradition- ally detected by immunodiffusion (ID), passive hemagglutination (PHA) or counterimmunoelec- tropheresis (CIE). However, these methods do not accurately distinguish between antibodies against different snRNA associated polypep-
164 Seminars in Arthritis and Rheumatism, Vol20, No 3 (December), 1990: pp 164- 173

ANTI-RNP ANTIBODIES IN SLE 165
tides. Reactivities with the individual RNAs and
polypeptides can be demonstrated by the RNA- immunoprecipitation (RNA-IP)6 and immuno- blotting (IB)’ techniques, respectively. IB has been found to be more sensitive than the conven- tional methods for the detection of anti-SmgV9 and
anti-nRNP.’ While disease activity in SLE frequently corre-
lates with levels of distinct antinuclear antibodies
(ANAs), in particular anti-dsDNA”*” reports associating ANA specificities with particular disease characteristics are less conclusive.3”2-15 It is uncertain, for example, whether SLE patients with anti-Sm antibodies have higher or lower
incidences of central nervous system disease and renal disease.2*3~‘2,‘3 Anti-nNRP antibodies in
SLE have been associated with a relatively be- nign disease and a low incidence of renal disease.83’3,‘6 SLE patients with anti-dsDNA an- tibodies only were found to have a lower preva- lence of pleuropericardial disease, myositis, and Raynaud’s phenomenon than those with anti-
nRNP antibodies only.‘6 The occurrence of anti- SSB antibodies in SLE has been associated with both increased’ and decreased” prevalences of
nephritis and with an increased frequency of rheumatoid factor (RF) positivity.18 In the pres-
ence of anti-SSA antibodies, an increased fre- quency of photosensitive skin disease, renal in- volvement, and RF positivity has been reported.” However, most of the aforementioned reports used conventional methods for detecting anti- bodies to ribonucleoproteins (anti-RNP antibod- ies) or have been performed in retrospect.
We initiated a cross-sectional study to investi-
gate whether the presence of anti-RNP anti- bodies in SLE is associated with particular clini- cal features, and compared the traditional CIE technique with the supposedly more sensitive IB technique. Special attention was given to the recognition of sclerodermalike features. All pa- tients completed a detailed questionnaire, physi- cal examination, and additional investigations including pulmonary function tests, radionuclide transit studies of the esophagus, and nailfold capillary microscopy.
MATERIALS AND METHODS
Patients
Fifty-eight unselected patients (44 women and 14 men), who agreed to participate in the study
and who fulfilled the revised ARA criteria for the diagnosis of SLE,*’ were included. At the time of study patients had no evidence of clinical disease activity or only minor (but stable) disease activ-
ity.
Diagnostic Criteria
Diagnosis of Raynaud’s phenomenon was based on a typical history of triphasic or biphasic symmetrical attacks of discoloration of the fin-
gers and/or toes on cold or emotional stimuli.*’ Systemic sclerosis, rheumatoid arthritis and
dermato/polymyositis were diagnosed according to previously published and well-accepted cri- teria.22-24 Definite MCTD was defined by the
criteria recently proposed by Sharp.25 CREST syndrome (subcutaneous calcinosis, Raynaud’s phenomenon, esophageal hypomotility, sclerodac- tyly, and teleangiectasia) was diagnosed when four out of the five characterizing criteria were present; all patients had subcutaneous calcinosis.*”
Study Design
Previous historical data, in particular the pres- ence of the 1982 revised SLE ARA criteria,*’
were noted from the chart. All patients com- pleted a detailed questionnaire and physical ex-
amination using a protocol emphasizing the symp- toms and features of connective tissue disorders. Clinical evaluation was performed without know-
ledge of the laboratory findings. All patients had roentgenograms of chest, hands, and feet, radio- nuclide transit studies of the esophagus, nailfold capillary microscopy, and pulmonary function testing. Laboratory investigations included: com- plete blood count, urinanalysis, serum creatinine,
serum creatine phosphokinase (CPK), immuno- globulin M-RF (IgM-RF), C3 and C4 levels. ANAs (titer and fluorescence pattern), anti-
dsDNA antibodies, and anti-RNP antibodies as assessed by CIE and IB.
Roentgenograms of chest, hands, and feet were performed according to routine procedures and judged by three observers without prior knowledge of clinical data. Chest roentgeno-
grams were examined for the presence of intersti- tial lung disease (reticular, nodular, or reticulo- nodular patterns). Roentgenograms of hands and feet were evaluated, in particular, for the pres- ence of erosive changes, narrowing of joint spaces,
166 TER BORG ET AL
acroosteolysis, subcutaneous calcifications, and soft tissue loss of the finger tips.
Radionuclide transit studies of the esophagus
were performed according to routine procedures.
Hypomotility of the esophagus was considered when at least two of three swallowing actions were prolonged.
Nailfold capillary microscopy was performed as described previously.*’ For this study, the total
number of capillaries and the number of enlarged
loops per 5 mm (representative area), as well as the number of giant loops, bushy patterns, and
pearl necklaces of extravasates for the whole distal row of the nailfold capillary wall were
scored. Average values of the left and right
fourth finger (or the third finger if the photo- graph of the fourth finger was missing or could
not be evaluated) were used for statistical analy-
sis. Pulmonary function testing included slow in-
spiratory vital capacity (IVC), forced expiratory
volume in one second (FEV,), total lung capacity
(TLC), and diffusion capacity for carbon monox-
ide (DLCO). Pulmonary function tests were performed after acute pulmonary events had
subsided. IVC and FEV, were measured by a standard water sealed spirometer. TLC was ob- tained by helium dilution according to standard-
ized techniques. IVC, FEV,, and TLC were expressed in liters BTPS (body temperature,
pressure, saturation). FEV, was then expressed
as a percentage of IVC (FEV,/IVC) to adjust for restrictive pulmonary function loss. DLCO
was measured using the single breath technique of Krogh, as modified by Ogilvie and Cotes.”
