Embed Size (px)
Citation preview
Daniel Woodward
East Tennessee State University, Year II
Mount Pleasant Manor
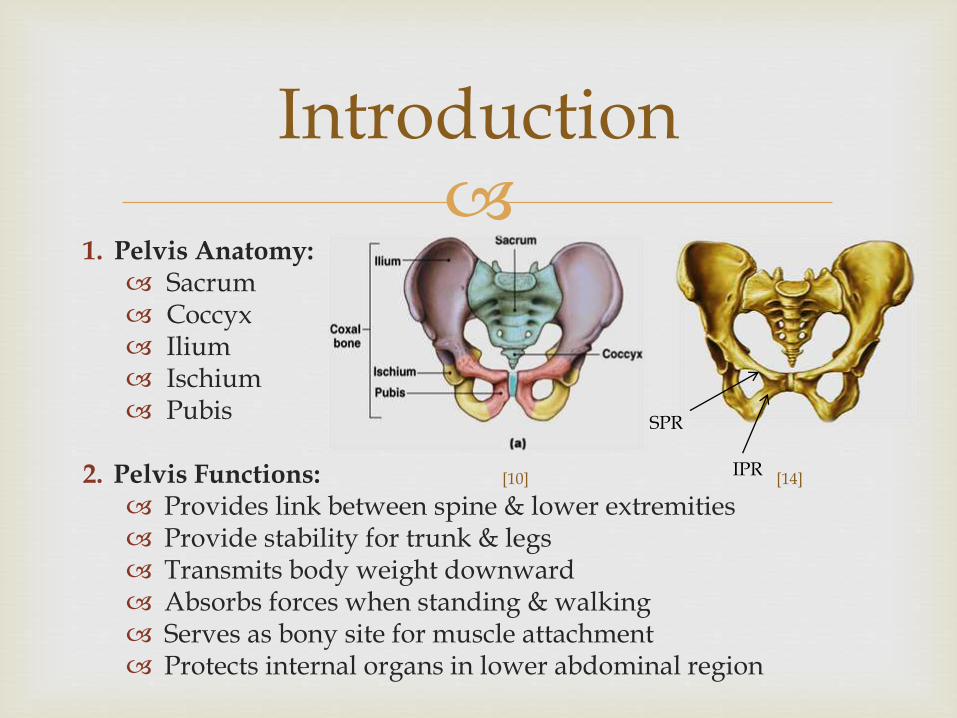
1. Pelvis Anatomy:
Sacrum Coccyx Ilium Ischium Pubis
2. Pelvis Functions: Provides link between spine & lower extremities Provide stability for trunk & legs Transmits body weight downward Absorbs forces when standing & walking Serves as bony site for muscle attachment Protects internal organs in lower abdominal region
Introduction
[10] [14]
SPR
IPR
1. Classification:
High Impact Injury vs. Low Impact Injury
Stable vs. Unstable
2. Pelvic Fractures associated with:
Increased mortality rates in the elderly
Decreased mobility & independence
Increased hospital stay
Substantial health care cost
Pelvic Ring Fractures
[2,4,11]
High Impact
Low Impact
Right Superior and Inferior Pubic Rami Fracture
1. Date of Injury: 1/08/13
2. Mechanism of Injury: Patient fell at home when walking to bathroom; legs gave way as she
fell on her bottom
3. X-Rays confirmed stable pubic rami fractures
4. Received Acute PT/OT for pain management in hospital
5. Discharged 1/15/13 from hospital to sub-acute rehab facility (Mount Pleasant Manor)
Patient Injury
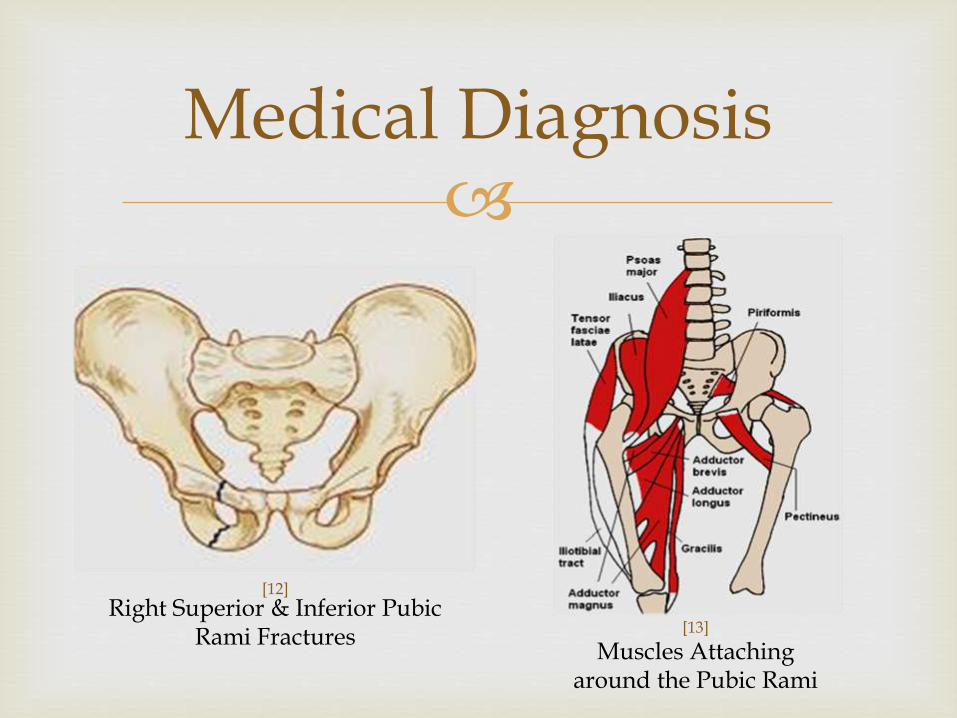
Medical Diagnosis
Right Superior & Inferior Pubic Rami Fractures [13]
Muscles Attaching around the Pubic Rami
[12]
1. Injury Classification:
Low Impact Stable
2. MOI: Trauma usually due to a simple fall (fall less than 3 feet)
3. Occurrence: Commonly occurs in the elderly (60+ years old)
4. Females > Males
5. Symptoms: Bruising, swelling, or crepitus in pubis region Pain in groin, lateral hip, or the buttock area when WB Decreased ROM/strength due to pain Decreased ability to perform SLR on affected side Antalgic gait for those who can ambulate
Epidemiology
[11]
1. Current Treatment Strategies:
Pain management, rest, maintain ROM & strength, & gait training with protected weight bearing.
