Embed Size (px)
DESCRIPTION
Clinical presentation of renal diseases. The presence of renal disease in a patient may be detected because of:. 1. presentation with a symptom or clinical sign that indicates an underlying renal disorder; 2. the presence of a systemic disease known to involve the kidneys; - PowerPoint PPT Presentation
Citation preview
Clinical presentation of renal diseases
The presence of renal disease in a patient may be detected because of:
1. presentation with a symptom or clinical sign that indicates an underlying renal disorder;
2. the presence of a systemic disease known to involve the kidneys;
3. a family history of inherited renal disease;4. the finding of asymptomatic urinary
abnormalities or disordered renal function tests.
Asymptomatic urinary abnormalities
• Asymptomatic proteinuria• Microalbuminuria• Microscopic haematuria
Asymptomatic proteinuria• Urinary protein excretion can amount to 150 mg daily in
normal persons, consisting of albumin, Tamm–Horsfall protein and secretory IgA.
• An accurate 24-h urine collection is difficult to obtain, particularly in outpatients, and therefore it is frequently more convenient to estimate the urinary protein/creatinine ratio on a mid-morning sample of urine, a normal value would be less than 130 (as this is a ratio it is without units). Approximately half consists of low molecular weight proteins or protein fragments, with the rest being albumin.
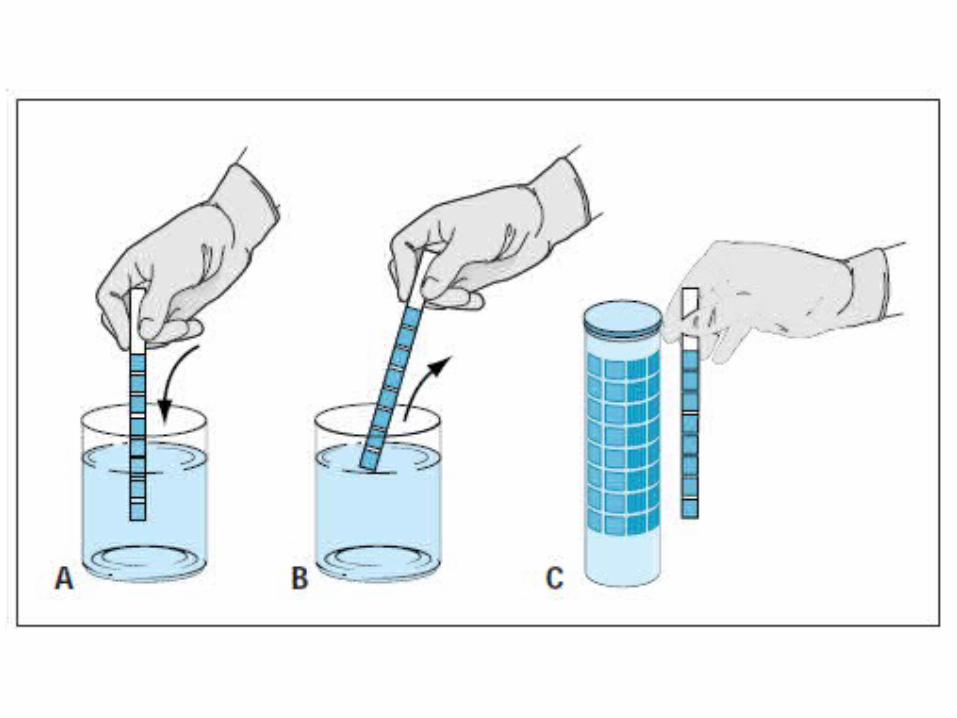
• The most common method of detecting proteinuria is by using dipstix. These paper strips are impregnated with tetrabromophenol blue which changes colour from yellow-green to blue-green in the presence of protein.
• This test is very observer-dependent and it should be remembered that Bence-Jones protein will not be detected and that false-positive results can occur both in alkaline urine and in urine contaminated with antiseptics
• Urinary protein excretion can increase during pyrexial illnesses, with strenuous exercise, congestive cardiac failure and hypertension.
• In such patients the proteinuria is commonly mild (generally less than 1.5 g daily) and resolves with remission of the underlying cause.
• If proteinuria is detected in these circumstances the test should be repeated once the potential cause has resolved.
• If persistent proteinuria is detected then further investigation to determine the nature of the underlying disease is indicated.
Microalbuminuria• 'Microalbuminuria' is the term used for urinary protein
excretion greater than normal but still less than that detectable by dipstix testing.
• The excretion of more than 30 μg/min of albumin in an overnight collection or 70 μg/min in a 24-h collection in a patient with diabetes mellitus is indicative of early diabetic nephropathy.
• It is, however, not specific for diabetes: microalbuminuria may also be present in hypertension, obesity, systemic lupus erythematosus, and following exercise.
• Specifically designed stix tests are now available for screening purposes, but these remain only semiquantitative.
Microscopic haematuria• There is no agreed definition of microscopic haematuria
as all urine samples contain some red blood cells. • The Scottish Intercollegiate Guideline Network (SIGN)
has suggested the presence of a positive result on dipstix testing and/or the presence of more than five red blood cells per high-power field on urine microscopy.
• Asymptomatic microscopic haematuria is occult haematuria, however detected and excludes haematuria visible to the naked eye or associated with urinary tract pain, infection or other symptom.
• The further investigation of a patient found to have asymptomatic haematuria depends on a number of factors.
• As haematuria can arise from any part of the urinary tract from the glomerulus to the urethra, the first issue is to determine whether further investigations should be urological or nephrological.
• In men, particularly those over the age of 50 years, it is most likely that urological investigations will be required because of the increasing incidence of prostatic problems and urothelial malignancy and in such patients clinical examination must include a rectal examination to determine whether any prostatic abnormality can be detected.
• By contrast, the presence of significant proteinuria, clinical evidence of renal disease and/or impaired renal function indicate the need for nephrological investigation.
• Urine microscopy can be of value if performed on a fresh sample. Red cell casts are diagnostic of glomerular bleeding and do not arise from bleeding anywhere else in the renal tract.
• Consideration of the morphology of red cells in the urine can also be useful: dysmorphic red cells, in particular those appearing as a ring form with bubbles, are probably the consequence of glomerular bleeding, whereas red cells of normal appearance are more likely to arise from a site in the lower urinary tract.
• However, discrimination is not always straightforward, considerable interobserver variability is reported and the technique is not robust enough to be routinely applied in most centres.
Symptomatic presentations
• Acute nephritic syndrome (haematoproteinuria syndrome)
• Nephrotic syndrome• Disorders of micturition• Pain• Disorders of renal function
Disorders of micturition
• Polakiuria• Nocturia• Dysuria• Polyuria• Olyguria and anuria
Polakiuria• Is the term applied when the bladder is emptied more
often than normal, hence in obtaining a history it is therefore necessary to determine how often the patient passes urine.
