Embed Size (px)
Citation preview

Coexisting Gastric and Duodenal Ulcers A Review
H~:aBERa" \VEIsBEa(;, M.D.,* a n d GEORCE B. JERZY GLASS, M.D.
W HETHER GA.STRIC I'LCER ((~,U) a n d d u o d e n a l u lcer (DU) are two m a n i f e s t a t i o n s of one disease or two d i f fe ren t diseases has given rise
to m u c h conf l ic t ing o p i n i o n . I n recen t years cons ide rab l e emphas i s has been p l aced u p o n charac te r i s t i c differences be tween the two lesions. Divergences ill age a n d sex inc idence , e x p e r i m e n t a l p r o d u c t i o n , gas t r ic m o t i l i t y and ac id secre tory pa t te rns , c l in ica l mani fes ta t ions , and b lood g r o u p types ~. " suggest tha t the two lesions are e t io log ica l ly d i s s imi la r and tend to occur in m u t u a l l y exclus ive p a t i e n t p o p u l a t i o n s . On the o the r hand , several au tho r s in the pas t have a d d u c e d ev idence p o i n t i n g e i the r to a gene ra l u lce r "d ia thes i s ' 'a,4 or to a f u n d a m e n t a l i den t i t y in the e t io logy of al l p e p t i c ulcers wi th differences in loca l i za t ion r e l a t ed only to local c o n d i t i o n i n g factors, a. 2, a
T h e presence of coex i s t ing{ gas t r ic a n d d u o d e n a l ulcers ( C G D U ) in the same p a t i e n t is s igni f icant in this r ega rd since it n a t u r a l l y raises a ques t i on as to w h e t h e r ( ; U and DU are in r ea l i t y conf ined to mutua l ly exclus ive p a t i e n t p o p u l a t i o n s . T h e i r coexis tence, if s t , ~c i en t l y f requent , w o u l d fu r t he r suggest tha t the f u n d a m e n t a l p a t h o l o g i c a l m e c h a n i s m re- spons ib le for the p r o d u c t i o n of pep t i c u l ce r a t i on may affect e i the r stom- ach or d u o d e n u m , or b o t h organs s i m u h a n e o u s l y , d e p e n d i n g Ul)on the inf luence of s econdary factors.
A l t h o u g h the f ind ing of C G D U is in fact no t unusua l , its f r equency has va r i ed g rea t ly in d i f fe ren t series. In 1917 Carman~3' repor ted the exis tence of 16 C G D U (2.5°o) in a surgical series of 629 pep t i c u lcer pa t ien ts , whi le in 1926 ~Vilkie z observed 42 such cases (14%) in a s imi la r series of 300 cases of pep t i c ulcer.
I n 1953 F e l d m a n s rev iewed most of the d a t a on C G D U ava i l ab le in the l i t e r a t u r e u p to tha t t ime. H e f o u n d tha t the inc idence of C G D U var ied
From the Section of Gastroenterology, Department of Medicine. New York Medical College-Metropolitan Medical Center New York, N. Y.
Su!oported by Graduate Training Grant TI-AM-5237 from the N.I.A.M.D., U.S.P.ILS. *U. S. Public Health Service Traince in Gastroenterology, New York Medical Col-
lege-Metropolitan Medical Center. "~Also referred to as coincident5 concomitqlH. TM associated. :~ combined?.4-L ~6 and
c o n c u r r e n t e g a s t r i c and duodenal ulcers.
992 American Journal of Digestive Diseases

Gasfrlc with Duodenal Ulcer
strikingl) with the source ol these data; i.e., whether from postnlorten~, surgical, or radiological stu-ve)s, t i e concluded that the composite in- cidence was lowest in unselected radiologi~al aud l)ostmortem series (0.155~ , and 0.,~42"~,) and highest in surgical series of benign and malig-
nant GU's (t7A~)~, and 24.(i{'o). When analyzed in terms of tile total number of peptic ulcer cases, the postmortem incidence ot CGDU was li.5°o and the surgical incidence 7.0(!~.
In the past 10 years several lalge studies of peptic ulcer cases inclnding C(;DU have been added to the literature. It will be the purpose of this paper to review the inlormation available on this type of lesion as it has been reported during this period with regard to comparative statistical incidence, age and sex of patients, acid secretory patterns, clinical course, pathogenesis, complications, and therapy. This information, based on a total of 1490 cases of 'CGDU, may increase our understanding of this type of lesion and the mechanism of peptic tdceration of tile stomach and duodenum.
REVIE\V OF FINDINGS
INCIDENCE OF CGDU
In Table 1 tile general incidence of CGDU is expressed as tile percent- age incidence of CGDU in the total number of GU's and DU's in all series containing both lesions for the 10-)ear period reviewed. This varies from a low of 3.0% in Mangotd's :~ combined radiological and surgical series of 5253 cases of peptic ulcer to a high of 29.5°o in Aagaard's 1° surgical series. Tim composite average for all surveys during tile past 10 years is 6.6°0, which is not significantly different from the composite average of 6.57~, in tile postmortem group and 7.0°:0 in tile surgical group analyzed by Fei(lman '~ in 1953.
Table 1 also lists the incidence of CGDU in benign GU. This varies from 7.9°~) to 38.350 with a composite mean of 23.5°~,, approximately 3 times that seen in the general peptic ulcer population. This incidence is also somewhat higher than that of 17.4% reported by' Feldman. s This in- crease over the past 10 years may be due either to a greater awareness of the disease and greater accuracy in the diagnosis of CGDU in patients with GU or to some change in the natural history of peptic ulcer.
The aver;:~e incidence of CGDU in DU cases is " o-, , 1 . 3 , o , as listed in Table 1. It is about ~,/.~ that noted for CGDU in benign GU's, and practically identical with that found for CGDU in the total number of peptic ulcer cases.
Table 2 contains a supplementary list of cases of CGDU drawn from
New Series, Vol. 8, No. 12, 1963 993