2. Prognosis:
Varies depending on patient age, mental status, & overall health
Injury usually heals quickly due to large amount of soft tissue in this area.
Most healthy patients require protected weight bearing for about 6 weeks until the pain has diminished
Epidemiology
[6, 8, 11 ]
1. To examine deficits of a patient who has suffered a right superior & inferior pubic rami fracture
2. To create an effective treatment plan utilizing evidence based practice to address deficits associated with injury
Purpose Statements
1. Tinetti’s Gait & Balance Assessment Score
2. Level of Assistance Required for Functional Tasks
3. Ambulatory Distance
4. Pain Rating
Outcome Measures
1. Medical History:
75 year old female
Severe osteoporosis with multiple fractures
Right TSR, Left RCT repair
Right THA, Left THA with 2 revisions (15 years ago)
Apparent & True Leg length discrepancy
April 2012 – Fracture of Left femur/patella due to fall
Most Recent: (R) superior & inferior pubic rami fracture (stable) & 4th finger fracture due to fall
The Patient
2. Medial History Continued:
Depression
History of Hypertension
Multiple Bowel Resections; residual spastic colon
Peptic Ulcer Disease
Chronic diarrhea
Inguinal hernia repair
Bilateral Cataract Surgeries
FALL RISK!
The Patient
3. Family History: (+) for cancer in her brother
Sister has peripheral artery disease
Father had diabetes
Mother had congestive heart failure
4. Social History: Smoked ~ 1 pack per day for more than 50 years
Does not drink alcohol or abuse any drugs
Manages well on her own with her ADL’s
The Patient
5. Medications and POSSIBLE side effects
Imodium: Dizziness and drowsiness
Temazepam: Day time drowsiness, muscle weakness, lack of balance or coordination.
Vilazodone: Dizziness, fatigue, feeling jittery
Losartan: Dizziness, drowsiness, confusion
Omeprazole: Dizziness, confusion, feeling jittery, weakness
KCl: Confusion, anxiety, muscle weakness
OxyContin: Drowsiness, dizziness
Lortab: Anxiety, dizziness, drowsiness, blurred vision.
The Patient
6. Occupation:
Retired
7. Living Situation: Lives with sister; 9 steps to enter home
8. Prior level of function: Ambulated at home without assistive device
9. Precautions: WBAT on Right Lower Extremity Full Code
The Patient
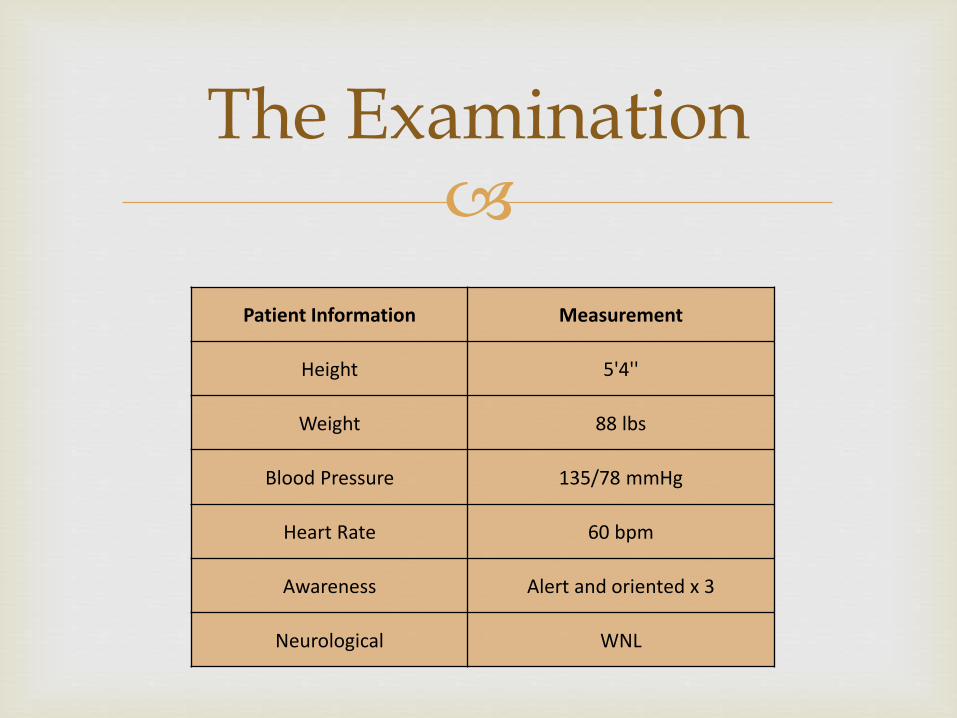
Patient Information Measurement
