Embed Size (px)
Citation preview
Archives of Gerontology and Geriatrics 49 Suppl. 2 (2009) S50–S54
Contents lists available at ScienceDirect
Archives of Gerontology and Geriatrics
journa l homepage: www.e lsev ier .com/ locate /archger
Clinical features of benign paroxysmal positional vertigo (BPPV) in Taiwan:
differences between young and senior age groups
Chung-Lan Kaoa,b,c, *, Wan-Ling Hsieha,c, Chang-Ming Chernb,d, Liang-Kung Chenb,c,e, Ming-Hsien Linb,c,e,Rai-Chi Chana,b
aDepartment of Physical Medicine and Rehabilitation, Taipei Veterans General Hospital, Shih-Pai Road, Section 2, 11217, Taipei, TaiwanbSchool of Medicine, National Yang-Ming University, No. 155, Sec. 2, Linong Street, Taipei, 11221, TaiwancCenter for Geriatrics and Gerontology, Taipei Veterans General Hospital, Shih-Pai Road, Section 2, 11217, Taipei, TaiwandDepartment of Neurology, Taipei Veterans General Hospital, Shih-Pai Road, Section 2, 11217, Taipei, TaiwaneDepartment of Family Medicine, Taipei Veterans General Hospital, Shih-Pai Road, Section 2, 11217, Taipei, Taiwan
a r t i c l e i n f o
Keywords:
Benign paroxysmal positional vertigo
Canalith repositioning procedure
Life quality
a b s t r a c t
BPPV is a common cause of vertigo. Several treatment procedures can facilitate recovery. In
this study, we aimed to identify the demographic features, resolution and recurrence rates and
impacts on daily activities in BPPV patient between young and senior age groups in Taiwan. This
retrospective study recruited 218 patients of BPPV. Medical history, canal involvement, treatment
required for complete resolution, symptom free period and recurrence rates were evaluated
between the two age groups. Up to 80.7% of patients were successfully treated by a single treatment.
For patients aged more than 65 years, the recurrence rate was 1.7 times higher than that in the
younger age group (p =0.07). The symptom-free period before recurrence was nearly 2.2 times
longer in the senior age group (p =0.03). Work-related activities were influenced more by BPPV in
the younger age group (p =0.03). We conclude that BPPV is prone to occur and recur in people of
senior age. Clinicians should have the knowledge to diagnose different types of BPPV and treat it
accordingly to prevent further complications.
© 2009 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
BPPV is one of the most common causes of vertigo. It is estimated
that BPPV accounts for 20–30% of all vertigo (Baloh et al., 1989;
Neuhauser et al., 2001; Yimtae et al., 2003). BPPV is characterized by
a sudden, brief period of vertigo when the patient’s head is moved
into a position in the affected semicircular canal. Although benign
in nature, BPPV can cause physical and psychological hazards in
patients’ daily activities (Lopez-Escamez et al., 2005). Fall accidents
resulted from vertiginous attacks in BPPV may subsequently
lead to further morbidity and disability. Even though BPPV may
resolve spontaneously, this sudden, unexpected symptom may be
frightening, and the relative immobilization period due to fear of
falling can cause secondary comorbidity, especially in the senior
age group. Therefore, it is crucial for the clinicians to accurately and
promptly diagnose and treat BPPV to reduce complications such as
fractures, immobility and muscle atrophy.
Several factors apparently predispose people to BPPV. They
include advanced age, head and neck trauma, inactivity, and other
ear diseases or surgeries (Steenerson et al., 2005). There are
* Corresponding author. C-L. Kao, Department of Physical Medicine
and Rehabilitation, Taipei Veterans General Hospital, Shih-Pai Road,
Section 2, 11217, Taipei, Taiwan.
Tel.: +(886-2) 28757363; fax: +(886-2) 28757359.
E-mail address: [email protected] (C-L. Kao).
two theories explaining the mechanisms of BPPV. The original
Schukencht’s “cupulolithiasis” theory (Schuknecht, 1969), attributes
the pathophysiology of BPPV to debris adhering to cupula. This
type of BPPV is less responsive to treatment maneuvers (Fife
et al., 2008). The “canalolithiasis” theory holds the view that the
mechanism of BPPV results from free floating clots trapped in the
ampullofugal branch of the semicircular canals. Whenever there are
head movements, the clots gravitate to the most dependent part
of the canal. The resultant endolymphatic flow causes vertigo and
nystagmus (Hall et al., 1979).
