Embed Size (px)
Citation preview

Clinical Research in Low-Literacy Populations: Using Teach-Back to Assess Comprehension ofInformed Consent and Privacy InformationAuthor(s): Sunil Kripalani, Rachel Bengtzen, Laura E. Henderson and Terry A. JacobsonSource: IRB: Ethics and Human Research, Vol. 30, No. 2 (Mar. - Apr., 2008), pp. 13-19Published by: The Hastings CenterStable URL: http://www.jstor.org/stable/30033265 .
Accessed: 12/06/2014 19:36
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
The Hastings Center is collaborating with JSTOR to digitize, preserve and extend access to IRB: Ethics andHuman Research.
http://www.jstor.org
This content downloaded from 62.122.72.154 on Thu, 12 Jun 2014 19:36:36 PMAll use subject to JSTOR Terms and Conditions

IN THE FIELD BY SUNIL KRIPALANI, RACHEL BENGTZEN, LAURA E. HENDERSON, AND TERRY A. JACOBSON
Clinical Research in Low-Literacy Populations: Using Teach-Back to Assess Comprehension of Informed Consent and Privacy Information Ensuring informed consent of participants in clini-
cal research is a significant challenge.' During the onsent process, prospective participants must be
provided with adequate information in order to make an educated decision about whether to enroll in the study, including details on the purpose, risks, benefits, and pro- cedures involved in the study, as well as the confidentiali-
ty of personal health information. However, prospective participants may understand only 30% to 81% of infor- mation in standard consent forms.2
A major reason for such poor comprehension is the
complexity of most consent and privacy documents, which often are written at too advanced a level for their intended audience.3 In addition, a wide range of factors such as older age,4 cognitive impairment, low education- al attainment,5 and poor literacy skills6 can adversely affect consent comprehension. The National Assessment of Adult Literacy estimated that only 13% of Americans have proficient literacy skills, the level that would be
required for understanding of typical informed consent
materials.7 Low literacy therefore presents a widespread and important barrier to informed participation in clini- cal research studies.
The National Cancer Institute, National Quality Forum, and other leading groups have recommended
steps to improve the informed consent process for all
prospective participants, particularly those with limited
literacy skills.8 They suggest providing enhanced consent documents written at an eighth grade reading level or lower. In addition, materials should be relatively short, clearly organized with subheadings, illustrated, and writ- ten in active voice with straightforward vocabulary. Individuals prefer material that is presented in a simpli- fied format,9 and several prior studies of enhanced con- sent forms have demonstrated improved understand-
ing.10 Other research has shown that providing both written and verbal information leads to better informa- tion recall than written or verbal information alone.11
Few studies in which the consent process was modi- fied have examined the role of literacy level on consent
comprehension." Moreover, we are not aware of any such studies which included comprehension of privacy information that must be provided as required under the
Privacy Rule of the Health Insurance Portability and
Accountability Act (HIPAA Privacy Rule). In the context of a randomized controlled trial to improve medication adherence, we provided patients eligible to enroll in the trial with simplified written documents, a short verbal
description of the study, and a visual aid to describe the randomization process. We examined the independent association of patients' age, cognition, years of educa-
tion, and literacy level with comprehension of informed consent and HIPAA Privacy Rule requirements regarding authorization for use and disclosure of protected health information.
Study Methods
0 Setting and Population. The study was conducted in the primary care clinics at an inner-city teaching hos-
pital in Atlanta, Georgia, that serves a predominately low-income, African American population. The study design and materials were approved by the university Institutional Review Board (IRB) and hospital Research
Oversight Committee.
Subjects for this analysis were among the 435 partici- pants in a larger randomized controlled trial-the
Improving Medication Adherence through Graphically Enhanced interventions in Coronary Heart Disease (IMAGE-CHD) study.13 The trial followed a zxz factori- al design; participants were assigned to receive usual
care, an illustrated medication schedule ("pill card"), refill reminder postcards, or both interventions for a
period of one year.14 The primary outcome was cardio- vascular medication adherence.