Height 5'4''
Weight 88 lbs
Blood Pressure 135/78 mmHg
Heart Rate 60 bpm
Awareness Alert and oriented x 3
Neurological WNL
The Examination
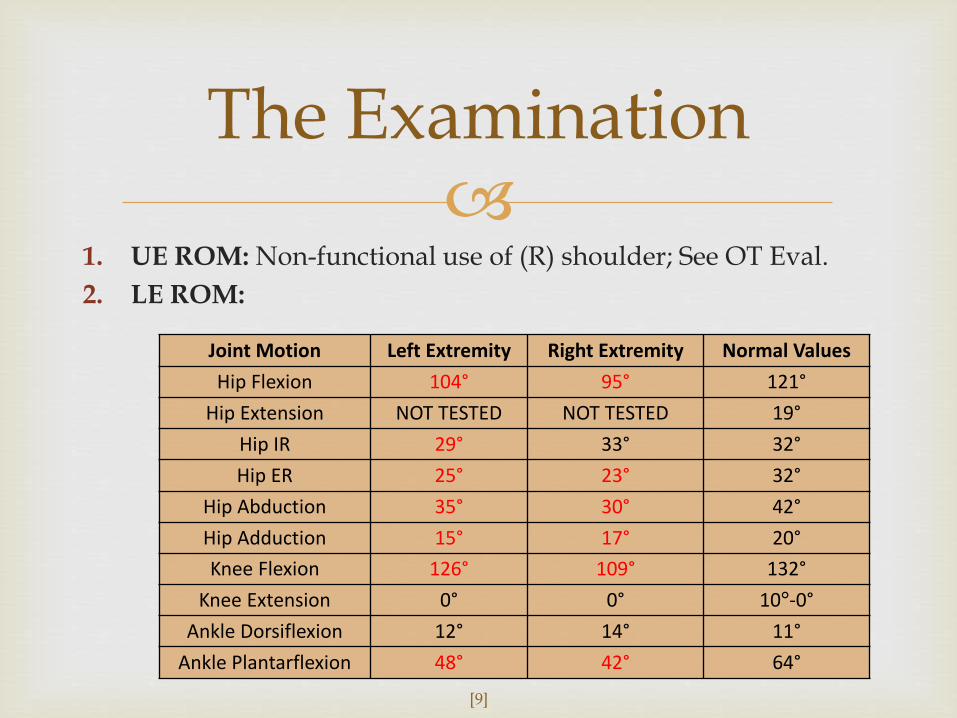
1. UE ROM: Non-functional use of (R) shoulder; See OT Eval.
2. LE ROM:
The Examination
Joint Motion Left Extremity Right Extremity Normal Values
Hip Flexion 104° 95° 121°
Hip Extension NOT TESTED NOT TESTED 19°
Hip IR 29° 33° 32°
Hip ER 25° 23° 32°
Hip Abduction 35° 30° 42°
Hip Adduction 15° 17° 20°
Knee Flexion 126° 109° 132°
Knee Extension 0° 0° 10°-0°
Ankle Dorsiflexion 12° 14° 11°
Ankle Plantarflexion 48° 42° 64°
[9]
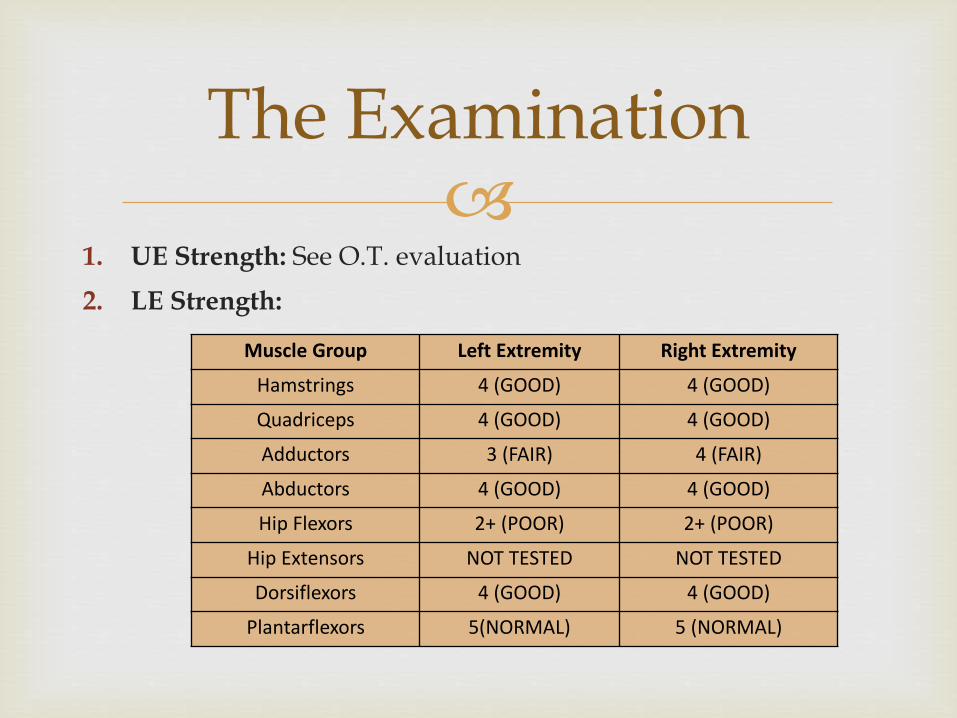
1. UE Strength: See O.T. evaluation
2. LE Strength:
The Examination
Muscle Group Left Extremity Right Extremity
Hamstrings 4 (GOOD) 4 (GOOD)
Quadriceps 4 (GOOD) 4 (GOOD)
Adductors 3 (FAIR) 4 (FAIR)
Abductors 4 (GOOD) 4 (GOOD)
Hip Flexors 2+ (POOR) 2+ (POOR)
Hip Extensors NOT TESTED NOT TESTED
Dorsiflexors 4 (GOOD) 4 (GOOD)
Plantarflexors 5(NORMAL) 5 (NORMAL)
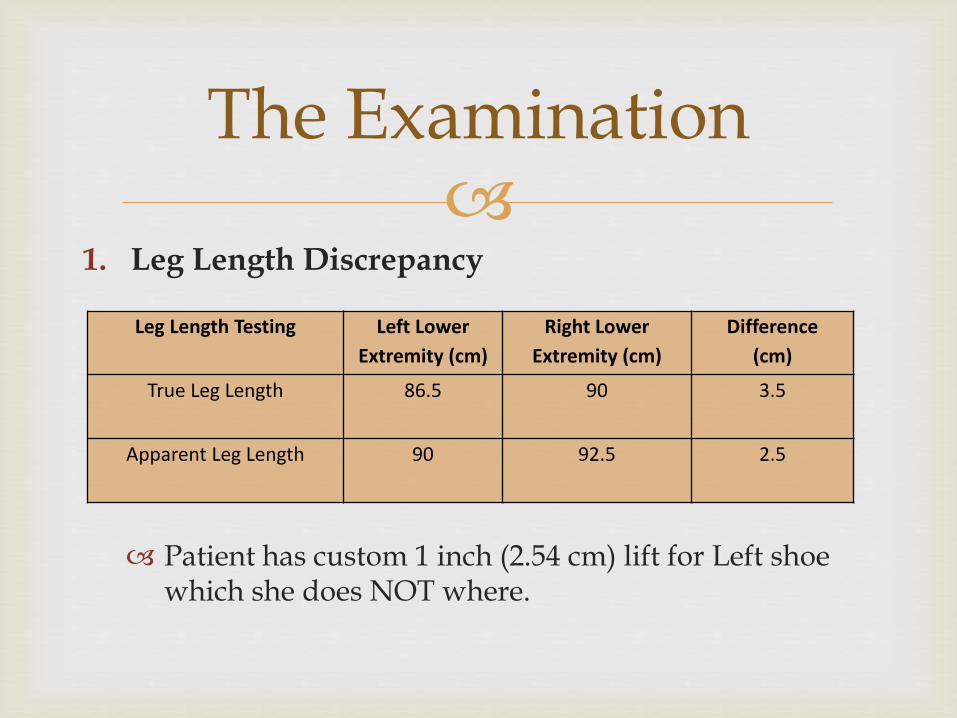
1. Leg Length Discrepancy
Patient has custom 1 inch (2.54 cm) lift for Left shoe which she does NOT where.