Several procedures are reported to be effective in the treatment
of BPPV. Based on the theory of cupulolithiasis, Brandt and
Daroff (1980) developed the first effective physical therapy of
redistribution exercise. Semont et al. (1988) introduced a liberatory
maneuver which cured 92.68% of BPPV patients, with only 4.22%
experiencing recurrences. The canalith repositioning procedure
(CRP), with several modifications since Epley’s original description
(Epley, 2001), has become a mainstay of treatment of posterior
canal BPPV (PC BPPV). Another procedure, so-called Lempert or
“barbeque” maneuver, was developed for the treatment of a BPPV
variant involving horizontal canal (HC) (Lempert and Tiel-Wilck,
1996). The purpose of this study was to identify the demographic
features, canal involvement, resolution and recurrence rates of BPPV
in Taiwan. We also attempted to answer questions about what
0167-4943 /$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved.

C-L. Kao et al. / Archives of Gerontology and Geriatrics 49 (2009) S50–S54 S51
differences exist in BPPV recurrence rates and impacts on daily
activities between young and senior age groups of the population.
2. Subjects and methods
2.1. The study sample
We retrospectively reviewed all BPPV patients who had received
treatment at the Department of Physical Medicine & Rehabilitation,
Taipei Veterans General Hospital between November, 2001 and
April, 2009. This research followed tenets of Declaration of Helsinki.
Past history including head trauma, falls and Meniere’s disease were
reviewed. Information about how dizziness had affected their work,
household and social activities were evaluated by subjects’ self-
rated questionnaires on their first visits.
2.2. Diagnosis
Diagnosis of BPPV was based on the patient’s history, subjective
symptom reports, and objective findings of Dix–Hallpike testing
(sensitivity 82%, specificity 71%) (Lopez-Escamez et al., 2000).
Patients with PC involvement typically reported vertigo when
lying down, rising up from bed, bending forward or tilting their
heads to reach overhead; and patients with HC involvement often
reported vertigo during rolling in bed or horizontal head movement
in the upright position (Steenerson et al., 2005). Each patient’s
semicircular canal involvement was determined by the direction
of nystagmus shown on the infra-red video fixation-block goggles
(Micromedical Computerized Real Eyes infrared video frenzel with
single, pivotal camera, Micromedical Technologies, Illinois, USA)
in the Dix-Hallpike position. An upbeat nystagmus with torsional
component towards the inferior ear confirmed the diagnosis of
PC BPPV. Patients with geotropic (canalolithaisis) or ageotropic
nystagmus (cupulolithiasis) were diagnosed as HC BPPV. Subjects
were grouped into posterior or horizontal canal involvement
on right side, left side or bilateral involvement. Patients who
had geotropic/ageotropic nystagmus in the roll test and torsional
nystamgus upon Hallpike maneuver were grouped as having two-
canal involvement. Those who had symptoms similar to BPPV, but
showed no typical nystagmus in the Dix-Hallpike position, were
grouped as subjective type of BPPV (Tirelli et al., 2001).
2.3. Treatment maneuvers
Posterior canal BPPV was treated by the CRP (Epley, 2001), and
horizontal canal BPPV was treated by the barbecue maneuver
(Lempert and Tiel-Wilck, 1996). Duration of nystagmus less than
60 seconds was diagnosed as canalolithiasis and nystamgus of more
than 60 seconds was cupulolithiasis (Herdman and Tusa, 2007b).
Each patient was treated with either CRP/barbecue maneuver for
canalolithiasis or liberatory maneuver for cupulolithiasis on the
symptomatic side. For those who had simultaneous posterior and
horizontal canal BPPV (two-canal involvement) of the same ear,
PC BPPV was treated first, followed by the barbecue maneuver
48 hours later. For subjective-type BPPV, CRP was performed on
the symptomatic side. No pre-medication or mastoid vibration
was given in our treatment procedures. On their following
visits 3–7 days later, Hallpike examination was performed again.
Treatments were repeated for those who had persistent or recurrent
signs. Brandt-Daroff redistribution exercise was applied for those
who experienced milder or residual complaints of vertigo. Home
program instructions were dispensed as necessary.
