Upload
others
View
7
Download
0
Embed Size (px)
Citation preview
J Clin Pathol 1987;40:1128-1144
Clinical biochemistry of the neonatal period:immaturity, hypoxia, and metabolic diseaseR A HARKNESS
From the Division of Inherited Metabolic Disease, Medical Research Centre, Harrow, Middlesex
SUMMARY This review attempts to provide practical information on common problems in thelaboratory medicine of newborn infants and also considers unresolved problems in achieving neo-natal diagnoses. A common cause of upset in the newborn-intrapartum asphyxia-can now bepositively diagnosed. This leaves a small group whom it is necessary to investigate because they mayhave metabolic disease. The initial investigation of metabolic disease at the district general hospitalshould be limited to the commoner conditions.
This review aims to present everyday practice of clin-ical biochemistry in the neonatal period and to con-sider how cases which need more detailedconsideration by a laboratory medicine team mightbe selected. The neonatal period is from birth to fourweeks of age. Newborn infants require special care,generally for immaturity. For those few whosecondition does not improve with age, a systemof investigation can be devised. Fig 1 shows thebasis for such an approach.For a baby born after a 40 week gestation the most
likely cause for upset is hypoxia during birth; the non-specific but extremely variable clinical changes pro-duced by hypoxia decrease with time after birth. Ondischarge from hospital at about 7-10 days no obvi-ous ill effects may be detectable, but the infant is ontotal bed rest and constantly nursed. Later in life in-creased demands on the central nervous system madeby reading and writing' or the necessity of secretingmore growth hormone2 may show up defects. Infec-tions, like congenital malformations and metabolicdisease, tend to get worse. The pattern of events overtime is of major diagnostic importance. In a preterminfant time also allows the clusters of adaptivechanges, described as maturation, to take place and inall infants permits the healing of birth trauma. Thesuccess of many of the supportive procedures like in-creased oxygen concentration and even ventilation inpreterm infants depends on such maturation.When the infant does not mature normally then a
wide variety of conditions are caused. Anatomical de-fects can be detected clinically or by various imagingtechniques, failing which, they may eventually beshown at necropsy. Congenital disease of the heart,
gut, or renal tract is often clinically apparent. Suchclinically obvious disease is generally detected using asystematic clinical approach. Serious defects whichare not obvious require conscious search with aspecific screening procedure. Congenital dislocationof the hip and phenylketonuria are examples whichare not fatal but later produce obvious and serious"disease".Much has been written about the neonatal period.
Books selected or written by local clinical staff areobviously the best guide to local clinical practice, butmany of them are long. There are also a few extremelypractical guides to clinical practice, but little help isavailable for those in laboratory medicine. The phys-iological principles entailed in the care of the new-born, especially preterm infants, have been reviewed3in addition to the relevant clinical biochemistry pro-cedures.4 Both these reviews focus on the principalworkload of special care baby units that is generatedby the problems of immaturity: "normal" values forconventional clinical biochemical results in newborninfants have been compiled.5The available reference values in the fetus and the
newborn need to be interpreted with caution as theseare often generated at or after delivery when theremight be undiagnosed asphyxia present. Asphyxiacan raise fetal inorganic phosphate and sulphate con-centrations, thus generating an apparent fetal-maternal gradient which may not have existed duringintrauterine life. Such a gradient has already beennoted for sulphate concentration at delivery. Theinclusion of values from infants with undiagnosedintrapartum asphyxia may also be responsible for thehigh upper limits of reference ranges for newborn in-
1128
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
Clinical biochemistry of the neonatal period: immaturity, hypoxia, and metabolic disease
Death
Inherited metabolic disease(congenital malformations)
Hypoxia
o 1 2 3 4 5 6 7 1 2 5 10 15 20Age (days) Age (years)
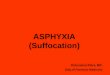
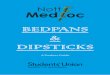
Fig I Changes seen in the patterns of disease intensity with age. Improvement withage occurs after trauma and in the common effects of immaturity and hypoxia.Deterioration with age occurs in the effects of infection, congenital malformations,and inherited metabolic disease.
fants. The values used at Northwick Park Hospital,for example, are uric acid concentration 90-580imol/l, serum aspartate transferase activity 30-75
IU/1, creatine kinase 40-500 IU/l and y glutamyltransferase activity 12-200 lU/1; the urate is a by-product of the increased purine output associatedwith adenosine triphosphate (ATP) depletion and theleakage of enzymes from cells depleted ofATP causesthe high upper limits for the enzyme activities.
This paper aims to help those workers in labora-tory medicine in hospitals which deliver between 1000and 4000 babies each year. Some responsibilities fornewborn infants will probably be a part of their rou-tine work and a relatively large part of theiremergency work. Units with smaller numbers of de-liveries will probably refer their perinatal problems,preferably in utero, or failing that, in ambulances.
Attempts are made later in this review to integratethe every day care of the newborn with the problemsof diagnosis of metabolic disease. The small range ofdiagnoses made in special care baby units contrastswith the long lists of possibilities and the success ofsome screening programmes.6 Antenatal diagnosismust also be mentioned as it is one factor that affectsthe incidence of open neural tube defects7 andchromosomal anomalies.8
Routine laboratory care of the newborn
GENERAL CONSIDERATIONSMost newborn infants require no special care. About10% are admitted to a special or intensive care unitfrom which many emergency requests can arise. New-
born infants change rapidly, and specimens for anal-ysis should be transported rapidly and biochemistryreports should be available twice daily to reduce theerrors and interruptions inherent in telephonereports. There is also a place for coordinated wardlaboratories used by medical and nursing staff tocarry out simple tests that are urgently needed.
Local experience is used extensively as the basis ofthis review. Such personal practice, however, may notalways be suitable for a different environment. Fur-thermore, accepted practice may not always havebeen adequately evaluated and may reflect the pastrather than the present. Accepted practices likethe extensive use of measurements of sodium andpotassium concentrations are difficult to evaluate andit is even more difficult to change their use. If practiceis not to become frozen into existing rituals it is advis-able to evaluate the uses and limitations of all pro-cedures, including those performed by nurses. Somelaboratories have stopped measuring chloride with-out ill effects, and this indicates that large changes canbe made safely. Safe reductions in emergency requestscan also be achieved by medical laboratory staff.9 1o
ANTENATAL CAREBiochemical care of the newborn begins in the ante-natal ward: routine clinical biochemistry is of littlebenefit. The obstetrician wants to know the fetal age,size, presentation, and fetal risk. Clinical biochem-istry can be fittingly used to measure fetal risk.
Pulmonary maturityIn preterm infants pulmonary immaturity is a majorproblem." Treatment by prolonged ventilation and
V
0
cx
1129
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
1130increased oxygen concentrations is expensive and notentirely safe. In a pregnancy of less than 36 weeks theassessment of pulmonary maturity by amniotic fluidphospholipid concentration-either by thin layerchromatography relative to the internal standard ofendogenous sphingomyelin concentration or by morequantitative methods12 13 provides information onthe risk of respiratory distress. It is true that suchinvestigations are not necessary if the baby must bedelivered for obstetric reasons. Evaluation of ob-stetric risk, however, is usually imprecise, and delaysin delivery are often justifiable because clinicalexperience shows that the stimulation of pulmonarydevelopment for 48 hours before delivery byglucocorticosteroids is effective.
Rhesus isoimmunisationThe extent of Rhesus isoimmunisation can be esti-mated by spectrophotometric estimations of bilirubinin filtered amniotic fluid.12 13 These results offer aprecise guide to treatment, including intrauterinetransfusion.