The Examination
Leg Length Testing Left Lower
Extremity (cm)
Right Lower
Extremity (cm)
Difference
(cm)
True Leg Length 86.5 90 3.5
Apparent Leg Length 90 92.5 2.5
The Examination
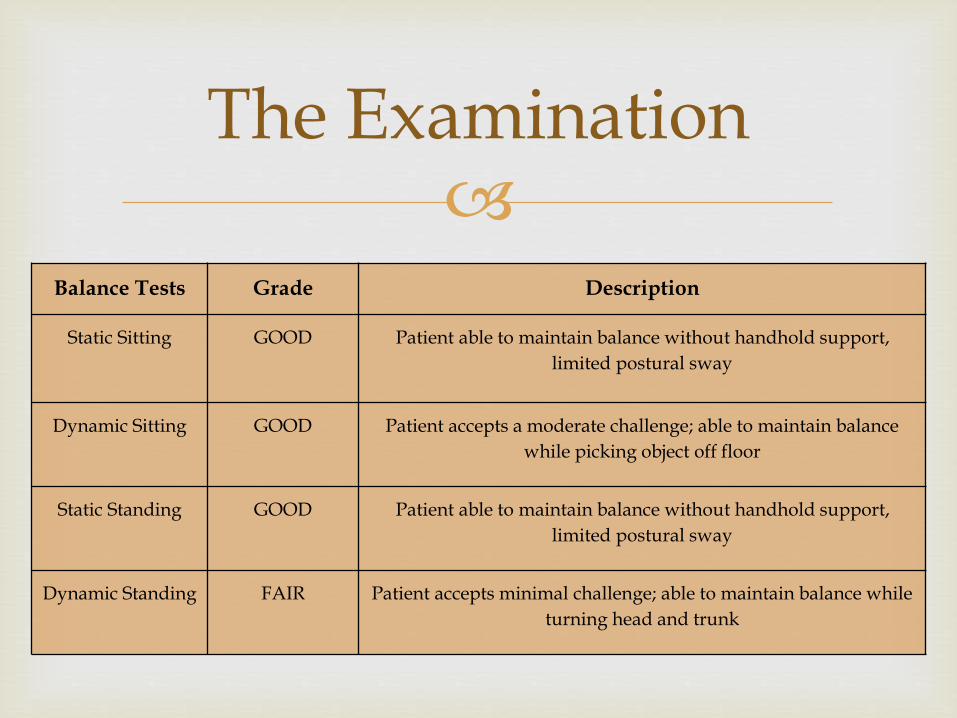
Balance Tests Grade Description
Static Sitting GOOD Patient able to maintain balance without handhold support,
limited postural sway
Dynamic Sitting GOOD Patient accepts a moderate challenge; able to maintain balance
while picking object off floor
Static Standing GOOD Patient able to maintain balance without handhold support,
limited postural sway
Dynamic Standing FAIR Patient accepts minimal challenge; able to maintain balance while
turning head and trunk
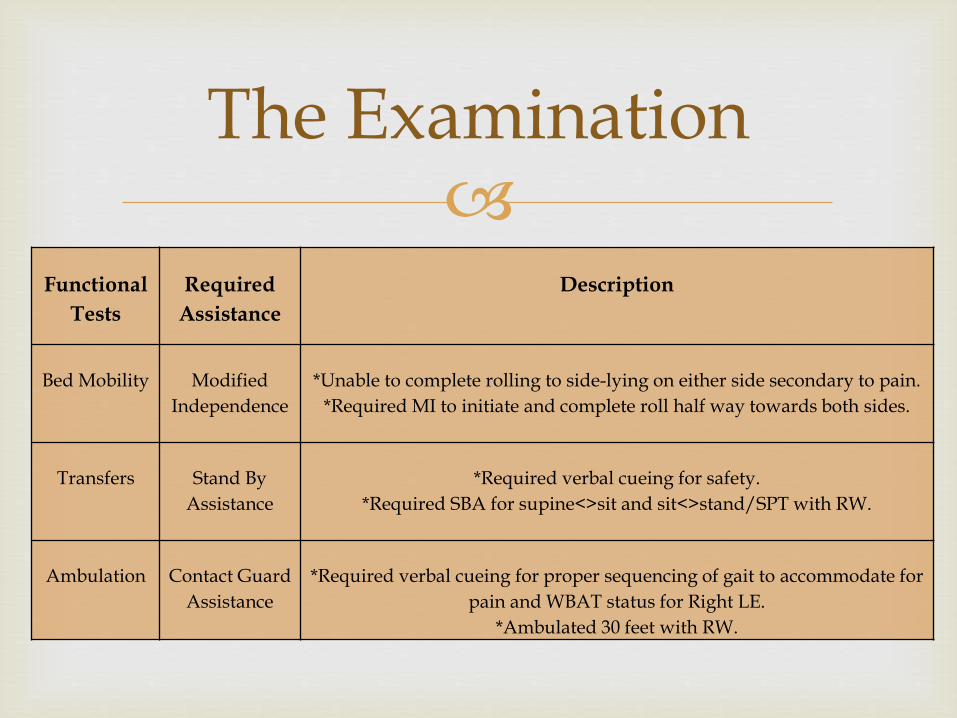
Functional
Tests
Required
Assistance
Description
Bed Mobility Modified
Independence
*Unable to complete rolling to side-lying on either side secondary to pain.
*Required MI to initiate and complete roll half way towards both sides.
Transfers Stand By
Assistance
*Required verbal cueing for safety.
*Required SBA for supine<>sit and sit<>stand/SPT with RW.
Ambulation Contact Guard
Assistance
*Required verbal cueing for proper sequencing of gait to accommodate for
pain and WBAT status for Right LE.
*Ambulated 30 feet with RW.