DLCO was corrected for hemoglobin concentra-
tions to obtain DLCO values under standard conditions and was expressed in mmol/kPa/min. Pulmonary function test results were given as percentages of the predicted value. A pulmonary function test was considered abnormal when below 80% of the predicted value.
Complete blood count, urinanalysis, serum creatinine (normal value ~110 pmol/L) and serum CPK (normal value ~100 U/L) were measured according to routine procedures. IgM-RF (normal value t10 IU/mL) was mea- sured by enzyme-linked immunosorbent assay (ELISA).29 C3 (normal value 0.64 to 1.20 g/L) and C4 (normal value 0.11 to 0.40 g/L) were measured by nephelometry.
ANAs and anti-ds DNA antibodies were deter-
mined by indirect immunofluorescence using hu-
man fetal fibroblasts3’ and Crithidia luciliae,3’ respectively, as a substrate. Serum was consid-
ered ANA positive when a serum dilution of 1:40
was positive. Fluorescence pattern was scored as
homogeneous, speckled (finely or coarsely), rim
or nucleolar. Serum was considered anti-dsDNA
positive when a serum dilution of 1:lO or more
was positive.
Antibodies to extractable nuclear antigens
(anti-ENA) were detected by CIE according to
Kurata and Tan3* using a crude extract from
rabbit thymus acetone powder (RTP; Pel Freeze,
Rogers, AR) as substrate and reference sera
showing identity with the corresponding Center
for Disease Control (CDC; Atlanta, GA) refer-
ences. Three reference sera were used: anti-Sm,
anti-(Ul)RNP and anti-SSB. Anti-SSA was
detected by CIE using human spleen extract as a
substrate. IB was performed with extracts from Hela cell
nuclei as a substrate. Hela cells were harvested at
400 g, washed with phosphate buffered saline
and resuspended in hypotonic buffer (10 mmol/L
Tris-HCl, pH 7.4, 10 mmol/L NaCl, 1.5 mmol/L MgCl,) at a concentration of 1 x 10’ cells/ml.
After swelling, cells were lysed using a Dounce
homogenizer. Nuclei were pelleted at 500 g,
resuspended in a second buffer (lOmmol/L Tris-
HCl, pH 7.4, 400 mmol/L NaCl, 1.5 mmol/L
MgCl,), sonificated four times for 15 seconds,
and centrifuged. The supernatant was put on gel
(extract of 4 x lo6 cells per cm of gel). All steps
were performed at 4°C and a mixture of protease
inhibitors was added throughout the procedure.
Proteins in the extract were separated according to their molecular weights on 12.5% SDS-PAA
gels and transferred electrophoretically onto ni-
trocellulose sheets. The blots were incubated
with the test sera (dilution 1:50) and the bound immunoglobulins were visualized by means of
peroxidase labeled anti-human IgG. Blots were read by two independent observers without knowl-
edge of the clinical data of the patients. For this study, only anti-Sm (BB’ and D) and anti- (Ul)RNP (70 kd, A and C) specific bands were
scored. Anti-Sm antibodies were considered in the presence of the D band with or without the BB’ band. Anti-(Ul)RNP antibodies were consid-
ANTI-RNP ANTIBODIES IN SLE
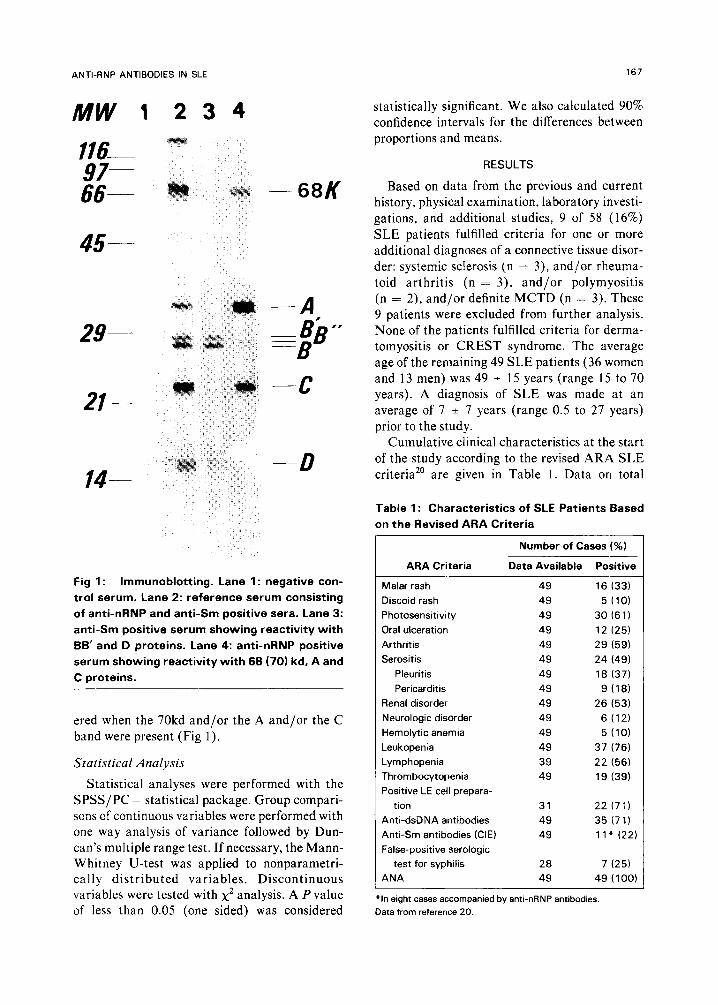
116- 97- 66- - 68K
45-
29-
21--
-A -Bb” =B
-- c
-D
Fig 1: Immunoblotting. Lane 1: negative con- trol serum. Lane 2: reference serum consisting of anti-nRNP and anti-Sm positive sera. Lane 3: anti-Sm positive serum showing reactivity with BB’ and D proteins. Lane 4: anti-nRNP positive serum showing reactivity with 66 (70) kd, A and C proteins.
ered when the 70kd and/or the A and/or the C
band were present (Fig 1).
