Embed Size (px)
Citation preview

Zurich Open Repository andArchiveUniversity of ZurichMain LibraryStrickhofstrasse 39CH-8057 Zurichwww.zora.uzh.ch
Year: 2011
Clinical evaluation of cochlear implant sound coding taking into accountconjectural masking functions, MP3000™
Buechner, A; Beynon, A; Szyfter, W; Niemczyk, K; Hoppe, U; Hey, M; Brokx, J; Eyles, J; Van deHeyning, P; Paludetti, G; Zarowski, A; Quaranta, Q; Wesarg, T; Festen, J; Olze, H; Dhooge, I;
Müller-Deile, J; Ramos, A; Roman, S; Piron, J P; Cuda, D; Burdo, S; Grolman, W; Roux Vaillard, S;Huarte, A; Frachet, B; Morera, C; Garcia-Ibáñez, L; Abels, D; Walger, M; Müller-Mazotta, J; Antonio
Leone, C; Meyer, B; Dillier, N; Steffens, T; Gentine, A; Mazzoli, M; Rypkema, G; Killian, M;Smoorenburg, G
Abstract: Efficacy of the SPEAK and ACE coding strategies was compared with that of a new strategy,MP3000™, by 37 European implant centers including 221 subjects. The SPEAK and ACE strategies arebased on selection of 8–10 spectral components with the highest levels, while MP3000 is based on theselection of only 4–6 components, with the highest levels relative to an estimate of the spread of masking.The pulse rate per component was fixed. No significant difference was found for the speech scores andfor coding preference between the SPEAK/ACE and MP3000 strategies. Battery life was 24% longer forthe MP3000 strategy. With MP3000 the best results were found for a selection of six components. Inaddition, the best results were found for a masking function with a low-frequency slope of 50 dB/Bark anda high-frequency slope of 37 dB/Bark (50/37) as compared to the other combinations examined of 40/30and 20/15 dB/ Bark. The best results found for the steepest slopes do not seem to agree with currentestimates of the spread of masking in electrical stimulation. Future research might reveal if performancewith respect to SPEAK/ACE can be enhanced by increasing the number of channels in MP3000 beyond4–6 and it should shed more light on the optimum steepness of the slopes of the masking functions appliedin MP3000.
DOI: https://doi.org/10.1179/1754762811Y0000000009
Posted at the Zurich Open Repository and Archive, University of ZurichZORA URL: https://doi.org/10.5167/uzh-53839Journal ArticlePublished Version
Originally published at:Buechner, A; Beynon, A; Szyfter, W; Niemczyk, K; Hoppe, U; Hey, M; Brokx, J; Eyles, J; Van deHeyning, P; Paludetti, G; Zarowski, A; Quaranta, Q; Wesarg, T; Festen, J; Olze, H; Dhooge, I; Müller-Deile, J; Ramos, A; Roman, S; Piron, J P; Cuda, D; Burdo, S; Grolman, W; Roux Vaillard, S; Huarte,A; Frachet, B; Morera, C; Garcia-Ibáñez, L; Abels, D; Walger, M; Müller-Mazotta, J; Antonio Leone,C; Meyer, B; Dillier, N; Steffens, T; Gentine, A; Mazzoli, M; Rypkema, G; Killian, M; Smoorenburg, G(2011). Clinical evaluation of cochlear implant sound coding taking into account conjectural maskingfunctions, MP3000™. Cochlear Implants International, 12(4):194-204.DOI: https://doi.org/10.1179/1754762811Y0000000009
Clinical evaluation of cochlear implant soundcoding taking into account conjecturalmasking functions, MP3000™Andreas Buechner1, Andy Beynon2, Witold Szyfter3, Kazimierz Niemczyk4,Ulrich Hoppe5, Matthias Hey6, Jan Brokx7, Julie Eyles8, Paul Van de Heyning9,Gaetano Paludetti10, Andrzej Zarowski11, Nicola Quaranta12, Thomas Wesarg13,Joost Festen14, Heidi Olze15, Ingeborg Dhooge16, Joachim Müller-Deile17,Angel Ramos18, Stephane Roman19, Jean-Pierre Piron20, Domenico Cuda21,Sandro Burdo22, Wilko Grolman23, Samantha Roux Vaillard24, Alicia Huarte25,Bruno Frachet26, Constantine Morera27, Luis Garcia-Ibáñez28, Daniel Abels29,Martin Walger30, Jochen Müller-Mazotta31, Carlo Antonio Leone32,Bernard Meyer33, Norbert Dillier34, Thomas Steffens35, André Gentine36,Manuela Mazzoli37, Gerben Rypkema38, Matthijs Killian39,Guido Smoorenburg40
1Medizinische Hochschule Hannover (MHH), Carl-Neuberg-Str. 1, 30625 Hannover, Germany, 2UMC st.Radboud Nijmegen, Postbus 9101, 6500 HB Nijmegen, The Netherlands, 3Department of OtolaryngologyPoznan University of Medical Sciences, ul. Przybyszewskiego 49, Poznan, Poland, 4Department ofOtolaryngology, Medical University of Warsaw, ul. Banacha 1a, Warszawa, Poland, 5UniversitätsklinikumErlangen, Hals-Nasen-Ohren-Klinik, Waldstraße 1, Erlangen, Germany, 6St. Salvator Krankenhaus, HNO-Klinik,Gleimstrasse 5, 38820 Halberstadt, Germany, 7Academisch Ziekenhuis Maastricht, P. Debyelaan 25, 6202 AZMaastricht, The Netherlands, 8SOECIC, Institute of Sound and Vibration Research, University of Southampton,SO17 1BJ Southampton, United Kingdom, 9Universitair Ziekenhuis Antwerpen, Wilrijkstraat 10, 2650 Edegem,Belgium, 10Istituto di Clinica Otorinolaringoiatrica, Policlinico Universitario “Agostino Gemelli”, L.go A.Gemelli, 8, 00168 Roma, Italy, 11Medisch Instituut St. Augustinus, Oosterveldlaan 24, 2610 Wilrijk, Belgium,12Ospedale Policlinico Consorziale, P.zza G. Cesare, 11, 70124 Bari, Italy, 13Klinikum der Albert-Ludwigs-Universitaet, Universitaetsklinik fuer Hals-, Nasen- und Ohrenheilkunde und Poliklinik, Killianstrasse 5, 79106Freiburg, Germany, 14VUMC Amsterdam, De Boelelaan 1117, 1007 MB Amsterdam, The Netherlands, 15CharitèCampus Virchow Klinikum, HNO Klinik und Poliklinik, Augustenburger Platz 1, Berlin, Germany, 16Universitairziekenhuis Gent, De Pintelaan 185, 9000 Gent, Belgium, 17Universitätsklinikum Schleswig-Holstein, Klinik fuerHals-, Nasen, Ohrenheilkunde, Kopf- und Halschirurgie, Arnold-Heller-Strasse 14, 24105 Kiel, Germany,18Hospital Insular de Gran Canaria/Materno Infantil, Servicio de Audiologia, Avda.Maritima del Sur, S/N 35016Las Palmas de Gran Canaria, Spain, 19CHU La Timone Children Hospital, Rue Saint Pierre 264, 13385 MarseilleCedex 5, France, 20Hôpital Gui de Chauliac, Service ORL, 80, avenue Augustin, Fliche 34295 Montpellier Cedex5, France, 21Ospedale Guglielmo da Saliceto, Via Taverna 49, 29100 Piacenza, Italy, 22Ospedale di Circolo eFondazione Macchi, Viale Luigi Borri 57, 21100 Varese, Italy, 23AMC Amsterdam, Meibergdreef 9, 1105 AZAmsterdam, The Netherlands, 24CHU Angers, 4 rue Larrey, 49033 Angers, France, 25Clinica Universitaria deNavarra, Avda. Pío XII 36, 31008 Pamplona, Spain, 26Hôpital Avicenne, Service ORL, 125 route de Stalingrad,Bobigny Cédex, France, 27Servicio de Otorrinolaringologia University Hospital “La Fe” of Valencia, Avda.Campanar, 21, 46009 Valencia, Spain, 28Otology Institute García-Ibáñez, Dr. Roux 91, 8017 Barcelona, Spain,29Uniklinik und Poliklinik fuer HNO-Krankheiten, Petersgraben 4, 4031 Basel, Switzerland, 30HNO-Universitätsklinik Köln, Audiologie und Pädaudiologie, Kerpenerstr.62, Köln, Germany, 31Philipps-UniversitätMarburg, Klinik u. Poliklinik f. HNO-Heilkunde, Deutschhausstraße 3, 35037 Marburg, Germany, 32U.O.C. diO.R.L, A.O. Monaldi - Napoli, Azienda di Rilievo Nazionale e di Alta Specializzazione, Via L. Bianchi, 80131Napoli, Italy, 33Hôpital Saint Antoine, 184 rue du faubourg Saint Antoine, 75012 Paris, France,