2.4. Introduction of canalith repositioning procedure and barbecue
maneuver
The procedure for CRP is as follows: 1. Patient begins in the long-
leg sitting position. 2. The head is rotated 45° towards the affected
side, then lowered down to the supine position, with neck extended
15–20° to the edge of the examination table. 3. Turn head away from
the affected side and bring the other ear down. 4. Lying on the unaf-
fected side of the body, the head is then turned to the ground so that
the patient’s nose is pointing to the ground. 5. Return to the upright
position. Positions 2 to 4 should be held for one minute or until the
nystagmus or vertigo subsides (Figure 1). The Barbecue maneuver:
1. Patient begin in the supine position. 2. Conduct three consecutive
90° head turns toward the unaffected side. 3. End in the starting
position. 4. Each turn was held until the symptom or nystagmus
subsided before proceeding to the next turn. 5. The entire maneuver
was repeated until no symptoms could be elicited (Figure 2).
Fig. 1. Canalith repositioning procedure. (a) Rotate head 45° towards the affected
side, then lower down to supine position, with neck extended 15°-20° to the edge
of the examination table. (b) Turn head away from the affected side and bring the
other ear down. (c) Lie on the unaffected side of the body, and then turn head to
the ground. (d) Back to the upright position.
Fig. 2. The barbeque maneuver (a) Patient in supine position. (b)–(d) Three
consecutive 90° head turns toward the unaffected side. (e) End in starting position.
S52 C-L. Kao et al. / Archives of Gerontology and Geriatrics 49 (2009) S50–S54
2.5. Definition for recurrence
Recurrence of BPPV was defined as recurrent symptoms and signs
of vertigo with positive results in the Dix-Hallpike test after at least
one month of symptom free status.
2.6. Impacts on daily activities
Patients were asked to rate their daily activities limited due
to symptoms caused by BPPV in three perspectives, i.e. work,
household and social activities, ranging from 0 (none) to 10 (most)
on their first visits.
2.7. Statistical analysis
Data was analysed by SPSS 16.0. The Chi-Square test was applied
to analyse the differences of recurrence rate between those aged
above and below 65. The Mann–Whitney U test was used to
evaluate whether there were gender or age differences in the
average duration of first BPPV recurrence. For comparison of the
functional limitation of daily activities between the two age groups,
independent t-test was used.
3. Results
3.1. Demographic data for BPPV patients
Two hundred and eighteen patients were included in this study
(mean age 68.1±14.4 years old, range 24–91 year-old). Past medical
history revealed 45 patients (20.83%) had head trauma and five
(2.35%) had Meniere’s disease. Among the 218 patients diagnosed as
BPPV, 74 were male and 144 were female (1:1.95). One hundred and