• This may be associated with a normal or increased 24-hour urine volume.
• It is important to distinguish between these two situations as frequency in the presence of a normal output indicates a bladder (lower urinary tract) problem, whereas an increase in output is indicative of a disorder of urinary concentration or excessive fluid intake
Nocturia • Nocturia may arise from the many conditions that cause
frequency. • On lying down there is an increase in renal perfusion resulting
in increased urine flow, but ADH is secreted during sleep, thereby increasing urinary concentration and meaning that urine volume diminishes during sleep. In patients with sleep disturbance there is less ADH production and thus urine concentration is reduced, with increased urine volume such that nocturia may occur.
• Enquiry should be made regarding sleep patterns in patients presenting with nocturia, in addition to considering those conditions that cause polyuria and frequenc
Dysuria
• Dysuria is pain or discomfort on micturition and one of the most frequent symptoms, accounting for about 2% of consultations in primary care.
• It is more common in women and is usually described as a burning, scalding or tingling sensation in the urethra or at the urethral meatus occurring during or immediately after micturition.
• Most commonly it is due to urinary infection, but it may also be caused by chemical irritation such as rarely occurs with cyclophosphamide. If associated with frequency and urgency of micturition it indicates bladder irritation such as cystitis. In young women this is usually associated with sexual activity, but in older persons it may indicate a lesion in the bladder or prostate.
• Prostatic inflammation usually gives rise to perineal or rectal pain. • Very young children will be unable to complain of dysuria but urethral
irritation may be inferred if the child cries during micturition.
Polyuria
• Polyuria is an increase in the daily volume of urine and may arise from a number of different conditions. The normal daily urine volume varies considerably depending on fluid intake and insensible loss, but is normally in the range of 1 to 2 litres.
• An increase in solute load, most commonly due to hyperglycaemia, reduces tubular reabsorption and increases urine production. Inadequate ADH secretion, such as following a head injury or associated with tumours or infection, result in an impaired urinary concentration and increased output (central diabetes insipidus).
• Conditions that impair the tubular response to ADH, such as potassium depletion, lithium toxicity and some rare inherited diseases, also increase urine volume (nephrogenic diabetes insipidus), as do renal disorders that impair medullary concentration, such as analgesic nephropathy, papillary necrosis, medullary cystic disease and nephrocalcinosis.
Olyguria and anuria• Oliguria is a reduction in urine volume to such an extent that
there is inability to excrete the residues of normal daily metabolic functions.
• This normally means to a volume of less than 500 ml daily in an adult, usually indicating acute renal failure of whatever cause.
• Anuria is the lack of any urine output and is indicative of obstruction, although it may occur in some forms of severe acute renal failure.
• If anuria is present it is essential to perform a rectal examination to determine if there is any pelvic malignancy, such as a rectal or cervical carcinoma, to account for the obstruction.
Renal pain• Stretching of the capsule of the kidney causes renal pain
that is felt in the loin ('renal angle'). • It can be produced by any condition that distends the
kidney, such as inflammation, mass lesions or an obstruction.
• The last is the most common cause, particularly obstruction of the pelviureteric junction, when the patient may give a history that anything that causes an acute increase in urine volume (for example, drinking a large quantity of water, beer, or lager or taking a diuretic) precipitates the pain.
Renal pain• Inflammatory pain, such as in pyelonephritis and
(uncommonly) in glomerulonephritis, develops gradually, is usually constant in nature and is variable in severity.
• A perirenal abscess, which may not always be associated with fever or tenderness, can give rise to symptoms and signs of diaphragmatic irritation and/or psoas irritation.
• In the latter case, the patient usually prefers to rest with the hips flexed and reports that extension of the hips is accompanied by an increase in pain.
Renal pain• It can be difficult to distinguish renal pain from
musculoskeletal pain, hence the history should enquire specifically about the relationship of pain to movement or position, neither of which greatly affects renal pain.
• Clinical examination of the back and spine should determine any limitation of movement or localized point tenderness, which would suggest a musculoskeletal problem.
• Some patients with polycystic renal disease complain of a constant dull loin ache. They may also suffer from the sudden onset of renal pain if there is bleeding into a cyst, or from pain of a more gradual onset if there is cyst infection.
Ureteric colic• Pain arising from an acute obstruction is frequently sudden in onset,
severe, colicky and may radiate to the groin, scrotum, labia or upper thigh.
• Many describe it as 'the worst pain that they have ever had' and the patient with ureteric colic typically thrashes about, unable to find comfort, looks pale and sweaty and often vomits, which can lead to diagnostic confusion.
• The pain is due to acute distention of the pelvis of the kidney and the upper ureter and the associated increased peristalsis. If the obstruction is ureteric the pain resolves rapidly once the cause is extruded into the bladder, although when in the bladder it may result in bladder irritation with strangury or further obstruction if it becomes impacted at the urethral orifice.
Renal colic
• Sudden onset• Very intense• Antalgic position• Unilateral• Lasts for minutes, hours, days (rare)• Precipitated by phisical effort, trepidations, wattery
diet, heat• Accompanied by urinary , digestive, circulatory
symptoms
Phisical exam
• Anxiety• Agitated• Antalgic position
• + Giordano
Causes
• Nephrolithyasis• Cancer• Renal tuberculosis• Renal trauma• Sulphamide and cytostatics intake
Ureteric colic
• The most common differential diagnoses of right-sided renal colic are biliary colic and appendicitis: diagnostic difficulty is less likely on the left side, although colonic pain requires consideration.
• Chronic obstruction may be surprisingly asymptomatic. Retroperitoneal fibrosis is accompanied by a dull-aching back discomfort but is not associated with colic in spite of an obstruction.