Correspondence to: G Smoorenburg. Email: [email protected]
© W.S. Maney & Son Ltd 2011MORE OpenChoice articles are open access and distributed under the terms of the Creative Commons Attribution License 3.0DOI 10.1179/1754762811Y0000000009 Cochlear Implants International 2011 VOL. 12 NO. 4194
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited

34Universitätsspital, ORL Klinik, Frauenklinikstrs 24, 8091 Zuerich, Switzerland, 35UniversitätsklinikumRegensburg, HNO-Klinik, Franz-Josef-Strauß-Allee 11, 93053 Regensburg, Germany, 36Hôpital Hautepierre,Service ORL, Avenue Molière, 67098 Strasbourg Cedex, France, 37Azienda ospedaliera di Padova, ViaGiustiniani 2, 35128 Padova, Italy, 38Cochlear Europe, 39Cochlear Europe, 40“La Palladienne”, Plan Peyrassou,83890 Besse sur Issole, France
Efficacy of the SPEAK and ACE coding strategies was compared with that of a new strategy, MP3000™, by 37European implant centers including 221 subjects. The SPEAK and ACE strategies are based on selection of8–10 spectral components with the highest levels, while MP3000 is based on the selection of only 4–6components, with the highest levels relative to an estimate of the spread of masking. The pulse rate percomponent was fixed. No significant difference was found for the speech scores and for codingpreference between the SPEAK/ACE and MP3000 strategies. Battery life was 24% longer for the MP3000strategy. With MP3000 the best results were found for a selection of six components. In addition, the bestresults were found for a masking function with a low-frequency slope of 50 dB/Bark and a high-frequencyslope of 37 dB/Bark (50/37) as compared to the other combinations examined of 40/30 and 20/15 dB/Bark. The best results found for the steepest slopes do not seem to agree with current estimates of thespread of masking in electrical stimulation. Future research might reveal if performance with respect toSPEAK/ACE can be enhanced by increasing the number of channels in MP3000 beyond 4–6 and itshould shed more light on the optimum steepness of the slopes of the masking functions applied in MP3000.
Keywords: Cochlear implant, Speech coding, Masking, Spread of excitation, Battery life
IntroductionPresent-day cochlear implant electronic circuitry offershigh processing capacity while taking little space. Thus,the bandwidth of sound coding is hardly limited butminiaturization of the sound processors requiressmall power supplies and consequently coding strat-egies with low energy consumption. Sampling theenvelopes rather than the fine structure of the outputof a set of contiguous band filters has been proved tobe an effective coding strategy for cochlear implants(Continuous Interleaved Sampling, CIS, Wilsonet al., 1991). The next step in reducing the informationto be transmitted, and thus the energy consumption,was implemented in the SPEAK and ACE strategiesof the Nucleus implant. Instead of transmitting to theneuronal array the stimulus levels across 22 frequencybands corresponding to 22 electrode locations, thenumber of stimulus levels transmitted after eachsample of the spectral energy distribution was limitedto, for example, 10 levels representing the highestlevels in that sample. This is referred to as N-of-Mcoding, in this example 10 of 22 (Wilson et al., 1988,1995; McKay et al., 1991; McDermott et al., 1992;Buechner et al., 2009). This strategy focused on trans-ferring the most salient sound properties, particularlyspeech properties, accepting that it suffices to transmitthe spectral peaks of the sound.In the past decade the opposite approach, focusing
on hearing properties, has been very successful insound coding for people with normal hearing. Innormal hearing, low-level frequency components of asound are masked by spectrally adjacent strong com-ponents because cochlear excitation introduced bythe strong components spreads out to adjacent
regions tuned to adjacent frequencies. This impliesthat one does not need to transfer the information inthe components that will be masked, which wasimplemented in the nowadays widely used MP3 com-pression strategy (Jayant et al., 1993). This approachin signal coding, derived from hearing properties,suggested including spread of excitation and sub-sequent masking in the ACE coding strategy.However, the new coding was not simply based onrejecting spectral components that are supposed tobe masked. In line with the ACE concept, the newcoding strategy again recruits N-of-M spectral com-ponents, but rather than taking N components withthe highest levels it takes N components with thehighest levels relative to the calculated maskedthreshold. Thus, components that well exceed the cal-culated masked threshold will be transmitted. Thiscoding strategy was coined MP3000.With ACE coding one may expect that two adjacent
spectral components are likely to be selected when thespectral energy distribution shows a broad maximum.However, the strongest component will stimulate anarray of nerve fibers that might well extend past theadjacent electrode. If subsequently the adjacent elec-trode is stimulated with the second strongest com-ponent, then many nerve fibers at that locationmight have responded already to the strongest com-ponent. With MP3000, it is not likely that an adjacentspectral component will be selected because the levelof the second strongest component relative to the cal-culated masked threshold will be very small. A moredistant spectral component will be selected. Thus,MP3000 avoids repetitive stimulation of groups ofneurons. It selects components that are dispersed
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4 195
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited

more widely across the spectrum (Nogueira et al.,2005, Table 2; Lai and Dillier, 2008).The present paper reports the results of a European
multi-center clinical study in which Nucleus® implantrecipients using the SPEAK/ACE strategy were con-verted to the MP3000 coding strategy. The studyincluded 221 subjects from 37 implant centers.Strategy preference and speech scores were collected.Battery life was recorded.