Sunil Kripalani, Rachel Bengtzen, Laura E. Henderson, and Terry A. Jacobson, "Clinical Research in Low-Literacy Populations: Using Teach-Back To Assess Comprehension of Informed Consent and Privacy Information," IRB: Ethics & Human Research 30, no. z (zoo8): 13-19;.
IRB: ETHICS & HUMAN RESEARCH MARCH-APRIL 2008 13
This content downloaded from 62.122.72.154 on Thu, 12 Jun 2014 19:36:36 PMAll use subject to JSTOR Terms and Conditions

Enrollment took place from March 20zoo4 to March
20zoo05. Patients were eligible for the study if they had a history of CHD, as determined by documentation in their medical chart of previous myocardial infarction, percutaneous transluminal coronary angioplasty, coro- nary artery bypass surgery, or greater than 30% stenosis on prior cardiac catheterization. Under a limited waiver of the authorization requirement of the HIPAA Privacy Rule permitting chart screening for study eligibility, research staff reviewed the charts of patients with upcoming appointments to select all those with CHD. On the day of the appointment, research staff approached the patients with CHD in the waiting room and screened them for enrollment while they waited to see their physician; patients were not previously notified about the study. Patients were deemed ineligible if they were too ill to complete the study interviews; were helped by a caregiver who managed their medications; lacked a mailing address or telephone number; already used an illustrated medication schedule that depicted their medical regimen; did not fill their prescriptions in the health system pharmacies; were in police custody; had a visual acuity lower than zo/6o; were unable to communicate in English; or had a diagnosis of schizo- phrenia or bipolar disorder. Patients with overt delirium or dementia who could not answer several screening questions for orientation to person, place, and time were also excluded.
N Protocol and Data Collection. In total, 968 patients with CHD were screened for the study, and 490 met criteria for enrollment. Eligible patients met individ- ually with a trained research interviewer in a private room in the primary care center, where study informa- tion was provided in three sequential steps: 1) patients received written informed consent and HIPAA forms and were prompted to look over them; z) they heard a scripted study overview; and 3) the interviewer assessed patients' comprehension of study information using "teach-back" techniques and provided additional teach-
ing as needed (details follow). The 440 patients who consented to participate in IMAGE-CHD were enrolled and randomized the same day; five participants later withdrew consent, leaving 435 in the parent study.
The consent document was two single-spaced pages containing 1,114 words, with an average sentence length of i6.5 words. The HIPAA form was a three-page, sin- gle-spaced document that contained 1,572 words. It had an average sentence length of 17.3 words and included a table that outlined the entities potentially able to access
participant information. As recommended, both the con- sent and HIPAA forms were written in the second per- son, and they followed additional guidelines for docu- ment design, such as the use of clear subheadings.5s Both documents had a reading grade level of 7.7 as deter- mined by the Flesch-Kincaid method.'6
The oral overview of the study contained essentially the same information as found in the consent and HIPAA documents, but in a more conversational tone. The interviewer followed a script to ensure uniform pro- vision of information to prospective participants. The verbal description highlighted the purpose of the study and noted that it involved an interview that day, as well as a follow-up interview approximately three months later. To explain that the patient could end up in any one of four study groups by chance, the interviewer used an illustration that contained similar pictures of four groups of people; they were labeled as "usual care," "pill cards," "postcards," or "pill cards + postcards." The interviewer also described the risks and benefits of par- ticipation, compensation (five dollars for each interview), study access to their medical records, procedures to pro- tect their confidentiality, the potential need to disclose information to regulatory agencies, the option not to participate, and how to withdraw from the study. While describing the study, the interviewer often indicated where the same information could be found in the con- sent and HIPAA documents. At the end, patients were encouraged to ask questions by the interviewer, who openly prompted them by asking, "What questions do you have for me?"