Non-colicative lumbar pain(renal origin)
• Acute – without irradiation, without disorders of micturition : APN, AGN
• Chronic – lower intensity: CGN, renal tuberculosis
• Differential diagnosis: muscular back pain (lumbago), hernia, spondilitis, spondilosis
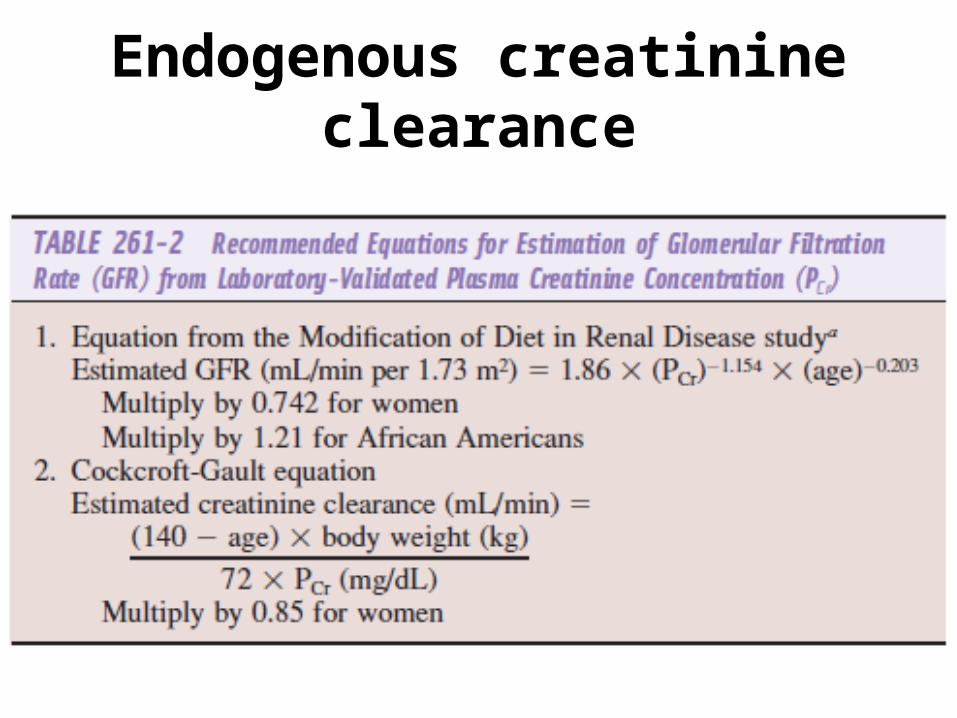
Endogenous creatinine clearance
NEPHRITIC SYNDROME
Definition
• This clinical syndrome typically presents with clinical findings of hematuria, proteinuria and dysmorphic red blood cells and/or red blood cell casts.
• The proteinuria can range from 200 mg per day to heavy proteinuria (greater than 10 grams per day). <3.5 g/day
• Clinically, it is accompanied by hypertension and edema.
Assessment
• In cases in which the nephritic syndrome is the predominant clinical presentation, a search for systemic diseases is warranted.
• The history and physical exam should particularly focus on the assessment of rashes, lung disease, neurologic abnormalities, evidence of viral or bacterial infections, and musculoskeletal and hematologic abnormalities.
• Laboratory assessment should be tailored to the clinical findings in the history and physical examination.
Clinical findings
• Not all four clinical features may be present simultaneously.
• In some patients there is oedema due to salt and water retention in the oliguric phase.
• Encephalopathy, particularly in children, may occur due to hypertension or electrolyte disorders such as hyponatraemia.
• Hypertension is variable and oliguria depends to a large extent on the degree of glomerular involvement.
Urine exam
• The urine typically appears 'smoky' due to the presence of red blood cell casts and rarely it will appear frankly red.
• Proteinuria is variable in amount.
Causes • The 'classical' cause of acute nephritis is poststreptococcal
glomerulonephritis and other infective causes . • However, these diseases are becoming less common,
particularly in developed countries and it is more usual to see patients who have proteinuria and haematuria accompanied by variable hypertension and renal functional impairment in whom no identifiable preceding infection can be identified.
• The presence of blood and protein in the urine is a sign of glomerular inflammation and is not indicative of any particular glomerular pathology.
• On investigation such patients have a wide variety of glomerular appearances , hence renal biopsy is essential for precise diagnosis.
Laboratory
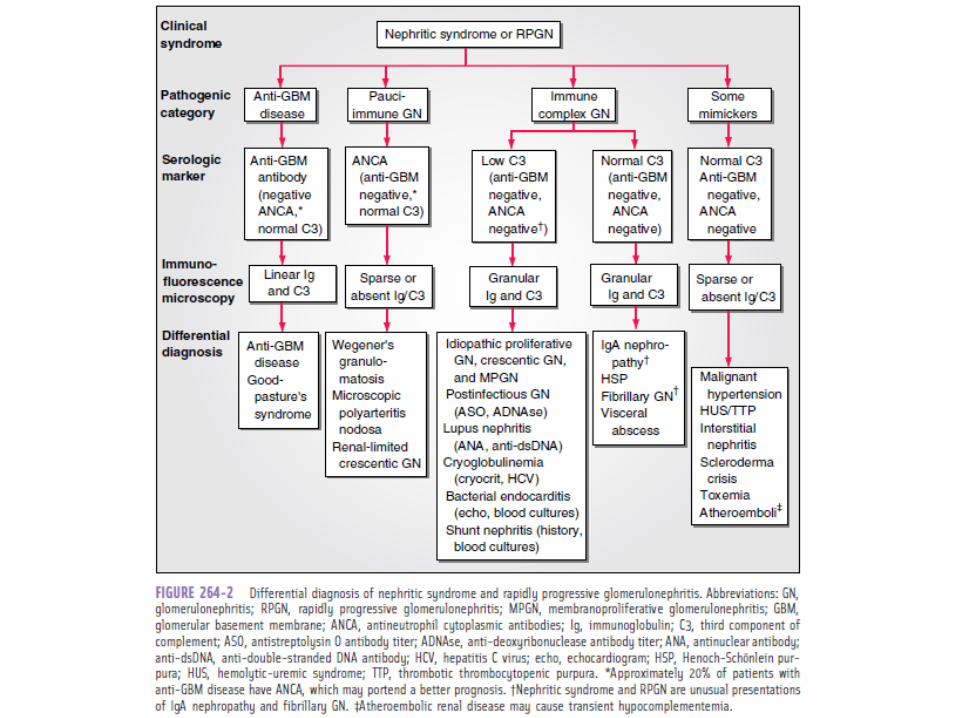
• A complete blood count (CBC), electrolyte panel, 24-hour urine collection for protein and creatinine clearance, and liver function tests should be obtained initially. Serum complement (C3) levels are often clinically helpful to assist in the diagnosis of a specific renal disease (Table 9-5).
Immunology
• Further laboratory assessment may be performed based on these findings, and may include an anti-streptolysin (ASO) titer, antinuclear antibody (ANA), antineutrophil cytoplasmic antibodies (ANCA), cryoglobulins, and/or an anti-GBM antibody. These early assessments may provide a presumptive diagnosis and should lead the clinician to an appropriate therapeutic intervention while awaiting renal biopsy results.
Renal biopsy
• tissue diagnosis confirms the clinical findings and provides information regarding the acuity and chronicity of the disease process can a glomerular disease can be properly managed
Acute glomerulonephritis• inflammatory process causing renal dysfunction over days
to weeks that may or may not resolve• If the inflammatory process is severe, the
glomerulonephritis may lead to a greater than 50% loss of nephron function over the course of just weeks to months.