'I'A
BI,
E
I.
INC
II)E
NC
E
()F
C
(;I)
U
IN
PE
PT
IC
U1
X:E
R.
l)I!
, A
ND
B
EN
I(;N
(;
U
Au
thO
r Y
r.
"typ
e N
o.
ol
smve
y C
(;D
U
(;lc
m~
g:
Har
riso
n s
t 19
51
Rau
cW '~
19
52
Sm
ith
et
a
ll ~
19
53
Tam
per
TM
19
54
Joh
n~
m ~
' 19
56
Co
mfo
rt
el
al?'
19
57
Mari
gold
°
1!)5
8
Bcr
nar
do
el
al
. "-'~
19
58
Aag
aard
et
a/
? ~
1959
Mar
ks
& S
hay
'~'
1959
~V
atk
inso
n TM
19
60
(;cl
b g
: B
eck
et 4~
19
(i2
TO
TA
L
1951
-
1962
Sm
gic
al
9
Su
rgic
al
90
Rad
iolo
gic
al
g: s
urg
ical
,% u
rgic
al
Sm
gic
al
32
Su
ngic
al
Rad
iolo
gic
al
157
&
surg
ical
Su
igic
al
- -
Rad
ioh
)gic
al
122
g: s
urg
ical
Su
rgic
al
Pos
t mo
rtem
22
7
Rad
iolo
gic
al
53
g:
surg
ical
%
(:(;
DU
%
(:
(;D
U
%
C(;
DU
T
ota
l N
o.
in t
ota
l N
o.
No
. i,
to
tal
No
. N
o.
in t
ota
l
PU
ca.
~cs
PU
cas
es
I)U
C
(;D
U
I)U
(;
[/
CG
DU
(;
U
289
3.1
215
9 .1
.2
S3
9 I 0
.8
8,15
10
.6
682
90
13.2
25
"~
90
"~5.
6
..
..
..
87
9 17
3 19
.7
..
..
..
..
..
.
25.0
347
9.2
203
2!)
I I.
'; I
16
29
25.0
..
..
..
.
779
181
23.6
5253
3.
0 39
01
157
,1.0
--
--
- --
..
..
.
469
52
I 1.
1
,I 13
29
.5
100
2 2.
0 31
3 12
0 38
.3
..
..
.
33
I 0
3o.3
1848
12
.3
1356
22
7 16
.7
677
227
33.5
1435
3.
7 11
20
36
3.2
315
25
7.9
Mix
ed
690
10-1
30
6.6
7577
55
0 7.
3 "L
ql7
919
23,5

Gastric wlfh Duodenal Ulcer
T A B L E 2. I N C I D E N C E OF C G D U IN PEPTIC ULCER*
% i n c i d e n c e ~V o %
T o t a l o / C G D U i n c i d e n c e i n c i d e n ( e N o , N o , P U in a t l P U T o t a l C G D U T o t a l C G D U
A u t h o r I'r. C G D U cases cases N o . G U in G U N o , D~" in D U
Aird et a l? '~ 1954 113 3011 3,8 1015 11,1 1851 0,1 Clarke et al. "~ 1955 48 1545 3,1 438 1 t .0 1059 4,5 K0ster et alY' 1955 30 1047 2,9 337 8.9 680 4,4 Pcebles Brown
et al. :~ 1956 38 1980 1.8 300 12.6 1642 2.3 Buckwaltcr et al. '~ 1956 69 1839 3.7 469 14.7 1301 5,3 Billington ~" 1958 83 1236 7,2 961 8.6 192 43.2 TOrAL 381 10,658 3,6 3520 10,8 6725 5.7
*Statistics drawn front blood group studies.
,eviews of large pep t ic ulcer p o p u l a t i o n s ill which the p r im a ry pu rpose
,)[ the inves t iga t ion was the cor re la t ion of b lood groups wi th pep t ic u lcer
disease. ~Ihey are inc luded in this review because of the large n u m b e r of
cases s tud ied bu t are listed separate ly since in all these series the detec-
t ion of C G D U was not the p r ima ry objec t o[ inves t iga t ion and only those
cases wi th avai lab le b lood g r o u p i n f o r m a t i o n were inc luded. As may be
seen, the compos i te inc idence of C G D U in all pep t ic ulcer cases and in
cases of ben ign G U analyzed in this m a n n e r is cons ide rab l ) lower than
that no ted in the studies previous ly cited.
FREQUENCY OF GASTRIC ~[AL1GNANCY IN C ( ; D U
T a b l e 3 shows the inc idence of m a l i g n a n t gastr ic u lcer in cases of single
G U and C G D U . \Vhi le the inc idence of ma l ignan¢y in single G U ranged
TABLE 3. FREQUENCY OF GASTRIC MALI(;NANCY IN GU AND CG1)U
C o e x i s t i n g gas tr ic a n d M n g t e Gas tr ic l ' l c e r (GU) d u o d e ~ a l ulcers ( C G D { ' )
N o . cases ~ , N o . cases % - i n c i d e n c e i n c i d e n c e
Ma l ig - o f ma t ig - 3 la l ig - o.( mal ig - T o t a l n a n t B e n i g n nancy" T o t a l na~ t I',e~ign nancy' ,4 u t h o r
Bernardo et al. ~''-" 464 47 417 10A2 55 3 52 5.45
Smith et al. :~ 810 71 739 8,76 190 17 173 8.94 f~omfort et al2 t 802 207 595 25.81 203 19 184 9,35 TOTAl. 2076 325 1751 15.65 448 39 409 8.71
New Series, Vol. 8, No. 12, 1963 995