In the third step of the consent process, the interview- er used a series of teach-backs to assess patients' com- prehension of several important points covered in the verbal study description and consent and HIPAA docu- ments. Teach-back is a technique recommended to enhance communication and confirm understanding, particularly among individuals with limited literacy skills.17 It involves asking individuals to recall or explain in their own words what has been discussed.'8 It is the
preferred approach for assessing consent comprehension, and engaging in this process with prospective partici- pants enhances both short-term and long-term recall of
study-related information.'9 To assess comprehension in the present investigation, patients were asked to explain the purpose of the study, timing of the follow-up inter-
view, treatment received by each of the four study groups, potential risks, and potential benefits of trial participation. Patients were also asked to recount what
MARCH-APRIL 2008 14
IRB: ETHICS & HUMAN RESEARCH
This content downloaded from 62.122.72.154 on Thu, 12 Jun 2014 19:36:36 PMAll use subject to JSTOR Terms and Conditions

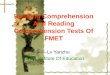
records the study personnel would like to access, what agencies might need to see patients' health information, and procedures for study withdrawal. The interviewer prompted each of these eight teach-backs in a standard- ized fashion by reading from a form; examples are pro- vided in Figure 1.
Teach-back scoring was done immediately by one of five trained interviewers. The method of scoring had been pilot tested among the first 27 patients who enrolled in the IMAGE-CHD study to reach agreement on which responses would be considered correct or incorrect, and interviewers received feedback on their scoring as a component of their training. In some cases, such as those in Figure 1, a correct answer required mul- tiple parts. No partial credit was given, and each of the eight areas was worth a single point. If the patient gave a correct answer, the interviewer proceeded to the next question. If the patient answered incorrectly, the inter- viewer employed a teach-to-goal approach, restating the information of interest and returning to the question within a few minutes to try to confirm comprehension again. For each item, the interviewer recorded whether patients were able to give a satisfactory answer on their first attempt, second attempt, or after giving verbal assent that they understood on a final try. We adopted this approach as a result of pilot testing and finding that patients preferred not to be asked to teach-back the same information more than twice. At the time of scor- ing, the interviewer was effectively blinded to literacy and other patient characteristics because this informa- tion had not yet been collected. Prior to study enroll- ment, all patients demonstrated understanding of the consent and HIPAA information through teach-backs, or if unable to teach-back an item after two attempts, indicated that their questions had been answered and that they felt comfortable enough with their understand- ing to proceed.
Patient characteristics were gathered during the IMAGE-CHD enrollment interview, including age, years of education, race, gender, marital status, and employ- ment status. Literacy was measured using the Rapid Estimate of Adult Literacy in Medicine (REALM). The REALM is a validated 66-point screening instrument that assesses a patient's ability to read and pronounce common medical words.zo The REALM was scored in the standard fashion to determine patients' reading grade level (a-8, less than or equal to third grade; 19-44, fourth to sixth grade; 45-60, seventh to eighth grade; and 61-66, greater than or equal to ninth grade
Figure 1. Teach-Back Example Questions
Informed Consent:
To evaluate the patients' understanding of the randomization process and study groups, "Tell me about the four groups and what we'll give you if you're in each one of the groups. You can look at the picture if you want."
A correct answer included a description of the four study groups, an indication that one group did not receive an inter- vention, and that patients would have an equal chance of being in any of the groups. Answers were judged incorrect, for example, when patients thought they could choose their study assignment.
HIPAA:
To evaluate patients' understanding of regulatory agencies potentially accessing study information, "Who else might need to look at our records and see your information?"
Correct answers included the funding source (American Heart Association) and the IRB committees of the respective hospital (Grady) and university (Emory). Example of an incor- rect answer: "My doctor/nurse."
level). In addition, patients completed the Mini-Mental State Examination (MMSE), a 30-point measure of cog- nitive function on which scores less than 2.4 can be used to indicate cognitive impairment."
