Embed Size (px)
Citation preview
Clinical leadership in teams in the ED
Sissel Eikeland Husebø, Post doctor,
University of Stavanger and Stavanger University Hospital
SimPro 2015
24.-25.8.2015, Jyväskylä, Finland
The ED at Stavanger University Hospital
Øystein Evjen Olsen, Chief Medical Officer
Triages approximately 30 000 patients per year
120 ICNs and RNs
40 physicians
Triage unit, 14 beds
Background Evaluation report from The regional office of the
Norwegian Board of Health Supervision in 2008
Conclusion follow-up report (2013): Inadequate
presence of qualified medical personnel
Response: A Steering Committee involving the top
leadership of the hospital and working groups
Rationale for the Clinical Leadership in
Teams course No presence of experienced medical doctors and nurses
(Doan et al. 2011)
The role of the nurse-in-charge has been reformulated
Senior doctors are not physically
present (Bjørnsen & Uleberg, 2012)
Healthcare education models do
not focus on the importance
of CL (Guedes dos Santos et al. 2013)
Reformulating the concept of CL
Health policy developments within the Norwegian
health care system
◦ A separate specialty in Emergency Medicine
◦ Development of separate municipal emergency care facilities
◦ New guidelines for the service levels, availability and
distribution of emergency services countrywide
◦ The Norwegian Board of Health Supervision (2008, 2013)
give hospitals in general, and SUH in particular, no other
options but to improve CL skill
Clinical leadership Lacking a standard definition and
poorly understood (Mannix et al.
2013)
Driving service improvement and
management of teams (Cook & Holt
2008)
Leadership skills for team building,
confidence in and respect for others
(McNamara et al. 2011)
Facilitating evidence-based practice
and improved patient outcomes
(Millward & Bryan 2005)
A prerequisite for quality of care and
patient safety (Dickinson & Ham
2008)
Defining Clinical Leadership –
Four core bedside values Trust Quality Responsiveness Efficiency
Trust (Giddens 1994)
Quality(Institute of Medicine Committee
on Health, 1990)
Responsiveness (WHO 2000)
Efficiency(Øvretveit 2005)
Definition of Clinical leadership:
“to take responsibility for clinical decision-making, within the
scope of your role in a clinical team at any given time, with
a patient-centred perspective addressing four key values; 1)
trust 2) quality 3) responsiveness 4) efficiency”
(Olsen et al. 2015)

Collaborative process – who
was involved?
Øystein Evjen Olsen Sigrunn Anna Qvindesland Helge Lorentzen
Development of the course
1) Align team training objectives and safety aims with
organizational goals