Oestrogen analyses and time intervals sampled bydifferent proceduresMeasurements of fetal size by ultrasound scanningmay detect fetal growth retardation over an intervalof one or more weeks. The biochemical function ofthe growth retarded or at risk fetoplacental unit canbe estimated from oestrogen excretion over 24 hours.If three or more results show a consistent fall to con-centrations below normal the risk to the fetus is high.If oestrogen excretion is consistently
Clinical biochemistry of the neonatal period: immaturity, hypoxia, and metabolic diseaseand is seen as oliguria or anuria.When oral feeding is difficult or impossible, or in
cases with excessive gut or even renal losses, mon-itoring serum sodium and potassium concentrationsis useful especially if combined with measurements ofserum creatinine. Renal immaturity in preterm in-fants can also result in excessive loss of renal sodiumwhich can be treated with supplements. Diagnostic-ally confusing amounts of lactose and galactose aswell as amino acids are also found in urine from pre-term infants.Hypoglycaemia The third major need is for an en-ergy source. Hypoglycaemia can occur in the new-born, particularly in preterm infants who haveinadequate glycogen stores and an inability to per-form gluconeogenesis, and in the infants of diabeticmothers. Hypoglycaemic infants may have used theirglycogen stores during intrapartum asphyxia. Regu-lar ward monitoring of blood glucose with dipsticksor tapes is standard practice. The role of the labora-tory is to confirm the dipstick results for which afluoride blood sample is advisable."9Hypocalcaemia Another example of physiologicalimmaturity is hypocalcaemia. This can also followintrapartum hypoxia, possible due to defectiverenal hydroxylation of 25-hydroxycholecalciferol.Experienced clinicians will recognise slight "jit-teriness" as a good guide to this condition. Mea-surement of serum or plasma calcium is thereforeoften requested and the results of treatment aregood.20 Only if there is no response to a calciumsupplement for about three days is it justifiable tomeasure serum magnesium. Hypomagnesaemiacomplicating hypocalcaemia has been reported andboth respond well to supplementary magnesium.Hypomagnesaemia alone is virtually unknown:emergency magnesium estimations cannot thereforebe justified. It is rare for any infants to require furtherinvestigation for any of the diseases associated withincorrect calcium metabolism despite clear and evenrecurrent evidence of neonatal hypocalcaemia. Suchinvestigations are only practicable in a metabolicallystable and mature infant.Jaundice The immaturity of detoxication systems isseen in the "physiological" jaundice of the newborn,in which rapid breakdown of fetal haemoglobin andits further metabolism can not be adequately per-formed by the liver. Unconjugated bilirubin concen-tration rises to a peak at 3-5 days of age, and this maybe measured by various side room bilirubinometersthat simply measure the yellow colour of plasma orserum, or even skin. These are adequate at bilirubinconcentrations of less than 200 pmol/l and can mon-itor the effects of phototherapy as well as hepatic mat-uration, thus saving the laboratory a large load ofemergency and routine bilirubin estimations. These
instruments are less reliable, however, at high concen-trations, and laboratory methods are needed for clin-ical decisions such as exchange transfusion. 17Jaundice is the clearest example of a condition whichis, initially, nearly always "physiological imma-turity." If it persists and especially if a pronouncedrise in conjugated bilirubin occurs investigation isrequired.The "problem oriented" case record has been used
in the systematic investigation of neonatal jaundiceby Mathew and Wharton.2' Their chart showingserial plots of plasma bilirubin against age in days,with an action limit for phototherapy at about 250/mol/l and that for exchange transfusion at about350 umol/l, is similar to charts used in many units.Their careful documentation of experience withinfants born in 1976 (n = 1988) suggested that theiraction limits may need changing and that the selectionof tests which are going to yield useful diagnoses fortheir population should be changed. Possible ABOincompatibility was common (34 cases) but un-suspected infection was rare (four cases), and tran-sient and questionable hypothyroidism occurred infour preterm infants. Congenital hyperbilirubinaemiawas found in three cases with probable neonatal"hepatitis". There were two infants with chronic ill-ness, one with a "pulmonary syndrome", and anotherhad propionic acidaemia that was unresponsive tobiotin. Neither glucose-6-phosphate dehydrogenasedeficiency nor galactosaemia were detected in any in-fant. A systematic review of the investigation ofjaun-dice will produce an effective local protocol.Breast milk jaundice The incidence of breast milkjaundice is between 1 and 2%.22 As the milk of aspecies is adapted to the nutrition of that species23breast feeding is encouraged. Breast feeding has againbecome more popular in some areas of the UnitedKingdom.24 Detailed consideration of breast milkjaundice is thus justified. The mean rise in bilirubinconcentration in breast fed infants may be no largerthan in formula fed term but not preterm infants.25 In1-2% ofmother and infant pairs, however, there is anicterogenic effect of human but not cow's milk.The often cited association between
5,B-pregnane-3a,20,B-diol in human milk and jaundicecame from New York. It has been confirmed that5#-pregnane-3cx,20#-diol was present in lactatingmothers with jaundiced infants26 but disappeared af-ter the end of lactation. These mothers probably hadsome abnormality of the steroid metabolism of thelactating mammary gland. The predominantly 5astructure for steroids in milk and studies ofmammarygland metabolism in vitro suggest that the breastchanges the pattern of steroids in milk from that inplasma.2728 Large doses of steroids can raise uncon-jugated bilirubin concentrations in plasma in the new-
1 131
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
Harkness
NEWBORN AND INFANTSeizures, convulsionsHypotoniaPersistert vomitingDrowsinessOdd smell
Acidotic breathingEstablished failure to thrive
DIAGNOSIS OF ORGANIC ACIDURIAS AND AMINO r
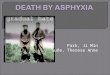
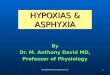
Fig 2 Scheme for the diagnosis of organic acidurias and amino acidopathies in sickchildren.90
born,29 and milk causing jaundice was inhibitory invitro to glucuronyl transferase activity. Such in-hibition, however, was not explained by the effects of5#-pregnane-3ca,20#-diol.30
General consideration of bilirubin metabolism sug-gested that a wide variety of medium molecularweight compounds could be responsible for breastmilk jaundice.31 Many steroids inhibit steroid gluc-uronyltransferase activity with similar micromolar in-hibition constants32 and might therefore inhibitbilirubin detoxication by these enzymes. A surveymethod, suitable for the identification of peaks usinggas chromatography-mass spectrometry (GC-MS),was applied to milk.33 -36 The method showed a lowconcentration of pregnanediones from pregnanediolsand pregnanolones in human milk (table 1), with noincreases found in milk causing breast milk jaundice.Another sensitive GC-MS method did not detectpregnanediols in human milk.37Many studies on the transmission of steroid ana-
logues,38 39 other drugs,40 and insecticides41 in milkhave shown low concentrations. Any such compoundfound in milk has been of a low and usually biologi-cally unimportant dose; the exceptions have beenlisted in advice to prescribers.42
Table I Steroids in human milkfrom mothers withjaundiced (n = 9) and normal (n = 6) infants
Quantity inNormal Age Steroid detected in GC finalfractioninfants* (days) survey (jag/lOOml milk) t1 4 Sa androstane-3,17-dione 0-572 S,B pregnane-3,20-dione 0-083 5a and 5S
androstane-3,17-dione 0-12 and 0-125a pregnane-3,20-dione 0-12
4 5x androstane-3,17-dione 0-29
Jaundiced infants*1 5 5cx androstane-3, 1 7-dione 0-462 14 S1 androstane-3,17-dione 0073 15 5a androstane-3,17-dione 0-15
17 0-164 18 Sa androstane-3,17-dione 0-17
23 0-215 28 Sac androstane-3,17-dione 0-06
42 0-2763 0-2184 Sf androstane-3,17-dione 0-06
6 21 Sf1 pregnane-3,20-dione 0-29
*Milk from three mothers with jaundiced infants and from twomothers with normal infants contained no detectable steroids.tOS0 jg/I00 ml = 14 nmol/l.Data from JAB Darling, the Department of PaediatricBiochemistry, Royal Hospital for Sick Children, Edinburgh.
1132
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
Clinical biochemistry of the neonatal period: immaturity, hypoxia, and metabolic disease
It was clear from gas chromatography (figs 1 and2)67 and from thin layer chromatography evidencethat human milk contained more lipid soluble me-dium molecular weight compounds than cows's milk.There was, however, no component on thin layerchromatography or gas chromatography that was as-sociated with jaundice in the infants receiving themilk (Darling and Harkness, unpublished obser-vations, 1975). There were, therefore, more potentialinhibitors in human milk30 but no one compound andcertainly no pregnanediol could account for the jaun-dice. The evidence suggests that some breast milkjaundice is due to cumulative inhibitory effects fromsmall amounts of many compounds on bilirubin de-toxication and excretion. Many different compoundsare detoxicated by the same mechanisms as bilirubin;specifically, the glucuronyl transferases are "recep-tors" of wide specificity.32
Care should be exercised in checking the specificityof analytical methods used on milk: it has not provedpossible to confirm reports of high vitamin D sul-phate concentrations in milk based on a colourimetricmethod.43The large numbers of compounds in human milk
may arise from a highly varied diet compared withthat of dairy cattle. Specifically, it seems pointless toanalyse milk for pregnanediols.