0 Statistical Analysis. Patient characteristics were summarized with descriptive statistics, including fre- quency, mean, median, and standard deviation. Patients' ability to teach-back each of the eight items from the consent and HIPAA information was also summarized with descriptive statistics. A composite dichotomous measure of consent and HIPAA comprehension was constructed to serve as the primary outcome variable; it indicated whether patients successfully taught-back all eight items on the first attempt. To assess the relation- ship of the characteristics of each patient with the com- posite outcome, univariate logistic regression analyses were performed to calculate unadjusted odds ratios and
95 % confidence intervals.Z The odds ratio is a measure of effect size commonly used in logistic regression. It is the ratio of the odds of an outcome occurring in group A to the odds of the outcome occurring in a reference group B. The null value is one. An odds ratio greater than one indicates the outcome is more common in group A, while a value less than one means the outcome is more common in group B. A 95 % confidence interval
MARCH-APRIL 2008 15
IRB: ETHICS & HUMAN RESEARCH
This content downloaded from 62.122.72.154 on Thu, 12 Jun 2014 19:36:36 PMAll use subject to JSTOR Terms and Conditions

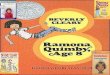
Figure 2. Frequency of Correct Consent and HIPAA Teach-Back by Literacy Level
frequency
%
100
90
80
70
60
50 40
30
20
10
O < 3rd grade 4th-6th grade 7th-8th grade > 9th grade
Literacy Level
that does not overlap one indicates statistical significance at a p-value of 0.05.
Significant predictors from the unadjusted analysis were then entered into a multivariable logistic regression model, which was reduced using a stepwise backwards elimination approach to arrive at the final model. Under this approach, the least significant variables are dropped from the model, one at a time, until dropping another variable would significantly affect the model fit. For each continuous predictor variable, different categorization methods (e.g., continuous, dichotomous, and ordinal) were examined in separate models, and the approach that provided the best model fit was adopted. For all
analyses, a p-value <o.o5 was considered statistically sig- nificant. Analyses were performed with SPSS 13.0 for Windows.
Study Results
A total of 408 patients enrolled in IMAGE-CHD dur-
ing the period of scoring consent comprehension and remained in the study. Complete data for compre- hension were available on 373 (91.4%). Their mean age was 64.0, 90.3% were African American, and 54.7% were female, which reflected the demographics of the overall clinic population. Participants completed a mean of 10.9 years of education (SD = 3.2), and they had a mean score of 24.6 on the MMSE (SD = 3.2). Scores on the REALM spanned the full possible range (o-66); approximately one-fourth of participants scored in each
of the four REALM categories for reading grade level (Table 1, at http://www.thehastingscenter.org/ pdf/irb_zoo8_mar_apr_Kripalanitables.pdf). Those for whom we had incomplete data (N = 35) did not differ significantly on any of the above characteristics.
The ability of patients to correctly teach-back individual items from the consent and privacy information on the first attempt ranged from
57.1% to 92.5% (Table z, at http://www.thehast- ingscenter.org/pdf/irb_zoo8_mar_aprKripalani _tables.pdf). They had greater difficulty explaining two areas-that they would be assigned by chance to one of the four study groups (57.1% correct), and naming the entities that might have access to their study information (68.6% correct). Overall, 38.9% correctly taught-back all eight of the items on their first attempt.
In unadjusted analyses, age, African American race, years of education, MMSE score, and litera-
cy level were each significantly associated with consent and HIPAA comprehension (Table 3, at http:// www.thehastingscenter.org/pdf/irb zoo8_marapr_ Kripalani_tables.pdf). Comprehension was lower among patients who were older or African American, and it was
higher among those who had more formal education, a
higher level of cognitive function, or better literacy skills. The percentage of patients who demonstrated compre- hension increased in a step-wise fashion by literacy level, from a low of 16.7% among adults who read at or below the third-grade level, to a high of 60.7% among those who read at a high school level (Figure z).
In multivariable models, only age and literacy remained significant independent predictors of compre- hension; MMSE score was nearly significant, but the
95% confidence interval overlapped one (Table 3, at
http://www.thehastingscenter.org/pdf/irb_ 2008_mar_apr_ Kripalani_tables.pdf). Compared to those who read at the lowest level (less than or equal to third grade), adults who read between the fourth- and eighth -grade levels had more than two times the odds of consent and HIPAA comprehension, and those who read at a high school level had more than four times the odds of com-
prehension after adjustment for age and cognitive func- tion. The odds of comprehension dropped by roughly 2-3 % for each additional year of age, or by approxi- mately half for a zo-year increase in age.