seventy-one patients were diagnosed as posterior canal BPPV, in
whom 99 patients had right-side involvement, and 72 patients had
left-side involvement. Eight patients were diagnosed as horizontal
BPPV, seven patients had left-side involvement, and one had right-
side involvement. There were nine patients with subjective-type of
BPPV. Twenty-eight patients had bilateral posterior canal BPPV and
two had two-canal involvement. The demographic data of different
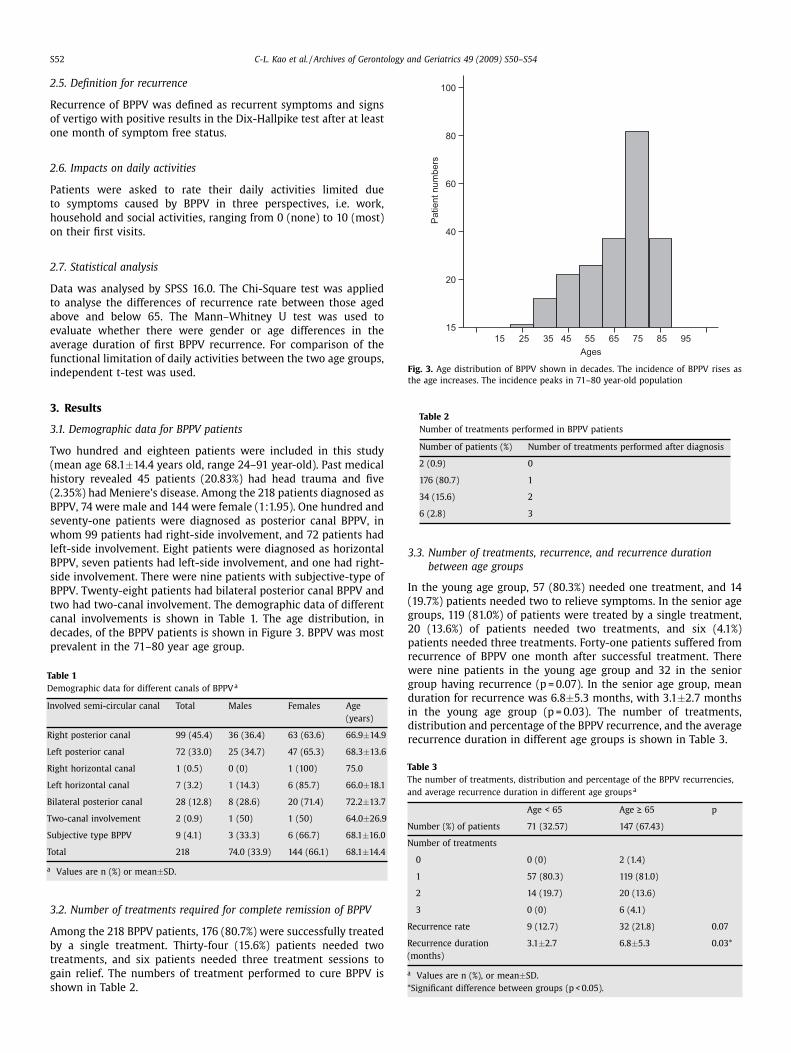
canal involvements is shown in Table 1. The age distribution, in
decades, of the BPPV patients is shown in Figure 3. BPPV was most
prevalent in the 71–80 year age group.
Table 1
Demographic data for different canals of BPPVa
Involved semi-circular canal Total Males Females Age
(years)
Right posterior canal 99 (45.4) 36 (36.4) 63 (63.6) 66.9±14.9
Left posterior canal 72 (33.0) 25 (34.7) 47 (65.3) 68.3±13.6
Right horizontal canal 1 (0.5) 0 (0) 1 (100) 75.0
Left horizontal canal 7 (3.2) 1 (14.3) 6 (85.7) 66.0±18.1
Bilateral posterior canal 28 (12.8) 8 (28.6) 20 (71.4) 72.2±13.7
Two-canal involvement 2 (0.9) 1 (50) 1 (50) 64.0±26.9
Subjective type BPPV 9 (4.1) 3 (33.3) 6 (66.7) 68.1±16.0
Total 218 74.0 (33.9) 144 (66.1) 68.1±14.4
a Values are n (%) or mean±SD.
3.2. Number of treatments required for complete remission of BPPV
Among the 218 BPPV patients, 176 (80.7%) were successfully treated
by a single treatment. Thirty-four (15.6%) patients needed two
treatments, and six patients needed three treatment sessions to
gain relief. The numbers of treatment performed to cure BPPV is
shown in Table 2.
15
15
20
40
60
80
100
25
Ages
Pa
tie
nt
nu
mb
ers
35 45 55 65 75 85 95
Fig. 3. Age distribution of BPPV shown in decades. The incidence of BPPV rises as
the age increases. The incidence peaks in 71–80 year-old population
Table 2
Number of treatments performed in BPPV patients
Number of patients (%) Number of treatments performed after diagnosis
2 (0.9) 0
176 (80.7) 1
34 (15.6) 2
6 (2.8) 3
3.3. Number of treatments, recurrence, and recurrence duration
between age groups
In the young age group, 57 (80.3%) needed one treatment, and 14
(19.7%) patients needed two to relieve symptoms. In the senior age
groups, 119 (81.0%) of patients were treated by a single treatment,
20 (13.6%) of patients needed two treatments, and six (4.1%)
patients needed three treatments. Forty-one patients suffered from
recurrence of BPPV one month after successful treatment. There
were nine patients in the young age group and 32 in the senior
group having recurrence (p =0.07). In the senior age group, mean
duration for recurrence was 6.8±5.3 months, with 3.1±2.7 months
in the young age group (p =0.03). The number of treatments,
distribution and percentage of the BPPV recurrence, and the average
recurrence duration in different age groups is shown in Table 3.