• Such a process, called rapidly progressive glomerulonephritis, can cause permanent damage to glomeruli if not identified and treated rapidly.
• Prolonged inflammatory changes can result in chronic glomerulonephritis with persistent renal abnormalities that progress to ESRD.
Symptoms and Signs
• Edema is first seen in regions of low tissue pressure such as the periorbital and scrotal areas.
• Hypertension, if present, is due to volume overload rather than vasoactive substances such as angiotensin II, whose levels are low.
Laboratory Findings
• Serum chemistries• Urinalysis• Biopsy
Serum chemistries
• There are no serum chemistries characteristic of nephritic syndrome, but certain special tests are often performed depending on the history and the results of the preliminary evaluation.
• These include complement levels, antinuclear antibodies (ANA), cryoglobulins, hepatitis serologies, ANCA, anti-GBM antibodies, antistreptolysin O (ASO) titers and C3 nephritic factor.
Urinalysis
• The urinalysis shows red blood cells. These may be misshapen from traversing a damaged capillary membrane—so-called dysmorphic red blood cells.
• Red blood cell casts and moderate degrees of proteinuria are also characteristic of the urinary sediment.
• Placing the patient in a lordotic position for an hour increases sensitivity for finding red cell casts in the next urine specimen.
Biopsy
• Renal biopsy should be considered if there are no other contraindications to biopsy (eg, bleeding disorders, thrombocytopenia, uncontrolled hypertension).
• Rapidly progressive glomerulonephritis is likely when over 50% of glomeruli contain crescents.
• The type of disease can be categorized according to the immunofluorescent pattern and appearance on electron microscopy
Essentials of Diagnosis
• Edema. • Hypertension. • Hematuria (with or without dysmorphic red
cells, red blood cell casts).
Nephrotic syndrome
Definition • Another major cause of edema is nephrotic syndrome, the
clinical hallmarks of which include proteinuria (>3.5 gm per day), hypoalbuminemia, hypercholesterolemia and edema.
• The degree of the edema may range from pedal edema to total body anasarca, including ascites and pleural effusions.
• The lower the plasma albumin concentration, the more likely the occurrence of anasarca; the degree of sodium intake is, however, also a determinant of the degree of edema.
Causes
• Systemic causes include diabetes mellitus, lupus erythematosus, drugs (e.g., phenytoin, heavy metals, NSAIDs), carcinomas and Hodgkin's disease
• Primary renal diseases such as minimal change nephropathy, membranous nephropathy, focal glomerulosclerosis and membranoproliferative glomerulonephritis.
Pathogenesis
• Traditionally, ECF volume expansion in nephrotic syndrome was believed to depend on hypoalbuminemia and underfilling of the arterial circulation. Several observations have raised questions about this hypothesis
Pathogenesis
• First, the interstitial oncotic pressure in normal individuals is higher than previously appreciated. Transudation of fluid during ECF volume expansion reduces the interstitial oncotic pressure, thus minimizing the change in transcapillary oncotic pressure.
Pathogenesis
• Second, patients recovering from minimal-change nephropathy frequently begin to excrete sodium before their serum albumin concentration rises.
• Third, the circulating concentrations of volume-regulatory hormones are not as high in nephrotic patients as in patients with severe cirrhosis or congestive heart failure. These and other observations have suggested a role for primary renal NaCl retention in the pathogenesis of nephrotic edema.
Hypoalbuminemia
• is compounded further by increased renal catabolism and inadequate, albeit usually increased, hepatic synthesis of albumin
• the greater the proteinuria, the lower the serum albumin level
Hyperlipidemia• Is believed to be a consequence of increased hepatic
lipoprotein synthesis that is triggered by reduced oncotic pressure and may be compounded by increased urinary loss of proteins that regulate lipid homeostasis.
• Defective lipid catabolism is also thought to play an important role. Low-density lipoproteins and cholesterol are increased in the majority of patients, whereas very low density lipoproteins and triglycerides tend to rise in patients with severe disease.
• Although not proven conclusively, hyperlipidemia may accelerate atherosclerosis and progression of renal disease.
Hypercoagulability
• Is probably multifactorial in origin and is caused, at least in part, by increased urinary loss of antithrombin III, altered levels and/or activity of proteins C and S, hyperfibrinogenemia due to increased hepatic synthesis, impaired fibrinolysis and increased platelet aggregability.
• As a consequence of these perturbations, patients can develop spontaneous peripheral arterial or venous thrombosis, renal vein thrombosis and pulmonary embolism.
Other metabolic complications of nephrotic syndrome include
• Protein malnutrition and iron-resistant microcytic hypochromic anemia due to transferrin loss
• Hypocalcemia and secondary hyperparathyroidism can occur as a consequence of vitamin D deficiency due to enhanced urinary excretion of cholecalciferol-binding protein, whereas loss of thyroxine-binding globulin can result in depressed thyroxine levels.
• An increased susceptibility to infection may reflect low levels of IgG that result from urinary loss and increased catabolism.
• In addition, patients are prone to unpredictable changes in the pharmacokinetics of therapeutic agents that are normally bound to plasma proteins.
Proteinuria
• It should be stressed that the key component of nephrotic syndrome is proteinuria, which results from altered permeability of the glomerular filtration barrier for protein, namely the GBM and the podocytes and their slit diaphragms.
• The other components of the nephrotic syndrome and the ensuing metabolic complications are all secondary to urine protein loss and can occur with lesser degrees of proteinuria or may be absent even in patients with massive proteinuria.
Six entities account for 90% of cases of nephrotic syndrome in adults
• minimal change disease (MCD)• focal and segmental glomerulosclerosis (FSGS)• membranous glomerulopathy• membranoproliferative glomerulonephritis
(MPGN)• diabetic nephropathy• amyloidosis
Essentials of Diagnosis
• Urine protein excretion > 3.5 g/1.73 m2 per 24 hours.
• Hypoalbuminemia (albumin < 3 g/dL). • Peripheral edema.