Materials and methodsSelection of spread of excitation parametersand number of componentsIn the MP3000 approach it was decided not to take acertain masking function or estimate of spread of exci-tation with electrical stimulation from the literature butto include several preset values as an experimental vari-able.Apriori, it was not clear that the electrophysiologicaland psychophysical measures of masking and spread ofexcitation available in the literature (Abbas et al., 2004;Cohen et al., 2004, 2005) would be appropriate. Themaskingmodel appliedwas based on psychophysical esti-mates for normal hearing in the sense that the maskingfunctions were assumed to follow linear filter slopes indB per Bark (Zwicker and Feldtkeller, 1967; Zwickerand Fastl, 1990). The frequency scale in Bark is derivedfrom the bandwidth of auditory filters. The band filtersin the Nucleus implant closely follow the Bark scale.Also, the current stimulus-level definition of theNucleus implant closely follows the dB scale, about 5.3current units per dB. Hence, the slopes were taken aslinear in current units per frequency channel.Remarkably, pilot experiments in CI subjects, varyingfilter slopes, showed that the highest speech scores werefound for quite steep slopes (Nogueira et al., 2005;Büchner et al., 2008). For normal hearing subjects, thelow-frequency slope is 27 dB/Bark, quite independentof stimulus level. The high-frequency slope is 27 dB/Bark at low stimulus levels decreasing to 5 dB/Bark athigh levels (Zwicker and Feldtkeller, 1967; Zwicker andFastl, 1990). In the pilot experiments in CI subjectsquoted above the highest speech scores were found foreven steeper slopes than 27 dB/Bark. In view of thosepreliminary results, we chose for the present experimentthree pairs of low- and high-frequency slopes, indepen-dently of stimulus level: 50/37, 40/30, and 20/15 dB/Bark.Since MP3000 selects spectral components more
widely dispersed than SPEAK/ACE (Nogueiraet al., 2005, Table 2), we expected that less frequencycomponents would be needed to cover the peaks ofthe spectral energy distribution. Where N (of M )was 6–14 in the existing SPEAK/ACE fittings of theparticipating subjects, we reduced N to threeexperimental values of 4, 5, and 6 in the presentexperiment.
Study designTwo sessions were planned to find for each subject theoptimum number of frequency bands or channels fromN= 4, 5, or 6 and the optimum pair of slopes (from50/37, 40/30, or 20/15 dB/Bark) in the MP3000strategy. Starting with nine conditions to choosefrom was considered to be too demanding for the sub-jects. Therefore, per subject the optimum number ofchannels, in terms of subjective preference andspeech perception, was first determined for only onepair of slopes, the slopes being assigned at randomto the subjects. Second, the optimum pair ofslopes was determined for only the optimum numberof channels found for each subject in the previoussession.
The SPEAK/ACE (A) and MP3000 (B) strategieswere compared in a sequential ABABA design. Thecomparison was conducted for only the optimum com-bination of number of channels and pair of slopesfound in each individual for MP3000. The numberof channels in the SPEAK/ACE condition was leftunchanged with respect to previous implant usage(8–14). Speech scores were collected as follows: firstspeech perception was measured for the SPEAK/ACE condition used previously by the subject (A1).After these measurements the subjects received threeMP3000 programs with 4, 5, and 6 channels for 4weeks and the pair of slopes assigned at random.The optimum number of channels was determinedfrom the individual’s preference and from speechscores after these 4 weeks. Next, the subjects receivedthree MP3000 programs with the pair of slopes of50/37, 40/30, or 20/15 dB/Bark and the individual’soptimum number of channels for another 4 weeks.Eight weeks after A1 speech scores were collected forthe individual’s optimum number of channels andthe optimum pair of slopes in MP3000 (B1).Subsequently, signal coding was switched back toSPEAK/ACE for 2 weeks after which speech scoresA2 were collected. Next, coding was switched backto MP3000 for another 2 weeks and scores B2 werecollected. Finally, after 2 more weeks of theSPEAK/ACE and MP3000 strategies at choice, thespeech scores A3 were measured for SPEAK/ACEand the individual’s preferred strategy was recorded.
In each subject the pulse rate per channel used pre-viously was kept unchanged in SPEAK/ACE duringthe study. This channel rate was copied intoMP3000. Thus, the total pulse rate was markedlylower in MP3000 (4–6 channels) than in SPEAK/ACE (6–14 channels). Battery life was recorded forboth strategies.
Speech testsThe subjects per language were Dutch 32, Dutch-Flemish 19, English 9, French 23, German 58,
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4196
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited

Italian 26, Polish 26, and Spanish 16. The German andSwiss centers used the same German test. In principle,the different languages do not constitute an exper-imental problem since the study addresses within-subject comparisons of the coding strategies. Inquiet, word tests were applied in all languages. Theywere scored in either phonemes or words correct(Dutch and Dutch-Flemish: Nederlandse Verenigingvoor Audiologie (NVA) monosyllables; English:Consonant Nucleus Consonant (CNC) monosyllables;French: Fournier disyllabic words; German: Freiburgmonosyllables; Italian: words; Polish: Pruszewiczmonosyllables; Spanish: bisyllabic words). In noise,sentence materials were used at a fixed speech-to-noise ratio of 10 dB for French, Italian, and Polish(French: MBAA2 sentences). For Dutch, Dutch-Flemish, English, German, and Spanish adaptive sen-tence tests were used. Speech level was varied adap-tively in noise fixed at 65 dB Sound Pressure Level(SPL) to find the speech-to-noise ratio at which thescore was 50% (Dutch: Plomp sentences, Dutch-Flemish: Leuven Intelligibility Sentence Test (LIST)sentences; English: Bamford Kowal Bench (BKB) sen-tences; German: Oldenburg sentences; Spanish:Hearing In Noise Test (HINT) sentences).
T and C levelsSince the MP3000 strategy investigated included fewerchannels and, thus, a smaller overall stimulus rate, itwas necessary to adjust the T and C levels for theMP3000 strategy in order to obtain a fair comparisonto the SPEAK/ACE strategy. T and C levels could beshifted in parallel and, if necessary, tilted. When deter-mining the MP3000 C levels subjects were asked tocarefully match the MP3000 loudness to the loudnessof the former SPEAK/ACE C levels. Comparing theaverage T and C profiles across the whole electrodearray for the two strategies, parallel upward shifts of6.9 (s.d.= 8.0) current units for the T levels ofMP3000 and 6.8 (s.d.= 6.3) current units for the Clevels were found. Some changes in the levels of indi-vidual electrodes and in the tilt of the profiles didoccur but the result can be well summarized by thisparallel shift. One may expect that the shift givenabove depends on the difference in number of channelsbetween the two strategies. This dependence was foundto be very small; only ±1 current unit for both the Tand C levels from the smallest difference in numberof channels of 8 in SPEAK/ACE and 6 in MP3000to the largest difference of 14 in SPEAK/ACE and 4in MP3000.
SubjectsThe study included 221 subjects from 37 Europeanimplant centers in 9 countries. Twelve subjects with-drew from the study because they were not willing to
take the risk that the change to MP3000 mightreduce their hearing performance. Thus, the quanti-tative data presented in this paper stem from 209subjects.The inclusion criteria were:
1. twelve years of age or older. For subjects youngerthan 18 years, a parental or guardian approval wasrequired;
2. actively using the Freedom™ system for 6 monthsor longer (CI24RE recipient) or actively using theFreedom BTE system for 1 month or longer(CI24R or CI24M recipient) at entry of the study;
3. ability to read and write in the language of the testmaterials;
4. sufficient open-set speech perception to allow com-parison of strategies;
5. willingness to participate in the study and to complywith all the requirements of the protocol.
