Embed Size (px)
Citation preview
CLINICAL CASE WITH INSIGHT ON
PRACTICAL, DIAGNOSTIC AND ETHICAL
ASPECTS
NATHALIE ANDERSSON CHRISTINE FONTEYNE
HUDERF UKZKF
11TH SYMPOSIUM OF THE BSPHO
NOVEMBER 2017

MultidisciplinaryTEAM
Support fonction
@ HOME & Hospital
Follows the patient & family
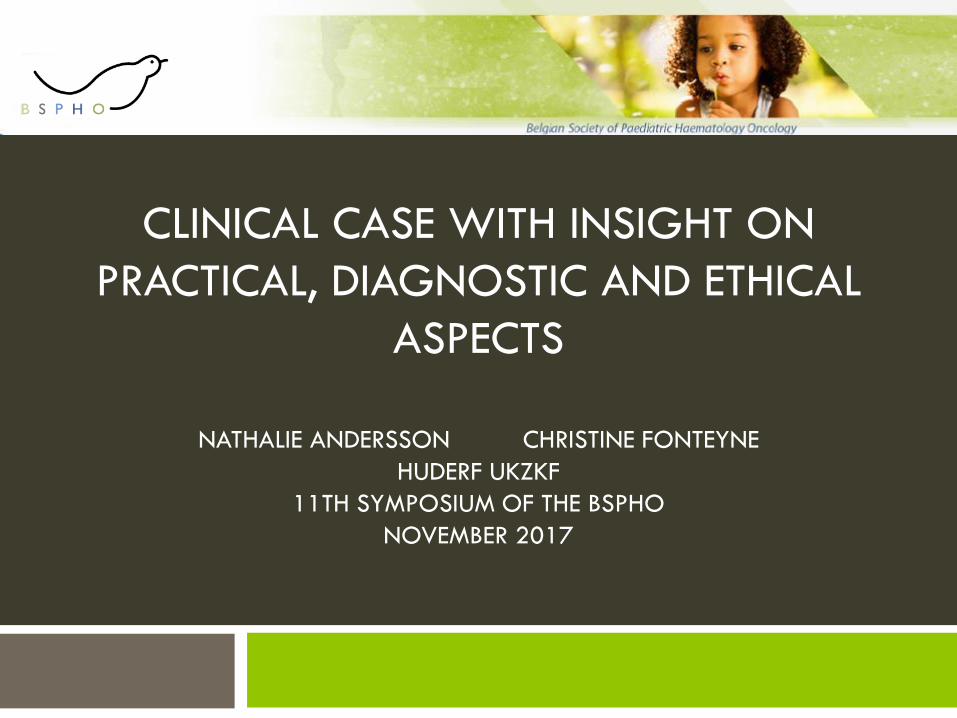
Evelyne
Chemotherapy/su
rgery
October 2015Birth
30/03/201
2
Diagnostic of
Neuroblastoma MS
July 2012
Spontaneous involution
October 2012
First relaps
Neuroblastoma IV
August 2015
Second combined
relaps 7 months after
BMT
October 2016
Hospitalisation
for pain
management &
fever
March 2017Anouncement of
palliative care
& pediatric
palliative care
team
April 2017
24/04/2017
Discharge ward
27/04/2017
readmission
Death
13/05/2017
Advanced
directory
8/05/2017
BMT
9/03/201
6
Question : Would you have announced palliative care at this moment?