The Examination
1. Tinetti’s Balance Assessment Tool:
Measures patient’s gait & balance Scoring: Ordinal scale ranging from 0 – 2
0 = most impairment 2 = independence of the patient Three measures: Gait assessment score, overall balance assessment
score, and gait & balance score Total Balance Score = 16 Total Gait Score = 12 Total Test Score = 28
2. Interpretation: 25 – 28 = Low Fall Risk 19 – 24 = Medium Fall Risk < 19 = High Fall Risk
The Examination
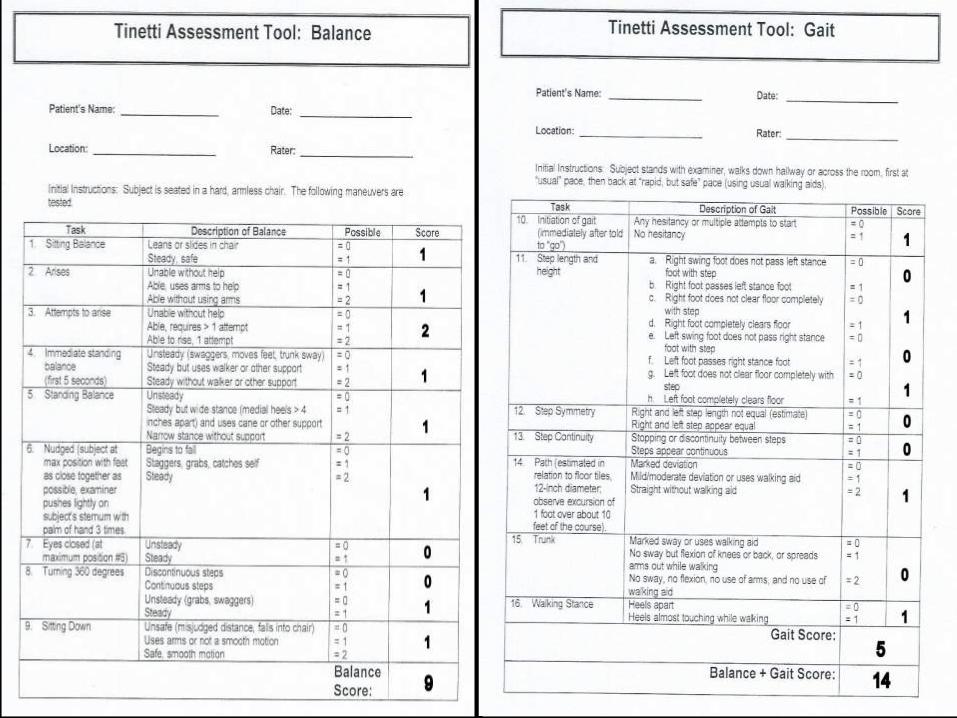
1. Tinetti’s Score = 14
Patient is a HIGH FALL RISK!
2. Pain = 7 / 10
Pain Description:
Pain in legs, lower back, pubic region. Pain increased with SLR, when turned onto side, or in WB; especially painful on (R) LE in hip & pubic region.
The Examination
1. Achieves ¾ side-lying to either side using bed rails & without
pain
2. Modified Independent Transfers Supine <> Sit Sit <> Stand/SPT with a RW
3. Modified Independent > SBA for ambulating with a RW up to 60’
4. GOOD dynamic standing balance
5. Tinetti’s score of 16
Short Term Goals
These goals changed from week to week as patient progressed

1. Independent Bed Mobility
2. Independent to modified independent Transfers Supine <> Sit <> Stand/SPT with RW
3. Modified Independent Ambulation up to 150’ with RW
4. Able to Ascend/Descend 9 steps
5. Final Tinetti’s minimal score of 19
Long Term Goals
1. Physical Therapy: 5x/week x 4 weeks
Safety & Moderate Independence with all of the following:
Demonstrate Functional LE ROM
Demonstrate Functional LE Strength
Demonstrate Functional Bed Mobility
Demonstrate Functional Transfers
Demonstrate Functional Gait
Be able to ascend and descend 9 steps
2. Discharge Plan Mount Pleasant Manor Home
Plan of Care
1. Cryotherapy5
Research confirms that cryotherapy results in: Decreased inflammation Decreased blood flow Reduced swelling Reduced pain
2. Nustep7
Research supporting this exercise suggests that it: Decreases blood pressure Increases strength Increases walking speed
Evidence Based Practice
3. Prophylactic Measures11
Range of Motion
Strength
Prevent Immobility
4. Standing Activities/Ambulation1
Research suggests that weight bearing activities are effective in preserving or even increasing bone mass.
Ambulation should be encouraged!
Evidence Based Practice
1. Warm Up
Nustep 15 minutes at Level 1
2. LE ROM Heel slides for hip flexion, hip abduction, & hip adduction; 3 sets of 10
3. LE Strengthening Knee extension (quads), bridging (gluts), knee raises (hip flexors); 3 sets of
10
4. Bed Mobility Worked on rolling from side to side using modified independence
5. Transfer Training Practiced sit<>stand/SPT & sit<>supine using modified independence
6. Cryotherapy Ice pack x 15 minutes to control pain
Initial Treatment Plan
1. Modified 3-point Gait Pattern while using
walker.