Welsberq & Glass
h o m 8.8~/£) to 25.8',!;0 ( m e a n 15.7':;), i t was c o n s i d e r a b l y l o w e r in C G D U
- - r a n g i n g l r o m 5 5 ~' to q 4 c ' w i t h a m e a n o [ o n h 8 7 <' I t m a y b e con- • " , O " " ( 2 ~ j ' , 0 ' ¢
e l u d e d , t h e r e f o r e , t h a t t h e g a s t r i c u h : e r in C ( ; D U is less f r e ( l u e n t l y m a l i g -
h a m t h a n G U a l o n e .
SI.:QI:I.:XCE OF UI.(:I'~RS IN C G D U
As s h o w n by s e r i a l r a d i o g r a p h y , t h e D U was t h e first l e s i o n o b s e r v e d in
5.9.8t]~, of t h e cases ( T a b l e 4 ) . I n a s m a l l n u m b e r of cases ( m e a n , 8.0v~,)
t h e r e v e r s e o r d e r was o b s e r v e d , w i t h t h e C U a p p e a r i n g first. I n t he re-
m a i n i n g cases b o t h uh-e rs e i t h e r a p t ) e a r e d s i m u h a n e o u s l y o r t h e i r se-
( ] uence o l a lJ l )e ;nant :e was u n ( l e t e r n l i n e d ,
ANAT()MICAL IX)CATION Ol" Till,: ( ; U IX C G D U
" l a b l e 5 l is ls tl'ie l o c a t i o n o l t h e g a s t r i c l e s ion i n C G D U . T h e r e g i o n of
i h e l )y lo r ic a n t r u n l a n d a n g u h l s , :is wel l :is t he m i d d l e }!~ of t h e lesser
c u r v a t u r e , w e r e t h e s i tes m o s t o f t e n i n v o l v e d . T h e s e a re a l so t h e m o s t
c o m m o n s i tes o f i n v o h e m e n t o f s i n g l e G U .
T A B I . E 4. S E Q U E N C E O F VI,CERS IN C ( ; I ) U
1)l" t i ~ t (;I" [it~t \ " ' L - . . . . . . . . . .
A ul/m~ (~lscs .\'o, <~[, ,Vo. ~'~,
N i # t H t ~ l ~ t ~ t e u U s
0 I"
l l I I ( [CI ( ' I I l l i H P d
No. %
JohnsonUL '~' 135 70 52.t} 7 5.2 58 42.9 MangohP 157 91 58.0 8 5.0 58 37.0 .'~ agaard et al. > 120 9 t 7~,.'1 1S 15.0 8 6.7 (;ell) & Bcckcr ~:" 53 23 -13. t t 7.5 26 49.0 T o ' r \ ~. 4 6 5 278 59 .8 37 8 .0 150 32,3
T\BI,I", 5. I~OCALIZATION OF G17 IN C(;1)U
.4n~u/us Midd l e I~ p)'lo~ic & of le~er
.4~thal region (ll#~,alllle . \ ' 0 . - . . . . . . . . . . . . . .
.4tHho~ r'a~es No. o~, .'%'o. o~,
Mangoht" 157 45 28.6 82 Comfort et al," 184 107 57,8 76 (;elb ,~ Beckcl"= 5":1 22 42.0 - -
Billington ~' 114 23 202 - - TOT X,l 508 l !)7 38.8 158
" l, pe,- 1/~ of les.ger
( ' l l l T J ( l l l l l ( "
No. %
5 2 . 2 3 0 19.1
41. t - - - -
31 .I 30 5.9
Fultdu~ "° bo(h' . !
~' tol l lac]#
.\'<,. %
26 50.0 91 79.8
117 23.0
996 AmerTcan Journal of Digestive Diseases

Gastric with Duodenal Ulcer
I t should be noted, however, tha t in the series of Comfor t e t al . '~ some differences in the d is t r ibu t ion ot GU in C G D U and single GU were found. In the C G D U g r o u p the GU was located in the area ot! the pylorus and pyloric an t rum in 57.8°~ of the cases and along the middle 1,, a of the lesser curwtture in 41.4'/~,. In the g r o u p of single benign GU, however, only ,t8.9°,~ were [ound in the pylor ic and antra l areas and 48.7(70 a long the middle 1/!~ of the lesser curvature .
In one selies ~ m u h i p l e gastric uh:ers were found to occur almost twice as often in patients with coexisting DU' s as in pat ients with gastric locali- zation of the lesion only, and in o ther series ~'. 4a m u h i p l e G U ' s were found in 90~ and 14,°0 of the cases of C G D U .
DIS'I'RH~tTI'IO.'X" OF C G D U A c c o m , x(; TO SEX AND AGE
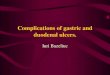
Figure 1 shows tile d i s t r ibu t ion of C G D U according to sex and age. T h e male : female rat io varied f rom 2.5:1 to 4.9:1 (mean 3.9: 1) in various series. Th i s mean figure is identical with the rat io f o u n d for C G D U (3.9:1) in Central Middlesex H o s p i t a P bu t closer to the figure for GU
found there lot 271 GU's (2.4:1) and 691 DU' s (6.8:1).1"_, Age dis t r ibut ion for C G D U shows un i fo rmi ty in different series. T h e
peak incidence occm-s between 40 anti 70 years, which parallels the age dis t r ibut ion of ( ;U. Statistical data at the Central Middlesex Hospital~=" showed that the age of peak incidence for G U and C G D U was between 45 anti 55, while that for DU was between 35 and 45. T h e pos tmor tem survey at Leeds Genera l Inf i rmar) ~3 shows a similar dis t r ibut ion. T h e study by C o m f o r 0 ~ also reveals a similar age d i s t r ibu t ion for C G D U and GU patients (50.3 and 53.4 years, respectively). T a n n e r TM noted in his
N o . o f RLtAo A g e : A u t h o r C a s e s M F M : F ) Z 5 Z S - Z 9 5 0 - 3 4 3 5 - 3 9 4 0 - 4 4 4 5 ~ 4 9 5 0 - 5 4 5 5 - 5 9 6 0 - 6 4 6 5 - 6 9 7 0 - 7 4 ) 7 4
9 M a n g o l d 157 125
W a t k i n s o ~ 3 2Z7 174
2 oh~lor~ 16 119 96
Gelb et &~5 53 38
C o m ~ q ? ' t 184 153 e t &l
~ a u c h 52 90 74
32 3 . 9 : 1 ~ q 27 J 5?. t
53 5 . 3 : I ~-3-+-- - 13 + 2:?. I 52 ......
23 4 , Z : 1 ~ - ~ ? * - - - ~ 13 I 34[ t a.3
15 2 . 5 : 1 ~------'Z ~ 4 ~ 7 4 16
S l 4 . 9 : 1 Mee, n A g e ~s4aS.eff = 4 9 . 9
16 4 . 6 : 1
4B * 28
72: ~ 4 9 * L ~
I 17 : 7------~
15 : 9 :
M e a n A g e ~ e m a l e 2 ~ 5 0 . 8
Toga,Lll 830 660 170 3.9:1
Fig. 1. Distribution of CGDU according to sex and age.
New Series, Vol. 8, No. 12, 1963 99'7