The exclusion criteria were:1. established user of the CIS coding strategy;2. implanted bilaterally with CI systems;3. additional handicaps that may prevent participation
in the evaluations;4. unrealistic expectations on the part of the recipient
regarding the possible benefits.Exclusion criteria (1) and (2) were included since thenumber of controllable experimental variables had tobe limited. The present investigation basicallyaddresses the comparison of the new MP3000 strategyto the conventional ACE strategy when selecting fewerchannels than available. The CIS strategy is not basedon dynamical selection of fewer channels than avail-able. Likewise, monolateral versus bilateral does nottouch the major question of the present study.Unrealistic expectations implied, of course, a subjec-tive assessment of the responsible clinician that hadto be respected.The median age was 55 years; the range was 12–85
years. Nine subjects were younger than 18 years.Median severe-to-profound hearing loss (SPHL) dur-ation was 10 years. SPHL duration in 12% of the209 subjects was larger than 30 years. Twenty-six sub-jects had pre-lingual SPHL. Still, these subjects hadenough open-set speech understanding to completethe speech tests. Ipsi-lateral residual hearing wasreported in 10 subjects (5%) and contra-lateral residualhearing in 73 subjects (35%). During the tests contra-lateral hearing was attenuated by inserting an ear plugin the non-implanted ear.The etiology of deafness corresponded to what one
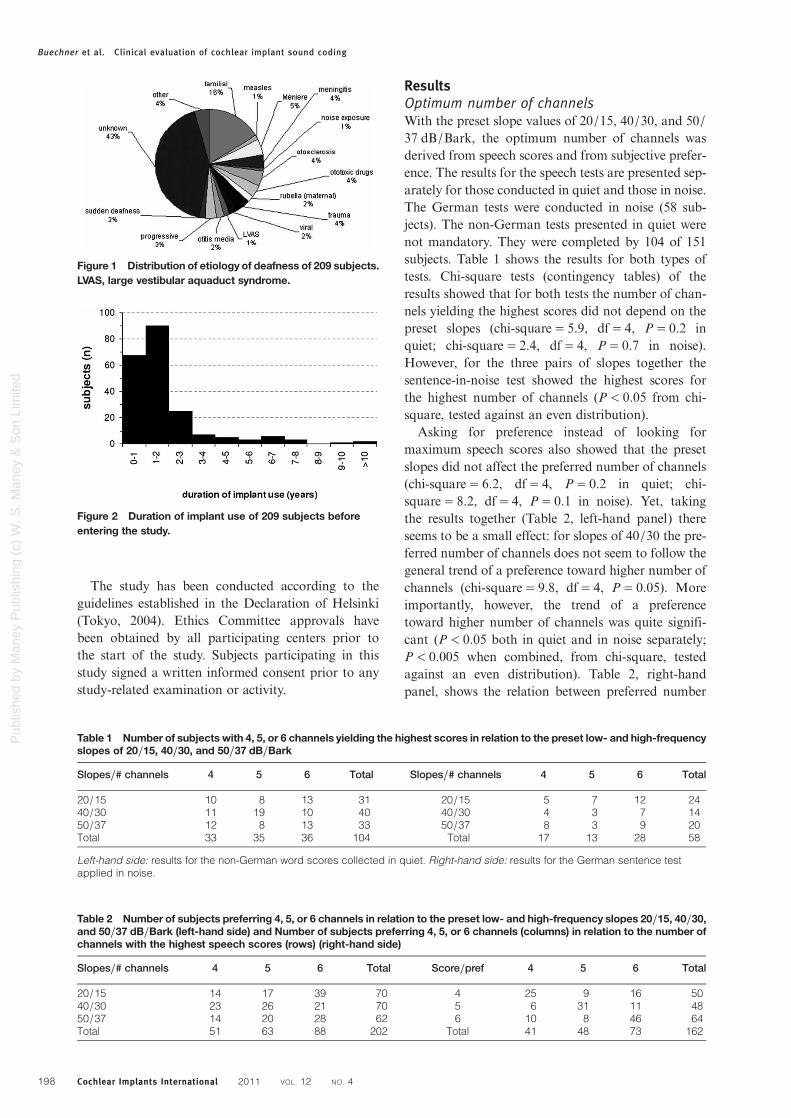
typically finds with 43% unknown origin of deafnessand 16% of hereditary/familial origin (Fig. 1). Fig. 2shows a histogram of the duration of implant usebefore entering the present study. Median implant usewas 1.4 years; the range was 0.2–12.8 years. Implantuse in seven subjects was shorter than 6 months, con-trary to the intake criterion but accepted.
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4 197
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited
The study has been conducted according to theguidelines established in the Declaration of Helsinki(Tokyo, 2004). Ethics Committee approvals havebeen obtained by all participating centers prior tothe start of the study. Subjects participating in thisstudy signed a written informed consent prior to anystudy-related examination or activity.
ResultsOptimum number of channelsWith the preset slope values of 20/15, 40/30, and 50/37 dB/Bark, the optimum number of channels wasderived from speech scores and from subjective prefer-ence. The results for the speech tests are presented sep-arately for those conducted in quiet and those in noise.The German tests were conducted in noise (58 sub-jects). The non-German tests presented in quiet werenot mandatory. They were completed by 104 of 151subjects. Table 1 shows the results for both types oftests. Chi-square tests (contingency tables) of theresults showed that for both tests the number of chan-nels yielding the highest scores did not depend on thepreset slopes (chi-square= 5.9, df= 4, P= 0.2 inquiet; chi-square= 2.4, df= 4, P= 0.7 in noise).However, for the three pairs of slopes together thesentence-in-noise test showed the highest scores forthe highest number of channels (P< 0.05 from chi-square, tested against an even distribution).
Asking for preference instead of looking formaximum speech scores also showed that the presetslopes did not affect the preferred number of channels(chi-square= 6.2, df= 4, P= 0.2 in quiet; chi-square= 8.2, df= 4, P= 0.1 in noise). Yet, takingthe results together (Table 2, left-hand panel) thereseems to be a small effect: for slopes of 40/30 the pre-ferred number of channels does not seem to follow thegeneral trend of a preference toward higher number ofchannels (chi-square= 9.8, df= 4, P= 0.05). Moreimportantly, however, the trend of a preferencetoward higher number of channels was quite signifi-cant (P< 0.05 both in quiet and in noise separately;P< 0.005 when combined, from chi-square, testedagainst an even distribution). Table 2, right-handpanel, shows the relation between preferred number
Table 1 Number of subjects with 4, 5, or 6 channels yielding the highest scores in relation to the preset low- and high-frequencyslopes of 20/15, 40/30, and 50/37 dB/Bark
Slopes/# channels 4 5 6 Total Slopes/# channels 4 5 6 Total
20/15 10 8 13 31 20/15 5 7 12 2440/30 11 19 10 40 40/30 4 3 7 1450/37 12 8 13 33 50/37 8 3 9 20Total 33 35 36 104 Total 17 13 28 58
Left-hand side: results for the non-German word scores collected in quiet. Right-hand side: results for the German sentence testapplied in noise.