Statistical Analysis
Statistical analyses were performed with the
SPSS/PC + statistical package. Group compari- sons of continuous variables were performed with one way analysis of variance followed by Dun- can’s multiple range test. If necessary, the Mann- Whitney U-test was applied to nonparametri- tally distributed variables. Discontinuous variables were tested with x2 analysis. A P value of less than 0.05 (one sided) was considered
167
statistically significant. We also calculated 90% confidence intervals for the differences between
proportions and means.
RESULTS
Based on data from the previous and current history, physical examination, laboratory investi- gations, and additional studies, 9 of 58 (16%)
SLE patients fulfilled criteria for one or more additional diagnoses of a connective tissue disor-
der: systemic sclerosis (n = 3), and/or rheuma- toid arthritis (n = 3), and/or polymyositis (n = 2), and/or definite MCTD (n = 3). These 9 patients were excluded from further analysis. None of the patients fulfilled criteria for derma- tomyositis or CREST syndrome. The average age of the remaining 49 SLE patients (36 women
and 13 men) was 49 * 15 years (range 15 to 70 years). A diagnosis of SLE was made at an
average of 7 + 7 years (range 0.5 to 27 years) prior to the study.
Cumulative clinical characteristics at the start of the study according to the revised ARA SLE
criteria” are given in Table 1. Data on total
Table 1: Characteristics of SLE Patients Based on the Revised ARA Criteria
Number of Cases (%)
ARA Criteria Data Available Positive
Malar rash 49 16 (33)
Discoid rash 49 5 (10)
Photosensitivity 49 30 (6 1) Oral ulceration 49 12 (25)
Arthritis 49 29 (59)
Serositis 49 24 (49)
Pleuritis 49 18 (37)
Pericarditis 49 9 (18)
Renal disorder 49 26 (53)
Neurologic disorder 49 6 (12)
Hemolytic anemia 49 5 (10)
Leukopenia 49 37 (76)
Lymphopenia 39 22 (56)
Thrombocytopenia 49 19 (39)
Positive LE cell prepara-
tion 31 22 (7 7)
Anti-dsDNA antibodies 49 35 1711
Anti-Sm antibodies (CIE) 49 1 1.e (22)
False-positive serologic
test for syphilis 28 7 (25)
ANA 49 49 (100)
“In eight cases accompanied by anti-nRNP antibodies.
Data from reference 20.

168
lymphocyte counts were not evaluable in some
patients because they were already on corticoster- oids at the time of referral to our hospital. In addition, in some cases LE cell and syphilis test
results are lacking as they are not routinely performed in our department.
Twenty-one patients (43%) used corticoste- roids. Four patients used cytostatic agents, three of whom also used corticosteroids. Raynaud’s phenomenon was present in 26 of 49 patients (53%). Eight patients had swollen fingers (16%) and sclerodactyly was present in five cases. Four patients had dysphagia by history and three of these had an increased radionuclide transit time of the esophagus. Persistent dyspnea and/or
dyspnea on exertion was present in 12 cases. Chest roentgenograms showed interstitial ab-
normalities in 19 patients (39%). Nodular pat-
terns occurred most frequently. Interstitial abnor- malities on chest roentgenograms were more frequently found in the patients with dyspnea (75%) compared with the patients without dys- pnea (27%; P < .005; 90% confidence intervals
0.24 to 0.72). Roentgenograms of the hands and feet showed
ligamentous calcifications of the small finger
joints in six cases. Erosive changes, narrowing of joint spaces, acroosteolysis, subcutaneous calcifi- cations, and loss of soft tissue of the finger tips were not observed. One patient had (nonerosive) deformities of the hands due to Jaccoud’s ar-
thropathy. Radionuclide transit time of the esophagus
was increased in 14 of 46 patients (30%). Only 3
of these 14 patients (2 1%) had dysphagia by history.
Nailfold capillary microscopy findings were evaluable in 42 patients. Mean (*SD) number of capillary loops per 5 mm was 38 + 6 loops (range 17 to 48). The average number of widened loops per 5 mm was 1.0 f 1.4 loops (range 0 to 6). Considering the whole distal row of the nailfold capillary wall, giant loops were observed in only 3
TER BORG ET AL
patients while bushy patterns and pearl neck- laces of extravasates were seen in 12 and 11 patients, respectively.
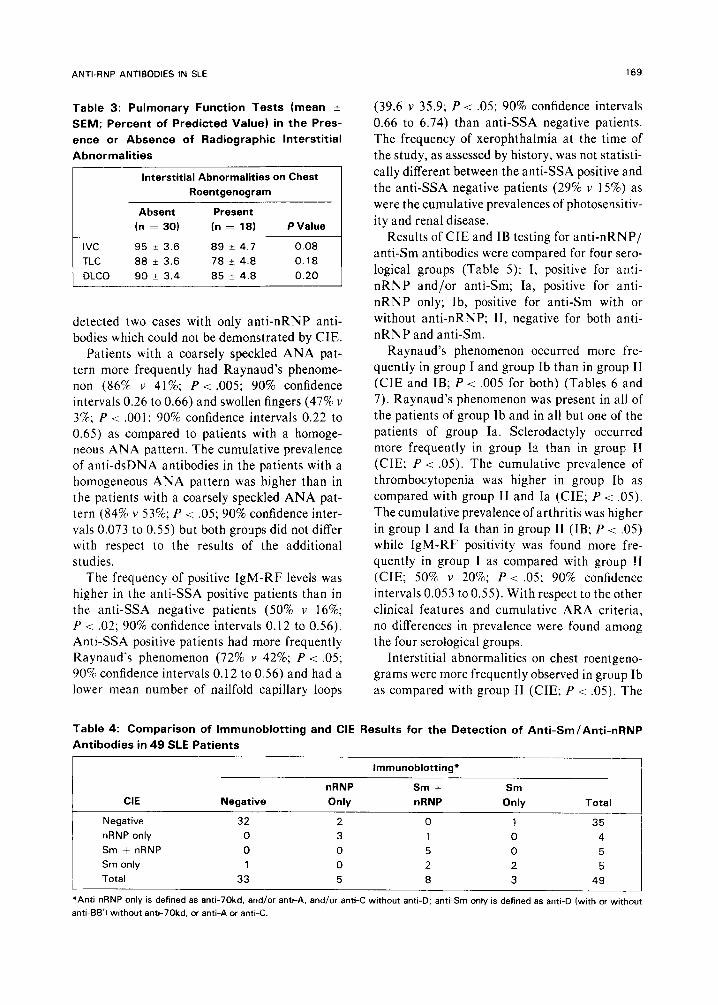
Pulmonary function test results, expressed as percentage of the predicted value, are given in Table 2. DLCO and IVC were the pulmonary function variables most frequently decreased. The prevalence of one or more disturbed (~80% of the predicted value) pulmonary function test (n = 28) was much higher than the prevalence of dyspnea (n = 12). In Table 3, results of pulmonary function tests are compared for pa- tients with (n = 19) and without (n = 30) inter- stitial abnormalities on chest roentgenogram. Values of IVC, TLC, and DLCO tended to be lower in the first group but the differences were not statistically significant.