Weisberq & Glass
group of surgical cases that the age at operation o[ the CGDU patients was close to that of GU patients.
Thus, it would appear that both the sex ratio and the age ot' peak in- idence for CGDU tend to approximate those for GU.
G A S T R I C A C I D SECRETION
Acid secretion in patients with CGDU has been shown to range be- tween that of patients with GU and DU or to approximate that of DU patients.
Marks arm Shay, 1'~ using the augmented histamine stimulation tech- aique of Kay ( M H R and MAO), and Comfort et al . T1 using the Ewald meal, reported acid valties for CGDU intermediate between those ob- served in GU and DU. In two other studies, one using tim measurement of nocturnal secretion ~ and the other a 24-hour test meal, ~; acid output was found to approach the DU pattern of hypersecretion. In only one study, using submaximal doses of histamine, were secretory values re- ported to be in the normal range. 4a
DIAGNOS IS AND C I . I N I C A I . COURSE
Tile diagnosis of CGDU has been made chiefly by X-rays or at opera- tion (Table 6).
\Vhile gastrointestinal X-rays are relied upon most frequently, the diffi- culties inherent in their interpretation in cases of CGDU have been un- derscored.n.~a hi 184 cases of CGDU ~ tim GU was missed by the ra- diologist in 37 instances (20r~,) and the DU in 41 cases (22~,). These errors were attributed (1) to the focusing of the radiologist on either the gastric or duodenal lesion, to the exchlsion of a second one, and (2) to the difficulty encountered in visualizing small gastric (prep,~loric) ulcers in the presence of varying degrees of pyloric obstruction.
Surgical exploration yields greater diagnostic accmacv. The difficuhies inherent in this metllod, similar to those confronting the radiologist, have
T A B L E 6. M E A N S O F D I A G N O S I S OF C G D U
Sit r ife~' X- ray ?,to.
A u t h o r cases N o . ~ , N o . %
A a g a a r d e t a l2 ° 118 108 91.5 10 8.5 M o r r i s o n g: F e l d m a n TM 21 - - - - 21 100.0 M a n g o l d 9 145 6 4. I 139 96.0 Sm i t h e t at. ~ 190 - - - - 190 I00.0
TOTAL 474 114 24.0 360 76.0
998 American Journal o{ Digesf~ve Diseases

Gastric with Duodenal Ulcer
also been emphasized. 1~, ~G T h i s is especial ly t rue for the surgeon opera t -
ing in an emergency such as p e r f o r a t i o n or h e m o n h a g e . T h e diagnosis of C G D U o n pure ly c l in ica l g rounds is ditticult. \V i th
the excep t ion of a t endency toward a longer d u r a t i o n of symptoms, the
ma in characterist ic, pain, was genera l ly ind i s t ingu i shab le f rom that due
to s i n g l e G U o r D U . 9, 11
In eva lua t ing the recur rence of nicer symptoms, o n e has to consider
that in a n u m b e r of such cases the r e (u r r enc e of symptoms may well be
due to the d e v e l o p m e n t of a new ulcer r a the r than to the ac t iva t ion of an
old one. In 41 of 104 pa t ien ts wi th C G D U ( 3 9 ~ ) in w h o m the DU was
d o c u m e n t e d as the ear l ie r lesion to appear , a symptom-fi-ee in terxa l of at
least one year was no ted be tween the onset of symptoms and the i r recur-
fence, at which t ime a new gastric lesion was demonstra ted." ~ Similar ly ,
in ano the r series of 2i D U patients , 6 expe r i enced a recur rence of symp-
toms f iom 1 to 27 years later, at which t ime the ear l ie r D U was radio-
logically shown to have comple te ly hea led and symptoms were due to the
d e v e l o p m e n t of a new GU. as
T h e act ivi ty of the lesions at the t ime of diagnosis or p o s tm o r t e m is
listed in T a b l e 7. At the t ime of c l inical diagnosis the mos t f r equen t find-
ings were act ive lesions at bo th sites (41.7°~,) or a healed D U coexis t ing
with an act ive G U (39 .5%). T a n n e r TM es t imated from his own surgical
mater ia l that the c o m b i n a t i o n of a healed D U and active G U accounted
for 90~, of the cases of C G D U c o m i n g to smgery. In those cases in which
the D U was ful ly act ive the G U was of ten in an early or suhacute stage.
T h e most f i e q u e n t pos tmor t em f inding was a healed lesion at bo th sites
(38.3%) and somewha t less f r equen t ly a hea led D U and active G U
(33.9%). Thus , the na tu ra l h is tory of C G D U is p robab ly as follows: tim Did is
TABLE 7. ACTIVITY OF UI.CERS IN CGDI" AT TIME OF DI\GNOSIS OR .'~T AUTOPSY*
B o t h ulcers H e a l e d D U , .4rlb,e DU. f t e , led DU. act ive act ive G U hea l ed G U hea l ed G U
A u t h o r ca~es No . % No . % No . o~, No. °7 o
Johnson TM 110 26 23.6 75 68.2 6 5.5 '~ 2.7 Morrison
Feldman is 2I 15 7I .5 6 2 8 . 5 . . . . Aagaard et alY' 79 14 17.7 64 81.0 - - - - 1 1.3 Mangold 9 157 98 62.4 Tanner TM 90.0 Tovm. 367 153 41.7 145 39.5 6 1.6 4 1 I *Watkinson '~ 227 49 21.6 77 33.9 14 6.2 87 38.3
New Series, Vol. 8, No. t2, ]963 999