Figure 1 Distribution of etiology of deafness of 209 subjects.LVAS, large vestibular aquaduct syndrome.
Figure 2 Duration of implant use of 209 subjects beforeentering the study.
Table 2 Number of subjects preferring 4, 5, or 6 channels in relation to the preset low- and high-frequency slopes 20/15, 40/30,and 50/37 dB/Bark (left-hand side) and Number of subjects preferring 4, 5, or 6 channels (columns) in relation to the number ofchannels with the highest speech scores (rows) (right-hand side)
Slopes/# channels 4 5 6 Total Score/pref 4 5 6 Total
20/15 14 17 39 70 4 25 9 16 5040/30 23 26 21 70 5 6 31 11 4850/37 14 20 28 62 6 10 8 46 64Total 51 63 88 202 Total 41 48 73 162
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4198
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited

of channels and the number for which the highestspeech scores were found. This panel shows that 102(sum of diagonal elements 25+ 31+ 46) of 162 sub-jects preferred the number of channels for which thehighest speech scores were found. In addition, itshows that 36 subjects preferred a higher and 24 sub-jects a lower number of channels (the sums of theoff-diagonal elements).In summary, across subjects there was little effect of
the preset slope values on the number of channels pre-ferred or on those with the highest speech scores.Overall, there was a preference toward the highestnumber of channels, which was also found for the sen-tence scores in noise. Whenever the preferred numberof channels did not correspond to the number of chan-nels yielding the highest speech score, the clinicianasked the subject whether or not the preferrednumber of channels was preferred above the numberof channels yielding the highest speech score. If notthe number of channels yielding the highest scorewas chosen, otherwise the preferred number of chan-nels was kept.
Optimum pair of slopesAfter the second phase of optimizing MP3000 inwhich the subjects were presented with three pairs ofslopes at the optimum number of channels found inthe first phase reported above, the results showedthat the slopes yielding the highest speech scores didnot depend on the optimum number of channels(chi-square= 1.0, df= 4, P= 0.9 in quiet; chi-square= 5.9, df= 4, P= 0.2 in noise). The same wasfound for the preferred slopes (chi-square= 5.3, df=4, P= 0.3 in quiet; chi-square= 4.2, df= 4, P= 0.4in noise). However, Table 3 shows that there was aclear preference for the steeper slopes, P< 0.001 forboth the preferred slopes and those yieldingmaximum speech scores (from chi-square, testedagainst an even distribution). This suggests that theslopes preset at the beginning of the experiment,which were about evenly spread, had little effect onthe preferred slopes and the slopes yieldingmaximum speech scores after 8 weeks. This is illus-trated in Table 4 showing the preferred slopes inrelation to the preset slopes. The number of preferredslopes equal to the preset slopes was 86 (sum of thediagonal elements); 91 preferred slopes were steeper
and 32 were shallower than the preset slopes (sum ofthe off-diagonal elements). In summary, these resultsshowed that the individual’s optimum number ofchannels had no effect on the optimum pair ofslopes. Overall, there is a clear preference towardsteeper slopes.Whenever the preferred pair of slopes did not corre-
spond to the slopes yielding the highest speech score,the investigator followed the same procedure as forthe number of channels described above. The preferredslopes were kept whenever these slopes were preferredabove the slopes yielding the highest scores; otherwisethe pair of slopes with the highest score was kept.
Comparison of the speech scores for SPEAK/ACEand MP3000Analysis of variance of the word scores collected inquiet in the ABABA sequence showed no effect ofstrategy (P= 0.5, F(1,191)= 0.5). Mean scores were65.6% for SPEAK/ACE and 66.2% for MP3000.There was a significant effect of order of measurement(P< 0.001). However, the effect was small. The scoresincreased by 3% from the first to the last session. Thescores among languages differed significantly (P<0.001) (Fig. 3).The word scores collected in noise at S/N=+10 dB
(French, Italian, and Polish) showed no effect of strat-egy (P= 0.6, F(1,65)= 0.3). Mean scores were 45.7%for SPEAK/ACE (A) and 46.8% for MP3000. Therewas no change of the scores over time (P= 0.5).Also, there was no effect of language (P= 0.6): themean scores for the three languages were 41–50%(Fig. 4). The adaptive sentence tests (Dutch, Dutch-Flemish, English, German, and Spanish) alsoshowed no effect of strategy (P= 1.0, F(1,118)=0.0). Mean S/N values were +7.6 dB both forSPEAK/ACE and MP3000. The only significanteffect was due to language (P< 0.001). Four testsshowed thresholds at S/N=+9 to +11 dB; the