MAINTENANCE OF WARD AND SIDE ROOMMETHODSMention has been made of the techniques wherebyward blood glucose monitoring can be checked andits quality maintained. The laboratory can also use-fully train medical and nursing staff and check theirperformance.17 -19 A simple technique to reduceanomalous results is for the performance of the actualbottle of sticks used to be checked. A poor batch mayresult from changes that have occurred during stor-age, or from operator errors. Quality control for thebilirubinometer can in practice depend on com-parison of results from ward and laboratory from thesame patient at about the same time.17 The increasinguse of dry stick methods is clinically desirable and willincrease.A simple and robust instrument like a refrac-
tometer used for measurements of urine specific grav-ity or a bilirubinometer in a side room may only needto be cleaned after use. A stock of commonly neededspares must also be kept. These requirements can beefficiently handled at ward level.Complex machinery like existing blood gas assem-
blies requires regular quality control and servicechecks by laboratory staff. The machine must there-fore be in continuous use to compensate for the workneeded to maintain it in good order, otherwise, it
should be placed in the general laboratory medicinearea.A careful and agreed definition of responsibilities in
the area of ward and side room methods, with a con-tinuing communication network among designatedstaff can avoid unnecessary conflicts. In the NHS thisis difficult except at consultant level. The recommen-ded guidelines on the performance of chemical pa-thology assays outside the laboratory18 provides auseful guide to harmonious working practices.
NEWER DEVELOPMENTS: DRUG MONITORINGExpensive developments in laboratory methods arean ongoing problem for those assigning resources.After enthusiasts show that their procedure can beuseful there is a need for critical assessment of costand of benefit and a clear description of where andhow such methods can solve or prevent clinical prob-lems.Drug monitoring is potentially one of the most ex-
pensive areas of laboratory medicine and may be ofparticular importance in the newborn period becausethe neonate lacks the necessary detoxication systems.The vulnerability of developing systems is also high:examples are the sensitivity of multiplying mito-chondria to chloramphenicol44 and of myelin tohexachlorophene."The prescription of antibiotics on suspicion or risk
of infection is common in special care baby units, al-though less than 40% of neonates have any definiteevidence of infection. Gentamicin is often used whichrequires regular monitoring to avoid toxicity. An-other widely used drug, which is regularly monitoredin the newborn, is theophylline, a stimulant to therespiratory centre used in preterm infants who haveperiodic apnoea. Apnoea is usually well tolerated andoccurs about five to seven days after delivery whenthe baby has excreted the caffeine derived from itsmother. Methylated xanthines have very much longerhalf lives in newborn infants than in adults. Althoughgood cost benefit assessments are not available, theuse of theophylline in the newborn has been re-viewed.46The use of drugs only on specific indications is ad-
visable but this is difficult in practice. The intensiveefforts made to save newborn infants, especially pre-term infants, require the administration of many po-tent drugs. To avoid unnecessary side effects thesafest course would be to improve the standards ofdiagnosis, an area in which laboratory medicine has amajor role.
THE CHRONIC CARE OF PRETERM INFANTSOnce the problems of pulmonary immaturity areover, the care of preterm infants focuses on nutrition,which makes great demands on mothers and nurses.
1133
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
Harkness
AI
468.3%0 * "4 95.5%--- .
*- 99.7% V /o
- 1
Mean Homeostasis
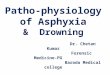
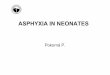
Fig 3 Convergence ofprocesses to produce any final product allows homeostasis to mask adefect five stages away from its initial cause (line 1). Unless variables at or near the primarydefect are measured, overlapping values will be found (lines 3 and 4). Lines 1-5 representvalues of different variables in a chain of causal events. The values of the different variablesare plotted as standard deviations of the normal population from the mean. The relativeamounts of the normal "population" encompassed by 1, 2, and 3 standard deviations, 68-3,95 5, and 99 7% respectively, are indicated below the normal distribution.
The excess loss of sodium caused by the failure of thekidney to respond to aldosterone can be detected byregular estimations of serum sodium and potassium.Calcium deficiency can also occur and cause rickets;radiological diagnosis is unequivocal but not soonenough. Gross increases of alkaline phosphatase ac-tivity in plasma can be shown but the wide variationin normal values still renders interpretation of earlychanges difficult.
Diagnosis in the newborn
The need for transient "homeostatic" care concealsmany diagnostic problems. A widely adopted solu-tion is to conduct diagnostic investigations only if thestate of the baby does not improve with time (fig 1).Many major and eventually fatal anomalies com-patible with live birth also allow four to five days ofextrauterine life. In the first two to three days of lifethe assumption that the major problems are transientproducts of immaturity and do not require a diagno-sis is probably justifiable, but severe infections and
intrapartum hypoxia must be diagnosed. At presentboth infections and intrapartum hypoxia are diag-nosed on non-specific signs similar to those listed intable 2 and fig 2, indicating metabolic disease.
DIAGNOSIS AND MEASUREMENT OF HYPOXICDAMAGEIntrapartum asphyxia is common, being severeenough to cause clinical problems in 1% of allbirths.47 Infection can usually be successfully treatedby antibiotics. Anatomical abnormalities are de-tectable by detailed clinical examination and imagingtechniques. The positive laboratory diagnosis ofintrapartum hypoxia would help obstetricians andallow a small group of children to be selected whoshow signs attributable to hypoxia, but in whom in-herited or congenital metabolic disease are consideredmore likely because they show no specific evidence ofhypoxic damage. It is probable that in this group arefound many of the permanent neurological defectspreviously ascribed to asphyxia. A variety of evidence
1134
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
Clinical biochemistry of the neonatal period: immaturity, hypoxia, and metabolic diseasesuggests that we may be overdiagnosing asphyxia as acause of long term handicap.
The diagnostic use of non-specific variables and therelated overlapping distribution of variables Why arewe continually trying to measure risk and evenachieve diagnoses using overlapping distributions ofvariables? Because we use commonly disturbed vari-ables which are the end products ofmany rarer, initialdefects. Many different initial defects converge to pro-duce a final effect like growth failure. Fig 3 gives anexplanation of the overlapping distribution of vari-ables, which represents values of several associatedvariables.Most variables used in monitoring show poor dis-
crimination between normal and abnormal (fig 3).This arises because the initial defects causing the dis-turbances are several stages removed, and thedifferent linking stages are all subject to homeostaticmechanisms that tend to restore values to normal. Inother words, the further away a measurement is madefrom the site of a primary defect, the greater the over-lap produced by homeostasis between normal and ab-normal distributions of values. Good discriminationis probably the reason for the consistent progress thatis being made in the diagnosis and treatment of rareconditions. This progress contrasts with the negativeor equivocal results of trials of methods detectingfinal common products, like intrauterine growth fail-ure.
Table 2 Features suggesting metabolic disease
I Clinical features and findings of routine investigations:Persistent vomitingPoor feeding, failure to thrive
Neurological abnormalities depressed consciousness fromsomnolence and lethargy to coma, convulsions, hypoventilationand hyperventilation, absence or loss of functions expected inthe newborn, such as ability to suck and swallow
Liver abnormalitiesAcute liver failure, jaundice, bleeding, depressed conscious state,
large or small liver depending on stage of diseasePronounced or prolonged jaundiceHepatomegaly with or without splenomegalyMetabolic acidosisAbnormal smellUnexplained hypoglycaemiaNeutropenia, thrombocytopenia, particularly with metabolic
acidosisHyponatraemia/hyperkalaemia with or without ambiguous
genitaliaMiscellaneous, and less commonly, diarrhoea, hypothermia,abnormal hair, cardiomegaly and heart failure, cataract
2 Important supporting factors:Family history of similar incidents or unexplained deathFamilial consanguinityOnset of illness corresponds to a change of feeding practice, or the
timing of symptoms related to feedsSymptoms improve on glucose/saline fluidsOnset of illness associated with infection, fasting, or surgery.
Data modified from Holton JB. Ann Clin Biochem 1982;19:389-95.
12-2 0 Meconumstaired
0E /-ho,; 0 4
O-
.C _-
' 48a :; 4 4
Umbilical cord Maternalartery vein peripheral
vein
* 0
* 0 0
Caesareansection 0
*
r X 1 1 X0 1 2 3 4 5 6 7 8 9 10
Hours after rupture of membranes
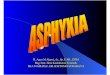
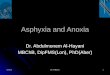
Fig 4 Amnioticfluid and cord blood plasma concentrationsof hypoxanthine, xanthine, and urate from mother and childmonitored during labour, showing criteria offetal distress,fetal heart rate abnormalities, and meconium stainedamniotic fluid.