Weisberq & Glass
the earlier lesion (Table 4), and as it progresses to chronicity or healing, t , e ( ;U ~teveiops. ~lhis is shown by the tart that the two largest c l inkal groups (81.2(/o) are fornmd of patients in whom the DU and GU are both a~tixe or in whom the DrY has progressed to complete healing, leaving an active GU.
Since the coexistence of healed lesions at both sites was the nlost fre- quent pos tmor tem trading (38.3~'~,), it appears that in a mmlber of these 1)atient~ tile course of the disease is favorable. Either spontaneously or as a result of therapy, complete healing of both lesions takes place. T h a t tile group with active lesions at both sites also consists of patients in whom the clinical course is not so favorable is suggested by the fact that they lonn a substantial p ropor t ion (21.6{'~) of CGDU at autopsy.
PATHOGENESIS
Both tile pr imacy in t ime of tile DU and tile frequent finding of acid hypersecretion have strongly intluenced tile concepts advanced to explain tile pathogenesis of CGDU.
It has been suggested that patients with CGDU have a primar) I)U, Ihe course of which is complicated hv the development of pyloric obstrtlc- tion. 1< 1:' T h e latter may be due to spasm, scarring, and deformity of the pyloric region following DU, leading to impaired gastric emptying and gastric retention. XVhile in patients with pyloric stenosis and nornlal acid secretion intragastric bulfering mechanisms may be adequate in neutraliz- ing acid retained in the stomach, in patients with acid h)persecretion nor- mal buffering may be inadequate and resuh in the formation of :t sec- ondar,v GU. 1G
An addit ional nlechanisnl operat ing under these circmnstances has been suggested by Dragstedt. ' : ' This was based upon his investigations into the different phases of gastric acid secretion in DU patients. Ac(ord- ing to Dragstedt, the DU in the major i ty of these" patients is usually the result of the vagally mediated, high basal acid secretion. \Vhen the DU is followed by pyloric obstruction, antral stasis will develop, st imulating ill turn the release of gastrin, e° thus fur ther increasing gastric acid se(re- lion. Once again, the combinat ion of pyloric obstruction anti acid hyper- secretion will favor the format ion of a secondary GU.
In support of this view, Johnson 'e' has reported that of 119 patients with CGDU, 76 (64%) had clinical, surgical, or radiological evidence of gastric retention, including 39 (33°~) with well-marked pyloric stenosis at surgery. He also noted that of 331 patients admit ted for pyloric steno- sis, 52 (16°~,) had GU. Of 16 cases with pyloric channel ulcer disease reported b v Burge et al. ," ' 9 (56(~,) had, in addition, a benign GU along
1000 American Journal of Dicjestlve Diseases

Gastric w;th Duodenal Ulcer
the lesser curvatme. Ahhough details regarding gastric emptying time were not given tor all cases, the authors state, "The re can be little doubt that the associated simple lesser curve gastric ulcer is (aused by gastric stasis in the pyloric channel syndrome."
The presence of pyloric obstruction in patients with CGDU has not been a constant finding, however. Using a retention meal, Aagaard et al. TM
found delayed gastric emptying in only 13 (16.0~0) of 81 patients with CGDU, and of 86 patients subjected to surgery, only 10 (11.6('~) showed evidence of pyloric stenosis. Mangold;' found either clinical or radiologi- cal evidence ot gastric retention in only 25 (19~(~) o[ 1,'41 patients with CGDU, and at surgery pyloric stenosis was present in only 12 (9.25~,). Of 51 cases of CGDU reported by Bernardo," ' only 9 (17.6~o) had evi- dence of pyloric obstruction on admission, and of 53 cases reported by Gelb and Becket, ~a g,'istric re tent ion was present in only 5 (9.4°0).
T h e fact that the GU is the first lesion to appear in a small number of cases also suggests that the development of pyloric obstruct ion is not the only pathogenetic mechanism responsible for the development of CGDU.
Decreased gastric mucosal resistance to acid hypersecretion has also been incriminated in the pathogenesis of CGDU. Several attthors have in the past suggested that the healing of DU coincides with the development of an associated gastritis in the hypersecreting s tomachJ 4, '_,a. e4 Heal ing under these circumstances may actually be due to the fall in acid secretion following inflammatory i n v o h e m e n t of the stomach. It has been sug- gested fur ther that persistent gastritis, together with the development of atrophic mucosal changes, lowers mucosal resistance as well and predis- poses to gastric ulcerat ionJ ~ This wouhl apply especially to cases of long- standing acid hypersecretion. ~a
Thus, the pathogenesis of CGDU may be no diff'erent from that of GU or DU occurring alone. T h e DU is the first lesion m appear in the ma- jority of cases since gastric mucosal resistance to acid hypersecretion is normally greater than that of the duodenum. T h e developInent of a (o- existing GU would then depend upon the degree and durat ion ot the gastritis and acid hypersecretion associated with the DU. T h e fact that, generally, free acid values are lower in patients with CGDU than in those with DU may be a consequence either of the associated gastritis or of the "zonal" gastritis surrounding the GU. -"a
While there is indeed evidence that chronic, and even atrophic, gastritis occurs to a greater or lesser degree in all patients with DU, this incidence varies greatly with the diagnostic method used. I t has been described as occurring cons i s ten t lyy --~s in slightly less than Ve of the cases, e~'. s0 occa- sionally,2a.."~. :u. a'.' anti infrequently, aa Where the antral region was ex-
New Series, Vol. B, No. 12, 1963 1001

Weisberq & Glass
amined histologically ill surgical and pos tmor tmn specimens, however, this was ahnost invar iably the site of active in l tammation. 2U-2s
Why the associated antra l gastritis should progress to f rank ulcerat ion in only a relat ively small n u m b e r of DU pat ients is not clear. Pyloric ob- s t ruct ion is not likely to be a critical tactor in view of its absence in m a n ) cases ol C ( ; D U . T h e small n u m b e r of cases in which the GU is the earlier lesion to appea r is also unexp la ined by this sequence of events.
I t is possible that the role of inher i tance may be significant in this re- gard. Doll and Kellock a4 f o u n d that 11 pat ients with C G D U had 18 rela- tives with pept ic ulcer, of w h o m 4 were siblings who had C G D U . In sev- eral of Mango ld ' s ' cases of C G D U near relatives were shown to be simi- larly affected.
Accord ing to Johnson, :~:' a p r e p o n d e r a n ( e of his patients with C(;I ) [J was of the b lood g r o u p O, most character isuc tor British patients af- le t ted with pept ic ulcer and par t icu lar ly DI.j. a~ as Similar findings were reported by Bi l l ington a:' in a large grou I) of Aust ra l ian patients. In some series,aT, as. 4o. 4~ while the major i ty of pat ients with C G D U were of the blood g r o u p O, the statistical significance of the quant i ta t ive difference between each of the b lood groups in cases of C G D U was not determined. In 2 of these, a< az a l t hough the b lood type O was found more f requent ly a m o n g pept ic ulcer pat ients than in a referente g roup and the association between the b lood g r o u p and pept ic ulcer was statisti(allv significant, no significant difference was found between DU and GU.
Thus , the p ropo r t i on of relatives with ulcers at 2 sites apl)ears to be great ly increased when proposi t i are similarly affected, and there is a tendency toward the p r edominance of blood g roup () in l)atients with C G D U .
\Vhile the significance of these findings is not certain, it may be that a critical factor in the pathogenesis of C G D U is wholly or l)artlv genetic:d- Ix' condi t ioned .
C O M P L I C A T I O N S Pyloric Obstruction
Pvloric obs t ruc t ion with gastric re tent ion is a more or less p rominen t ('omT~lkation of C G D U and has already heen discussed in the section on pathogenesis.
Hemorrhage
In one series of 157 patients/~ 59 (37.6~,) had a total of 89 hemor- rhages. In 91 pat ients of this series in w h o m the sequence of develop- ment of the lesions was k n o w n (the DU preceding the G U ) , there were .8(; instances of b leeding in 27 patients, all occur r ing within a year follmv-
1002. Amedcan Journal of D~gestive Diseases