Table 3 Number of subjects with preferred slopes (left-hand side) and with slopes yielding the highest scores (right-hand side)in relation to the optimum number of channels
# channels/slope 20/15 40/30 50/37 Total # channels/slope 20/15 40/30 50/37
4 5 22 29 56 4 5 17 195 5 21 40 66 5 10 12 276 15 34 38 87 6 10 23 32Total 25 77 107 209 Total 25 52 78
Table 4 Preferred slopes in relation to the preset slopes atthe beginning of the experiment
Pre/post 20/15 40/30 50/37 Total
20/15 11 26 35 7240/30 9 33 30 7250/37 5 18 42 65Total 25 77 107 209
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4 199
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited
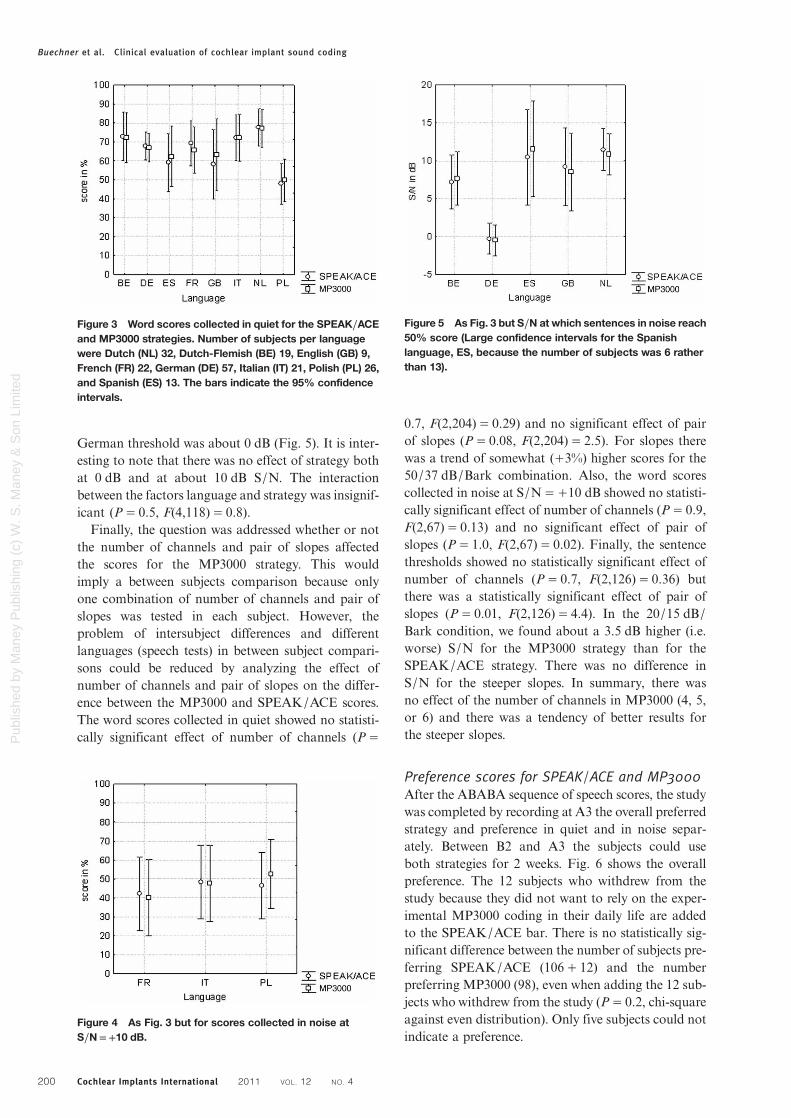
German threshold was about 0 dB (Fig. 5). It is inter-esting to note that there was no effect of strategy bothat 0 dB and at about 10 dB S/N. The interactionbetween the factors language and strategy was insignif-icant (P= 0.5, F(4,118)= 0.8).Finally, the question was addressed whether or not
the number of channels and pair of slopes affectedthe scores for the MP3000 strategy. This wouldimply a between subjects comparison because onlyone combination of number of channels and pair ofslopes was tested in each subject. However, theproblem of intersubject differences and differentlanguages (speech tests) in between subject compari-sons could be reduced by analyzing the effect ofnumber of channels and pair of slopes on the differ-ence between the MP3000 and SPEAK/ACE scores.The word scores collected in quiet showed no statisti-cally significant effect of number of channels (P=
0.7, F(2,204)= 0.29) and no significant effect of pairof slopes (P= 0.08, F(2,204)= 2.5). For slopes therewas a trend of somewhat (+3%) higher scores for the50/37 dB/Bark combination. Also, the word scorescollected in noise at S/N=+10 dB showed no statisti-cally significant effect of number of channels (P= 0.9,F(2,67)= 0.13) and no significant effect of pair ofslopes (P= 1.0, F(2,67)= 0.02). Finally, the sentencethresholds showed no statistically significant effect ofnumber of channels (P= 0.7, F(2,126)= 0.36) butthere was a statistically significant effect of pair ofslopes (P= 0.01, F(2,126)= 4.4). In the 20/15 dB/Bark condition, we found about a 3.5 dB higher (i.e.worse) S/N for the MP3000 strategy than for theSPEAK/ACE strategy. There was no difference inS/N for the steeper slopes. In summary, there wasno effect of the number of channels in MP3000 (4, 5,or 6) and there was a tendency of better results forthe steeper slopes.
Preference scores for SPEAK/ACE and MP3000After the ABABA sequence of speech scores, the studywas completed by recording at A3 the overall preferredstrategy and preference in quiet and in noise separ-ately. Between B2 and A3 the subjects could useboth strategies for 2 weeks. Fig. 6 shows the overallpreference. The 12 subjects who withdrew from thestudy because they did not want to rely on the exper-imental MP3000 coding in their daily life are addedto the SPEAK/ACE bar. There is no statistically sig-nificant difference between the number of subjects pre-ferring SPEAK/ACE (106+ 12) and the numberpreferring MP3000 (98), even when adding the 12 sub-jects who withdrew from the study (P= 0.2, chi-squareagainst even distribution). Only five subjects could notindicate a preference.
Figure 3 Word scores collected in quiet for the SPEAK/ACEand MP3000 strategies. Number of subjects per languagewere Dutch (NL) 32, Dutch-Flemish (BE) 19, English (GB) 9,French (FR) 22, German (DE) 57, Italian (IT) 21, Polish (PL) 26,and Spanish (ES) 13. The bars indicate the 95% confidenceintervals.
Figure 5 As Fig. 3 but S/N at which sentences in noise reach50% score (Large confidence intervals for the Spanishlanguage, ES, because the number of subjects was 6 ratherthan 13).
Figure 4 As Fig. 3 but for scores collected in noise atS/N=+10 dB.
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4200
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited
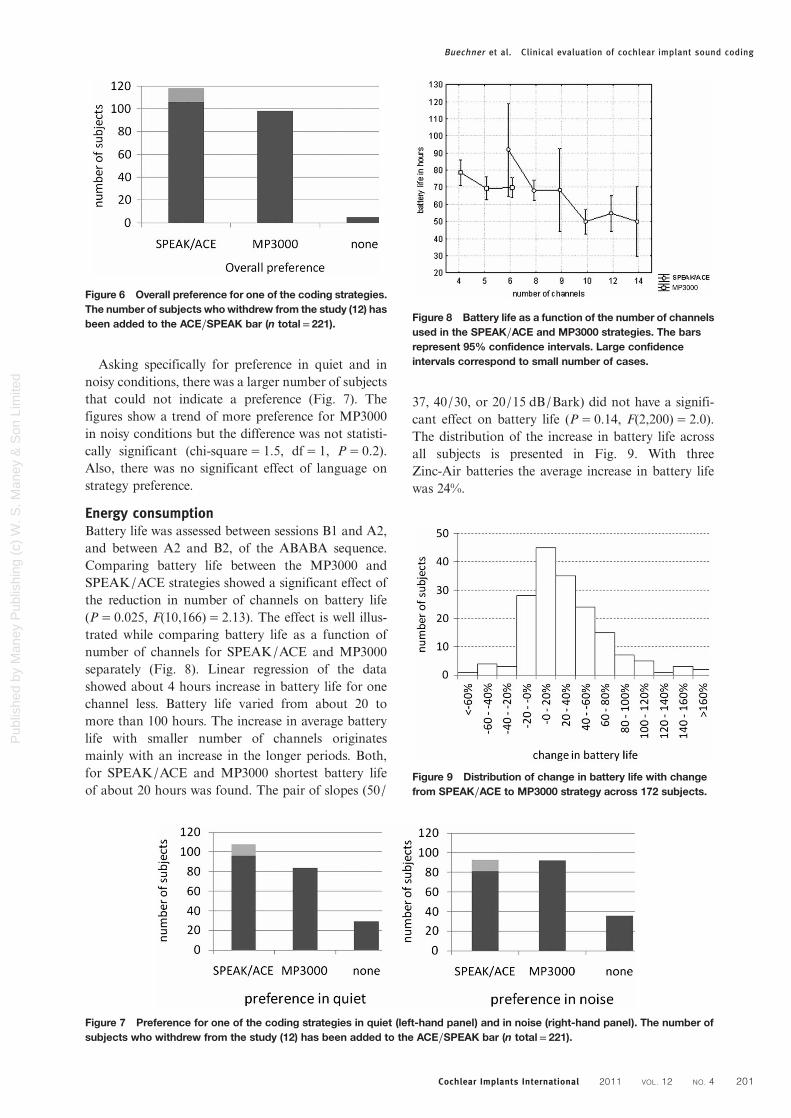
Asking specifically for preference in quiet and innoisy conditions, there was a larger number of subjectsthat could not indicate a preference (Fig. 7). Thefigures show a trend of more preference for MP3000in noisy conditions but the difference was not statisti-cally significant (chi-square= 1.5, df= 1, P= 0.2).Also, there was no significant effect of language onstrategy preference.