Because several initial or primary defects convergeto produce changes in growth, for example, growthfailure is more common than any one individual pri-mary or initial defect and is therefore a tempting tar-get. Clinically, it is rarely practicable to measure eachdifferent primary or initial defect, but the routine de-tection of intrauterine growth failure by ultrasoundexamination is only useful in a high risk group be-cause of the overlapping distributions of values.Clinical assessment Clinical diagnosis and assess-ment of damage due to intrapartum hypoxia dependon non-specific signs,48 49 many of which are rankedto produce a cumulative Apgar score.50 The Apgarscore, however, is too insensitive to measure theefficacy of obstetric procedures which are now begin-ning to lower the stillbirth rate. If obstetric inter-vention is successful infants are born with high Apgarscores after showing signs of intrauterine hypoxia,such as slowing of the fetal heart following uterinecontractions and meconium staining of amnioticfluid.pH and blood gas variables The use of pH and bloodgas variables in cord blood and even from fetal scalpto assess hypoxia are limited in their application. Theperiod of time sampled is limited to about 30 minutesor less.5' The widespread evidence of a lack of cor-relation of cord blood pH or hypoxanthine52 5 (fig 4)or newborn pH after resuscitation54 with fetal dam-age is largely due to the rapid changes of pH andother variables in blood. As labour generally lastsmore than four hours a more "cumulative" record ofhypoxic damage is needed. Moreover, most changes
1135
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
1136
Hypoxanthi neCarbon dioxide pCO2
Fig 5 Energy generation in the cell by the mitochondriaand cytosol using oxygen and glucose to produce the energycurrency of the cell ATP. During depletion ATP is brokendown to hypoxanthine. Glycolysis is reflected by lactateconcentrations which can affect blood pH. The sites ofdefects in A TP generation are indicated by asterisks andinclude hypoxia, hypoglycaemia, and ischaemia, as well asintracellular defects in glycolysis, organic acid metabolism,other mitochondrialfunctions and a variety ofgeneticdefects in nuclear DNA.
in pH are due to metabolic acidosis and reflect lactateconcentrations which are produced by anaerobic gly-colysis. Anaerobic glycolysis can maintain ATP con-centrations in many tissues, especially in the fetus.Measurement of pH does not reflect a fall in ATPconcentrations, which is the critical initial event inmetabolic damage caused by hypoxia.
ATP METABOLISM IN HYPOXIANew methods of assessmentIt is possible to define asphyxia at the molecular levelas a failure ofenergy supply sufficient to cause cellulardamage. As the energy currency of cells is the purinenucleotide ATP the definition is, "ATP depletionsufficient to cause irreversible or partially reversiblecellular damage," (which also covers damage byhypoglycaemia). ATP is confined to living cells butATP depletion can be measured in extracellular fluidsbecause such depletion increases output of hypoxan-thine, the central intermediate product in purinemetabolism, from tissues into blood, urine, amnioticfluid and cerebrospinal fluid. The mechanisms andquantitative associations between concentrations ofhypoxanthine and tissue energy supply have been es-tablished.S5-60 Fig 5 represents the information pro-
Harknessvided by lactate on the rate of glycolysis and byhypoxanthine on the extent of ATP depletion.The relation between ATP depletion and sub-
sequent tissue damage is more difficult to estab-lish.61 62 Unexpectedly, there is a close positivecorrelation between neurological damage, assessedclinically, and persistently excessive hypoxanthine ex-cretion occurring 24 hours after ATP depletion andlasting for several days.54 63
Anatomical origin of the changes in ATP metabolitesand methods ofsamplingfor clinical analysisEvidence from studies of progesterone and human
5
,g E 2 -$04-
Cc E
87
c, 6s 5
x 4E
O-3' 2
10-
- ~d
4:' .9''b
& 9l- alls0
Fig 6 Plasma concentrations at elective operative deliveriesofhypoxanthine, xanthine, and uridine in samplesfrommaternal artery, peripheral vein, and uterine vein, as well asfetal umbilical vein and artery. Individual patients and theirinfants are shown by the symbols 0, 0, and M.
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
Clinical biochemistry of the neonatal period: immaturity, hypoxia, and metabolic disease
placental lactogen production shows that the fetus,and especially its brain, is more easily damaged thanthe placenta. Systematic studies on this area havebeen made in sheep.64 In man the vulnerability of thefetus was shown from studies of concentrations ofATP metabolites and the related pyrimidine nucleo-side uridine present in maternal artery, peripheral anduterine veins, and fetal umbilical vein and artery sam-ples at operative delivery. Fig 6 shows the results from
5-4-
01rbE 2-1
5-
4-
coa, 3--c E 2-
a :: 1
8-7-
6-- 54
I 2
1-
0-
U.~
IN. Z
Fig 7 Plasma concentrations ofhypoxanthine, xanthine,and uridine samples at emergency operative deliveries frommaternal artery, peripheral vein, and uterine vein, as well asfrom fetal umbilical vein and artery. These patients andtheir infants had only one criterion offetal distress and areshown by the symbols 0, 0, and *.
elective operative deliveries. There is no steep gra-dient, suggesting that there is no excess ATP break-down in the normal fetus. In contrast, emergencyoperative deliveries without evidence of fetal distressshow a trend for higher hypoxanthine concentrationsin the uterine vein (fig 7), consistent with the activemyometrium consuming ATP and releasing hypoxan-thine. In cases with two or more clinical criteria offetal distress, however, the increases in metabolites inuterine vein and umbilical artery compared with um-bilical vein (fig 8) are consistent with a sharp increasein hypoxanthine output due to ATP breakdown bythe fetus but not the placenta during fetal distress.The increases in uridine concentrations show a some-what more consistent pattern and are compatible withthe hypoxanthine concentrations (figs 6-8).The slower breakdown of ATP in the placenta
compared with that of the fetus has been confirmed inthe rat and guinea pig. Their tissue concentrations ofhypoxanthine, xanthine, and uridine are alsosignificantly negatively correlated with the relativeATP concentrations expressed as energy charges.65Similar correlations also exist in human placenta.66The changes occurring in amniotic fluid over a con-
siderable time period, possibly of about 12 to 24hours, however (fig 4),67 68 and later in neonatal urinegive more diagnostic information than the rapidchanges in blood and tissues. Fig 4 shows an abnor-mally high concentration of hypoxanthine in am-niotic fluid in association with meconium staining,and fetal heart rate patterns justifying emergency cae-sarean section. The umbilical artery and vein concen-trations and those in maternal peripheral veinreturned to normal. The study in fig 4 thus illustratesthe weak correlation of the rapidly responsive cordblood variables with antecedent state. It is also clearthat obstetric intervention removes evidence of as-phyxia. Amniotic fluid concentrations of hypoxan-thine may thus become a means of validating andmeasuring the common obstetric diagnosis of fetaldistress.67 68Although the placenta can be a source of tissue for
enzymological confirmation of a diagnosis,69 there isno good biochemical evidence that placentalinsufficiency exists apart from arylsulphatase C or ste-roid sulphatase deficiency. 14 Many routine pro-cedures which assess the placenta are therefore ofdubious value. In the more vulnerable fetus cere-brospinal fluid can be analysed to obtain a neu-rological prognosis from the hypoxanthineconcentration. 55 56 59 60 Hypoxanthine output inurine and amniotic fluid are a record of hypoxia overabout the previous 24-48 hours.57 58 Analyses ofthese fluids in varying combinations may thereforehelp diagnose and assess the effects of intrapartumasphyxia67 68 and cardiac and ventilatory arrest.
1137
!.si -Z(.Zi
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
1138Tissue damage after A TP depletionA wealth of clinical and experimental evidence fromdrowning70 shows that it is the duration of anoxiarelative to the irreducible energy requirements associ-ated with an organ's temperature which determine thereversibility of the changes. After 10 minutes of extra-uterine anoxia the prognosis is poor. In perfused rathearts the duration of low ATP concentrations seems
10-9
8-7-
Z 6E
:D 2~4-32-1-O-
5-
ax 1
0-
11 -
10-a' 8-zz_ 7-
I: 3_2-10i
13-1
77
0-0
(- 4~
c,+ s5 Sa"
&SC
Clinical biochemistry of the neonatal period: immaturity, hypoxia, and metabolic diseaseTable 3 Approximate incidence ofsome metabolic diseasesin populations ofwestern European origin
Approximate No ofDisorder diagnoses per 100 000 births
Cystic fibrosis 50Neonatal hypothyroidism* 25Other endocrine disorderst 30Phenylketonuria 5-25(Histidinemia) 6Homocystinuria IMaple syrup urine disease* IUrea cycle defects* 4Cystinuria 8Non-ketotic hyperglycinaemia* IOrganic acidoses* 3Galactosaemia 2Other carbohydrate disorders* 9Mucopolysaccharidoses 8Other storage disorders 19
*Can cause acute disorder in the perinatal period.tMainly steroid 21-hydroxylase defects and arylsulphatase C orsteroid sulphatase defects.Data modified from Association of Clinical Biochemists Broadsheet,No 237.
most common lethal genetic disease of caucasian pop-ulations.78 In newborn infants it presents as me-conium ileus and the usual pattern of lung diseasedevelops later. The diagnosis depends on the classicsweat test which shows the characteristic abnormallyhigh sodium concentrations. This test combined withthose for meconium albumin and pancreatic functionrequires care and experience with good clinical-laboratory liaison.The high detection rate for endocrine disease may
be due to the early arousal of suspicion by the clin-ically obvious effects of hormones, like virilisation ofexternal genitalia. Similarly, many infants deficient inadenosine deaminase activity (ADA) manifest insevere combined immunodeficiency, have been diag-nosed, although this condition is very rare-about1000 times rarer than phenylketonuria.79 An exten-sive screening programme to detect ADA deficiencyin infants in New York was not helpful and was aban-doned.The known incidence of the storage disorders
caused by acid hydrolase deficiencies has been esti-mated at 27 in 100 000 births, which is high (table 3).In older children the protracted and characteristicclinical course of the storage disorders has been asso-ciated with many successful diagnoses in large num-bers of index cases. As a consequence of successfuldiagnosis of index cases, antenatal diagnoses have be-come highly developed.