Poststreptococcal acute glomerulonephritis
• Beta hemolytic group A streptococcus, type 4,12,23,25
• At 7-12 days after streptococcal infection• Pro-s: - history of infection - epidemiology - streptococcus positive cultures - ↑ASLO
Predisposing factors
• Age – maximum incidence at 5-10 yrs• Sex – men>women• Cold• Fatigue
Pathogenesis
• Circulating immune complexes accumulated in glomeruli – inflammatory reaction
Onset • Sudden (rare) – fever - chills - headache - vomiting - lumbar pain - olyguria• Insidious (frequent) – malaise - anorexia - low fever - lumbar pain
Urinary syndrome
• Olyguria• High urine density• Medium proteinuria (2-3 g/24h)• Hematuria (micro/macroscopic)• Casts
Cardio-vascular syndrome
• HBP• Bradicardia• Heart failure• Ecg: T wave aplatization, ↓ ST, rithm
disorders
Edema
• White, smooth• For the beginning – face (eyelids, periorbitary
region)• Limbs, generalised
Neurological disorders
• Amaurosis• Vomiting• Headache• Seizures
Chronic glomerulonephritis
• Microscopic hematuria• Medium proteinuria• Absence of edema (except when nephrotic
syndrome)• Signs of renal failure (advanced stages)
Urinary tract infections
Classification
• Acute infections of the urinary tract can be subdivided into two general anatomic categories: lower tract infection (urethritis and cystitis) and upper tract infection (acute pyelonephritis, prostatitis and intrarenal and perinephric abscesses).
Cystitis
• Patients with cystitis usually report dysuria, frequency, urgency, and suprapubic pain.
• The urine often becomes grossly cloudy and malodorous, and it is bloody in 30% of cases.
Acute pielonephritis
• Symptoms of acute pyelonephritis generally develop rapidly over a few hours or a day and include a fever (39-40 C), shaking chills, nausea, vomiting and diarrhea.
• Symptoms of cystitis may or may not be present.• Besides fever, tachycardia and generalized muscle
tenderness, physical examination reveals marked tenderness on deep pressure in one or both costovertebral angles or on deep abdominal palpation.
• In some patients, signs and symptoms of gram-negative sepsis predominate.
• Most patients have significant leukocytosis and bacteria detectable in Gram-stained unspun urine.
• Piuria and leukocyte casts are present in the urine of some patients and the detection of these casts is pathognomonic.
• Hematuria may be demonstrated during the acute phase of the disease; if it persists after acute manifestations of infection have subsided, a stone, a tumor or tuberculosis should be considered.
Diagnosis
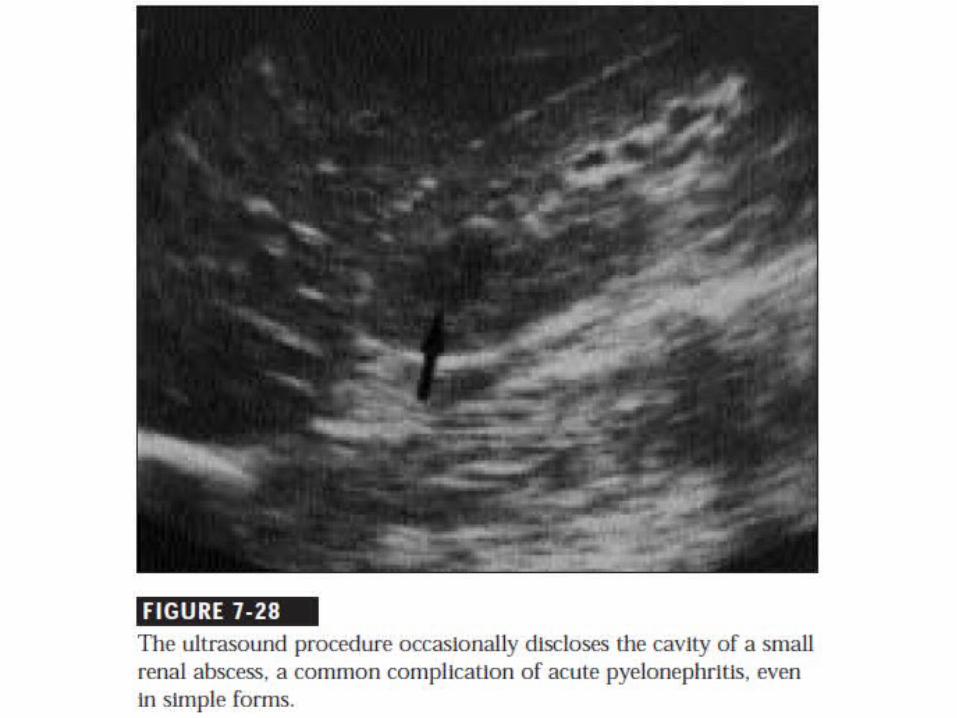
• Blood tests• Urinalysis• Renal ultrasound
Urinalysis
• Determination of the number and type of bacteria in the urine is an extremely important diagnostic procedure.
• In symptomatic patients, bacteria are usually present in the urine in large numbers (100000/mL).
• In asymptomatic patients, two consecutive urine specimens should be examined bacteriologically before therapy is instituted and 100000 bacteria of a single species per milliliter should be demonstrable in both specimens.
Microscopy of urine • Microscopic bacteriuria, which is best assessed with Gram-
stained uncentrifuged urine, is found in 90% of specimens from patients whose infections are associated with colony counts of at least 100000/mL and this finding is very specific.
• Bacteria cannot usually be detected microscopically in infections with lower colony counts (10,000/mL).
• The detection of bacteria by urinary microscopy thus constitutes firm evidence of infection, but the absence of microscopically detectable bacteria does not exclude the diagnosis.