Leukopenia (~4.0 x 109/1) and thrombocy- topenia (cl00 x 109/1) were present in 11 and 5 cases, respectively. Fourteen patients had posi- tive IgM-RF titers. Eight patients had increased
levels of serum creatinine (> 110 hmol/L) while levels of CPK were increased in three cases. Twenty-one and 13 cases had decreased levels of C3 and C4, respectively. Dip-stick method test- ing showed proteinuria in 16 patients. Microhe- maturia (>5 erythrocytes per high power field) and erythrocyte casts were observed in eight and
one cases, respectively. Forty-eight of 49 patients had a positive (21:
40) ANA test while anti-dsDNA was detected in
16 (33%) patients. Most patients had a homoge- neous (n = 32, 65%) or coarsely speckled (n = 15, 31%) ANA pattern. One patient had a finely speckled pattern; nucleolar and rim pat- terns were not observed. By CIE, anti-SSA antibodies were detected in 18 patients. In two of
these cases anti-SSB was also found. Results of CIE and IB with respect to the detection of anti-RNP (anti-Sm/anti-nRNP) antibodies are
given in Table 4. CIE proved somewhat less sensitive for the detection of anti-RNP anti- bodies (n = 14,29%) than IB (n = 16,33%). IB
Table 2: Results of Pulmonary Function Tests Expressed as Percent of Predicted Value
No. No. of Patients
of Patients Mean f SD Range ~80% Predicted Value
WC 48 84 20 35-136 18 TLC 48 93 20 46-148 12 DLCO 45 88 19 59-135 18
ANTI-RNP ANTIBODIES IN SLE 169
Table 3: Pulmonary Function Tests (mean k
SEM; Percent of Predicted Value) in the Pres-
ence or Absence of Radiographic Interstitial
Abnormalities
Interstitial Abnormalities on Chest
Roentgenogram
IVC
TLC
DLCO
Absent
(n = 30)
95 + 3.6
88 -+ 3.6
90 + 3.4
Present
(n = 181
89 + 4.7
78 + 4.8
85 k 4.8
P Value
0.08
0.18
0.20
(39.6 v 35.9; P -c .05; 90% confidence intervals
0.66 to 6.74) than anti-SSA negative patients.
The frequency of xerophthalmia at the time of
the study, as assessed by history, was not statisti-
cally different between the anti-SSA positive and
the anti-SSA negative patients (29% v 15%) as
were the cumulative prevalences of photosensitiv-
ity and renal disease.
detected two cases with only anti-nRNP anti- bodies which could not be demonstrated by CIE.
Results of CIE and IB testing for anti-nRNP/ anti-Sm antibodies were compared for four sero-
logical groups (Table 5): I, positive for anti-
nRNP and/or anti-Sm; Ia, positive for anti-
nRNP only; Ib, positive for anti-Sm with or
without anti-nRNP; II, negative for both anti-
nRNP and anti-Sm.
Patients with a coarsely speckled ANA pat-
tern more frequently had Raynaud’s phenome- non (86% v 41%; P -c .005; 90% confidence intervals 0.26 to 0.66) and swollen fingers (47% v 3%; P < .OOl; 90% confidence intervals 0.22 to 0.65) as compared to patients with a homoge- neous ANA pattern. The cumulative prevalence
of anti-dsDNA antibodies in the patients with a homogeneous ANA pattern was higher than in the patients with a coarsely speckled ANA pat-
tern (84% v 53%; P < .05; 90% confidence inter- vals 0.073 to 0.55) but both groups did not differ with respect to the results of the additional studies.