Energy consumptionBattery life was assessed between sessions B1 and A2,and between A2 and B2, of the ABABA sequence.Comparing battery life between the MP3000 andSPEAK/ACE strategies showed a significant effect ofthe reduction in number of channels on battery life(P= 0.025, F(10,166)= 2.13). The effect is well illus-trated while comparing battery life as a function ofnumber of channels for SPEAK/ACE and MP3000separately (Fig. 8). Linear regression of the datashowed about 4 hours increase in battery life for onechannel less. Battery life varied from about 20 tomore than 100 hours. The increase in average batterylife with smaller number of channels originatesmainly with an increase in the longer periods. Both,for SPEAK/ACE and MP3000 shortest battery lifeof about 20 hours was found. The pair of slopes (50/
37, 40/30, or 20/15 dB/Bark) did not have a signifi-cant effect on battery life (P= 0.14, F(2,200)= 2.0).The distribution of the increase in battery life acrossall subjects is presented in Fig. 9. With threeZinc-Air batteries the average increase in battery lifewas 24%.
Figure 6 Overall preference for one of the coding strategies.The number of subjects whowithdrew from the study (12) hasbeen added to the ACE/SPEAK bar (n total= 221).
Figure 7 Preference for one of the coding strategies in quiet (left-hand panel) and in noise (right-hand panel). The number ofsubjects who withdrew from the study (12) has been added to the ACE/SPEAK bar (n total= 221).
Figure 8 Battery life as a function of the number of channelsused in the SPEAK/ACE and MP3000 strategies. The barsrepresent 95% confidence intervals. Large confidenceintervals correspond to small number of cases.
Figure 9 Distribution of change in battery life with changefrom SPEAK/ACE to MP3000 strategy across 172 subjects.
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4 201
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited

DiscussionThe present study shows that there is no differencebetween the speech scores found for individually opti-mized SPEAK/ACE and MP3000 strategies. Thisresult is found for speech scores collected both in aquiet and in a noisy background and moreover forspeech scores collected in noise at S/N=+10 and0 dB. Also, there are no differences between the twostrategies for eight languages with their respectivespeech tests. In addition, strategy preference wasabout equally distributed between the SPEAK/ACEand MP3000 strategies (Figs 6–8).Equal scores were found for the two strategies while
the number of channels was 6–14 in SPEAK/ACE andonly 4–6 in MP3000. Since the pulse rate per channelwas not changed when switching from SPEAK/ACEto MP3000, it implied that equal scores were foundfor markedly lower total pulse rates in MP3000 thanin SPEAK/ACE. This is reflected in battery life,which for MP3000 was 24% longer with three Zinc-Air batteries than for SPEAK/ACE.The present study did not include a SPEAK/ACE
condition with 4–6 channels. Thus, it does not provethat the MP3000 coding principle accounts for main-taining the scores while reducing the number of chan-nels. However, a previous study has shown that at leasteight channels are required to achieve maximumspeech scores with the ACE strategy (Plant et al.,2002). Also, other SPEAK or N-of-M studies inwhich both the number of channels and channel ratewere varied suggest that maximum speech scores arereached with at least 8–10 channels (Fishman et al.,1997; Ziese et al., 2000; Friesen et al., 2001).Moreover, Buechner et al. (2008) showed for theOldenburg sentence test that ACE with eight channelsyielded significantly higher (worse) thresholds than anMP3000 type of coding scheme with eight channelsand even with four channels. Thus, the high scoresfound for MP3000 may be attributed to its codingprinciple that results in more dispersion, less clusteringof the channels stimulated. These results mightsuggest that MP3000 could yield even better resultsthan ACE for number of channels higher thaneight. However, the advantage of more dispersion inthe channels sampled decreases as the number of chan-nels increases. Obviously, there is no differencebetween the two coding strategies if all channels(M-of-M ) are used. Kals et al. (2010) found that thenumber of channels could be reduced from 11 to 4without losing speech performance in noise if forcingthe selection of the smaller number of selectedfrequency components into a wider spectral distri-bution (less cluttering). This technique is comput-ationally less intensive. However, it forces theselection of channels into a wider spectral distributionaccording to a fixed preset scheme, not according to a
physiologically based masking function operatingdynamically.
The MP3000 strategy was individually optimizedchoosing among 4, 5, or 6 channels and three combi-nations of slopes: 50/37, 40/30, and 20/15 dB/Bark.Since it was considered to be too demanding for thesubject to start with nine conditions to choose from, itwas decided to determine the individual’s optimum intwo steps: starting by determining the optimumnumber of channels with one fixed pair of slopesassigned at random and subsequently determining theoptimum pair of slopes for the optimum number ofchannels found in the first step. Tables 1 and 2 showedthat there was no effect of the preset pair of slopes oneither the number of channels with the highest score orthe preferred number of channels. Although individualdependence of the best number of channels on thepreset pair of slopes cannot be excluded, this resultsuggests that the preset values had little effect on theresulting best number of channels. The next stepshowed a similar result: the optimum pair of slopes didnot depend on the best number of channels found inthe previous step (Table 3). Comparing the best pair ofslopes with the preset values shows quite a shift towardthe steeper slopes (Table 4). Together these resultsstrongly suggest that the two-step approach towardfinding the best combination of number of channelsand pair of slopes, starting with preset slopes, did notintroduce undesired interactions in the procedure.
For all preset pairs of slopes, the preferred numberof channels was evenly distributed for the speechscores collected in quiet but the larger number of chan-nels showed better performance for sentences pre-sented in noise and there was a clear preference forthe higher number of channels. The rate per channelwas independent of the number of channels. Thus,more channels implied a higher total rate. Both,total rate or number of channels could have yieldedbetter speech information transfer. The present resultsuggests a default value of six channels.
The result for the best pair of slopes is intriguing,although in line with the results of pilot experiments(e.g. Nogueira et al., 2005). The speech scores arehighest for the steepest slopes and these slopes arealso preferred. This implies that one prefers the con-dition with the smallest amount of spectral spread.This might be a habituation result. The subjects wereaccustomed to the SPEAK/ACE strategy for amedian period of 1.4 years (Fig. 2). However, thisfinding may also be related to the dispersion of theselected spectral components. With shallower slopesthere is more dispersion resulting in more spectralpeaks represented by two or only one frequency com-ponent (see Nogueira et al., 2005, Table 2). This rep-resentation may jump across channels from onespectral sample to the next, which could produce a
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4202
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited

noisier percept. Still, it is not quite understood whysuch steep slopes are preferred whereas the estimatesof spread of excitation are much broader (Abbaset al., 2004; Cohen et al., 2004, 2005). Most estimatesof spread of excitation are based on the old straightarray electrode. One might assume smaller spread ofexcitation for the new Contour™ electrode. Cohenet al. (2005) did not find significant differences inspread of excitation between these two types of electro-des, whereas van Weert et al. (2005) and Cohen (2009)found slightly less spread of excitation for the Contourelectrode but the results do not suggest that the ade-quate masking function for MP3000 should haveslopes steeper than the typical psychoacousticalslopes of 24 dB/Bark (Zwicker and Feldtkeller, 1967;Zwicker and Fastl, 1990). Yet, the present resultsuggests that one could use the 50/37 dB/Bark combi-nation as the default value. Steeper slopes were notincluded in the present study. Thus, it cannot beexcluded that steeper slopes might have yielded evenbetter results. However, in view of the above discussionthis is not expected.In conclusion, the new MP3000 coding strategy,
taking into account spread of masking, allows for areduction in number of channels from typically 8–12in conventional coding (SPEAK/ACE) to 4–6 inMP3000 without losing performance. The reductionin number of channels implies 24% increase inbattery life. If one is interested in increasing perform-ance rather than in increasing battery life one mighttry to use more than 4–6 channels in MP3000.However, the increase in performance will be limitedbecause the difference between the two codingstrategies will decrease as the number of channelsincreases. The best speech scores were found for thesteepest masking slopes applied in the MP3000coding strategy. This result was not quite expected. Itwas discussed above but future research shouldreveal the optimum steepness of the slopes and itshould clarify the relation between the optimum steep-ness and known estimates of spread of masking andspread of excitation.