Table 3
The number of treatments, distribution and percentage of the BPPV recurrencies,
and average recurrence duration in different age groupsa
Age < 65 Age ≥ 65 p
Number (%) of patients 71 (32.57) 147 (67.43)
Number of treatments
0 0 (0) 2 (1.4)
1 57 (80.3) 119 (81.0)
2 14 (19.7) 20 (13.6)
3 0 (0) 6 (4.1)
Recurrence rate 9 (12.7) 32 (21.8) 0.07
Recurrence duration
(months)
3.1±2.7 6.8±5.3 0.03*
a Values are n (%), or mean±SD.
*Significant difference between groups (p < 0.05).

C-L. Kao et al. / Archives of Gerontology and Geriatrics 49 (2009) S50–S54 S53
10
8
6
4
2
0
work_VAS household_VAS social_VAS
Daily activities limitation items
Va
lue
age <65
age ≥65
Fig. 4. Impacts on daily activities. For work-related activity limitations: 5.2±3.3 in
the young and 4.1±3.2 in the senior age groups. *Indicates significant difference
between two groups, p < 0.05. For household activity limitations: 5.4±2.5 in the
young and 5.7±2.7 in the senior age groups (p = 0.51). Social activity limitations:
5.6±3.3 in the young and 5.8±2.9 in the senior age groups (p = 0.81).
3.4. Impacts on daily activities
In young and senior age groups, no statistical difference was
found between the subjective feeling of poor balance (p = 0.63), fall
(p = 0.27) and trouble with walking (p = 0.20). The rating of work-
related activity limitation was 5.2±3.3 in the young and 4.1±3.2
in senior age groups (p = 0.03). The rating for household activity
limitation was 5.4±2.5 in the young and 5.7±2.7 in the senior age
groups (p = 0.51). Social activity limitation was 5.6±3.3 in the young
and 5.8±2.9 in the senior age groups (p = 0.81) (Figure 4).
4. Discussion
Our results are in accordance with previous reports (Lynn et al.,
1995; Angeli et al., 2003; Yimtae et al., 2003; Steenerson et al.,
2005), which showed a higher disposition in females of advanced
age, with posterior canal involvement predominating. The incidence
of PC BPPV varies from 76% to 90.2% (Korres et al., 2002; Prokopakis
et al., 2005; Herdman and Tusa, 2007a). It has been proposed that
the incidence of PC BPPV is highest in all canals because PC is
the most gravity-dependent semicircular canal (Korres et al., 2002).
Women are 2.3 times more likely to acquire idiopathic BPPV than
men (1.95 fold in our study) (Katsarkas, 1999). It has been reported
that the age of onset is most commonly seen between 50 and 70
years of age (Mizukoshi et al., 1988; Oas, 2001). According to our
observation, the incidence peaked in the 71–80-year-old age group,
which was older than that reported in the literature. The reason for
this may be due for the fact that our hospital provides services for
both veterans and the civilians, with a high proportion of veterans
visiting the hospital. They are generally older and exclusively male.
This may affect our results for the age distribution and for the male
to female ratio of BPPV occurrence.
Our treatment yielded an 80.7% of success rate after a single
treatment. The treatment efficacy reached 90.8% in PC BPPV (data
not shown). The successful rate of the repositioning maneuver
for posterior canal BPPV ranged from 30% to 100% in one meta-
analysis report (Parnes et al., 2003). Our result was similar to
that of Wolf’s study, which included 102 patients with a 93%
success rate (Wolf et al., 1999). It has been documented that the
secondary causes of BPPV include head trauma, viral labyrninthitis,
Meniere’s disease, migraines and inner ear surgery (Parnes et al.,
2003). In our study, 20.83% of the patients had head trauma
and 2.35% had Meniere’s disease, compared with the 7–17% of
head trauma and 5% Meniere’s reported in the literature (Parnes
et al., 2003). Our incidence of BPPV secondary to other otological
conditions was different because patients’ self-reported past history
might not be accurate. Apart from this, our data did not show
that patients with Meniere’s disease required more treatment
maneuvers, which contradicts with reports that BPPV coinciding
with other vestibular dysfunctions requires more treatment cycles
for a complete symptomatic resolution (Pollak et al., 2002).
Therefore, the value of additional diagnostic tests in the evaluation
of BPPV remains questionable.
Another important issue about BPPV is the recurrence rate.