The frequency of positive IgM-RF levels was higher in the anti-SSA positive patients than in the anti-SSA negative patients (50% v 16%; P < .02; 90% confidence intervals 0.12 to 0.56). Anti-SSA positive patients had more frequently Raynaud’s phenomenon (72% v 42%; P -c .05; 90% confidence intervals 0.12 to 0.56) and had a lower mean number of nailfold capillary loops
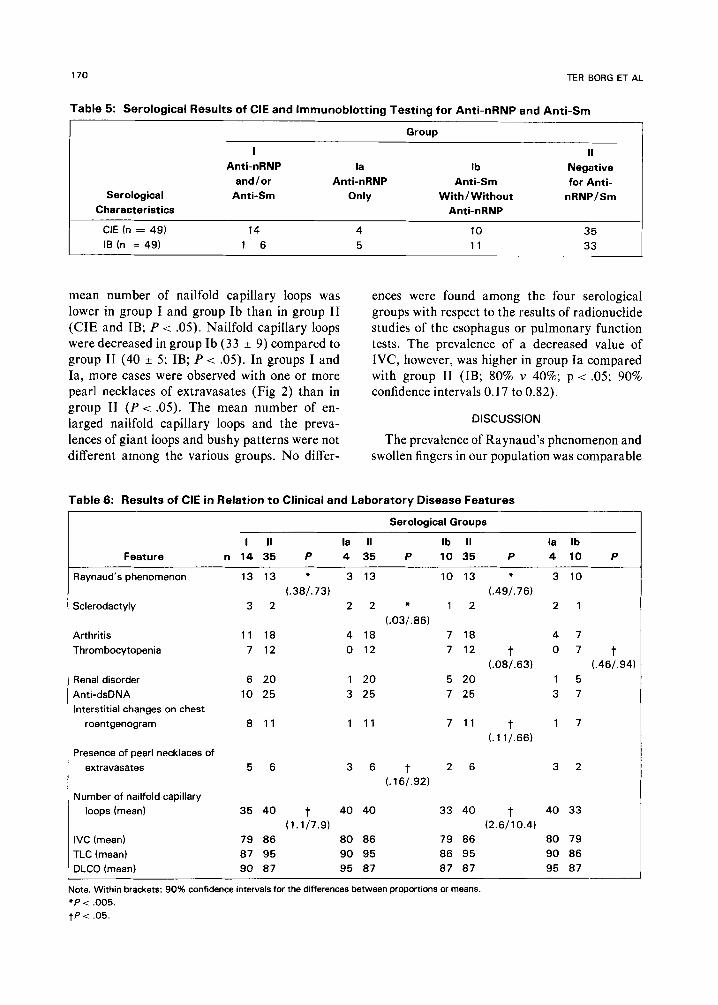
Raynaud’s phenomenon occurred more fre- quently in group I and group Ib than in group II
(CIE and IB; P < ,005 for both) (Tables 6 and
7). Raynaud’s phenomenon was present in all of the patients of group Ib and in all but one of the
patients of group la. Sclerodactyly occurred more frequently in group Ia than in group II
(CIE; P < .05). The cumulative prevalence of
thrombocytopenia was higher in group Ib as compared with group II and Ia (CIE; P <: .05).
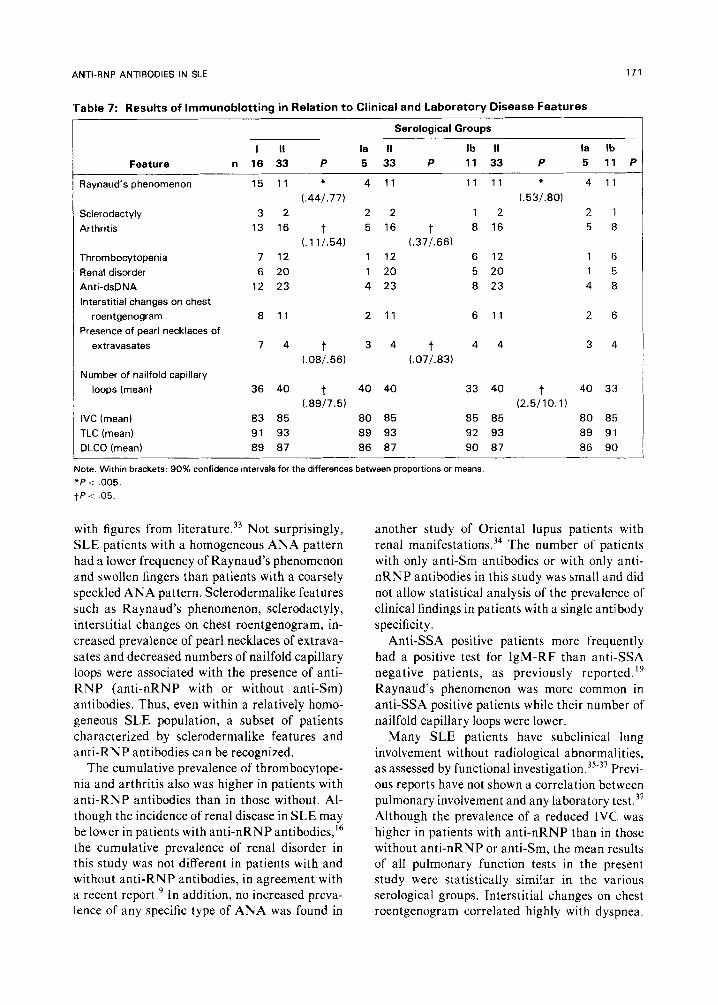
The cumulative prevalence of arthritis was higher
in group I and la than in group II (IB; P -z .05) while IgM-RF positivity was found more fre-
quently in group I as compared with group !I
(CIE; 50% v 20%; P < .05; 90% confidence intervals 0.053 to 0.55). With respect to the other
clinical features and cumulative ARA criteria,
no differences in prevalence were found among the four serological groups.
Interstitial abnormalities on chest roentgeno-
grams were more frequently observed in group Ib
as compared with group II (CIE; P < .05). The
Table 4: Comparison of lmmunoblotting and CIE Results for the Detection of Anti-Sm/Anti-nRNP
Antibodies in 49 SLE Patients -
Immunoblotting’
nRNP Sm + Sm CIE Negative Only nRNP Only Total
Negative 32 2 0 1 35
nRNP only 0 3 1 0 4
Sm + nRNP 0 0 5 0 5
Sm only 1 0 2 2 5
Total 33 5 8 3 49
j ‘Anti-nRNP only is defined as anti-70kd, and/or anti-A, and/or anti-C without anti-D; anti-Sm only is defined as anti-D (with or 3without
anti-BB’) without ant!-70kd. or anti-A or anti-C.