MARCH-APRIL 2008 IRB: ETHICS & HUMAN RESEARCH 16 This content downloaded from 62.122.72.154 on Thu, 12 Jun 2014 19:36:36 PM
All use subject to JSTOR Terms and Conditions

Discussion
In this analysis of adults enrolling in a randomized trial, literacy was significantly associated with compre-
hension of consent and privacy information, even when recommended steps were taken to simplify the informa- tion and a verbal study description was provided.23 Compared to those who read at or below a third-grade level, patients who read at a fourth- to eighth-grade level had approximately twice the odds of comprehension, and those at a high school reading level demonstrated more than four times the odds of comprehension, as measured by teach-back of key information about the study. These findings suggest that individuals with limit- ed literacy skills should be considered a vulnerable popu- lation. Special consideration should be given to their protection in clinical research studies, as is currently done for children, prisoners, and other at-risk groups. In the context of informed consent, additional steps should be taken to ensure comprehension among all individuals recruited for clinical trials, particularly those with limit- ed literacy skills. This work will be facilitated by a new health literacy and informed consent toolkit expected to be released by the Agency for Healthcare Research and Quality in the coming year.
The results of this investigation are consistent with prior research demonstrating that low literacy is associ- ated with poor comprehension of consent materials.14 In those studies, however, investigators used true/false or multiple-choice questions to assess understanding,25 or they studied materials in a hypothetical setting with vol- unteers.26 Strengths of the present investigation include its performance with real patients going through the consent process and its use of teach-back to assess con- sent comprehension. Teach-back is the preferred method to confirm understanding of consent information, and its use is advocated by the National Quality Forum,27 the Agency for Healthcare Research and Quality,i8 and other groups.
Using a series of teach-backs is a feasible and general- izable approach that could be adopted in most research
settings to help assess comprehension of consent and HIPAA information prior to study enrollment. As we did in this trial, research staff could ask prospective trial par- ticipants to describe their understanding of the study's purpose, procedures, risks, and benefits. Additional
questions that pertain to study procedures or human subjects protection could be added where appropriate to ensure comprehension of other areas, such as voluntari- ness, freedom to withdraw, duration of study, random-
IRB: ETHICS & HUMAN RESEARCH
ization, and whom to contact.29 When personal health information is being collected, individuals could be asked to describe the types of information collected, pro- cedures for maintaining confidentiality, and the process of revoking HIPAA authorization. To assess understand- ing in this manner requires about five minutes, which compares favorably to the seven to twelve minutes required to administer other measures of consent com- prehension.30
Moreover, asking individuals to teach-back study information allows the researcher to find out in real time how well the prospective trial participants understood the material. Specific points can be clarified immediately, and individuals can be asked again to teach-back the information to ensure their comprehension.31 This approach is called the teach-to-goal strategy, a method of targeted education that repeats material until under- standing is achieved.32 It is unclear how often teach-back or teach-to-goal strategies are used in the informed con- sent process, but available data suggest their use is uncommon. One study of principal investigators demon- strated that only zo% used open-ended prompts to assess understanding (e.g., "Tell me in your own words the purpose of the study"), while 8o% used closed- ended questions such as, "Do you understand?"33 The latter is clearly inadequate given that many people enroll in a study and consider themselves informed but demon- strate poor performance on tests that assess their under- standing of the research.34 Additional measures must be taken to facilitate comprehension and assess understand- ing prior to study enrollment, especially in groups with limited literacy skills and other vulnerable populations.35
Limitations of this study included recruitment from a single center that serves a predominantly inner-city, African American population. Other racial groups were not well represented and require further investigation. Second, the consent and HIPAA documents were written at approximately an eighth-grade reading level; further reduction in their complexity might have facilitated com- prehension among patients with limited literacy skills. Third, study documents in this investigation were pro- vided at the time of the consent interview. Providing con- sent material in advance may foster better comprehen- sion.36 However, memory for consent information declines over time.37 If patients had received study infor- mation in advance, it is uncertain how this might have affected their performance on the teach-back assessment of comprehension, and on the association of literacy with comprehension. Fourth, immediate scoring of
MARCH-APRIL 2008 17
This content downloaded from 62.122.72.154 on Thu, 12 Jun 2014 19:36:36 PMAll use subject to JSTOR Terms and Conditions

teach-back responses can be subjective. Although study interviewers completed similar training and we believe their scoring to be comparable, we did not formally assess interrater reliability. Finally, although this analysis has the advantage of being conducted in the context of clinical trial enrollment, the trial was relatively straight- forward and noninvasive with minimal risk and follow-
up requirements. Recall of study information would like- ly be appreciably worse in a typical clinical trial, which is usually more complex.