USE OF INCIDENCE DATA FOR TREATABLECONDITIONS TO LIMIT INITIAL INVESTIGATIONSAs many paediatric teams care for 2-4000 births peryear they are unlikely to encounter diseases rarer than1 in 10-20 000, in other words one every five years. It
therefore seems practical to suggest that once theteam is clear that a baby is probably ill, an in-vestigation protocol should be initially restricted todiseases with an incidence of about 1 in 10-20000.This proposal is in line with current screening practicefor phenylketonuria, which has an incidence of 1 in10000 and hypothyroidism, which has an incidence of2 in 10000. Of the several thousand possible defects,the number which should be considered by a non-specialist can probably be limited to between 10 and30. Considering the incidence of diagnosable and, as afirst priority, treatable diseases in the population inone's care generally yields a small group of diseases inthe United Kingdom (tables 3 and 4) and for Switzer-land.80The introduction of methods capable of detecting
organic acidoses may increase the detection rate ofthese diseases.8" Three groups are commonly encoun-tered: methylmalonic acidaemias, some of which areB12 responsive; multiple carboxylase deficiencies,which may be biotin responsive; and the generally fa-tal propionic acidaemias. The total incidence may beas high as I in 10 000. From this evidence the neces-sary methods for preliminary diagnosis can bedefined.
It might be helpful to indicate a condition which isimpracticable to detect usefully by whole populationscreening. Maple syrup urine disease is too rare andtoo rapidly fatal for the index case to be saved in mostcases. It is practicable, however, to diagnose a secondcase in an affected family. Newborn infants in whomserious metabolic disease is anticipated can be fed glu-cose and thoroughly and rapidly investigated. Such aprocedure organised from a reference laboratory car-ing for 75 000 births a year detected only six babies atrisk, of whom four were normal. One had massivehepatic necrosis of unknown cause and the other cit-rullinaemia.82
POPULATION SCREENINGPhenylketonuria and congenital hypothyroidism arecommon enough- I and 2 in 10 000-respectively, toproduce a considerable number of live born irre-
Table 4 Incidence ofdiagnosed inherited metabolicdisorders over two years in the United Kingdom
Births
Group Manchester Sheffield Bristoldiagnosis (n = 110000) (n = 60000) (n = 70000)
Amino acids 5 4 1Organic acids 5 2 Not testedUrea cycle 2 1Galactosaemia I 1
Data modified from Association of Clinical Biochemists NewsheetNo 237.
1139
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
1140versibly damaged infants who require continued insti-tutional care. These two conditions are not commonenough, however, to be an effective part of a pae-diatrician's clinical response to their very vague andoften late clinical signs. The unexpected success of thelaboratory screening programmes for phenyl-ketonuria and later for hypothyroidism mitigatesagainst a policy of dismissing all such metabolic dis-ease as too rare to justify diagnostic consideration.With so many possible diseases it is hardly
surprising that such insidious and vague early signsare missed in newborn infants. Reference laboratoriesoften care for patients who have shown early signs(table 2) that were not investigated, but it is imprac-tical to investigate all patients with such signs. Amajor problem is the selection of a high risk group.This needs positive diagnoses for the common causesof the ill defined clinical signs that provide the initialclues. Before it can be justified to adopt screeningprocedures for specific disease most centres regard agood cheap overall screening method with a mini-mum of false positive or negative results and aneffective treatment as vital.
Screening programmes also have limitations.Samples are generally taken on the fifth to eighth dayof life when rapid changes are taking place. Theanalytical problems of measuring large numbers ofcompounds are considerable. In addition, substrateloading by milk feeding is also necessary in galacto-saemia. The success of adapting the hypothyroidand steroid 21-hydroxylation deficiency screeningprogramme to the dried blood sample used forphenylalanine analyses suggests that many morecompounds could be included if abnormalities werecommon enough. Various methods are already avail-able.83 84
Histidinaemia can be reduced with an appropriatediet, but a recent careful and extensive prospectivestudy of histidinaemia detected by whole populationscreening in North America and Japan has shownthat there seems to be no associated disease. Previousassociations were due to selective investigation of anabnormal group.85-88 Histidinaemia is not a "dis-adaptive" phenotype or disease. As well as abnormal-ity being treatable when detected in the second weekof life it is also necessary for there to be an associatedclinical abnormality. Antenatal treatment for mostdefects is at the experimental stage.
In summary, the present pattern seems to be firstly,national population screening by central laboratoriesfor common genuinely treatable disorders with an in-sidious clinically indistinguishable onset and course.The latest candidate for population screening issteroid 21-hydroxylase defects.89 Secondly, stepwiseinvestigation of chronic, progressive severe disease isneeded, in which a conventional clinical approach of-
Harknessten provides a diagnosis, even in very rare conditions.In some United Kingdom centres, alert clinicianshave detected about as many patients with congenitaladrenal hyperplasia as those with phenylketonuria:therefore screening may be avoidable. Thirdly, onlytried and tested beneficial procedures should be ac-cepted into everyday clinical practice.As there are a large number of rapidly fatal meta-
bolic diseases in the newborn period and a high mor-tality we need more effective positive procedures forthis age group. Two cases, which were recently con-sidered at the United Kingdom Medical ResearchCouncil Clinical Research Centre, of the generally fa-tal but treatable condition of congenital ade-nocortical hypoplasia, were admitted to special carebaby units in their respective hospitals with intra-partum asphyxia. This diagnosis is made in a "col-lapsed" infant and both oxygen and cortisoldeficiency cause metabolic failure. After four to fivedays these infants were investigated for persistent un-conjugated hyperbilirubinaemia, a developmentalfailure due to cortisol deficiency.90 Until intrapartumhypoxia can be reliably and rapidly diagnosed, suchneonates with a treatable condition will probably die,diagnosed as asphyxia. In adrenocortical hypoplasia,unlike many other metabolic diseases, a diagnosis atnecropsy is possible and is commonly made.
Diagnosis of rare metabolic causes of disease and therole of the reference laboratories
A severely ill infant aged four to five days or more,without gross congenital anatomical defects or infec-tion, probably has one of more than a 1000 rare dis-eases. The only practicable mechanism for thediagnosis and management of these diseases has beenthe creation of reference centres.9' 92 In this review Ihave indicated how patients should be selected forreferral. Widening the criteria for acceptance of pa-tients for detailed investigation of organic acid-aemias, however, has not increased the number ofcases detected.93 Preliminary local investigation by awell informed paediatric and laboratory team can re-sult in a higher proportion of positive diagnoses.93The investigative flow diagram in fig 2 is similar tothat agreed by a United Kingdom working party.94 Itwas emphasised that the district general hospitalshould take investigation to the second line; the refer-ence laboratory then takes over at the third and finalline.94 It was also emphasised that the reference labo-ratory is available for consultation, and to accept ma-terial it must have been initially consulted. Manyproblems, when defined clearly on the telephone or ina summary letter, are soluble with the clinical andbiochemical experience of the reference laboratoryand require no further investigation. The reference
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
Clinical biochemistry of the neonatal period: immaturity, hypoxia, and metabolic disease
centre can guide initial investigation and interimtreatment. Many endocrine diseases are amenable todiagnosis by a team which can recognise the clinicaleffects of hormones and systematically test even rarepossibilities.95
If the newborn period alone is considered, pub-lished tables of possible causes of metabolic diseaseare lengthy. Haan and Danks96 listed 38 conditions;these tables have been condensed by Holton.97 Con-sideration of the actual United Kingdom incidenceslisted in tables 3 and 4 shows that most of these can beinitially disregarded. The evidence in fig 2 and tables3 and 4 suggest that the following tests should beavailable at a district general hospital.1 Careful check for sodium loss due to steroid
21-hydroxylation deficiency which has an inci-dence of about I in 10000.8489 Urinary concen-trations of sodium greater than 20 mmol/l shouldbe regarded as high in a normally fed full terminfant.