2) Provide organizational support for the team training
initiative
3) Get frontline care leaders on board
4) Prepare the environment and trainees for team training
5) Determine required resources and time commitment and
ensure their availability
6) Facilitate application of trained teamwork skills on the job
7) Measure the effectiveness of the team training program
(Salas et al. 2009)
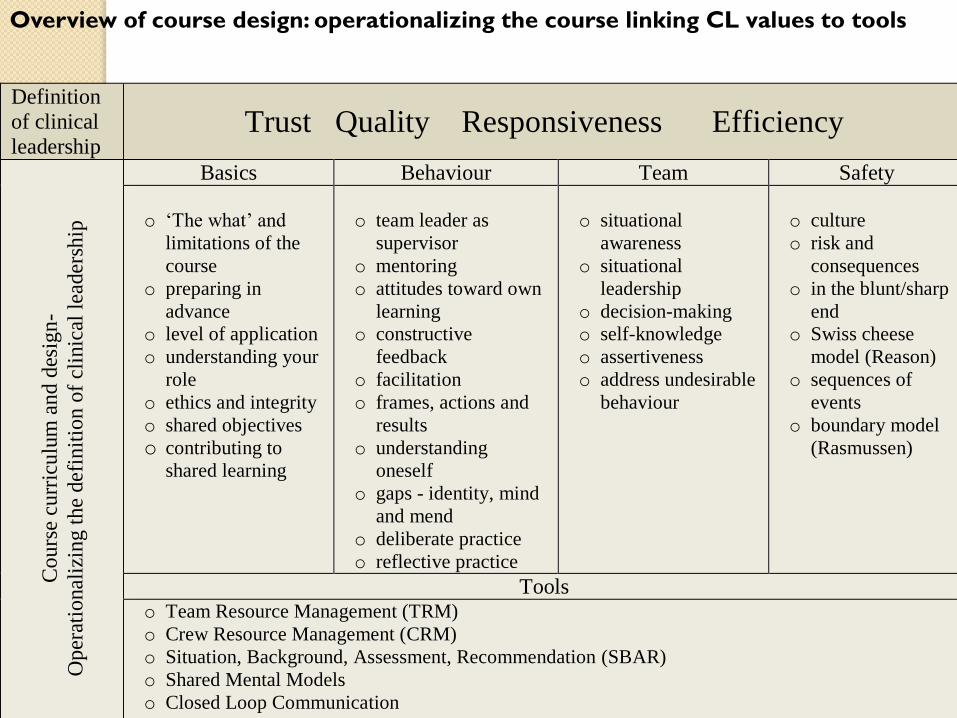
Definition
of clinical
leadership Trust Quality Responsiveness Efficiency
Cours
e cu
rric
ulu
m a
nd d
esig
n-
Oper
atio
nal
izin
g t
he
def
init
ion o
f cl
inic
al l
eader
ship
Basics Behaviour Team Safety
o ‘The what’ and
limitations of the
course
o preparing in
advance
o level of application
o understanding your
role
o ethics and integrity
o shared objectives
o contributing to
shared learning
o team leader as
supervisor
o mentoring
o attitudes toward own
learning
o constructive
feedback
o facilitation
o frames, actions and
results
o understanding
oneself
o gaps - identity, mind
and mend
o deliberate practice
o reflective practice
o situational
awareness
o situational
leadership
o decision-making
o self-knowledge
o assertiveness
o address undesirable
behaviour
o culture
o risk and
consequences
o in the blunt/sharp
end
o Swiss cheese
model (Reason)
o sequences of
events
o boundary model
(Rasmussen)
Tools o Team Resource Management (TRM)
o Crew Resource Management (CRM)
o Situation, Background, Assessment, Recommendation (SBAR)
o Shared Mental Models
o Closed Loop Communication
o Communication processes
Overview of course design: operationalizing the course linking CL values to tools
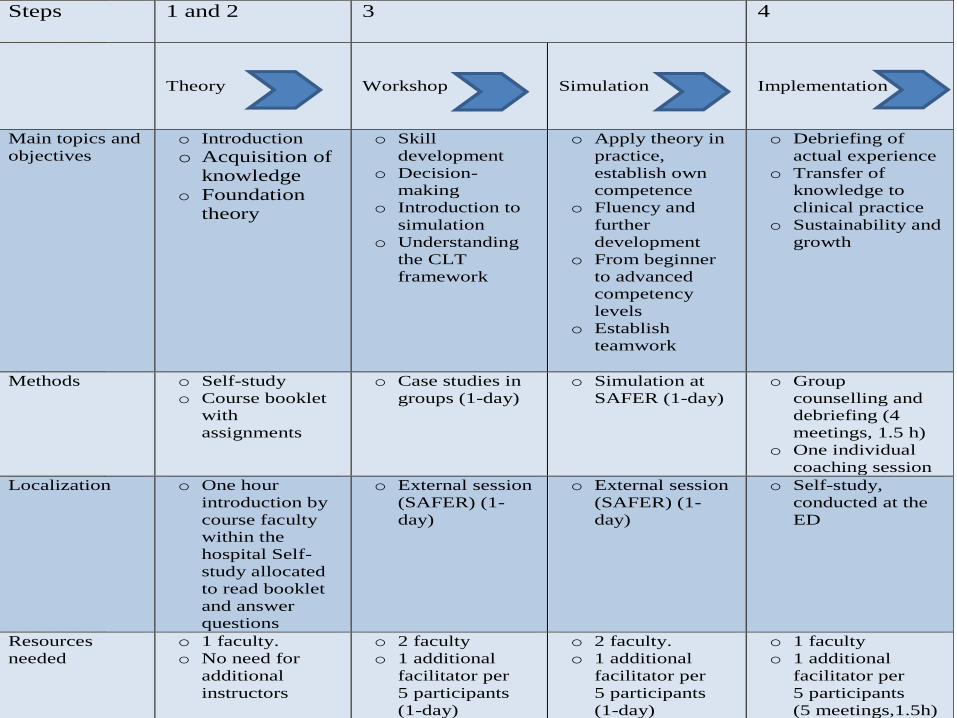
Steps
1 and 2 3
4
Theory
Workshop
Simulation
Implementation
Main topics and
objectives
o Introduction
o Acquisition of
knowledge
o Foundation
theory
o Skill
development
o Decision-
making
o Introduction to
simulation
o Understanding
the CLT
framework
o Apply theory in
practice,
establish own
competence
o Fluency and
further
development
o From beginner
to advanced
competency
levels
o Establish
teamwork
o Debriefing of
actual experience
o Transfer of
knowledge to
clinical practice
o Sustainability and
growth
Methods o Self-study
o Course booklet
with
assignments
o Case studies in
groups (1-day)
o Simulation at
SAFER (1-day)
o Group
counselling and
debriefing (4
meetings, 1.5 h)
o One individual
coaching session
Localization o One hour
introduction by
course faculty
within the
hospital Self-
study allocated
to read booklet
and answer
questions
o External session
(SAFER) (1-
day)
o External session
(SAFER) (1-
day)
o Self-study,
conducted at the
ED
Resources
needed
o 1 faculty.