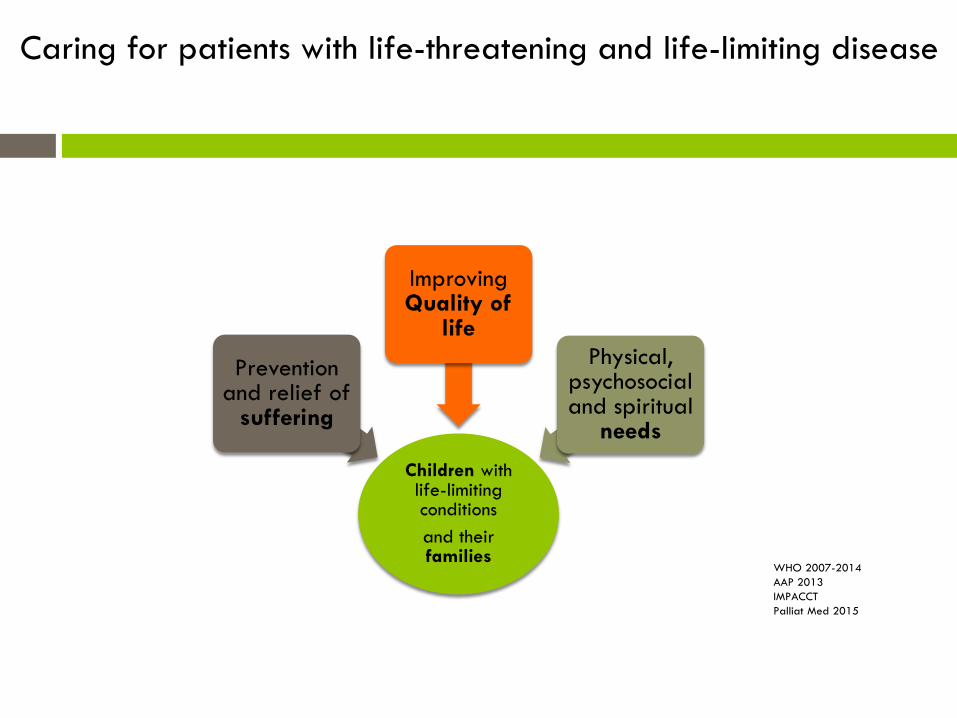
Children withlife-limitingconditions
and theirfamilies
Preventionand relief of
suffering
ImprovingQuality of
life
Physical, psychosocial and spiritual
needs
WHO 2007-2014
AAP 2013
IMPACCT
Palliat Med 2015
Caring for patients with life-threatening and life-limiting disease
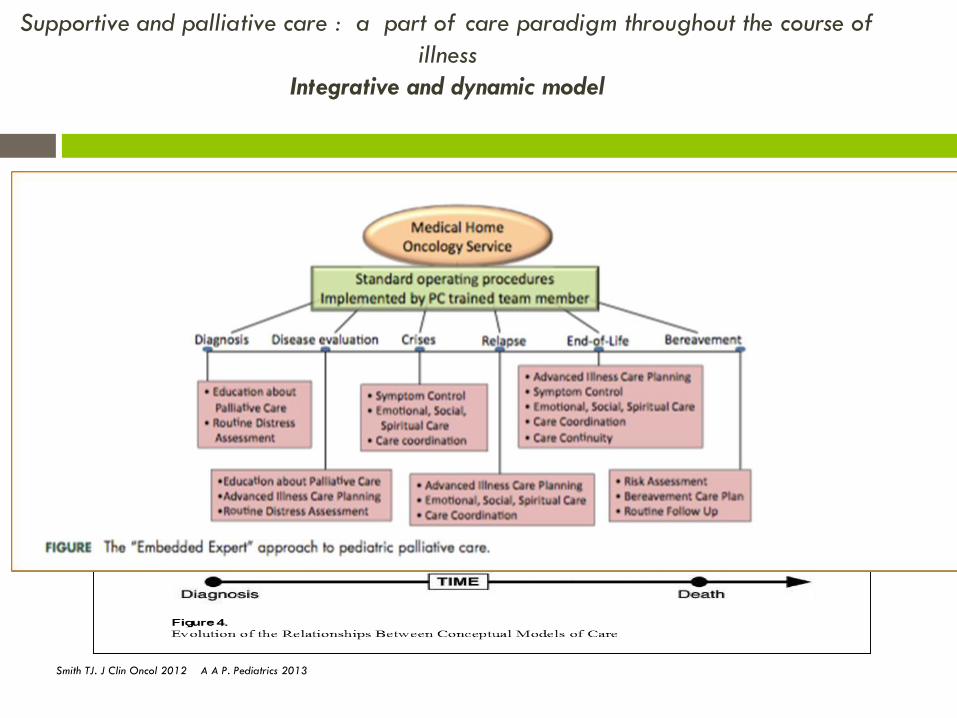
Supportive and palliative care : a part of care paradigm throughout the course of
illness
Integrative and dynamic model
Smith TJ. J Clin Oncol 2012 A A P. Pediatrics 2013
Outcomes improved with pediatric
palliative care involvement ( EBM)
High quality palliative care (control of symptoms pain, dyspnea, anxiety)
Understanding of the goals and values of patient and families
Psychosocial and spiritual support for children and families
↓ hospital admissions
↓ death in intensive care units
Location of death (home)
Prolongs survival (adults)