2 An amino acid chromatogram of blood and urinewill show various disorders ofamino acid metabo-lism.
3 Check for persistent metabolic acidosis (at leastplasma bicarbonate) as a reduced concentration isusually seen in organic acidaemia. Simple chro-matographic methods for organic acids are useful.
4 Possibly check plasma ammonia. This is very highin urea cycle defects and hepatic failure.
5 Do a test for galactose. This is a reducing sub-stance that, if shown not to be glucose in the urineof a mature milk fed infant, indicates galac-tosaemia.
6 Perform a sweat test for cystic fibrosis.These tests cover most of the conditions which are
at present recognised and emphasise those which aretreatable. Mucopolysacchridoses and other storagedisorders do not usually present as acute metabolicdisorders in the newborn.
If there are doubts about the results of these teststhen the reference laboratory should be consulted andthe results checked by those with more experience,especially in interpreting amino acid patterns. If allthe test results are negative and the infant is still dete-riorating transfer of the patient to the care of a spe-cialised clinical and laboratory team is advisable.Incurable damage due to failure to detect a treatablecondition should thus be avoided.
It is the role of the reference laboratory to reachsystematically98 one of the many possible diag-noses.99 Current evidence suggests that this is an un-solved problem.100The use of a conventional 12 channel clinical chem-
istry analyser to generate an "admission" profile at apaediatric referral centre made only a small con-tribution to overall care.'0' Most conventional clin-
ical chemistry analyses are of limited use in diagnosisdespite their value in the problems of immaturity. Ex-tensive chromatographic skills can show a variety ofdefects-the profiling of organic and amino acids andof steroids, for example. For confirming diagnoses,the ability to estimate enzyme activities in tissues gen-erally on a micro scale may be required by referencecentres, which will also need extensive clinical experi-ence.
Conclusions
The field of neonatal diagnosis and treatment is con-tinually developing. The acquisition of diagnosticskills is shown in the clustering of case reports of newdiseases.Management of suspected metabolic disease is to
feed the patient only glucose and water for about12-48 hours, when preliminary results should beavailable.82 100 In cases in which death is imminentthe aim should still be to secure a diagnosis. Diagno-sis after death of an index case of maple syrup diseasecan help the affected family. For such diagnosis Bur-ton and Nadler'02 recommended that measurementsof urine, plasma, and sterile skin kept at 37'C or atleast at room temperature in tissue culture medium oreven 5% glucose in physiological saline should be se-cured. The preliminary use of an ethyl chloride spraysterilises skin; alternatively, fascia can be used. Fi-broblasts grow if obtained up to about 48 hours afterdeath. If a necropsy is performed a specimen of freshliver stored at -20°C is also recommended. If thenecropsy shows grossly affected tissues these shouldbe retained. Vitreous humour can be taken atnecropsy'03 and gives clearer amino acid patternsthan other available extracellular fluids. Every effortshould be made, however, to take specimens of blood,urine, and even cerebrospinal fluid before death. Ingeneral, analyses of necropsy specimens are extremelydifficult to interpret.97 104 105 In severely ill infants ahigh index of suspicion for inherited metabolic dis-ease and a readiness to do some tests can produceuseful results.'06
This article could not have been written without theworking collaboration of many clinical and labora-tory medicine colleagues. I acknowledge permissionfor the use of fig 2 from the Journal ofInherited Met-abolic Disease, with permission from the Society forthe Study of Inborn Errors of Metabolism and MTPPress.
The original work reported was undertaken inaccordance with the regulations of the NorthwickPark Hospital and Clinical Research Centre EthicalCommittee.
1 141
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
1142 Harkness
Bibliography
Practical guides for clinicians providing insight into theimmediate care of newborn
Inspect the guides local clinicians use.Brown EJK, Valman HB. Practical neonatal paediatrics.Oxford: Blackwell Scientific Publications, 1979.Chiswick ML. Neonatal medicine. London: Update, 1978.Davies PA, Robinson RJ, Scopes JW, Tizard JPM,Wigglesworth JS. Medical care ofnewborn babies. Clinics indevelopmental medicine. 1972.Keay AJ, Morgan DM. Craig's care ofthe newly born infant.Edinburgh: Churchill Livingstone, 1982.Phillip AGS. Neonatology a practical guide. London: HenryKimpton, 1980.Insley J, Wood B. A paediatric vade mecum. 10th Ed.London: Lloyd Luke, 1982.Roberton NRC. Textbook of neonatology. Edinburgh:Churchill Livinstone, 1986.O'Brien D, Ibbot FA, Rodgerson DO. Laboratory manual ofpaediatric microbiochemical techniques. New York: Harper& Row, 1963. (A guide to early work.)Meites S, ed. Paediatric clinical chemistry. 3rd Edn. AACCPress, 1988.
Major textbooks with references of original articles
Bondy PK, Rosenberg LE. Metabolic control and disease.London: WB Saunders, 1980.Cockburn F, Drillien CM. Neonatal medicine. Oxford:Blackwell Scientific Publications, 1974.Goodwin JW, Godden JD, Chance GW. Perinatalmedicine-the basic science underlying clinical practice.Baltimore: Williams & Wilkins, 1976.Klaus MH, Fanroff AM. Care of the high risk neonate.London: WB Saunders, 1979.Schaffer AJ, Avery ME. Diseases of the newborn. London:WB Saunders, 1977.Wold NJ. Antenatal and neonatal screening. London: OxfordUniversity Press, 1984.
Series of review articles
Clinics in perinatology. London: WB Saunders.Clinics in obstetrics and gynecology. London: WB Saunders.(Relatively little on newborn.)Pediatric Clinics of North America. London: WB Saunders.Advances in pediatrics. Chicago: Yearbook publishers.
References
1 D'Souza SW, McCartney E, Nolan M, Taylor IG. Hearing,speech and language in survivors of severe perinatal asphyxia.Arch Dis Child 1981;56:245-52.
2 Steendijk R. Diagnostic and aetiologic features of idiopathicand symptomatic growth hormone deficiency in the Nether-lands. Helv Paediatr Acta 1980;35:129-39.
3 Hey EN. Physiological principles involved in the care of thepreterm human infant. In: Austin CR, ed. Mammalianfetus invitro. London: Chapman and Hall, 1973:251-356.
4 Evans SE, Durbin GM. Aspects of the physiological and pathol-
ogical background to neonatal clinical chemistry. Ann ClinBiochem 1983;20:193-207.
5 Clayton BE, Jenkins P, Round JM. Paediatric chemicalpathology-clinical tests and reference ranges. Oxford: Black-well Scientific Publications, 1980.
6 New England Congenital Hypothyroidism Collaborative.Effects of neonatal screening for hypothyroidism; preventionof mental retardation before clinical manifestations. Lancet1981;ii:1095-8.
7 Brock DJH. Impact ofmaternal serum alpha-fetoprotein screen-ing on antenatal diagnosis. Br Med J 1982;285:365-7.
8 Weatherall JAC. A review of some effects of recent medicalpractices in reducing the numbers of children born with con-genital abnormalities. Health Trends 1982;14:85-8.
9 Smith ADS, Shenkin A, Dryburgh FJ, Morgan HG. Emergencybiochemistry services-are they abused? Ann Clin Biochem1982;19:325-8.
10 Grivell AR, Forgie HJ, Fraser CG, Berry MN. Effect of feed-back to clinical staff of information on clinical biochemistryrequesting patterns. Clin Chem 1981;27:1717-20.
11 Strang LB. Neonatal respiration physiological and clinical studies.Oxford: Blackwell Scientific Publications, 1977.
12 Holton JB. Diagnostic tests on amniotic fluid. Essays MedBiochem 1977;3:75-107.
13 Fairweather DVI, Eskes TKAB. Amnioticfluid research and clin-ical application. 2nd Ed. Amsterdam: Excerpta Medica 1978.
14 Taylor NF. Placental sulphatase deficiency. J Inher Metab Dis1982;5:164-75.
15 Harkness RA, Taylor NF, Crawford MA, Rose FA. X-linkedichthyosis, cervical dystocia and placental sterolid sulphatasedeficiency. Br Med J 1983;287:2-3.
16 Harkness RA. Fertility, pregnancy and contraception. In:Brown SS, Mitchell FL, Young DS, eds. Chemical diagnosis ofdisease. Amsterdam: Elsevier, 1979:833-50.