G~stric with Duodenal Ulcer
ing the diagnosis of the combined lesion. The GU proved to be the source of the bleeding in 16 (60')o) of these patients and in the remainder the bleeding site was not determined. In at least 45 patients (28.5%) hemorrhage took place while both the GU and DU were coexistent for a little more than 1.5 years. Thus, at least every third patient with CGDU bled at least once, and most of them within a short time following the diagnosis. This incidence was higher than that in the period preceding the CGDU and higher than that observed in a comparable time perio:l in patients with GU or Did a l o n e Y '-~a
In another series of 119 patients with CGDU, ~ 47°,~ experienced at least one episode of hemorrhage and, of these, _..9"°:.o had several episodes. The incidence of hemorrhage in the general GU populat ion from which these patients were drawn was only 8, 0 for the same time period. Thir- teen patients with C(;DU underwent emergency gastrectomy for active bleeding and GU was the source of the bleeding in all of them. In 2 pa- tients, bleeding was from several acute gastric ulcerations.
Of 53 cases of CGDU reported by C-elb and Becker ~a, 28 experienced at least one hemorrhage and 9 of these experienced more than one.
Hemorrhage is therefore a prominent complication of C(;DU, oc(ur ring in from 37.6'!~, to 53['~, ot the cases and often within a short time following the development of the two coexisting lesions. The most fre- quent source of bleeding was the GU, accounting for 60~v~ to 100°~, of those cases in which the bleeding site was identified.
Perforation The incidence of perforation was 24 times in 22 patients (14°~,) in one
series of t57 cases of CGDU, ~ and 5 times in 3 patients (5,6<71,) in another ,eries of 53 cases?:' \Vith two exceptions, all perforations occurred in the duodenum.
7~IORTALITY IN CGDU
johnson TM placed the mortality as high as 10'~, in his surgical series in contrast with an over-all mortality of 4°~, noted in a series of 3000 gas- trectomies. Mangold:' reported 5 deaths (3.2[~,) directly attributahle to ulcer disease in his group of medical and surgical patients, In a postmor- tem survey, ~Vatkinson 1:~ noted 85 deaths (37(r~,) due to ulcer disease in 227 patients with CGDU, of which 73 were in men and 12 in women. This compared with 531 deaths (32.85{,) due to ulcer disease in 1621 pa- tients with either GU or DU alone. In the group of patients with CGDU, death was most often caused by active lesions at both sites or to a chronic gastric ulcer in the presence of a duodenal scar.
New Se~ie~, Vol. 8, No. 12, 1963 1003

Weisberq & Glas~
It appears, therefore, that GGDU tends to run a more sexere course with a higher mortality rate than that due to either Gtl or 1)U alone.
T R E A T M E N T
Because ol the more severe course and higher incidence of complica- tions in patients with CGDU, greater emphasis has been placed upon surgical treatment. Partial gastric resection has emerged as the proce- dure of choice with no apparent dit[erence in the resuhs obtained with either the Billroth I or Billroth II operations.
\Valters 4~ observed 7,'4 patients with CGDU for a period of 5 years, 54 (74cJo) of whom had been subjected to Billroth 11 gastrectomy and 19 (26(Jo) to Billroth i. There were no recurrences in either group during the period covered by the stud), Hickenbotham ~7 performed Billroth I operations on 19 patients with CGDU with one operatixe and 2 postdis- charge deaths. There was one relapse during a 2-}r. follow-up period. Johnson a° strongly urges that all cases ol CGDU be treated by surgical procedures designed to control h)persecretion o[ acid. This should con- sist either of extensive Billroth 11 resection or a more limited resection combined with vagotomy.
Following the hypothesis that in CGDU the GU is caused by an aug- mented gastrin phase of gastric secretion in patients with a primary DU complicated by pytoric obstruction and gastric retention, several authors described the treatment of 4 patients with CGDU by means of vagotomy alone or vagotomy combined with gastroenterostomy or pyloroplasty. In all cases, the ulcers healed promptly. For similar rea- sons, Burge e t a l . "q treated 9 patients with pyloric channel ulcers and as- sociated lesser curvature ulcers with vagotomy and ])ylorol)lasty. Imme- diate resuhs were described as encouraging.
In one series of 157 patients, 9 82 (5200) were subjected to one or more operations, ol which 68 were partial gastrectomies; In another series, 4a 30 (57"(~) of 53 patients with CGDU underwent partial gastrectomy. In the
latter series the indication for surgery in most of the cases was hemor- rhage. In the remaining 23 of these 53 cases, medical therapy was applied with good results including healing of ttle gastric ulcers as confirmed by repeated GI series.
No detailed, controlled study of the results of medical versus surgical therapy is available and therefore no adequate comparison of these two modalities is possible at this time. However, the autopsy finding of a high proportion of healed lesions at both sites (38°~,) suggests that in a large group of these patients healing does oc(-ur and that such a comparative study is warranted.
1004 American Journal of Dicjesfive Diseases