Sterile pyuria
• may indicate infection with unusual bacterial agents • C. trachomatis• U. urealyticum• Mycobacterium tuberculosis • Fungi • may be demonstrated in noninfectious urologic
conditions such as calculi, anatomic abnormality, nephrocalcinosis, vesicoureteral reflux, interstitial nephritis or polycystic disease
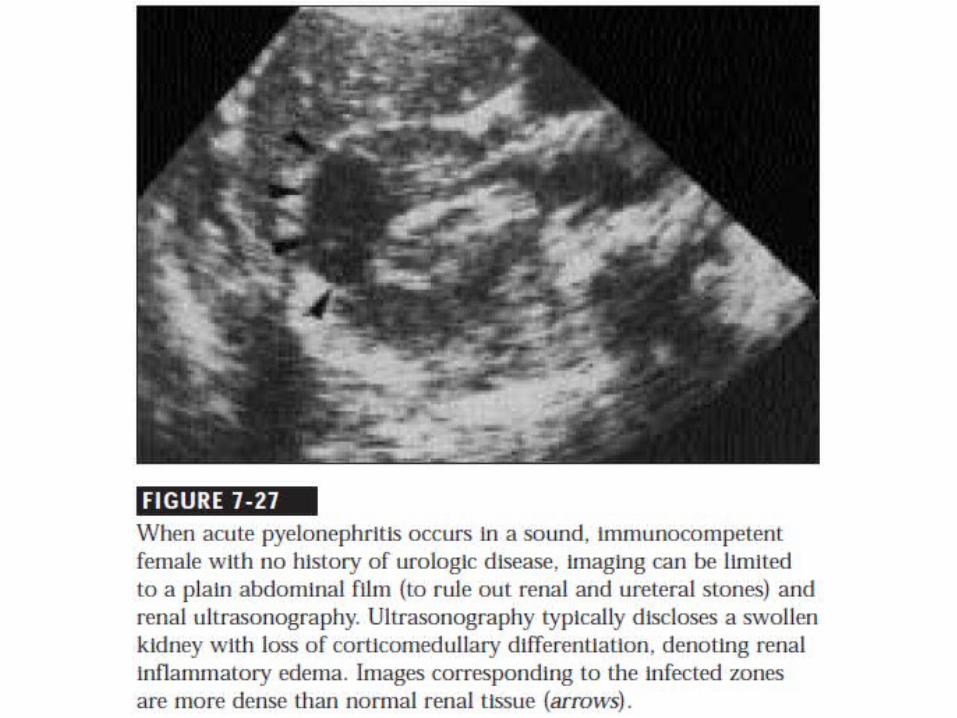
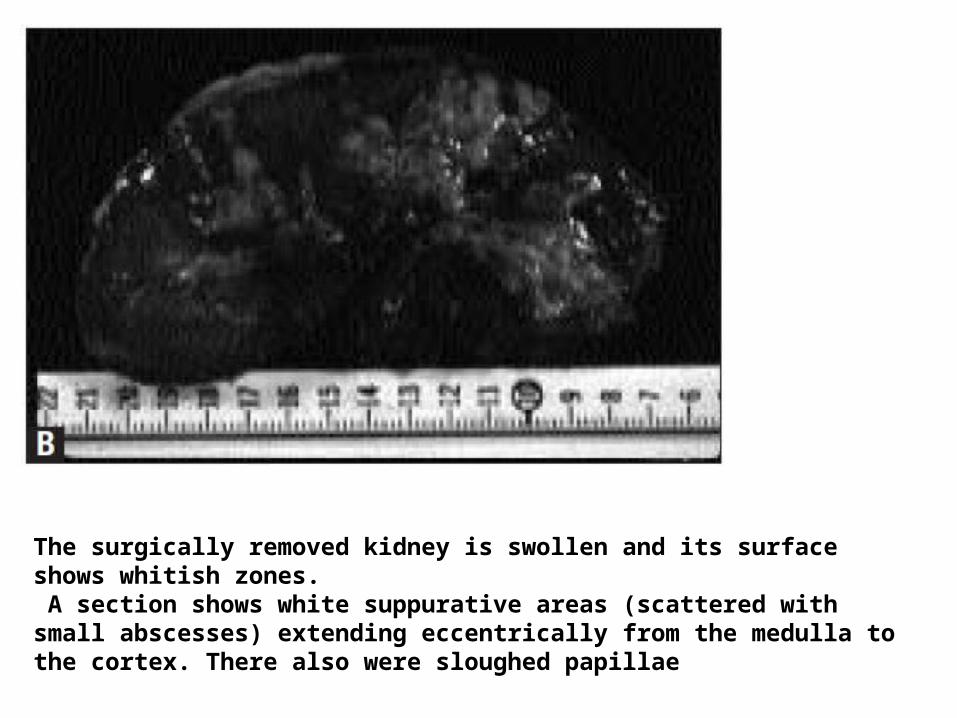
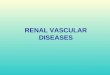
The surgically removed kidney is swollen and its surface shows whitish zones. A section shows white suppurative areas (scattered with small abscesses) extending eccentrically from the medulla to the cortex. There also were sloughed papillae
UROLOGIC EVALUATION• Urologic evaluation should be performed in selected
instances— namely, in women with relapsing infection, a history of childhood infections, stones or painless hematuria or recurrent pyelonephritis.
• Most males with UTI should be considered to have complicated infection and thus should be evaluated urologically.
• Men or women presenting with acute infection and signs or symptoms suggestive of an obstruction or stones should undergo prompt urologic evaluation, generally by means of ultrasound.
Prognosis
• Acute uncomplicated pyelonephritis in adults rarely progresses to renal functional impairment and chronic renal disease.
• Repeated upper tract infections often represent relapse rather than reinfection and a vigorous search for renal calculi or an underlying urologic abnormality should be undertaken.
Chronic pielonephritis
• Insidious onset
• Symptoms and signs of acute pielonephritis
General signs
• Astenia • Fever• Headaches• Nausea and vomiting
Renal signs
• Lumbar pain• Polakiuria• Disuria• Piuria
Signs of sclerotic lesions
• HBP
• CRF
Urinalysis
• Piuria• Sternhelmer – Malbin cells• Leucocyte casts• Proteinuria• Positive urine cultures
Renal function
• Low urine concentration
• Low PSP retention (less than 30% in 15 min)• Low creatinine clearence – renal failure
Blood tests
• Leucocytosis• ↑ alfa-2 and gammaglobulins• Hyponatremia• Acidosis• ↑ureea and creatinine levels (advanced
disease)
Investigations
• Abdominal X-ray: lithiasis, renal asymetry
• IVU: reduced renal mass, unregulated shape, thiner cortical, lithiasis
• Abdominal ultrasound• CT
nephrolithiasis
TYPES OF STONES
• Calcium salts, uric acid, cystine and struvite (MgNH4PO4) are the basic constituents of most kidney stones in the western hemisphere.
• Calcium oxalate and calcium phosphate stones make up 75 to 85% of the total and may be admixed in the same stone.
Manifestations • As stones grow on the surfaces of the renal papillae or
within th collecting system, they need not produce symptoms.
• Asymptomatic stones may be discovered during the course of radiographic studies undertaken for unrelated reasons.
• Stones rank, along with benign and malignant neoplasms, and renal cysts, among the common causes of isolated hematuria.
• Much of the time, however, stones break loose and enter the ureter or occlude the ureteropelvic junction, causing pain and obstruction.
STONE PASSAGE
• A stone can traverse the ureter without symptoms, but passage usually produces pain and bleeding. The pain begins gradually, usually in the flank, but increases over the next 20 to 60 min to become so severe that narcotic drugs may be needed for its control.
• The pain may remain in the flank or spread downward and anteriorly toward the ipsilateral loin, testis or vulva.