AcknowledgementsThe authors would like to express their gratitude to thefollowing contributors: John Allum, Roberto Bartoli,Elisabeth Estrada, Juan Carlos Falcón González,Stefan Gräbel, Heinrich Iro, WaiKong Lai, RolandLaszig, Manuel Manrique, Andreas Nägeli, ErwinOffeciers, Cathy Silhol, Guillermina Tarayre, AlainUziel, and Simone Volpert.
GlossaryACE: advanced combinational encoder, similar to
SPEAK but with higher pulse rates
CIS: continuous interleaved sampling, a strategy inwhich a fixed number of frequency channels issampled continuously in a fixed orderMP3000: a coding strategy in which only N channels
ofM available channels are chosen dynamically accord-ing to the instantaneous peak levels in all channelsrelative to a physiologically-based masking functionN-of-M: a coding strategy in which only N channels
of M available channels are chosen dynamicallySPEAK: spectral peak strategy, a strategy in which
only N channels of M available channels are chosendynamically according to the instantaneous peaklevels in all channels
ReferencesAbbas P.J., Hughes M.L., Brown C.J., Miller C.A., South H. 2004.
Channel interaction in cochlear implant users evaluated usingthe electrically evoked compound action potential. Audiologyand Neuro-Otology, 9(4): 203–213.
Buechner A., Noguiera W., Edler B., Battmer R.-D., Lenarz T. 2008.Results from a psychoacoustic model-based strategy for theNucleus-24 and Freedom cochlear implants. Otology &Neurotology, 29: 189–192.
Buechner A., Frohe-Buechner C., Boyle P., Battmer R.-D., LenarzT. 2009. A high rate n-of-m speech processing strategy for thefirst generation Clarion cochlear implant. InternationalJournal of Audiology, 48: 868–875.
Cohen L.T. 2009. Practical model description of peripheral neuralexcitation in cochlear implant recipients: 2. Spread of the effec-tive stimulation field (ESF) from ECAP and FEA. HearingResearch, 247: 100–111.
Cohen L.T., Saunders E., Richardson L.M. 2004. Spatial spread ofneural excitation: comparison of compound action potentialand forward-masking data in cochlear implant patients.International Journal of Audiology, 43: 346–355.
Cohen L.T., Lenarz T., Battmer R.-D., Bender von Saebelkampf C.,Busby P.A., Cowan R.S.C. 2005. A psychophysical forwardmasking comparison of longitudinal spread of neural excitationin the Contour and straight Nucleus electrode arrays.International Journal of Audiology, 44: 559–566.
Fishman K.E., Shannon R.V., Slatterly W.H. 1997. Speech recog-nition as a function of the number of electrodes used in theSPEAK cochlear implant speech processor. Journal ofSpeech, Language and Hearing Research, 40: 1201–1215.
Friesen L.M., ShannonR.V., Baskent D.,WangX. 2001. Speech rec-ognition in noise as a function of the number of spectral chan-nels: comparison of acoustic hearing and cochlear implants.Journal of Acoustic Society of America, 110: 1150–1163.
Jayant N., Johnston J., Safranek R. 1993. Signal compression basedon models of human perception. Proceedings of the IEEE 81,10: 1385–1422.
KalsM., Schatzer R., Krenmayr A., Vermeire K., Visser D., Bader P.,et al. 2010. Results with a cochlear implant channel-picking strat-egy base on ‘Selected Groups’. Hearing Research, 260: 63–39.
Lai W., Dillier N. 2008. Investigating the MP3000 coding strategyfor music perception. Proceedings 11th. Jahrestagung derDeutschen Gesellschaft für Audiologie, Kiel, 1–3.
McDermott H.J., McKay C.M., Vandali A.E. 1992. A new portablesound processor for the University of Melbourne/Nucleusmulti-electrode cochlear implant. Journal of Acoustic Societyof America, 91: 3367–3371.
McKay C.M., McDermott H.J., Vandali A.E., Clark G. 1991.Preliminary results with a six spectral maxima sound processorfor the University of Melbourne/Nucleus multiple-electrodecochlear implant. Journal of Otolaryngological Society ofAustralia, 6: 354–359.
NogueiraW., BüchnerA., LenarzT., EdlerB. 2005.Apsychoacoustic‘NofM’-type speech coding strategy for cochlear implants.EURASIP Journal of Applied Signal Processing, 18: 3044–3059.
Plant K.L., Whitford L.A., Psarros C.E., Vandali A.E. 2002.Parameter selection and programming recommendations forthe ACE and CIS speech-processing strategies in the Nucleus24 cochlear implant system. Cochlear Implant International, 3:104–125.
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4 203
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited

Weert S., van Stokroos R.J., Rikers M.M.J.G., van Dijk P. 2005.Effect of peri-modiolar cochlear implant positioning on audi-tory nerve responses: A neural response telemetry study. ActaOtolaryngology, 125: 725–731.
Wilson B.S., Finley C.C., Farmer J.C., Lawson D.T., Weber B.A.,Wolford R.D., et al. 1988. Comparative studies of speech pro-cessing strategies for cochlear implants. Laryngoscope, 98:1069–1077.
Wilson B.S., Finley C.C., Lawson D.T., Wolford R.D., EddingtonD.L., Rabinowitz W.M. 1991. Better speech recognition withcochlear implants. Nature, 352: 236–238.
Wilson B.S., Lawson D.T., Zerbi M., Finley C.C., Wolford R.D.1995. New processing strategies in cochlear implantation.American Journal of Otology, 16: 669–675.
Ziese M., Stutzel A., Specht A., von Begall H., Freigang B., SrokaB,, Nopp P. 2000. Speech understanding with the CIS and then-of-m strategy in the MED-EL COMBI 40+ system. Journalof Otorhinolaryngology Related Species, 62: 321–329.
Zwicker E., Feldtkeller R. 1967. Das Ohr als Nachrichtenempfänger.S. Hirzel Verlag, Stuttgart
Zwicker E,, Fastl H. 1990. Psychoacoustics: Facts and Models.Berlin: Springer.
Buechner et al. Clinical evaluation of cochlear implant sound coding
Cochlear Implants International 2011 VOL. 12 NO. 4204
Pub
lishe
d by
Man
ey P
ublis
hing
(c)
W. S
. Man
ey &
Son
Lim
ited





