2. Importance of using assistive device during gait/transfers at all times
3. Importance of wearing proper shoes with custom lift for left shoe
4. Pain Rating Scale
Patient Education
Pain Scale Interpretation
1. Initial Rating = 7 (Very Intense):
Pain completely dominates your senses, causing you to think unclearly about half the time. At this point you are effectively disabled and frequently cannot live alone. Comparable to an average migraine headache
2. After Education = 4 (Distressing):
Strong, deep pain, like an average toothache, the initial pain from a bee sting, or minor trauma to part of the body, such as stubbing your toe real hard. So strong you notice the pain all the time and cannot completely adapt.

1. Warm Up:
Nustep 20 minutes at Level 1
2. LE Strengthening and ROM Exercises: Heel slides for hip flexion, abduction, adduction Knee extension (quads), bridging (gluts); 3 sets of 10
3. Gait Training: CGA ambulation 30’ x 2 with a rolling walker, breaks, & a more continuous
and symmetrical gait Knee raises over small hurdles while ambulating in parallel bars (hip
flexors)
4. Step Exercise: CGA stepping exercise on to 2 ½ inch step while in parallel bars ; 3 sets of 10 Leading with both LE’s
Treatment Progression 1
Step Exercise
1. Warm Up:
Nustep 20 minutes at Level 1
2. LE Strengthening Exercises:
Knee extension (quads); 3 sets of 10
3. Gait Training
SBA Ambulation 75’ x 2
4. Dynamic Standing Balance Activities
Tic-Tac-Toe Toss in standing
Balloon Volleyball in standing
5. Step Exercise:
CGA stepping exercise on to 4 inch step while in parallel bars ; 3 sets of 10
Leading with both LE’s
Treatment Progression 2
Tic-Tac-Toe Toss Balloon Volleyball
1. After three weeks, patient demonstrated sufficient
safety, endurance, and strength with all transfers and ambulation
2. In order to continue the progression towards further independence, the W/C was discharged
3. Patient was educated on current status & was asked to use supervision when ambulating away from her hall
W/C Discharge

1. Warm Up:
Nustep 20 minutes at Level 1
2. Gait Training:
MI ambulation 150’ x 2 with a rolling walker
3. Standing Balance Activities
Balloon Volleyball in standing
Kicking ball activity with Right LE
4. Step Exercise:
CGA stepping exercise on to 6 inch step on therapy stair set ; 3 sets of 10
Leading with both LE’s
Treatment Progression 3
Single Leg Stance Activity
1. Warm Up:
Nustep 20 minutes at Level 1
2. Gait Training:
MI ambulation 150’ x 2 with a rolling walker
3. Standing Balance Activities
Balloon Volleyball in standing
Kicking ball activity with Right LE
4. Step Exercise:
CGA ascending with the Left LE and descending leading with the Right LE 4 steps 3x
Also worked on ascending/descending steps sideways to simulate home environment.
Final Treatment
Therapy Steps
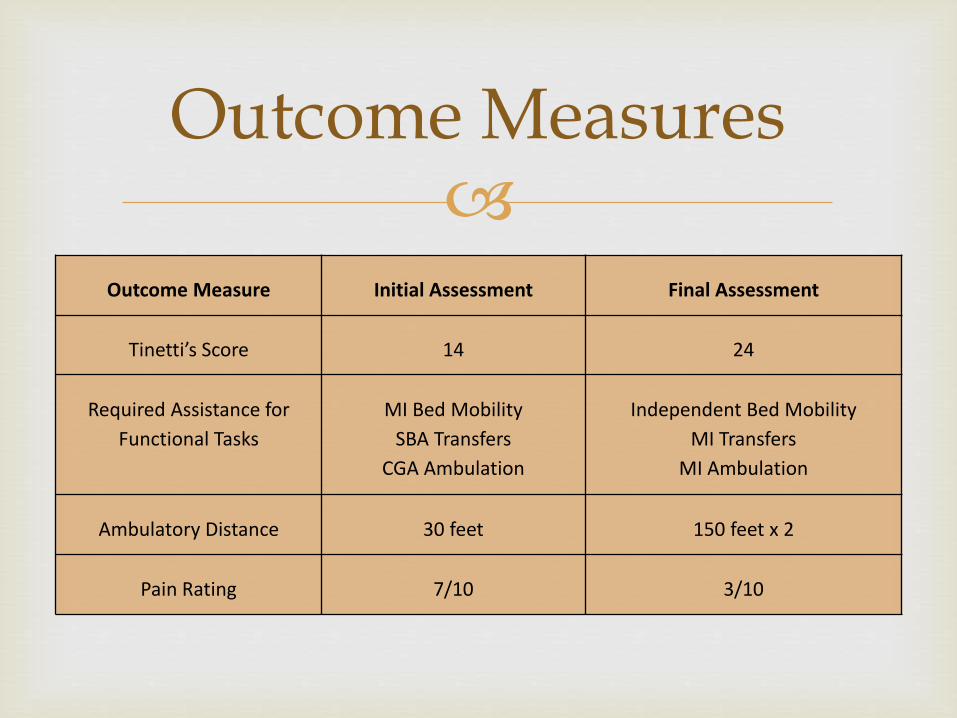
Outcome Measures
Outcome Measure Initial Assessment Final Assessment
Tinetti’s Score 14 24
Required Assistance for
Functional Tasks
MI Bed Mobility
SBA Transfers
CGA Ambulation
Independent Bed Mobility
MI Transfers
MI Ambulation
Ambulatory Distance 30 feet 150 feet x 2
Pain Rating 7/10 3/10
1. Wii Therapy (Balance/Decreased Fall Risk)3
Research shows that six 1 hour sessions of Wii bowling simulation significantly improved Berg Balance, DGI, and TUG scores for an 89 year old female
Alternative Treatment
1. Aisenbrey, Jeannie A. "Exercise in the Prevention and Management of Osteoporosis." Journal of the American Physical
Therapy Association 67.7 (1987): 1100-104. PubMed. Web. 18 Mar. 2013. <http://www.physther.org/content/67/7/1100.full.pdf+html>.