Gastric with Duodenal Ulcer
SUMMARY AND C O N C L U S I O N S
The literature on coexisting gastric and duodenal ulcers (CGDU) cov- ering the past 10 years, encompassing a total of 1490 cases, is reviewed. This forln of peptic ulceration comprises 6.~r,°'/o of all peptic ulcers, 23.5% of all benign gastric ulcers (GU), and 7.3°0 of all duodenal ulcers (DU).
When cases of CGDU are compared with those of single GU or DU, the following features of CGDU are apparent:
1. The DU is the earlier lesion to appear in the majority of cases. 2. The acid secretory pattern in the majority of cases is either inter-
mediate between that of DU and GU or tends to approach that of DU. 3. The most common clinical feature is an active lesion at both sites,
the next most common finding being a healed DU and an active GU. In contrast, the most frequent autopsy finding in these cases has been a healed lesion at both sites.
4. The incidence of complications in CGDU, especially hemorrhage, is higher than that for GU or DU alone. In hemorrhage, the GU is the most frequent site of bleeding; in cases of perforation, the duodenum is the main site.
5. The incidence of malignancy is lower in the GU of CGDU than in GU occurring alone.
6. As in cases of GU occurring alone, the most common sites of GU in CGDU are the pyloric antrum and middle 1/~ of the lesser curvature.
7. The sex ratio and age distribution for CGDU are intermediate be- tween those for DU and GU occurring alone, with a tendency for the sex ratio (males predominating) and the age distribution to parallel that for GU.
8. The duration of pain in CGDU is somewhat longer than in GU or DU alone. The characteristics of the pain itself, however, are indistin- guishable from those due to either GU or DU alone.
9. Because of the more severe course of CGDU, the higher incidence of complications, and the higher mortality, emphasis in recent years has been on surgical treatment. There have been no controlled studies, how- ever, of the usefulness of medical therapy in this condition, al though there is evidence to suggest that it may be of value in selected cases.
Section of Gastroenterology Metropolitan Hospital
1901 First Ave. New York 29, N. Y.
REFERENCES
1. IvY. A. C.. (',ROSS~f~X. M. I.. and BACHRACH. ~,V. H. Peptic Ulcer. Blakiston. New York. 1950. pp. 17. 315, 649650.
New Series, Vol. 8, No. 12, 1963 1005

Weisbercj & Glass
2. SHAY, 1{., and Sux, D. C. H. Etiology and pathology of gastric nicer. Ill (,astro- enterology, Vol. I, Bockus, H. L., Ed. Saunders, Phi lade lphia , 1963, pp. 448-451.
3. BALINT, R., Ci ted in HURST, A. F., and S'rI~WART, M. J. Gastric and Duodenal Ulter. Oxford, London , 1929, pp. 57-59.
4. MUIJ.ER, O. Cited in HURST, A. F.. and STEWARI ", ~[. J. Gastric and I)uodetmt Ulcer. Oxford, London , 1929.
5. HOLI.ANDER, F. Are ga~r ic and duodena l ulcers different diseases? S, Clin. North America 27:265, 1947.
6. CARMAN, R. D. Roen tgen diagnosis of concur ren t gastric and duodena l ulcer. Am. ]. Roentgenol. 4:552, 1917,
7. VCn,Kir;, D. P. D. Coinc iden t duodena l and gastric ulcer. B~it. M. I. 2:469. 1926. 8. FI~LD,~IAS, M, T h e incidence of the coexistence of gastric and duodena l ulceration.
Gastroenterology 23:304, 1953. 9. MAXCOLD, R. C o m b i n e d gastric and duodena l ulcerat ion, B~it. M. ]. 2:1193, 1958.
10. AAGAARD, P., ANDREASSEN, M., and KIRZ, L. Duodena l and gastric ulcer in the same pat ient . Lancet 1:1111, 1959.
11. COMFORT, M. W., PRIESTI.EY, J. T.. DOCKERT'¢, M. B.. X~'EBER, H, M.. GAt;L', R. P., Soils. J., and EVI'ERSON, D. P. T h e small benign and m a l i g n a n t gastric lesion. Su*g. Gvnee. ?: Obst. 10~:435, 1957.
12. Joxr:s. F. A., and POt,LACK. H. Civil ian dyspepsia. Brit. M. J. 1:797. 1945. 13. ~,V:vrKiNsox, G. q-he incidence of chronic pept ic ulcer found at necropsy. Gut l:
14. 1960. 14. TANNER, N. C. Surgery of peptic ulcerat ion and its complicat ions, Postgrad. Med.
]. 30:~48, 1954. 15. MARKS, I. N., and SHAY, H. Observat ions on the pathogcnesis of gastric ulcer.
Lancet 1:1107, 1959. 16. JOHNSON, H. D. T h e special significance of concomi tan t gastric and duodenal
ulcers. Lancet •:266, 1955. 17. V¢:~'rKINSON, G. A s tudy of the changes in p H of gastric contents in peptic nicer
us ing the 24-hour test meat . Gastroenterology 18:377, 1951, 18. MORRISON, S.. and FH,DM.~N, M. T h e hea l ing of a p r imary duodenal ulcer with
the later deve lopmen t of a gastric ulcer. Am. J. Digest. Dis. lS:296, 1951. 19. DR~.CSTEIYr. I , R. T h e pathogenesis of gastric and duodena l ulcers. Ann. New Yo;k
Acad. So. 99:190, 1962. 20. Ru:t.r3R. S. P., OI~rRHEI.XIAX. H. A., JR., BR~Sm.:R. T. H.. and I)RXCSrFt3T. L. R.
Pvloric stenosis and gastric ulcer. Ar(h. Sung. 71:191. 1955. 21. BtR(;t:, H., (;[I.L, A. M., and LEw~s. R. H. T h e pyloric channe l syndrome and
gastric ulcerat ion. Lancet 1:73. 1963. 22. BERNARDO, J. R., SOI)ERBERG, C. It., and Mmrl:~Celx. . \~ V. ( ,astric ulcer. Surgery
44:804. 1958. 23. PAl,Mr R, E. D. On the morphologic state of the gastric mucosa in the duodenal
ulcer pat ient . Gastroenterology 18:8, 1951. 24. Wooo, I. J., and TART, L, I. Diffuse lesions of the s tomach. Arnohl . 1,ondon. 1958. 25. C.~,Rn. W. I., and MAR~S, I. N. In Modern Trends in Gastroenterology, 2nd series.
Jones. F. A., Ed. Hoeher . New York, 1958, p. 187 26. MAt';Sis. H. A. In 31odern Trends in Gastroenterology, 1st series. Jones. F, A,. Ed.
But te rwor th . London . 1952. p. 346. 27. KONJEZTNY, G. E. Die entzi indl iche G r n n d l a g e der typischen Geschwfirsbihhmg im
Magcn u n d D u o d e n u m , Springer, Berlin, 1930, p. 155. 28. HEI~m!J, R. Chronic gastritis: its relation to gastric and duodena l ulcer and to
gastric carcinoma. Am. J, Path. 19:43, t943. 29. JosKt:, R. A,, FIXC~H. E. S., and Woon. I. J, Gastr ic biopsy: a s tudy of 1,000 con-
secutive successful gastric hiopsies. Quart. J. 3led, 24:269, 1955.
1006 American Journal of Dicjes¢ive Diseases