17 Harkness RA, Lawrence CR, Renshaw A, Barr IC, BrownSS, Rinsler MG. Assessment of the performance and clinicalutility of a ward side room bilirubinometer. Ann Clin Biochem1983;20:149-52.
18 Anderson JR, Linsell WD, Mitchell FL. Guidelines on the per-formance of chemical pathology assays outside the labora-tory. Br Med J 1981;282:743.
19 King G, Steggles D, Harrop JS. Performance and storage ofreagent strips for measuring blood glucose. Br Med J1982;285:1 165.
20 Salle BL, David L, Chopard JP, Grafmeyer DC, Renaud H.Prevention of early neonatal hypocalcaemia in low birthweight infants with continuous calcium infusion: effect onserum calcium, phosphorus, magnesium and circulatingimmunoreactive parathyroid hormone and calcitonin. PediatrRes 1977;11:1180-5.
21 Mathew PM, Wharton BA. Investigation and management ofneonatal jaundice: a problem oriented case record. Arch DisChild 1981;56:949-53.
22 Stiehm ER, Ryan J. Breast milk jaundice. Am J Dis Child1965;109:212-6.
23 Jelliffe DB, Jelliffe EFP. Human milk in the modern world.Oxford: University Press, 1978:4-8.
24 Coles EC, Cotter S, Valman HB. Increasing prevalence of breastfeeding. Br Med J 1978;2:1122.
25 Editorial Correspondence and cited references. Breast-feedingjaundice. J Pediatr 1982;100:334-46.
26 Rosenfeld RS, Arias IM, Gartner LM, Hellman L,Gallagher TF. Studies of urinary pregnane-3a, 20fl-diolduring pregnancy, postpartum, lactation and progesteroneingestion. J Clin Endocrinol 1967;27:1705-10.
27 Smith JA, King RJB. The metabolism of testosterone by tissuefrom normal and neoplastic mouse breast. J Endocrinol1966;35:281-7.
28 Chatterton RT, Chatterton AJ, Hellman L. Metabolism ofprogesterone by the rabbit mammary gland. Endocrinology
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
Clinical biochemistry of the neonatal period: immaturity, hypoxia, and metabolic disease 11431969;85:16-24.
29 Lauritzen Ch, Lehmann WD. The significance of steroidhormones for the development of hyperbilirubinaemia andicterus in the newborn infant. J Endocrinol 1967;39:183-8.
30 Hargreaves T, Piper RF. Breast milk jaundice effect of inhibi-tory breast milk and 3a, 20fi-pregnanediol on glucuronyltransferase. Arch Dis Child 1971;46:195-8.
31 Dutton GJ. Glucuronic acid. London: Academic Press, 1966:185-99.
32 Rao GS, Rao ML, Breuer H. Partial purification and kinetics ofoestriol 16a-glucuronyltransferase from the cytosol fractionof human liver. Biochem J 1970;118:625-34.
33 Darling JAB, Harkness RA. A method for the group analysis ofsteroids in milk. Acta Endocrinol 1973;72:390-400.
34 Darling JAB, Kelly RW, Laing AH, Harkness RA. The iso-lation and identification of progesterone obtained from cows'milk during pregnancy. J Endocrinol 1972;54:347-8.
35 Heap RB, Gwyn M, Laing JA, Walters DE. Pregnancy diag-nosis in cows; changes in milk progesterone concentrationduring the oestrous cycle and pregnancy measured by rapidimmunoassay. Journal of Agricultural Science (Cambridge)1973;81:1 51-7.
36 Kulshi JK, Smith M, Hartmann PE. Perinatal concentrations ofprogesterone, lactose and a-lactalbumin in the mammarysecretion of women. J Endocrinol 1977;74:509- 10.
37 Murphy JF, Hughes I, Jones ERV, Gashell S, Pike AW.Pregnanediols and breast milk jaundice. Arch Dis Child 1981;56:474-6.
38 Van der Molen HJ, Hart PG, Wijmenga HG. Studies with4-4C-Lynestrenol in normal and lactating women. ActaEndocrinol (Copenhagen) 1969;61:255-74.
39 Wijmenga HG, Van der Molen HG. Studies with 4-"C-Mestranol in lactating women. Acta Endocrinol 1969;61:665-77.
40 Knowles JA. Excretion of drugs in milk-a review. J Pediatr1965;66:1068-82.
41 Wickizer TM, Brilliant LB, Copeland R, Tilden R. Poly-chlorinated biphenyl contamination of nursing mothers milkin Michigan. Am J Public Health 1981;71:132-7.
42 British National Formulary. London. 1983:17-20.43 Greer FR, Reeve LE, Chesney RW, De Luca HF. Water-soluble
vitamin D in human milk: a myth. Pediatrics 1982;69:238.44 Hallman M. Effects of intraperitoneal chloramphenicol on some
mitochondrial enzymes in neonatal rats. Biochem Pharmacol1971;20:1797-809.
45 Anderson JM, Cockburn F, Forfar JO, Harkness RA, KellyRW, Kilshaw B. Neonatal spongioform myelinopathy afterrestricted application of a hexachlorophane skin disinfectant.J Clin Pathol 1981;34:25-9.
46 Soyka LF. Developmental pharmacology of the methyl-xanthines. Semin Perinatol 1981;5:303-8.
47 Brown JK. Infants damaged during birth. In: Hull D, ed. Recentadvances in paediatrics. Edinburgh: Churchill Livingstone,1976:35-86.
48 Beard RW, Rivers RPA. Fetal asphyxia in labour. Lancet1979;ii:1 1 17-9.
49 Chamberlain R, Chamberlain G, Howlett B, Claireaux A.British births 1970. Vol. 1. London: Heinemann, 1970:97-100.
50 Jennett RJ, Warford HS, Kreinick C, Waterkotte GW. Apgarindex: a statistical tool. Am J Obstet Gynecol 1981;140:206-12.
51 Swanstrom S, Bratteby LE. Hypoxanthine as a test of perinatalhypoxia as compared to lactate base deficit and pH. PediatrRes 1982;16:156-60.
52 O'Connor MC, Harkness RA, Simmonds RJ, Hytten FE. Themeasurement of hypoxanthine, xanthine, inosine and uridinein umbilical cord blood and fetal scalp blood samples as ameasure of fetal hypoxia. Br J Obstet Gynaecol 1981;88:381-90.
53 Bossart M, Perret C. Lactate in acute conditions. Basel: Karger,
1979.54 Harkness RA, Whitelaw AGL, Simmonds RJ. Intrapartum
hypoxia: the association between neurological assessment ofdamage and abnormal excretion of ATP metabolites. J ClinPathol 1982;35:999-1007.
55 Harkness RA, Lund RJ. Cerebrospinal fluid concentrations ofhypoxanthine, uridine and inosine: high concentrations of theATP metabolite, hypoxanthine, after hypoxia. J Clin Pathol1983;36:1-8.
56 Meberg A, Saugstad OD. Hypoxanthine in cerebrospinal fluidof children. Scand J Clin Lab Invest 1978;38:437-40.
57 Harkness RA, Simmonds RJ, Coade SB. Purine transport andmetabolism in man: the effect of exercise on concentrations ofpurine bases, nucleosides and nucleotides in plasma, urine,leucocytes and erythrocytes. Clin Sci 1983;64:333-40.
58 Harkness RA, Coade SB, Walton KR, Wright D. Xanthine oxi-dase deficiency and "Dalmatian" hypouricaemia: incidenceand effect of exercise. J Inher Metab Dis 1983;6:114-20.
59 Hallgren R, Niklasson F, Terent A, Akerblom A, Widerlow E.Oxypurines in cerebrospinal fluid as indices of disturbed brainmetabolism. Stroke 1983;14:382-8.
60 Levin SD, Brown JK, Harkness RA. Cerebrospinal fluid hypo-xanthine and xanthine concentrations as indicators of meta-bolic damage due to raised intracranial pressure inhydrocephalic children. J Neurol Neurosurg Psychiatr 1984;47:730-3.
61 Warnick CT, Lazarus HM. Recovery of nucleotide levels aftercell injury. Can J Biochem 1981;59:1 16-21.
62 Kloner RA, Ganote E, Whalen DA, Jennings RB. Effect of atransient period of ischaemia on myocardial cells. Am JPathol 1974;74:399-422.
63 Harkness RA, Simmonds RJ, Coade SB, Lawrence CR. Theratio of the concentration of hypoxanthine to creatinine inurine from newborn infants: a possible indicator for the meta-bolic damage due to hypoxia. Br J Obstet Gynaecol 1983;90:447-52.