Our data yielded 18.8% of recurrence rate, which was close to
Furman’s and Prokopakis’ findings (a yearly 15% and 12% recurrence
respectively) (Furman and Cass, 1999; Prokopakis et al., 2005).
Whether right or left side PC BPPV is more prone to recur lacks
a definitive conclusion in previous studies. Our right and left PC
BPPV had approximately the same recurrence rate (16.2% and 16.7%,
respectively), and the bilateral PC BPPV group had the highest
recurrence rate among all canals (35.7%). We found the recurrence
rate in our senior age group was 1.7 times higher than the younger
age group (p =0.07). This finding supports Prokopakis’s conclusion
that age greater than 70 years was the most-identifiable reason
for recurrence, rather than head trauma or vestibular neuropathy
(Prokopakis et al., 2005). The symptom-free duration before BPPV
recurrence was nearly 2.2 times longer in the senior age group
(p =0.03). The reason for this was never proposed in previous
literature, but three possible explanations could be given for this
seemingly contradictory finding. (1) The posterior semicircular
canal is the most commonly involved canal in BPPV. In order to
provoke the symptoms of vertigo, the density and volume of free-
floating clots in the semicircular canals are important factors. It
is possible that older people become less sensitive to the sensory
impulses produced by the free-floating particles and thus BPPV
becomes subclinical. (2) The neck motion in vertical plane in
older people is generally less abrupt and vigorous. Therefore, the
chance for older people to be in triggering positions of PC BPPV
is decreased. (3) Older people are less active, and HC BPPV can be
self-treated when lying on the asymptomatic side.
Previous literature has already documented that BPPV has a
significant impact on the health-related quality of life in elderly
patients (Gamiz and Lopez-Escamez, 2004). In our observation, the
young population perceived significantly more limitations on work-
related functional activities (p = 0.03). The impact on household
and social activities was similar in both age groups. The physical
limitations of BPPV itself can be debilitating. Both young and old
populations had poor balance and trouble with walking, and more
than 20% of them had falls. Whether our patients improved in ADL
functions after treatment were not evaluated in this study.
5. Conclusion
Our study has demonstrated a higher occurrence and recurrence
rate of BPPV in those of senior age. Life quality could be affected by
the violent sensation of vertigo and more than 80% of BPPV patients
could be cured by a single treatment. Although the nature of this
disease is benign, the sequelae of BPPV may be devastating if left
untreated. Early diagnosis and prompt management are mandatory
to facilitate recovery and reduce medical expense.
Conflict of interest statement
The authors have no conflicts of interest to report.
References
Angeli, S.I., Hawley, R., Gomez, O., 2003. Systematic approach to benign paroxys-mal
positional vertigo in the elderly. Otolaryngol. Head Neck Surg. 128, 719–725.
Baloh, R.W., Sloane, P.D., Honrubia, V., 1989. Quantitative vestibular function testing
in elderly patients with dizziness. Ear Nose Throat J. 68, 935–939.

S54 C-L. Kao et al. / Archives of Gerontology and Geriatrics 49 (2009) S50–S54
Brandt, T., Daroff, R.B., 1980. Physical therapy for benign paroxysmal positional
vertigo. Arch. Otolaryngol. Head Neck Surg. 106, 484–485.
Epley, J.M., 2001. Human experience with canalith repositioning maneuvers. Ann. N.
Y. Acad. Sci. 942, 179–191.
Fife, T.D., Iverson, D.J., Lempert, T., Furman, J.M., Baloh, R.W., Tusa, R.U., Hain, T.C.,
Herdman, S., Morrow, M.J., Gronseth, G.S., 2008. Practice Parameter: Therapies for
benign paroxysmal Positional Vertigo (an Evidence-based review). Neurology 70,
2067–2074.
Furman, J.M., Cass, S.P., 1999. Benign paroxysmal positional vertigo. N. Engl. J. Med.
341, 1591–1596.
Gamiz, M.J., Lopez-Escamez, J.A., 2004. Health-related quality of life in patients
over sixty years old with benign paroxysmal positional vergito. Gerontology 50,
82–86.
Hall, S.F., Ruby, R.R., McClure, J.A., 1979. The mechanics of benign paroxysmal vertigo.