~astrlc with Duodenal Ulcer
30. P c . t , I1. Die V e l l i n d c n m g c n der l ) uodena l s ch l e imhau t beim Ulcusleiden, Arch. path. Anat . 265:160, 1927,
31. RmKt:rrs, W. E., K1RSXr:R, J. B., and Pu.~It:R, W. I,. T h e gastroscopic appearance of the gastric mucosa iJ~ pept ic ulcer. A m . y. M. So. 217:542, 1949.
32. 1)E Ia:CA, V. A., Ja., and SmRO, t t . M. (;astric mucosa in acute duodena l ulcer. Arch, Int . Med. 3:145, 1963.
33. ~V:~,LTERS, XV., and Sr:uE,xix{;, ~V. A compar i son of lesions associated wi th duodena l ulcer in G e r m a n y and in the Uni ted States. Minnesota Med, 15:579, 1932.
34. DOLL, R., and KELLOCK, T. 1). T h e separate inher i t ance of gastric and duodena l ulcers. Ann. Eugenics 16:231, 1951.
35. Jonxso,x, H. D. Etiology and classilication of gastric ulcers. Gastroenterology 33: 121, 1957.
36. AIRD, L., BEXT.~t.I, H. A., NIEHIG3,N, J. A., and ROBERtS, J. A. F. T h e blood g roups in relation to peptic ulcerat ion and carc inoma of colon, rectuln, breast and broil- chus, Brit. 31. J. 2:315, 1954.
37. CLARKt. C. A., Cow:,,x, XV. K., XV~'x EmvAaoS, J., HowH, l:Ex,xys, A. XV., McCoxxrt , l . , R. B,, WOODROW, j . c . , and SHzt'l'.~RI), P. M. T h e re la t ionship of the ABO blood groups to duodena l a0d gastric ulcerat ion. B~it. M. J. 2:643, 1955.
38. PI<F.BI,IqS BROWS, D. A., MEt~ROS~:. A. G., and XVAI,LXC'E, J. T h e blood groups in peptic ulceration. Brit. M. J, 2:135, 1956.
~'~9. BII,LINt;TOS, B. P. C o m b i n e d gastric and duodena l ulcer. Imnte t 2:753. 1958. 40. Kos'rtR, K. H.. SlYl~Rll', E., and SEELF, V. ABO blood g roups and gastric acidity.
Lancet 2:52, 1955. 41. BUCKWAI,TER, j , a . , W o m w E x o , B. E,. CoI:rFR, D, C., TIDRICK, R, T,, and Kxowt,rlt ,
L, A. Peptic ulcerat ion and ABO blood groups. J.A.M.A. 162:1215, 1956. -t2. MARTL',', L., and Ltwzs, N. Peptic ulcer cases reviewed after ten years; effect of
medical t r ea tmen t and indicat ions for gastrectomy, Lancet 2:1115, 1949. 43. E~lFav. E. S., and MOXROL R. T. Peptic ulcer. Arch. Int . Med. 55:271, 1935. 44. BAt,rOt:R, D. C. T h e surgical t r ea tmen t of haemor rhag ic duodena l ulcer. Ann ,
Surg. 96:58I. 1932. 45. G~t.u, A. M., and BECKI~R, _\. C o m b i n e d gastric and duodena l ulcers, t . Mt . Sinai
Hosp. 29:426. 1962. 46. XV.xL'r~:as, '~V. Resul ts of the surgical t r ea tmen t of duodena l , gastric and gastro-
je juna l ulcer. S. Clin. Nor th America 8:921, 1957. 47. HmKIXBO'rHAM. P. T h e Bil l roth I gastrcctomy. Brit. ,1, Surg. 44:206, 1956. 48. DR~¢S'rEDT, L. R,, and ~Voomv:~RD, E. R. Coexis tent duodena l and gastric ulcers
treated by vagotomy and pyloroplast~. I,~t.M.A. 184:1014, 1963, 49. H , u p [ a , P, V., J~., and DaAC, SW~)T, t . R, Section of *agus nerves to s tomach in
t r ea tmen t of benign gastric ulcer. Arch. Surg. 35:141, 1947. 50. JoHxso.',', H. D. Associated gastric and duodena l ulcer, Surg. Gvnec. 6 ~ Obst. 102:
287, 1956. 51. (;t,}-xN, F., anti HAa~sox , C. S. Gastric resection in the t r ea tmen t of pept ic ulcer.
A~wh. Sung, 62:151, 1951. 52. RAvC~, R. F. An evalua t ion of gastric resection for pept ic ulcer. Surgery 32:638,
1952. 53. SstI'rH, F. H., BoLts, R. S., Ja., and Joat).~y. S. M. P rob lem of the gastric ulcer re-
viewed. I.A.M.A. 153:1505, 1953.
New Series, Vol. 8, No. 12, 1963 1007









![Advanced Hepatocellular Carcinoma...later, he presented hematemesis and an upper digestive endoscopy was performed, with small esophageal varices and duodenal ulcers Forrest IIc [8]](https://img.pdfslide.net/doc/110x75/608600fafd367b42502944cd/advanced-hepatocellular-carcinoma-later-he-presented-hematemesis-and-an-upper.jpg)