Wolfe J. J Clin Oncol 2008 Greer JA. J Clin Oncol 2012 Kassam 2015 Friedrischdorf 2015 Temel JS. N Engl J Med 2010
Belgian legislation
2016
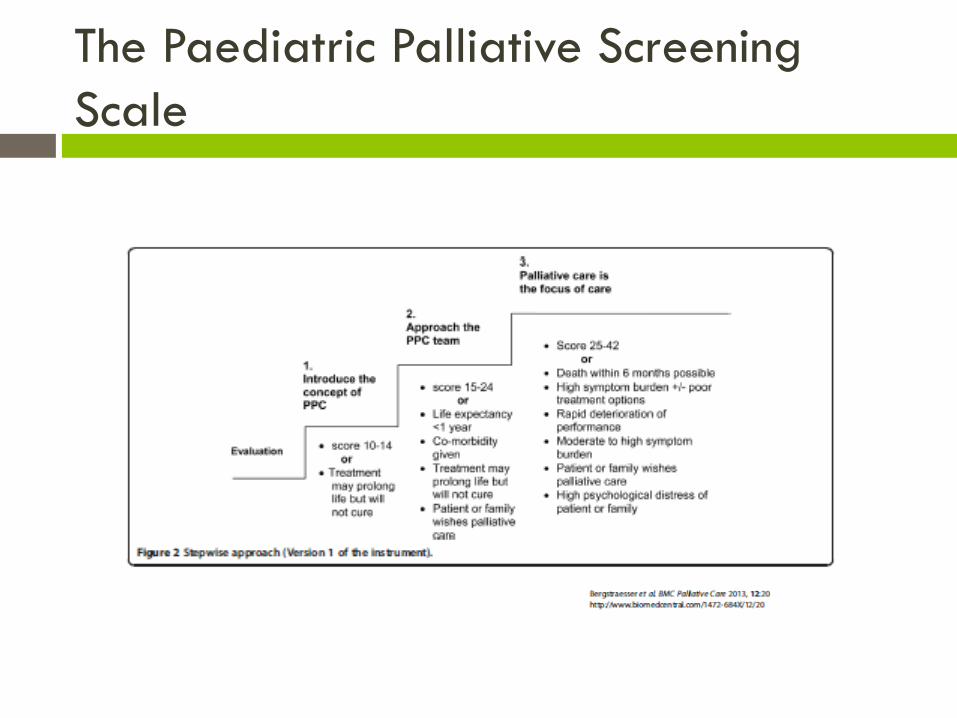
The Paediatric Palliative Screening
Scale
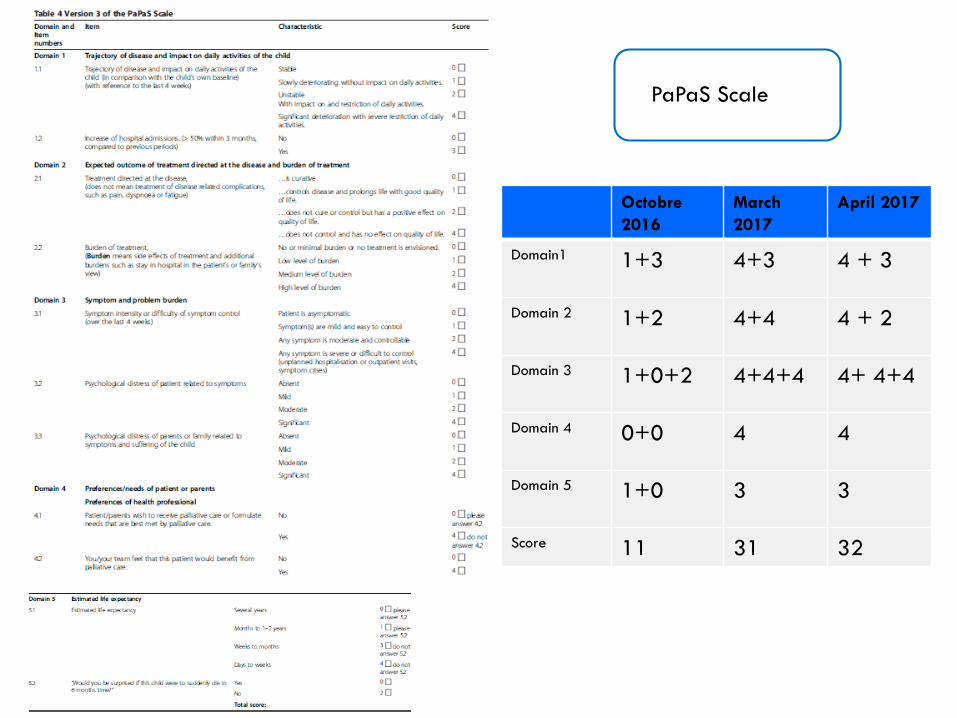
Octobre
2016
March
2017
April 2017
Domain1 1+3 4+3 4 + 3
Domain 2 1+2 4+4 4 + 2
Domain 3 1+0+2 4+4+4 4+ 4+4
Domain 4 0+0 4 4
Domain 5 1+0 3 3
Score 11 31 32
PaPaS Scale
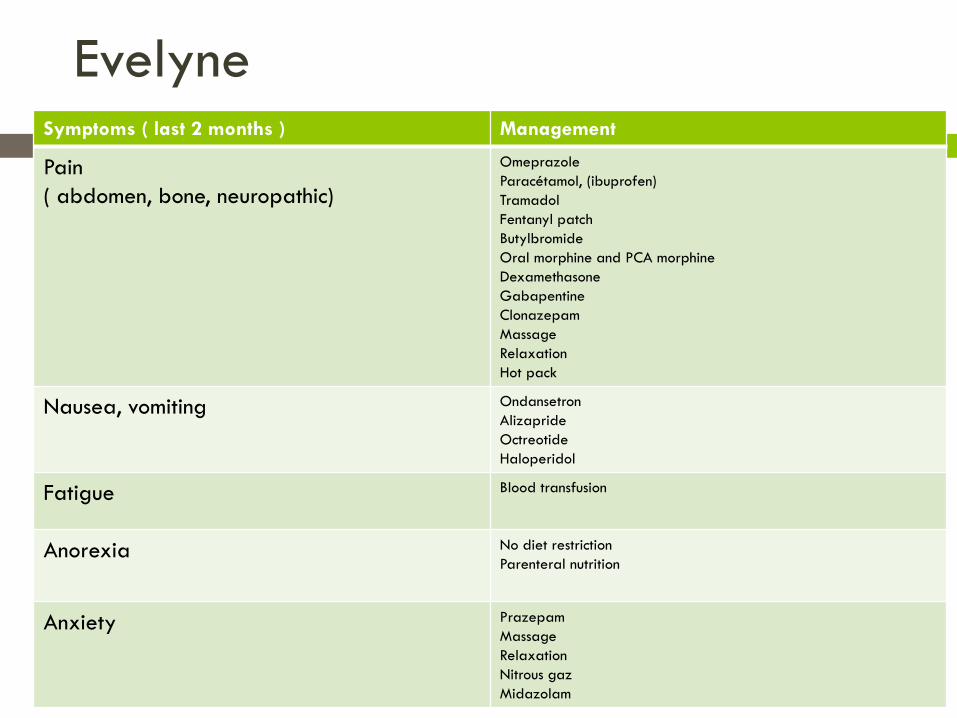
EvelyneSymptoms ( last 2 months ) Management
Pain
( abdomen, bone, neuropathic)
Omeprazole
Paracétamol, (ibuprofen)
Tramadol
Fentanyl patch
Butylbromide
Oral morphine and PCA morphine
Dexamethasone
Gabapentine
Clonazepam
Massage
Relaxation
Hot pack
Nausea, vomiting Ondansetron
Alizapride
Octreotide
Haloperidol
Fatigue Blood transfusion
Anorexia No diet restriction
Parenteral nutrition
Anxiety Prazepam
Massage
Relaxation
Nitrous gaz