64 Thiringer K. Hypoxanthine as a measure of foetal asphyxia.Sheep experiments and clinical study in human neonates.Goteborg: University of Goteborg, 1982 (Thesis.) pp183.
65 Harkness RA, Coade SB, Simmonds RJ, Duffy S. Effect of afailure of energy supply on adenine nucleotide breakdown inplacentae and other fetal tissues from rat and guinea pig.Placenta 1985;6:199-216.
66 Simmonds RJ, Coade SB, Harkness RA, Drury L, Hytten FE.Nucleotide, nucleoside and purine base concentrations inhuman placentae. Placenta 1981;3:29-39.
67 O'Connor MC, Harkness RA, Simmonds RJ, Hytten FE.Raised hypoxanthine, xanthine and uridine concentrations inmeconium stained amniotic fluid and during labour. Br JObstet Gynaecol 1981;88:375-80.
68 Harkness RA, Geirsson RT, McFadyen IR. Concentrations ofhypoxanthine, xanthine, uridine and urate in amniotic fluid atCaesarean section and the association of raised levels withprenatal risk factors and fetal distress. Br J Obstet Gynaecol1983;90:815-20.
69 Rose FA. Review: The mammalian sulphatases and placentalsulphatase deficiency in man. J Inher Metab Dis 1982;5:145-52.
70 Kruus S, Bergstrom L, Suutarinen T, Hyvonen R. The progno-sis of near drowned children. Acta Paediatr Scand 1979;68:315-22.
71 Reibel DK, Roveto MJ. Myocardial ATP synthesis andmechanical function following oxygen deficiency. Am JPhysiol 1978;234:H620-4.
72 Fysh WJ, Turner GM, Dunn PM. Neurological normality afterextreme birth asphyxia. Case report. Br J Obstet Gynaecol1982;89:24-6.
73 Porter R, Whelan J. Human muscle fatigue: physiological mech-anisms. Ciba Foundation Symposium 82. London: PitmanMedical, 1981.
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/
1144 Harkness74 Myers RE, Wagner KR, Courten G. Lactic acid accumulation
in tissue as a cause of brain injury and death. In: LauersenNH, Hochberg HM, eds. Clinical perinatal biochemical moni-toring. Baltimore: Williams and Wilkins, 1981:1 1-34.
75 Bode JC, Zelder 0, Rumpett HJ, Wittkamp U. Depletion ofliver adenosine phosphates and metabolic effects of intra-venous infusion of fructose or sorbitol in man and in the rat.Eur J Clin Invest 1973;3:436-41.
76 Vogt MT, Farber E. On the pathology of ischaemic renal celldeath. Reversible and irreversible cellular and mitochondrialmetabolic alterations. Am J Pathol 1968;53:1-26.
77 Pampiglione G, Chaloner J, Harden A, O'Brien J. Transitoryischaemia/anoxia in young children and the prediction of thequality of survival. Ann NY Acad Sci 1978;315:281-92.
78 Nadler HL, Rao GJS, Taussig LM. Cystic Fibrosis. In:Stanbury JB, Wyngaarden JB, Frederickson DS, eds.Metabolic basis of inherited metabolic disease. New York:McGraw-Hill, 1978:1683-710.
79 Guttler F, Seakins JWT, Harkness RA. Inborn errors of immu-nity and phagocytosis. Lancaster: MTP, 1979.
80 Bachmann C, Colombo JP. Incidence of disorders tested bysystematic screening: confidence limits and comparison ofprogrammes. J Inher Metab Dis 1982;5:3-5.
81 Krieger I, Nigro M, Taqi Q. Screening for metabolic disease ina metropolitan hospital. Am J Dis Child 1982;136:125-8.
82 Danks DM. Management of newborn babies in whom seriousmetabolic illness is anticipated. Arch Dis Child 1974;49:576-8.
83 Murphey WH, Patchen L, Guthrie R. Screening tests forarginosuccinic aciduria, orotic aciduria and other inheritedenzyme deficiencies using dried blood specimens. BiochemGenet 1972;6:51-9.
84 Pang S, Murphey W, Levine LS, Spence DA, Leon A, La-Franchi S, Surve AS, New MI. A pilot newborn screeningprogram for congenital adrenal hyperplasia in Alaska. J ClinEndocrinol 1982;55:413-20.
85 Tade L. Intellectual development in patients with untreatedhistidinemia. A collaborative group study of neonatal screen-ing for inborn errors in Japan. J Pediatr 1983;101:562-3.
86 Scriver CR, Levy HL. Histidinemia Part I: reconciling retro-spective and prospective findings. J Inher Metab Dis 1983;6:51-3.
87 Rosenmann A, Scriver CR, Clow CL, Levy HL. HistidinemiaPart II: Impact, retrospective study. J Inher Metab Dis1 983;6:54-7.
88 Coulombe JT, Kammerer BL, Hirsch BZ, Levy HL, Scriver CR.Histidinemia Part III: Impact; prospective study. J InherMetab Dis 1983;6:58-61.
89 Workshop on screening for congenital adrenal hyperplasia(steroid 21-hydroxylase deficiency). J Inher Metab Dis 1986;9(suppl 1):1 1 1-55.
90 Harkness RA, Taylor NF, Bowman PR, Gordon H, CumminsM, Valman HB. The causes of low oestrogen excretion inpregnancy: the development of diagnostic methods for theantenatal detection of congenital adrenocortical hypoplasia.Clin Endocrinol 1980;12:453-60.
91 Raine DN. Management of inherited metabolic disease. Br Med
J 1972;i:329-36.92 Raine DN. Some principles in the management of inherited
metabolic disease. In: Cockburn F, Gitzelmann R, eds. Inbornerrors of metabolism in humans. Lancaster: MTP, 1982:267-85.
93 Chalmers RA, Purkiss P, Watts RWE, Lawson AM. Screeningfor organic acidurias and amino acidopathies in newborn andchildren. J Inher Metab Dis 1980;3:27-43.
94 Proposals for a co-ordinated scheme for the postnatal diagnosisof inherited metabolic disease in infancy. Association ofClini-cal Biochemists News Sheet 1983;237:6-12.
95 Harkness RA, Thistlethwaite D, Darling JAB, Skakkebaek NE,Corker CS. Neutral 1 7#-hydroxysteroid oxidoreductasedeficiency in testes causing male psuedohermaphroditism inan infant. J Inher Metab Dis 1979;2:51-4.
96 Haan EA, Danks DM. Clinical investigation of suspected meta-bolic disease. In: Barson AJ, ed. Laboratory investigation offetal disease. Bristol: PG Wright, 1981:410-28.
97 Holton JB. Diagnosis of inherited metabolis disease in severelyill children. Ann Clin Biochem 1982;19:389-95.
98 Applegarth DA, Toone JR, MacLeod PM. Laboratory diag-nosis of inborn errors of metabolism in children. PediatricPathology 1983;1:107-30.
99 McKusick VA. Mendelian inheritance in man-catalogs of theautosomal dominant, autosomal recessive and X-linked pheno-types. Baltimore: Johns Hopkins University Press, 1983.
100 Danks DM. Plan of management for newborn babies in whommetabolic disease is anticipated or suspected. In: AmpolaMG, ed. Early detection andmanagement ofinborn errors. ClinPerinatol 1976;3:251-60.
101 Leonard JV, Clayton BE, Colley JRT. Use of a biochemicalprofile in a childrens' hospital: results of two controlled trials.Br Med J 1975;2:662-6.
102 Burton BK, Nadler HL. Clinical diagnosis of the inborn errorsof metabolism in the neonatal period. Pediatrics 1978;61:398-405.
103 Mason JK, Harkness RA, Elton RA, Bartholomew S. Cotdeaths in Edinburgh: infant feeding and socioeconomic fac-tors. J Epidemiol Community Health 1980;34:35-41.
104 Harkness RA, Darling JAB, Bain AD, Syme J. Plasma lecithin-cholesterol acyltransferase deficiency in a child with terminalpulmonary hyaline membrane disease. Arch Dis Child1973;48:906- 10.
105 Adams A, Harkness RA. Adenosine deaminase activity inthymus and other human tissues. Clin Exp Immunol 1976;26:647-9.
106 Nyhan WL. Heriditable metabolic disease in the differential di-agnosis of asphyxia. In: Gluck L, ed. Intrauterine asphyxiaand the developing brain. Chicago: Year Book Publishers Inc,1977:421-9.
Requests for reprints to: Dr RA Harkness, Division ofInherited Metabolic Disease, MRC Clinical ResearchCentre, Watford Road, Harrow, Middlesex HAI 3UJ,England.
copyright. on A
pril 6, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.40.9.1128 on 1 S
eptember 1987. D
ownloaded from
http://jcp.bmj.com/