2. Boufous, Soufiane, Caroline Finch, Stephen Lord, and Jacqueline Close. "The Increasing Burden of Pelvic Fractures in Older People, New South Wales, Australia." Injury 36.11 (2005): 1323-329. PubMed. Web. 12 Mar. 2013. <http://www.sciencedirect.com.ezproxy.etsu.edu:2048/science/article/pii/S0020138305000495>.
3. Clark, Robert, and Theresa Kraema. "Clinical Use of Nintendo Wii(TM) Bowling Simulation to Decrease Fall Risk in an Elderly Resident of a Nursing Home: A Case Report." Journal of Geriatric Physical Therapy 32.4 (2009): 174-80. Ebscohost. Web. 10 Apr. 2013. <http://search.proquest.com.ezproxy.etsu.edu:2048/docview/736484473?accountid=10771>.
4. Dodge, Greg, and Rob Brison. "Low-impact Pelvic Fractures in the Emergency Department." Canadian Journal of Emergency Medicine 12.6 (2010): 509-13. PubMed. Web. 12 Mar. 2013. <http://www.cjem-online.ca/v12/n6/p509>.
5. Greenstein, Gary. "Therapeutic Efficacy of Cold Therapy After Intraoral Surgical Procedures: A Literature Review." Journal of Periodontology 78.5 (2007): 790-800. PubMed. Web. 12 March 2013. <http://www.joponline.org/doi/pdf/10.1902/jop.2007.060319>.
6. Hill, R., C. M. Robinson, and J. F. Keating. "Fractures of the Pubic Rami: Epidemiology and Five-year Survival." The Journal of Bone and Joint Surgery 83-B.8 (2013): 1141-144. Google Scholar. Web. 12 Mar. 2013. <http://www.bjj.boneandjoint.org.uk/content/83-B/8/1141.full.pdf+html>.
7. Johnson, Timothy, Scott McPhee, and Mary Dietrich. "Effects of Recumbent Stepper Exercise on Blood Pressure, Strength and Mobility in Residents of Assisted Living Communities: A Pilot Study." Physical & Occupational Therapy In Geriatrics 21.2 (2002): 27-40. Google Scholar. Web. 12 Mar. 2013. <http://informahealthcare.com/doi/abs/10.1080/J148v21n02_03>.
References
8. Krappinger, Dietmar, Peter Struve, Rene Schmid, Jakob Kroesslhuber, and Michael Blauth. "Fractures of the Pubic
Rami: A Retrospective Review of 534 Cases." Archives of Orthopaedic and Trauma Surgery 129.12 (2009): 1685-690. PubMed. Web. 12 Mar. 2013. <http://link.springer.com/article/10.1007%2Fs00402-009-0942-5?LI=true>.
9. Norkin, Cynthia C., and D. Joyce. White. "Normative Range of Motion Values." Measurement of Joint Motion: A Guide to Goniometry. 4th ed. Philadelphia: F.A. Davis, 2009. 427-28. Print.
10. O'Connor, Shaun. "STUDYBLUE", n.d. Web. 13 Mar. 2013. <http://www.studyblue.com/notes/note/n/chapter-8-appendicular-skeleton-lecture/deck/4262031>
11. Sarwark, John F. "Fracture of the Pelvis." Essentials of Musculoskeletal Care. 4th ed. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2010. 558-61. Print.
12. Vivere, Amare, Ridere: Pubic Ramus Fracture in the Distance Runner." Vivere, Amare, Ridere: Pubic Ramus Fracture in the Distance Runner. N.p., n.d. Web. 13 Mar. 2013. <http://gazelle74.blogspot.com/2012/05/pubic-ramus-fracture-in-distance-runner.html>.
13. Where Is the Pubic Rami?" Where Is the Pubic Rami? InnovateUs Inc, n.d. Web. 13 Mar. 2013. <http://www.innovateus.net/innopedia/where-pubic-rami>.
14. "Why Pelvis In Men and Women Different Size and Shape?" Nanda Books. N.p., 2010. Web. 13 Apr. 2013. <http://nandabooks.blogspot.com/2012/11/why-pelvis-in-men-and-women-different.html>.
References





