Midazolam

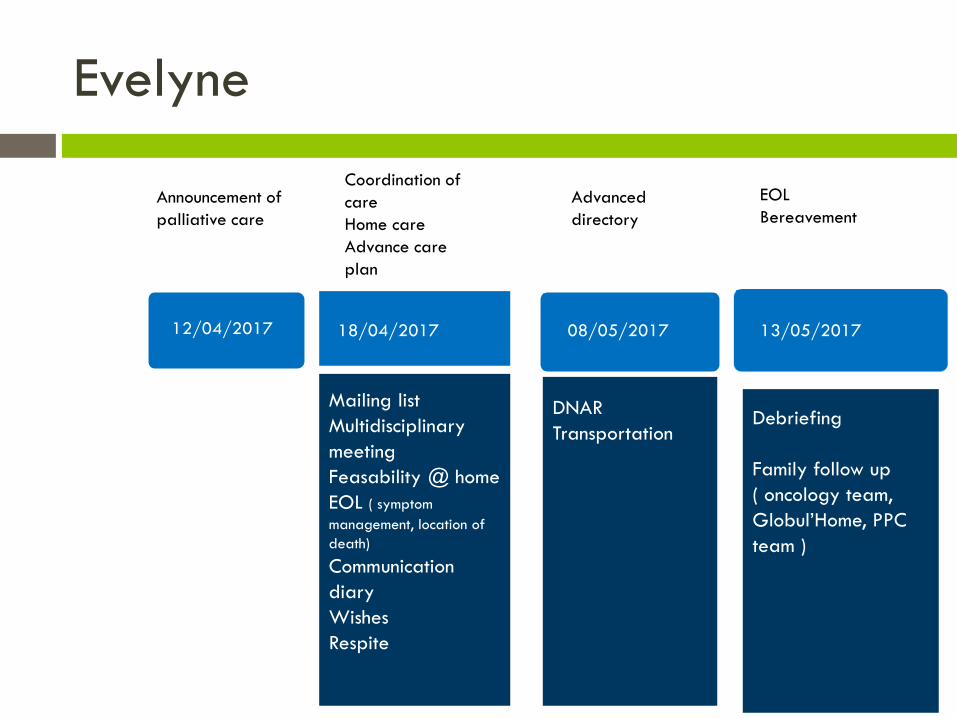
Evelyne
Announcement of
palliative care
Coordination of
care
Home care
Advance care
plan
Advanced
directory
12/04/2017 18/04/2017 08/05/2017
13/05/2017Mailing list
Multidisciplinary
meeting
Feasability @ home
EOL ( symptom
management, location of
death)
Communication
diary
Wishes
Respite
DNAR
Transportation
EOL
Bereavement
13/05/2017
Debriefing
Family follow up
( oncology team,
Globul’Home, PPC
team )
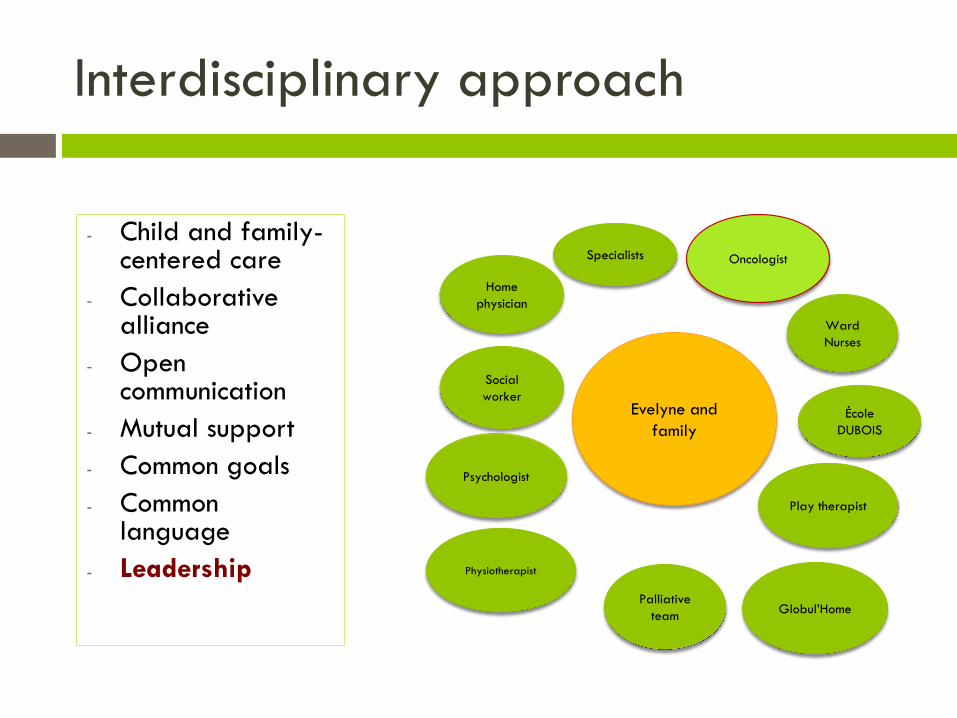
Interdisciplinary approach
- Child and family-centered care
- Collaborative alliance
- Open communication
- Mutual support
- Common goals
- Common language
- Leadership
Ward
Nurses
Oncologist
École
DUBOIS
Home
physician
Palliative
team
Social
workerEvelyne and
family
Psychologist
Specialists
Physiotherapist
Globul’Home
Play therapist
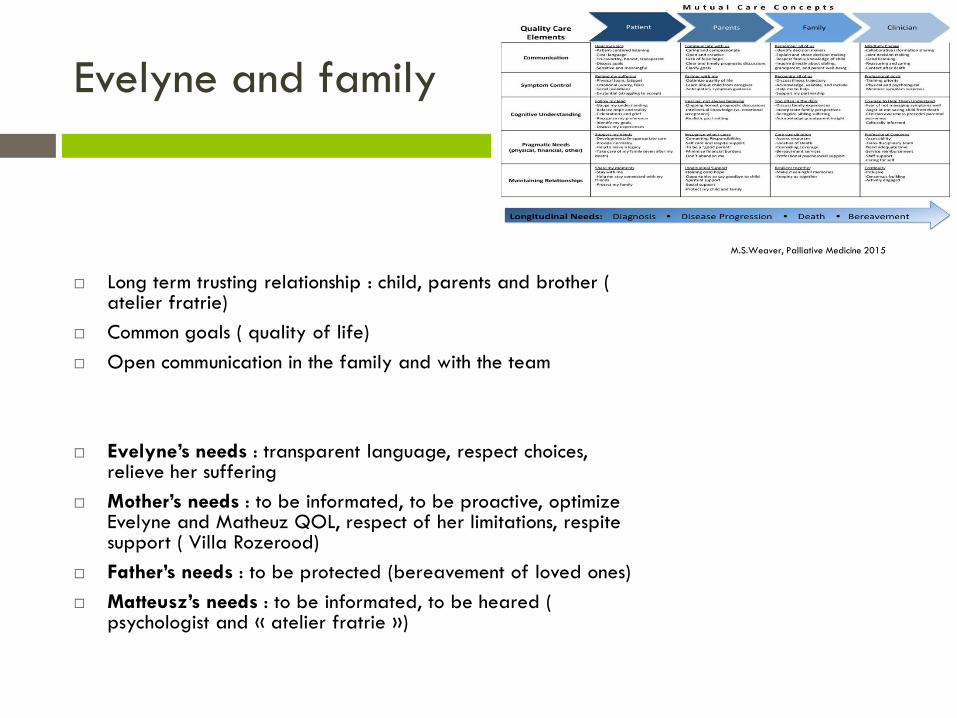
Evelyne and family