o No need for
additional
instructors
o 2 faculty
o 1 additional
facilitator per
5 participants
(1-day)
o 2 faculty.
o 1 additional
facilitator per
5 participants
(1-day)
o 1 faculty
o 1 additional
facilitator per
5 participants
(5 meetings,1.5h)
Workshop
day 1
How does the ED
look like?
Who is
communicating
with who?
Scenarios S1. Limited trauma with chest pain S2. Lack of resources/overcrowding in units S3: Prolonged length of stay S4: Unclarified patient S5: Bullying at work S6: Medication error with consequences
Trust
Quality
Responsiveness
Efficacy
S1. Limited trauma with chest pain
Objectives
Identification of prioritized
interventions
Leadership
Teamwork
Short description
A female, 68 years old, with
no known medical history,
fell on bike downhill is
transported to the ED in
ambulance
S2. Lack of resources/overcrowding in the units
Objectives
situational awareness
apply leadership techniques
Short description
A male, 45 years old, afebrile
with a lot of coughing and
atrial flutter. He needs cardiac
monitoring, but no relevant
units have bed space
S3: Prolonged length of stay in the ED
Objectives
identification of responsible
professional for the patient
ensuring progress
prioritizing actions and
distribution of resources
Short description
An 85 year old demented female,
accompanied by her daughter, is
admitted five o’clock in the
afternoon with suspected
femoral neck fracture. Eight
o’clock the next morning she is
still in the ED waiting for a
clinical decision to be made
S4: Unclarified patient
Objectives
collaborate with relevant
specialities to make a
decision regarding the
patient
Short description
A female, aged 52 is
brought to the ED by her
husband with suspected
chest pain and syncope.
During examination an