Future research should test the feasibility of using teach-back to assess comprehension in demographically diverse populations and across a variety of study proto- cols as might be found in clinical research centers. The teach-back method should also be compared to other measures of consent comprehension for feasibility, acceptability, and relative value in helping to ensure ade-
quate understanding prior to enrollment.38 Moreover, the optimal method for using teach-back in the informed consent process (e.g., how many times the cycle should be repeated) needs to be determined. Other areas for future study that were not assessed in the present analy- sis include the effect of literacy on individuals' willing- ness to participate in research, as well as on study with- drawal rates.
Low literacy presents a significant barrier to compre- hension of consent and privacy information in clinical research. Given the high prevalence of limited literacy skills in the United States and the frequency with which prospective trial participants struggle to understand research protocols, researchers should take greater meas- ures to assess and ensure comprehension of study infor- mation during the informed consent process.39 The available evidence suggests that teach-back and teach-to- goal strategies are beneficial, and broader use of these approaches is recommended.4
Acknowledgments This work was supported by a grant from the American
Heart Association. The study design and materials were approved by the Emory University Institutional Review Board and the Grady Health System Research Oversight Committee. We thank Rashanda Robertson for project management and Marra G. Katz and Courtney Cawthon for editorial assistance.
U Sunil Kripalani, MD, MSc, is Associate Professor and Director, Section of Hospital Medicine, Division of General Internal Medicine and Public Health, Vanderbilt University, Nashville, TN; Rachel Bengtzen, AB, is a medical student at Emory University School of Medicine, Atlanta, GA; Laura E. Henderson, MS, is Research Coordinator, Division of General Medicine, Department of Medicine, Emory University School of Medicine, Atlanta, GA; and Terry A.
Jacobson, MD, is Professor, Division of General Medicine, Department of Medicine, Emory University School of Medicine, Atlanta, GA.
References 1. Wendler D. Can we ensure that all research subjects give valid
consent? Archives of Internal Medicine zoo4; 164(zo):z22o1-zzo4; Flory J, Emanuel E. Interventions to improve research participants' understanding in informed consent for research: A systematic review. JAMA zoo004;292(13):1593-1601.
z. See ref. 1, Flory and Emanuel 200oo4. 3. Breese P, Burman W, Rietmeijer C, et al. The Health Insurance
Portability and Accountability Act and the informed consent process. Annals of Internal Medicine zoo4;141(11):897-898; Paasche-Orlow MK, Jacob DM, Powell JN. Notices of privacy practices: A survey of the Health Insurance Portability and Accountability Act of 1996 docu- ments presented to patients at U.S. hospitals. Medical Care
2zoo005;43(6):558-564; Paasche-Orlow MK, Taylor HA, Brancati FL. Readability standards for informed-consent forms as compared with actual readability. NEJM zoo003;348(8):721-7-6.
4. Sugarman J, McCrory DC, Hubal RC. Getting meaningful informed consent from older adults: A structured literature review of empirical research. Journal of the American Geriatrics Society 1i998;46(4):517-524.