Long term trusting relationship : child, parents and brother ( atelier fratrie)
Common goals ( quality of life)
Open communication in the family and with the team
Evelyne’s needs : transparent language, respect choices, relieve her suffering
Mother’s needs : to be informated, to be proactive, optimize Evelyne and Matheuz QOL, respect of her limitations, respite support ( Villa Rozerood)
Father’s needs : to be protected (bereavement of loved ones)
Matteusz’s needs : to be informated, to be heared ( psychologist and « atelier fratrie »)
M.S.Weaver, Palliative Medicine 2015
Complex challenges
Home : demand during one weekend for her
anniversary but no anticipation (stop IV medication)
: fiasco ( pain, anxiety on behalf of everyone) and
ward admission
Villa Rozerood = success because of anticipation (
transportation,drugs, material, primary care,
continuity of care)

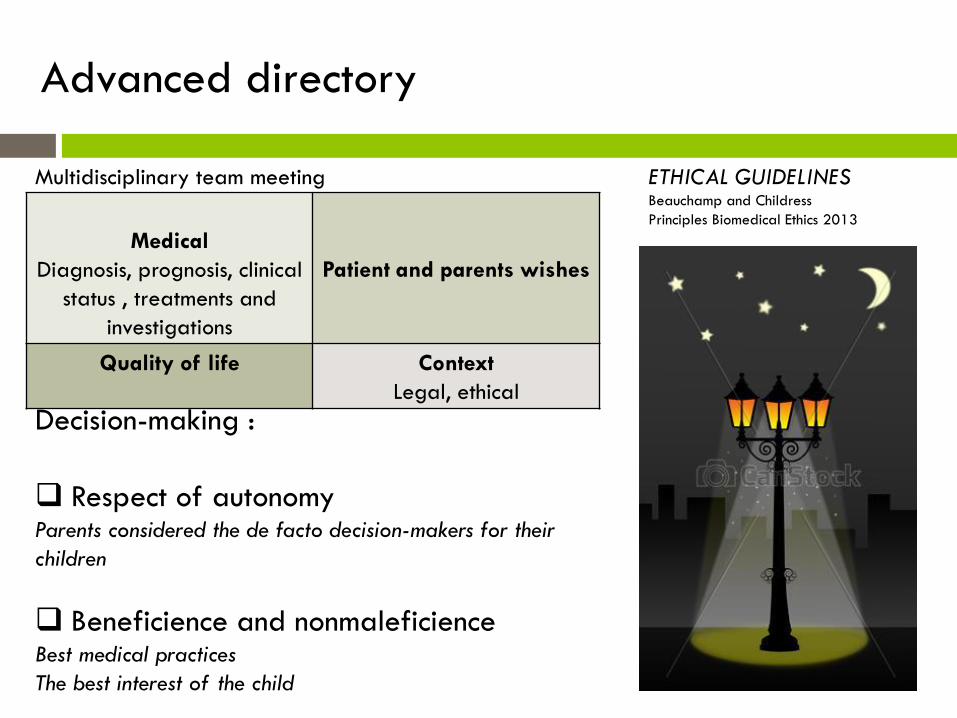