STONE PASSAGE
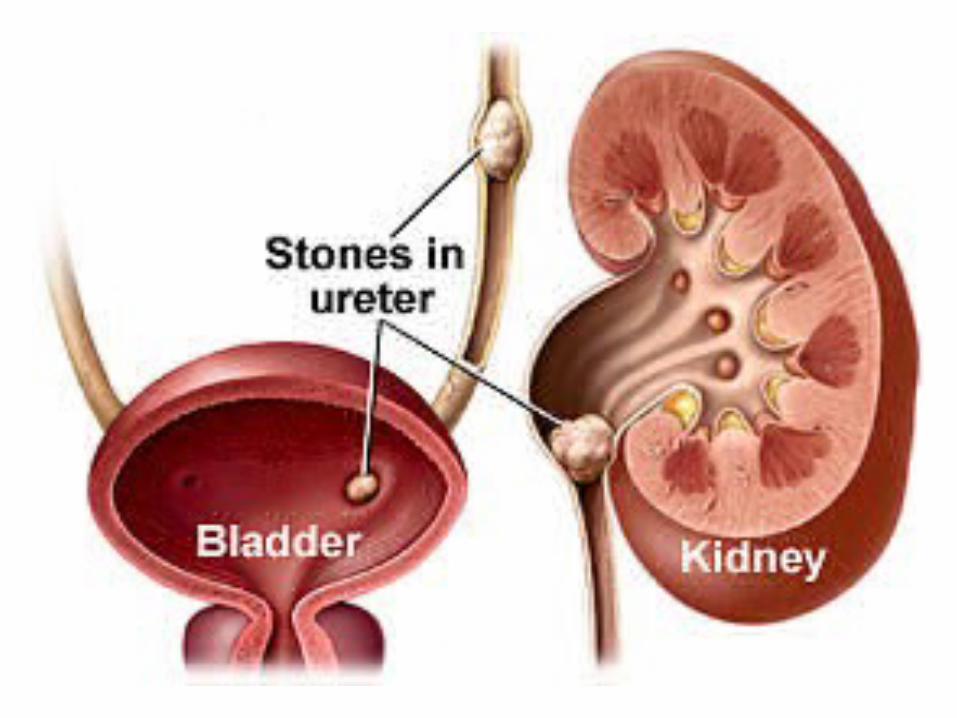
• Pain that migrates downward indicates that the stone has passed to the lower third of the ureter, but if the pain does not migrate, the position of the stone cannot be predicted.
• A stone in the portion of the ureter within the bladder wall causes frequency, urgency, and dysuria that may be confused with urinary tract infection.
• The vast majority of ureteral stones less than 0.5 cm in diameter will pass spontaneously.
PATHOGENESIS OF STONES• Urinary stones usually arise because of the breakdown
of a delicate balance. The kidneys must conserve water, but they must excrete materials that have a low solubility. These two opposing requirements must be balanced during adaptation to diet, climate and activity.
• When the urine becomes supersaturated with insoluble materials, because excretion rates are excessive and/or because water conservation is extreme, crystals form and may grow and aggregate to form a stone.
Symptoms
• Lumbar pain – renal colic• Digestive intolerance (nausia, vomiting)• Hematuria (micro/macroscopic)
Signs
• + Giordano• Uretral pain
Urinalysis
• Hematuria• Leucocyturia• Leucocyte casts
Investigations
• Echo-litiasis • X-ray-radio-opaque stones• IVU-radio-transparent stones• CT
Evaluation
• Most patients with nephrolithiasis have remediable metabolic disorders that cause stones and can be detected by chemical analyses of serum and urine.
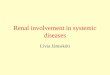
Renal cell carcinoma
Epidemiology
• Renal cell carcinoma represents 2% of all cancers and 2% of all cancer deaths.
• Worldwide, the mortality from renal cell carcinoma was estimated to exceed 100,000 per year
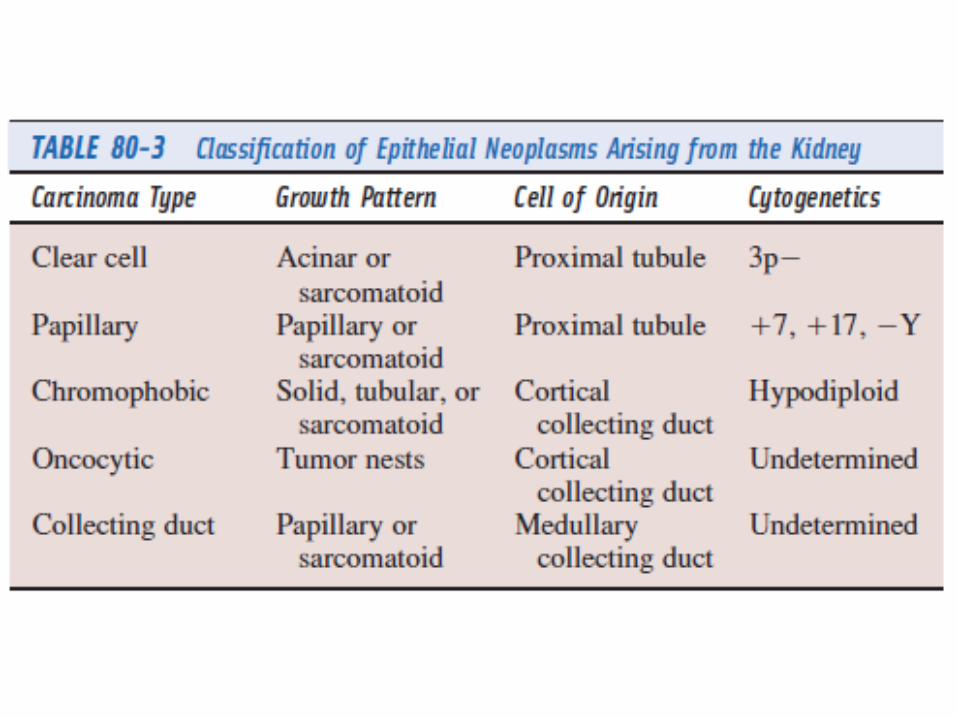
Classification • Renal cell carcinomas have historically been classified according
to cell type (clear, granular, spindle, or oncocytic) and growth pattern (acinar, papillary, or sarcomatoid).
• This classification has undergone a transformation to more accurately reflect the morphologic, histochemical, and molecular basis of differing types of adenocarcinomas .
• Based on these studies, five distinct subtypes have been identified. These include clear cell (conventional), chromophilic (papillary), chromophobic, oncocytic, and collecting duct (Bellini duct) tumors.
• Each of these tumors has a unique growth pattern, cell of origin, and cytogenetic characteristics.
Clinical manifestations• The clinical presentation of renal cell carcinoma can be extremely variable. • Many tumors are clinically occult for much of their course, thus delaying
diagnosis. Indeed, 25% of individuals have distant metastases or locally advanced disease at the time of presentation. By contrast, other patients harboring renal cell carcinoma experience a wide array of symptoms or have a variety of laboratory abnormalities, even in the absence of metastatic disease.
• This propensity of renal cell carcinoma to present itself as a panoply of diverse and often obscure signs and symptoms has led to its being labeled the “internist's tumor.”
• The increasing incidental discovery of renal cancer on abdominal imaging, mentioned previously, has led to the re-characterization of the disease as the “radiologists tumor.”