5. See ref. 4, Sugarman et al. 1998; Benson PR, Roth LH, Appelbaum PS, et al. Information disclosure, subject understanding, and informed consent in psychiatric research. Law & Human Behavior 1988;12(4):455-475; Daugherty C, Ratain MJ, Grochowski E, et al. Perceptions of cancer patients and their physicians involved in phase I trials. Journal of Clinical Oncology 1995;I13(5):1062-10o72; Joffe S, Cook EF, Cleary PD, et al. Quality of informed consent in cancer clini- cal trials: A cross-sectional survey. Lancet zoo1;358(9295):1772-1777; Kucia AM, Horowitz JD. Is informed consent to clinical trials an "upside selective" process in acute coronary syndromes? American Heart Journal 00zooo;14o(1):94-97.
6. Coyne CA, Xu R, Raich P, et al. Randomized, controlled trial of an easy-to-read informed consent statement for clinical trial participa- tion: A study of the Eastern Cooperative Oncology Group. Journal of Clinical Oncology zoo3;z1(5):836-842; Raich PC, Plomer KD, Coyne CA. Literacy, comprehension, and informed consent in clinical research. Cancer Investigation zool1;19(4):437-445; Davis TC, Holcombe RF, Berkel HJ, et al. Informed consent for clinical trials: A comparative study of standard versus simplified forms. Journal of the National Cancer Institute 1998;9o(9):668-674; Sudore RL, Landefeld CS, Williams B, et al. Use of a modified informed consent process among vulnerable patients: A descriptive study. Journal of General Internal Medicine 200oo6;21(8):867-873.
7. Kutner M, Greenberg E, Baer J. National Assessment of Adult Literacy (NAAL). A first look at the literacy of America's adults in the 21st century. http://nces.ed.gov/naal.
8. See ref. 3, Paasche-Orlow et al. zoo003; Campbell FA, Goldman BD, Boccia ML, et al. The effect of format modifications and reading comprehension on recall of informed consent information by low- income parents: A comparison of print, video, and computer-based presentations. Patient Education & Counseling zoo4;53(z):2o5-z1 6; Meade CD, Howser DM. Consent forms: How to determine and improve their readability. Oncology Nursing Forum 1992;19(1o): 1523-15z8.
9. See ref. 6, Coyne et al. zoo3; Tait AR, Voepel-Lewis T, Malviya S, et al. Improving the readability and process ability of a pediatric informed consent document: Effects on parents' understanding. Archives of Pediatrics & Adolescent Medicine zoo5;159(4):347-352.
io. See ref. 1, Flory and Emanuel zoo4. 11. Winfield AC, Ford CV, James AE, et al. Response of patients to
informed consent for excretory urography. Urologic Radiology 1986;8(1):35-39.
iz. See ref. 6, Coyne et al. zoo3; Davis et al. 1998; Sudore et al. zoo6; see ref. 9, Tait et al. zoo005.
13. Kripalani S, Robertson RS, Schmotzer B, et al. Improving med- ication adherence through graphically enhanced interventions in coro-
MARCH-APRIL 2008 18
IRB: ETHICS & HUMAN RESEARCH
This content downloaded from 62.122.72.154 on Thu, 12 Jun 2014 19:36:36 PMAll use subject to JSTOR Terms and Conditions

nary heart disease: The IMAGE-CHD Study. Journal of General Internal Medicine zoo6;zi(S1): 151.
14. Kripalani S, Robertson R, Love-Ghaffari MH, et al. Development of an illustrated medication schedule as a low-literacy patient education tool. Patient Education & Counseling 20zoo7;66(3):368-377.
15. National Cancer Institute Comprehensive Working Group on Informed Consent in Cancer Clinical Trials. Recommendations for the development of informed consent documents for cancer clinical trials. http://cancertrials.nci.nih.gov/clinicaltrials/understanding/simplification- of-informed-consent-docs/pagez.
16. Dave Taylor and Intuitive Systems. Online readability calcula- tor. http://www.readability.info.
17. Kripalani S, Weiss BD. Teaching about health literacy and clear communication. Journal of General Internal Medicine zoo6;21:888- 890.