Decision-making :
Respect of autonomyParents considered the de facto decision-makers for their
children
Beneficience and nonmaleficienceBest medical practices
The best interest of the child
ETHICAL GUIDELINESBeauchamp and Childress
Principles Biomedical Ethics 2013
Advanced directory
Medical
Diagnosis, prognosis, clinical
status , treatments and
investigations
Patient and parents wishes
Quality of life Context
Legal, ethical
Multidisciplinary team meeting
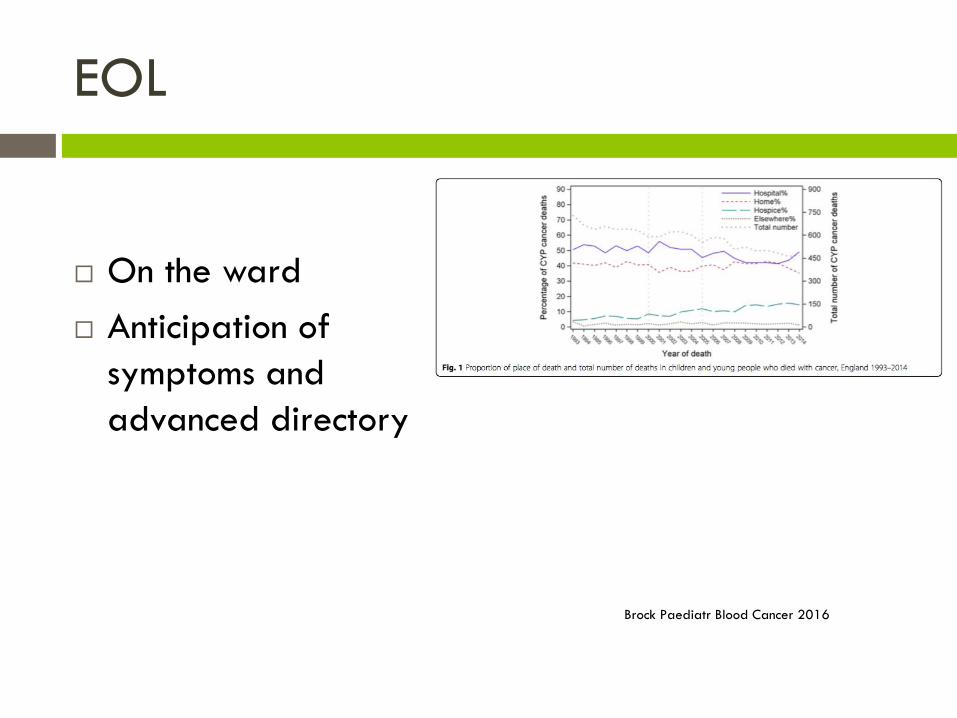
EOL
On the ward
Anticipation of
symptoms and
advanced directory
Brock Paediatr Blood Cancer 2016
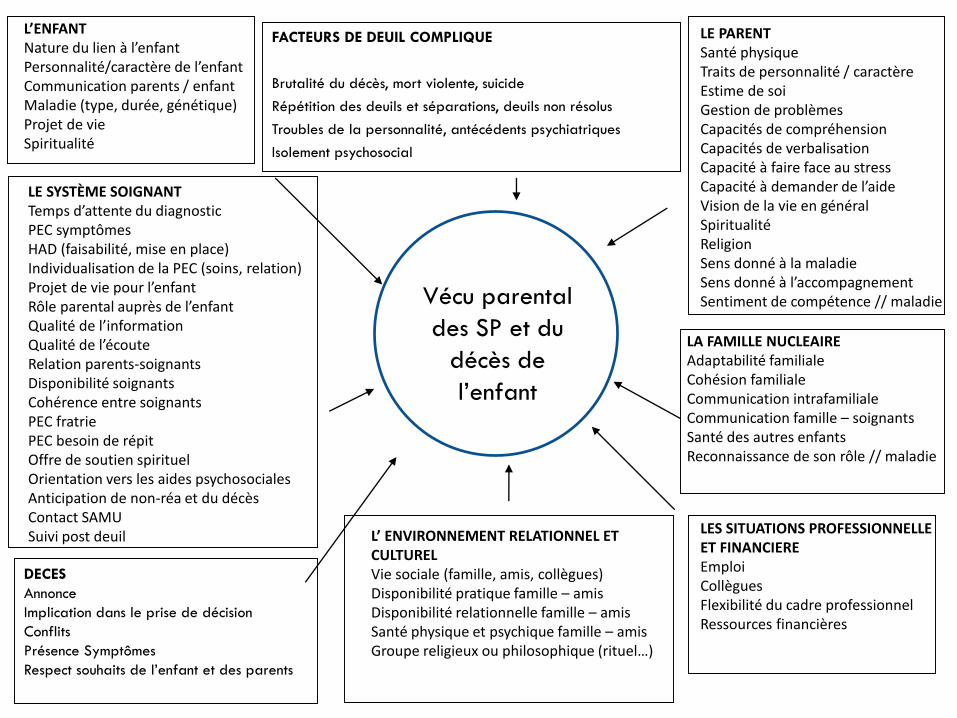
L’ENFANT Nature du lien à l’enfantPersonnalité/caractère de l’enfantCommunication parents / enfantMaladie (type, durée, génétique)Projet de vieSpiritualité