ankle fracture is detected
S5: Bullying at work
Objectives
defusing and professional guidance on the shift
maintaining progress and flow
Short description
A doctor realizes a colleague has been bullied by her senior doctor. She is distracted and distraught reducing her ability to function during the shift.
S6: Medication error with consequences
Objectives
defusing and professional guidance on busy shift
handling breaches in procedures with potentially serious consequences during a shift
Short description
A nurse and doctor were involved in a medication error with serious consequences due to a misunderstanding
Research protocol
Clinical Leadership in Teams course in the ED
AimTo evaluate the impact of a CLT course on quality, efficiency, responsiveness of health care services and interprofessional trust
Study design
Trailing research Multiple quantitative and qualitative
methods Pre-test and post-test Formative evaluation
(Song et al. 2010)
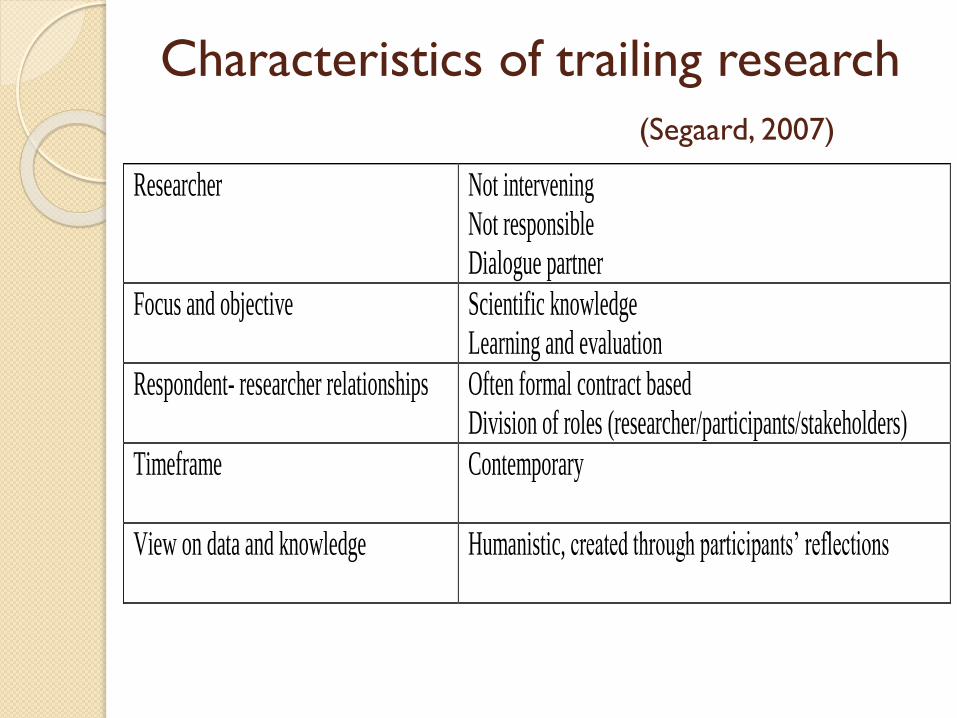
Characteristics of trailing research
(Segaard, 2007)
Researcher Not intervening
Not responsible
Dialogue partner
Focus and objective Scientific knowledge
Learning and evaluation
Respondent- researcher relationships Often formal contract based
Division of roles (researcher/participants/stakeholders)
Timeframe Contemporary
View on data and knowledge Humanistic, created through participants’ reflections
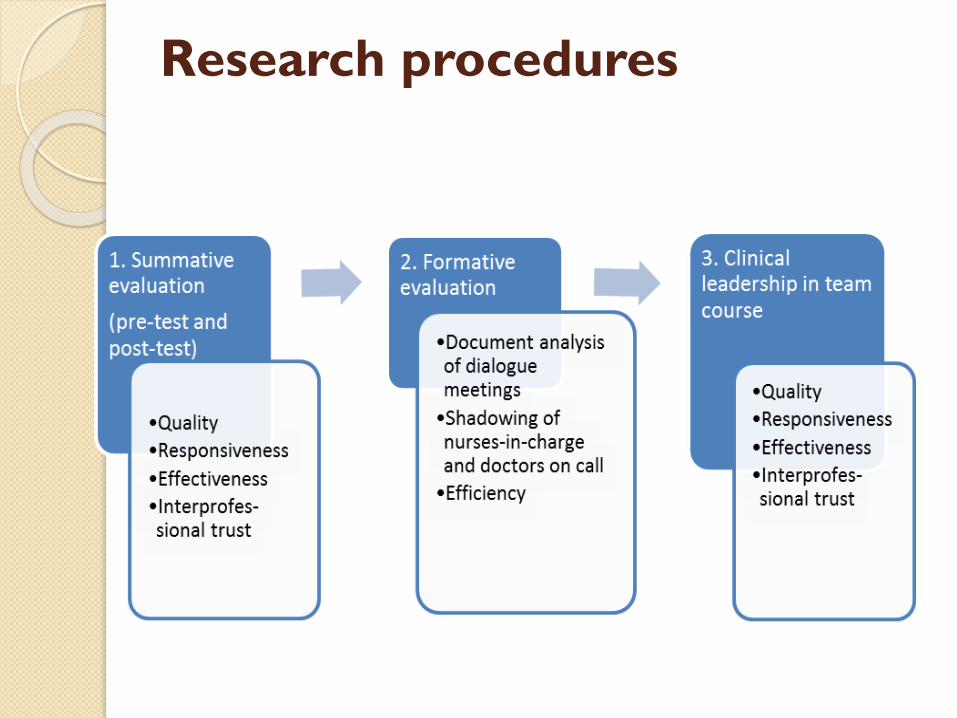
Research procedures
DISCUSSION AND CONCLUSION
The definition of CL is reformulated
not based on empirical evidence
Close link to hospital, Norwegian, European and
global health policy
Rooted in the actual clinical setting of the participants
Improvement in patient-centered care and workforce
satisfaction