170 TER BORG ET AL
Table 5: Serological Results of CIE and lmmunoblotting Testing for Anti-nRNP and Anti-Sm
Group
I II Anti-nRNP la lb Negative
and/or Anti-nRNP Anti-Sm for Anti- Serological Anti-Sm Only With/ Without nRNP/Sm
Characteristics Anti-nRNP
CIE (n = 49) 14 4 10 35
IB (n = 49) 1 6 5 11 33
mean number of nailfold capillary loops was
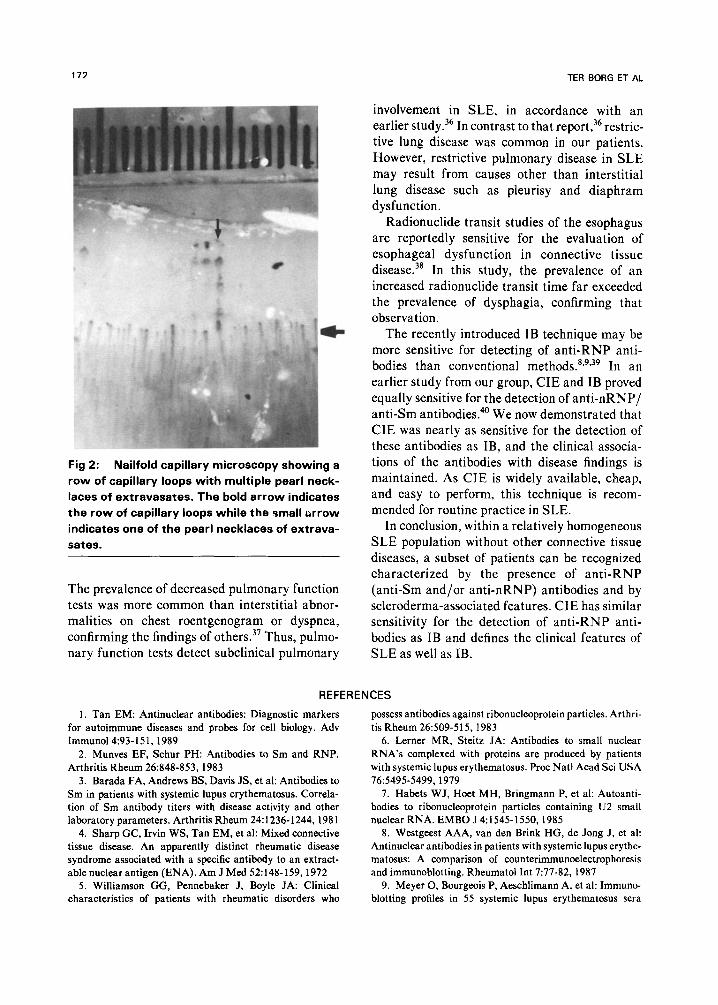
lower in group I and group Ib than in group II (CIE and IB; P < .05). Nailfold capiIlary loops were decreased in group Ib (33 * 9) compared to group II (40 f 5; IB; P -c .05). In groups I and Ia, more cases were observed with one or more pearl necklaces of extravasates (Fig 2) than in
group II (P -c .05). The mean number of en- larged nailfold capillary loops and the preva- lences of giant loops and bushy patterns were not
different among the various groups. No differ-
ences were found among the four serological groups with respect to the results of radionuclide studies of the esophagus or pulmonary function tests. The prevalence of a decreased value of
IVC, however, was higher in group Ia compared with group II (IB; 80% v 40%; p < .05; 90% confidence intervals 0.17 to 0.82).
DISCUSSION
The prevalence of Raynaud’s phenomenon and
swollen fingers in our population was comparable
Table 6: Results of CIE in Relation to Clinical and Laboratory Disease Features
Serological Groups
I II la II lb II la lb
Feature n 14 35 P 435 P 10 35 P 410 P
Raynaud’s phenomenon 13 13 l 3 13 10 13 l 3 10
(.38/.73) (.49/.76)
Sclerodactyly 3 2 22 l 1 2 2 1
(.03/.86)
Arthritis 11 18 4 18 7 18 4 7
Thrombocytopenia 7 12 0 12 7 12 t 07 t (.08/.63) (.46/.94)
Renal disorder 6 20 1 20 5 20 1 5
Anti-dsDNA 10 25 3 25 7 25 3 7
Interstitial changes on chest
roentgenogram 8 11 1 11 7 11 t 1 7
(. 1 l/.66)
Presence of pearl necklaces of
extravasates 5 6 36 t 2 6 3 2
(. 16,‘.921
Number of nailfold capillary
loops (mean) 35 40 t 40 40 33 40 t 40 33
(1.1/7.9) (2.6/10.4)
IVC (mean) 79 86 80 86 79 86 80 79
TLC (mean) 87 95 90 95 86 95 90 86
DLCO (mean) 90 87 95 87 87 87 95 87
Note. Within brackets: 90% confidence intervals for the differences between proportions or means.
l P < .005.
tP < .05.
ANTI-RNP ANTIBODIES IN SLE 171
Table 7: Results of lmmunoblotting in Relation to Clinical and Laboratory Disease Features
Serological Groups
I II la II lb II la lb Feature n 16 33 P 5 33 P 11 33 P 5 11 P
Raynaud’s phenomenon 1511 + 4 11 1111 l 4 1’1
C.441.77) (.53/.80)
Scterodactyly 3 2 2 2 1 2 2 1
Arthritis 13 16 t 5 16 t 8 16 5 8
(. 111.54) (.37/.66)
Thrombocytopenia 7 12 1 12 6 12 1 6
Renal disorder 6 20 1 20 5 20 1 5
Anti-dsDNA 12 23 4 23 8 23 4 6
Interstitial changes on chest
roentgenogram 8 11 2 11 6 11 2 6
Presence of pearl necklaces of
extravasates 7 4 t 3 4 t 44 3 4
(.08/.56) (.07/.83)
Number of nailfold capillary
loops (mean) 36 40 t 40 40 33 40 t 40 33
(.89/7.5) (2.5/10.1)
IVC (mean) 83 85 80 85 85 85 80 85
TLC (mean) 91 93 89 93 92 93 89 9’1
DLCO (mean) 89 87 86 87 90 87 86 90
Note. Within brackets: 90% confidence intervals for the differences between proportions or means
fP < ,005.
tP < .05.
with figures from literature.33 Not surprisingly, SLE patients with a homogeneous ANA pattern had a lower frequency of Raynaud’s phenomenon and swollen fingers than patients with a coarsely
speckled ANA pattern. Sclerodermalike features such as Raynaud’s phenomenon, sclerodactyly, interstitial changes on chest roentgenogram, in- creased prevalence of pearl necklaces of extrava- sates and decreased numbers of nailfold capillary loops were associated with the presence of anti- RNP (anti-nRNP with or without anti-Sm) antibodies. Thus, even within a relatively homo- geneous SLE population, a subset of patients characterized by sclerodermalike features and anti-RNP antibodies can be recognized.