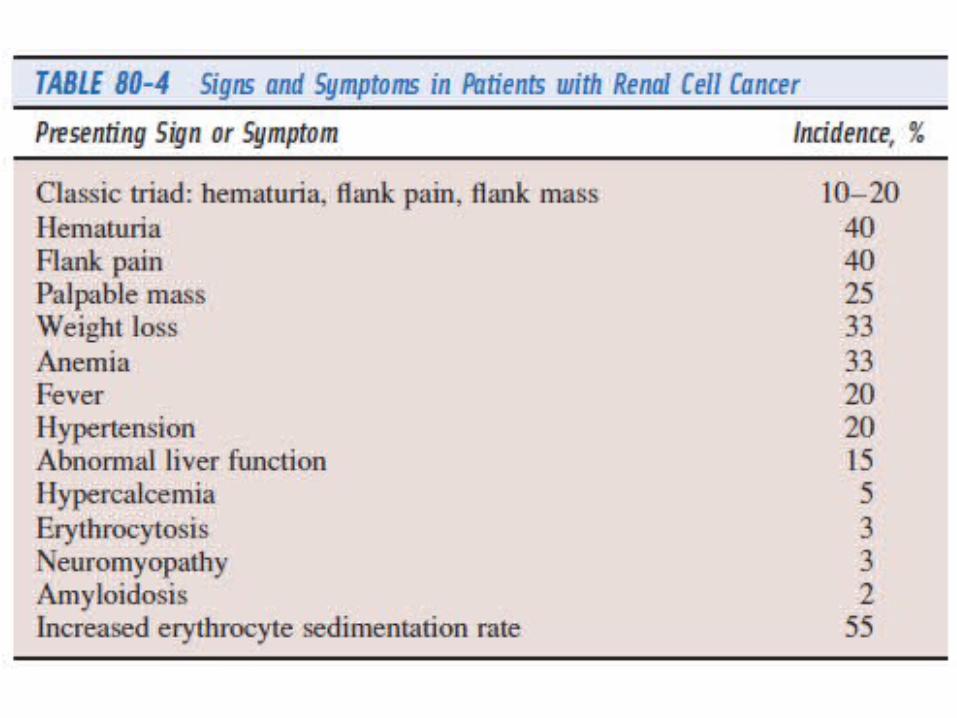
Symptoms
• Lumbar pain • Abdominal or flank mass• Wheight loss• Hematuria
• The classic triad of flank pain, hematuria and palpable abdominal renal mass occurs in at most 9% of patients and when present it strongly suggests advanced disease
Metastatic signs
• Most (75%) patients presenting with metastatic disease have lung involvement. Other common sites include lymph nodes, bone and liver.
• Patients may present with pathologic fractures, cough, hemoptysis, dyspnea related to pleural effusions or palpable nodal masses.
• Clear cell pathology in the metastatic lesion or the finding of a renal mass on staging CT scan (or both) usually leads to the proper diagnosis.
• Fever is one of the more common manifestations of renal cell carcinoma, occurring in up to 20% of patients.
• It is usually intermittent and is often accompanied by night sweats, anorexia, weight loss and fatigue.
• Anemia is also common in patients with renal cell carcinoma
and frequently precedes the diagnosis by several months. Although hematuria, hemolysis or bone marrow replacement by tumor may be contributing factors, the anemia is often out of proportion to these factors. It can be either normocytic or microcytic and is frequently associated with both low serum iron titer and low iron-binding capacity that is typical of the anemia of chronic disease.
• Hepatic dysfunction in the absence of metastatic disease is noted and labeled “Stauffer's syndrome”.
• A spectrum of paraneoplastic syndromes has been associated with these malignancies, including erythrocytosis, hypercalcemia, nonmetastatic hepatic dysfunction (Stauffer syndrome) and acquired dysfibrinogenemia.
• Erythrocytosis is noted at presentation in only about 3% of patients.
• Anemia, a sign of advanced disease, is more common.
Investigations
• Blood tests - ↑ ESR - Anemia - Polyglobulia • X-ray – enlarged renal shadow• Echo – tumoral mass• Selective renal arteriography
Investigations
• The standard evaluation of patients with suspected renal cell tumors includes:
• a CTscan of the abdomen and pelvis• a chest radiograph• urine analysis • urine cytology
• For patients with symptoms suggestive of renal cell carcinoma, numerous radiologic approaches are available for the evaluation of the kidney.
• With the advent of CT, magnetic resonance imaging and sophisticated ultrasonography, many of the more invasive procedures of the past are largely of historical interest and rarely used in clinical practice.
• Although intravenous pyelography remains useful in the evaluation of hematuria, CT and ultrasonography are the mainstays of evaluation of a suspected renal mass.
• As seen on CT, the typical renal cell carcinoma is generally greater than 4 cm in diameter, has a heterogeneous density and enhances with contrast.
MTS evaluation• A CT of the chest is warranted if metastatic disease is
suspected from the chest radiograph, as it will detect significantly smaller lesions, and their presence may influence the approach to the primary tumor.
• MRI is useful in evaluating the inferior vena cava in cases of suspected tumor involvement or invasion by thrombus, as well as for patients in whom contrast cannot be administered owing to either allergy or renal dysfunction.
• In clinical practice, any solid renal masses should be considered malignant until proven otherwise; a definitive diagnosis is required.
Differential diagnosis• cysts• benign neoplasms (adenoma, angiomyolipoma,
oncocytoma)• inflammatory (pyelonephritis or abscesses)• other primary or metastatic malignant neoplasms
• Other malignancies that may involve the kidney include transitional cell carcinoma of the renal pelvis, sarcoma, lymphoma, Wilms’ tumor and metastatic disease, especially from melanoma.
Staging
Two staging systems used commonly are:
• Robson classification and
• American Joint Committee on Cancer (AJCC) staging system
The Robson system
• stage I tumors are confined to the kidney; • stage II tumors extend through the renal capsule
but are confined to Gerota’s fascia;• stage III tumors involve the renal vein or vena
cava (stage III A) or the hilar lymph nodes (stage III B);
• stage IV disease includes tumors that are locally invasive to adjacent organs (excluding the adrenal gland) or distant metastases.
Prognosis
The rate of 5-year survival varies by stage: • 66% for stage I• 64% for stage II• 42% for stage III• 11% for stage IV
• The prognosis for patients with stage IIIA lesions is similar to that of stage II disease; 5-year survival for patients with stage IIIB disease is only 20%, closer to that of stage IV.
Essentials of Diagnosis
• Gross or microscopic hematuria. • Flank pain or mass in some patients. • Systemic symptoms such as fever, weight loss
may be prominent. • Solid renal mass on imaging.