LE PARENT Santé physiqueTraits de personnalité / caractèreEstime de soiGestion de problèmesCapacités de compréhensionCapacités de verbalisationCapacité à faire face au stressCapacité à demander de l’aideVision de la vie en généralSpiritualitéReligionSens donné à la maladieSens donné à l’accompagnementSentiment de compétence // maladie
LA FAMILLE NUCLEAIRE Adaptabilité familialeCohésion familialeCommunication intrafamilialeCommunication famille – soignantsSanté des autres enfantsReconnaissance de son rôle // maladie
LES SITUATIONS PROFESSIONNELLE ET FINANCIERE EmploiCollèguesFlexibilité du cadre professionnelRessources financières
LE SYSTÈME SOIGNANT Temps d’attente du diagnostic PEC symptômesHAD (faisabilité, mise en place)Individualisation de la PEC (soins, relation)Projet de vie pour l’enfantRôle parental auprès de l’enfantQualité de l’informationQualité de l’écouteRelation parents-soignantsDisponibilité soignantsCohérence entre soignantsPEC fratriePEC besoin de répitOffre de soutien spirituelOrientation vers les aides psychosocialesAnticipation de non-réa et du décèsContact SAMUSuivi post deuil L’ ENVIRONNEMENT RELATIONNEL ET
CULTURELVie sociale (famille, amis, collègues)Disponibilité pratique famille – amisDisponibilité relationnelle famille – amisSanté physique et psychique famille – amisGroupe religieux ou philosophique (rituel…)
Vécu parental
des SP et du
décès de
l’enfant
FACTEURS DE DEUIL COMPLIQUE
Brutalité du décès, mort violente, suicide
Répétition des deuils et séparations, deuils non résolus
Troubles de la personnalité, antécédents psychiatriques
Isolement psychosocial
DECES
Annonce
Implication dans le prise de décision
Conflits
Présence Symptômes
Respect souhaits de l’enfant et des parents
Take home message
Pediatric palliative care team
Complementary
May involve second opinion regarding
• Decision making
• Symptom management
• Coordination of care
• Home care