The cumulative prevalence of thrombocytope- nia and arthritis also was higher in patients with anti-RNP antibodies than in those without. Al- though the incidence of renal disease in SLE may be lower in patients with anti-nRNP antibodies,16
the cumulative prevalence of renal disorder in this study was not different in patients with and without anti-RNP antibodies, in agreement with a recent report.’ In addition, no increased preva- lence of any specific type of ANA was found in
another study of Oriental lupus patients with renal manifestations. 34 The number of patients with only anti-Sm antibodies or with only anti- nRNP antibodies in this study was small and did not allow statistical analysis of the prevalence of clinical findings in patients with a single antibody
specificity. Anti-SSA positive patients more frequently
had a positive test for IgM-RF than anti-SSA negative patients, as previously reported.” Raynaud’s phenomenon was more common in anti-SSA positive patients while their number of
nailfold capillary loops were lower. Many SLE patients have subclinical lung
involvement without radiological abnormalities, as assessed by functional investigation.35-37 Previ- ous reports have not shown a correlation between pulmonary involvement and any laboratory test.37 Although the prevalence of a reduced IVC was higher in patients with anti-nRNP than in those without anti-nRNP or anti-Sm, the mean results of all pulmonary function tests in the present study were statistically similar in the various serological groups. Interstitial changes on chest roentgenogram correlated highly with dyspnea.
172 TER BORG ET AL
Fig 2: Nailfold capillary microscopy showing a
row of capillary loops with multiple pearl neck-
laces of extravasates. The bold arrow indicates
the row of capillary loops while the small arrow
indicates one of the pearl necklaces of extrava-
sates.
The prevalence of decreased pulmonary function tests was more common than interstitial abnor- malities on chest roentgenogram or dyspnea, confirming the findings of others.37 Thus, pulmo- nary function tests detect subclinical pulmonary
involvement in SLE, in accordance with an earlier study.36 In contrast to that report,36 restric- tive lung disease was common in our patients. However, restrictive pulmonary disease in SLE may result from causes other than interstitial
lung disease such as pleurisy and diaphram dysfunction.
Radionuclide transit studies of the esophagus are reportedly sensitive for the evaluation of
esophageal dysfunction in connective tissue disease.38 In this study, the prevalence of an increased radionuclide transit time far exceeded the prevalence of dysphagia, confirming that observation.
The recently introduced IB technique may be more sensitive for detecting of anti-RNP anti- bodies than conventional methods.8*9”9 In an
earlier study from our group, CIE and IB proved equally sensitive for the detection of anti-nRNP/ anti-Sm antibodies.40 We now demonstrated that CIE was nearly as sensitive for the detection of these antibodies as IB, and the clinical associa- tions of the antibodies with disease findings is maintained. As CIE is widely available, cheap, and easy to perform, this technique is recom- mended for routine practice in SLE.
In conclusion, within a relatively homogeneous SLE population without other connective tissue
diseases, a subset of patients can be recognized characterized by the presence of anti-RNP
(anti-Sm and/or anti-nRNP) antibodies and by scleroderma-associated features. CIE has similar sensitivity for the detection of anti-RNP anti-
bodies as IB and defines the clinical features of SLE as well as IB.
REFERENCES
1. Tan EM: Antinuclear antibodies: Diagnostic markers
for autoimmune diseases and probes for cell biology. Adv
immunoI4:93-151,1989
2. Munves EF, Schur PH: Antibodies to Sm and RNP.
Arthritis Rheum 26:848-853, 1983
3. Barada FA, Andrews BS, Davis JS, et al: Antibodies to
Sm in patients with systemic lupus erythematosus. Correla-
tion of Sm antibody titers with disease activity and other
laboratory parameters. Arthritis Rheum 24:1236-1244,198l
4. Sharp GC, Irvin WS, Tan EM, et al: Mixed connective
tissue disease. An apparently distinct rheumatic disease
syndrome associated with a specific antibody to an extract-
able nuclear antigen (ENA). Am J Med 52:148-159, 1972
5. Williamson GG, Pennebaker J, Boyle JA: Clinical characteristics of patients with rheumatic disorders who
possess antibodies against ribonucleoprotein particles. Arthri-
tis Rheum 26509-515, I983
6. Lerner MR, Steitz JA: Antibodies to small nuclear
RNA’s complexed with proteins are produced by patients
with systemic lupus erythematosus. Proc Nat1 Acad Sci USA
X:5495-5499,1919
7. Habets WJ, Hoet MH, Bringmann P, et al: Autoanti-
bodies to ribonucleoprotein particles containing U2 small
nuclear RNA. EMBO J 4:1545-1550,1985
8. Westgeest AAA, van den Brink HG, de Jong J, et al:
Antinuclear antibodies in patients with systemic lupus erythe-
matosus: A comparison of counterimmunoelectrophoresis
and immunoblotting. Rheumatol Int 7:77-82, 1987
9. Meyer 0, Bourgeois P, Aeschlimann A, et al: Immuno-
blotting profiles in 55 systemic lupus erythematosus sera
ANTI-RNP ANTIBODIES IN SLE 173
lacking precipitating antibodies to extractable nuclear anti-
gens. Ann Rheum Dis 48:594-599,1989
10. Borg ter EJ, Horst G, Hummel EJ, et al: Predictive
value of rises in anti-double stranded DNA antibody levels
for disease exacerbation in systemic lupus erythematosus: a
long term prospective study. Arthritis Rheum 33:634-643,
1990 11. Swaak AJG, Groenwold J, Bronsveld W: Predictive
value of complement profiles and anti-ds DNA in systemic
lupus erythematosus. Ann Rheum Dis 45:359-366, 1986 12. Winfield JB, Brunner CM, Koffler D: Serologic studies
in patients with systemic lupus erythematosus and central
nervous system dysfunction. Arthritis Rheum 21:289-294,
1978
13. Winn DM, Wolfe JR, Lindberg DA: Identification of
a clinical subset of systemic lupus erythematosus by anti-
bodies to the Sm antigen. Arthritis Rheum 22:1334-1337,
1979
14. Field M, Williams DG, Charles P, et al: Specificity of
anti-Sm antibodies by ELISA for systemic lupus erythemato-
sus: Increased sensitivity of detection using purified peptide
antigens. Ann Rheum Dis 47:820-825, 1988
15. Keiser HD, Weinstein J: The detection and identifica-
tion of antibodies to saline extractable nuclear antigens by
counterimmunoelectrophoresis. Arthritis Rheum 23:1026-
1035,198O
16. Reichlin M, Mattioli M: Correlation of a precipitin
reaction to an RNA protein antigen and a low prevalence of
nephritis in patients with systemic lupus erythematosus. N
Engl J Med 286:908-911, 1972 17. Wacicek CA, Reichlin M: Clinical and serological