18. Schillinger D, Piette J, Grumbach K, et al. Closing the loop: Physician communication with diabetic patients who have low health literacy. Archives of Internal Medicine 20oo3;163:83-90.
19. National Quality Forum, editor. Improving Patient Safety through Informed Consent for Patients with Limited Health Literacy. Washington, DC: National Quality Forum, 2005; Wadey V, Frank C. The effectiveness of patient verbalization on informed consent. Canadian Journal of Surgery 1997;4o(2):124-128; White CS, Mason AC, Feehan M, et al. Informed consent for percutaneous lung biopsy: Comparison of two consent protocols based on patient recall after the procedure. American Journal of Roentgenology 1995; 165 (5): 1139- 1142.
zo. Davis TC, Crouch MA, Long SW, et al. Rapid assessment of lit- eracy levels of adult primary care patients. Family Medicine 1991;23 (6):433-435.
z21. Folstein MF, Folstein SE, McHugh PR. "Mini-Mental State": A practical method for grading the cognitive state of patients for the cli- nician. Journal of Psychiatric Research 1975;12:189-198.
zz. Kleinbaum DG, Klein M. Logistic Regression: A Self-Learning Text. New York: Springer Verlag, 20oo02.
23. See ref. 3, Paasche-Orlow et al. 200oo3; see ref. 8, Campbell et al. 2oo4; see ref. 8, Meade et al. 1992.
24. See ref. 6, Coyne et al. 2z00oo3; Davis et al. 1998; Sudore et al. 2zoo6; see ref. 9, Tait et al. 2.005.
2.5. See ref. 6, Coyne et al. 2z003; Sudore et al. zoo6. 2z6. See ref. 6, Davis et al. 1998; see ref. 9, Tait et al. 2zo0o5. 27. See ref. 19, National Quality Forum 2005. z8. Shojania KG, Duncan BW, McDonald KM, et al., eds. Making
Healthcare Safer: A Critical Analysis of Patient Safety Practices. Evidence Report No. 43 from the Agency for Healthcare Research and Quality. AHRQ Publication No. ol-Eo58, zool. July 2zo, zoo.
29. Department of Health and Human Services. Protection of Human Subjects. 45 CFR 46.
30. Joffe S, Cook EF, Cleary PD, et al. Quality of informed consent: A new measure of understanding among research subjects. Journal of the National Cancer Institute 2zool;93(2):139-147; Miller CK, O'Donnell DC, Searight HR, et al. The Deaconess Informed Consent Comprehension Test: An assessment tool for clinical research subjects. Pharmacotherapy 1996;16(5):872-878.
31. See ref. 18, Schillinger et al. 2zoo3. 32. See ref. 6, Sudore et al. zoo6. 33. See ref. 6, Raich et al. zool; Titus SL, Keane MA. Do you
understand? An ethical assessment of researchers' description of the consenting process. Journal of Clinical Ethics 1996;7(1):6o-68.
34. See ref. 5, Daugherty et al. 1995; Joffe et al. zool; see ref. 30, Miller et al. 1996.
35. See ref. 1, Wendler zoo004; Flory and Emanuel zoo4; see ref. 19, National Quality Forum zoo5.
36. See ref. 5, Joffe et al. 2zoo1. 37. See ref. 4, Sugarman et al. 1998; Herz DA, Looman JE, Lewis
SK. Informed consent: Is it a myth? Neurosurgery 1992;30(3):453-458; Wade TC. Patients may not recall disclosure of risk of death: Implications for informed consent. Medicine, Science, & the Law 1990;30(3):z59-262.
38. See ref. 30, Joffe et al. zool; Miller et al. 1996. 39. See ref. 6, Raich et al. 2zool. 40. See ref. 19, National Quality Forum zoo5; see ref. 28, Shojania
et al. 2ool.
IRB: ETHICS & HUMAN RESEARCH MARCH-APRIL 2008 19
This content downloaded from 62.122.72.154 on Thu, 12 Jun 2014 19:36:36 PMAll use subject to JSTOR Terms and Conditions