J. Otolaryngol. 8, 151–158.
Herdman, S.J., Tusa, R.J., 2007a. Physical therapy management of benign positional
vertigo, in: Herdman S.J. (Eds.), Vestibular Rehabilitation. Davis Company,
Philadelphia F.A., pp. 234.
Herdman, S.J., Tusa, R.J., 2007b. Physical therapy management of benign positional
vertigo, in: Herdman S.J. (Eds.), Vestibular Rehabilitation. Davis Company,
Philadelphia F.A., pp. 252.
Katsarkas, A., 1999. Benign Paroxysmal positional vertigo (BPPV): idiopathic versus
post-traumatic. Acta Otolaryngo. (Stockh). 119, 745–749.
Korres, S., Balatsouras, D.G., Kaeros, A., 2002. Occurrence of semicircular canal
involvement in benign paroxysmal postional vertigo. Otol. Neurotol. 23, 926–932.
Lempert, T., Tiel-Wilck, K., 1996. A positional maneuver for treatment of horizontal-
canal benign positional vertigo. Laryngoscope 106, 476–478.
Lopez-Escamez, J.A., Lopez-Nevot, A., Gamiz, M.J., Moreno, P.M., Bracero, F.,
Castillo, J.L., Salinero, J., 2000. Diagnosis of common causes of vertigo using a
structured clinical history. Acta Otorrinolaringol. Esp. 51, 25–30.
Lopez-Escamez, J.A., Gamiz, M.J., Fernandez-Perez, A., Gomez-Finana, M., 2005. Long-
term outcome and health-related quality of life in benign paroxysmal positional
vertigo. Eur. Arch. Otorhinolaryngol. 262, 507–511.
Lynn, S., Pool, A., Rose, D., Brey, R., Suman, V., 1995. Randomized trial of the canalith
repositioning procedure. Otolaryngol. Head Neck Surg. 113, 712–720.
Mizukoshi, K., Watanabe, Y., Shojaku, H., Okubo, J., Watanabe, I., 1988.
Epidemiological studies on benign paroxysmal positional vertigo in Japan. Acta
Otolaryngol. Suppl. 447, 67–72.
Neuhauser, H., Leopold, M., Von Brevern, M., Arnold, G., Lempert, T., 2001. The
interrelations of migraine, vertigo and migrainous vertigo. Neurology 56, 436–
441.
Oas, J.G., 2001. Genign paroxysmal positional vertigo: a clinician’s perspective. Ann.
N. Y. Acad. Sci. 942, 201–209.
Parnes, L.S., Agrawal, S.K., Atlas, J., 2003. Diagnosis and management of benign
paroxysmal positional vertigo (BPPV). Can. Med. Assoc. J. 169, 681–693.
Pollak, L., Davies, R.A., Luxon, L.L., 2002. Effectiveness of the particle repositioning
maneuver in benign paroxysmal positional vertigo with and without additional
vestibular pathology. Otology & Neurotology 23, 79–83.
Prokopakis, E.P., Chimona, T., Tsagournisakis, M., Christodoulou P, Hirsch, B.E.,
Lachanas, V.A., Helidonis, E.S., Plaitakis, A., Velegrakis, G.A., 2005. Benign
paroxysmal positional vertigo: 10-year experience in treating 592 patients with
canalith repositioning procedure. Laryngoscope 115, 1667–1671.
Schuknecht, H.F., 1969. Cupulolithiasis. Arch Otolaryngol Head Neck Surg. 90, 765–
778.
Semont, A., Freyss, G., Vitte, E., 1988. Curing the BPPV with a liberatory maneuver.
Adv. Otorhinolaryngol. 42, 290–293.
Steenerson, R.L., Cronin, G.W., Marbach, P.M., 2005. Effectiveness of treatment
techniques in 923 cases of benign paroxysmal positional vertigo. Laryngoscope
115, 226–231.
Tirelli, G., D’Orlando, E., Giacomarra, V., Russolo, M., 2001. Benign positional vertigo
without detectable nystagmus. Laryngoscope 111, 1053–1056.
Wolf, J.S., Boyev, K.P., Manokey, B.J., Mattox, D.E., 1999. Success of the modified
Epley maneuver in treating benign paroxysmal positional vertigo. Laryngoscope
109, 900–903.
Yimtae, K., Srirompotong, S., Sae-Seaw, P., 2003. A randomized trial of the canalith
repositioning procedure. Laryngoscope 113, 828–832.