differences between systemic lupus erythematosus patients
with antibodies to Ro versus patients with antibodies to Ro
and La. J Clin Invest 69:835-843,1982
18. Provost TT: Subsets in systemic lupus erythematosus.
Review article. J Invest Dermatol 72:110-l 13, 1979
19. Provost TT, Ahmed AR, Maddison PJ, et al: Anti-
bodies to cytoplasmic antigens in lupus erythematosus: Sero-
logical marker for systemic disease. Arthritis Rheum 20: 1457-
1463, 1977
20. Tan EM, Cohen AS, Fries JF, et al: The 1982 revised
criteria for the classification of systemic lupus erythematosus.
Arthritis Rheum 25:1271-1277, 1982
21. Allen EV, Brown GE: Raynaud’s disease affecting
men. Ann Intern Med 5:1384-1386, 1932
22. Masi AT, Rodnan GP, Medsger TA, et al: Preliminary
criteria for the classification of systemic sclerosis (sclero-
derma). Arthritis Rheum 23:581-590, 1980
23. Ropes MW, Bennett GA, Cobb S, et al: 1985 revision
of diagnostic criteria for rheumatoid arthritis. Bull Rheum
Dis 9:175-176, 1958
24. Bohan A, Peter JB, Bowman RL, et al: A computer-
assisted analysis of 153 patients with polymyositis and dermatomyositis. Medicine 56:255-286, 1977
25. Sharp GC: Diagnostic criteria for classification of
MCTD, in Kasukawa R, Sharp GC feds): Mixed Connective
Tissue Diseases and Anti-Nuclear Antibodies. Amsterdam,
The Netherlands, Elsevier Science, BV:23-32, 1987
26. Groen H, Withers G, Borg ter EJ, et al: Puhnonary
diffusing capacity disturbances are related to nailfold capil-
lary changes in patients with Raynaud’s phenomenon with
and without an underlying connective tissue disease. Am J
Med 89:34-41, 1990
27. Houtman PM: Microvascular and immunological stud-
ies in Raynaud’s phenomenon. Thesis 1985, University Hos-
pital Groningen, the Netherlands
28. Cotes JE: Lung Function (ed 4). Oxford, UK. Black-
well Scientific, 1979
29. Leeuwen van MH, Westra J, Limburg PC. et al:
Quantitation of IgM, IgA and IgM Rheumatoid factors by
ELISA in rheumatoid arthritis and other rheumatic disor-
ders. Stand J Rheumatol75:25-31, 1988 (suppl)
30. Kallenberg CGM, Snijder JAM, Feltkamp TEW, et
al: Human tibroblasts as a substrate for titration of .antinu-
clear antibodies. Stand J Rheumatol 14:95-96, 1985
3 1. Aarden LA, de Groot ER, Feltkamp TEW: Immunol-
ogy of DNA. III. Crithidin fuciliae: A simple substrate for
the determination of anti-ds DNA with the immunofluores-
cence technique. Ann NY Acad Sci 245:505-515, 1975
32. Kurata N, Tan EM: Identification of antibodies to
nuclear acidic antigens by counter-immunoelectrophoresis.
Arthritis Rheum 19:574-580, 1976
33. Clerck de LS, Meyers KAE, Cats A: Is MCTD a
distinct entity? Comparison of clinical and laboratory tind-
ings in MCTD, SLE, PSS, and RA patients. Clin Rheumatol
8:29-36, 1989
34. Boey ML, Peebles CL, Tsay G, et al: Clinical and
autoantibody correlations in Orientals with systemic lupus
erythematosus. Ann Rheum Dis47:918-923, 1988
35. Holgate ST, Glass DN, Haslam P, et al: Respiratory
involvement in systemic lupus erythematosus. A clinical and
immunological study. Clin Exp Immunol 24:385-395, 1976
36. Andonopoulos AP, Constantopoulos SH, Galanopou-
lou V. et al: Pulmonary function of nonsmoking patients with
systemic lupus erythematosus. Chest 943 12-3 15, 1988
37. Grennan DM, Howie AD, Moran F, et al: Pulmonary
involvement in systemic lupus erythematosus. Ann Rheum Dis 37:536-539, 1978
38. Fitzgerald OM, Bongiovanni G, Hess EV, et al:
Esophageal motility studies in patients with Raynaud’s
phenomenon. J Rheumatol 14:273-277, 1987
39. Combe B, Rucheton M, Graafland H, et al: Clinical
significance of anti-RNP and anti-Sm autoantibodies as
determined by immunoblotting and immunoprecipitation in
sera from patients with connective tissue diseases. Clin Exp
Immunol75: 18-24, 1989
40. Kallenberg CGM, Borg ter EJ, Jaarsma D, et al:
Detection of autoantibodies to ribonucleoproteins by counter-
immunoelectrophoresis, immunoblotting and RNA-immuno-
precipitation: Comparison of results. Clin Exp Rheumatol 8:35-40, 1990