Embed Size (px)
Citation preview
Cognitive & Behavioral Consequences
of Traumatic Brain Injury in Adults
Presentation for the Michigan Public Health Institute
Kristen L. Votruba, Ph.D.
Outline• Traumatic Brain Injury (TBI) Basic Information
– Types of TBI– Frequency and Causes of TBI– Levels of TBI severity
• Potential moderators of cognition and emotion after TBI
• Cognitive Effects of TBI– Common cognitive problems– Recovery of cognitive skills and recommendations following TBI
• Psychological Effects of TBI– Common emotional and behavioral problems– Recovery in psychological functioning following TBI– Treatment of psychological problems after TBI– Caregiver Effects and Effects on Family Functioning following TBI
Types of TBI• Focal Contusions / Contact Injuries
– Contact between the brain & skull– Damage scalp, skull, and brain surface
• Most common damage is to orbitofrontal lobe and inferior anterior temporal lobes
• Diffuse Axonal Injury (DAI)– Brain is stretched and rotated within skull
• Stretching and twisting of nerve axons– Often result of acceleration / deceleration injuries– Often accompanied by loss of consciousness & associated with coma length
• Penetrating Injuries (GSW)– DAI and lengthy Post Traumatic Amnesia are less common– Infection and post-traumatic seizures are more common– Outcome worse than contact injuries but dependent on trajectory of projectile– Increased morbidity
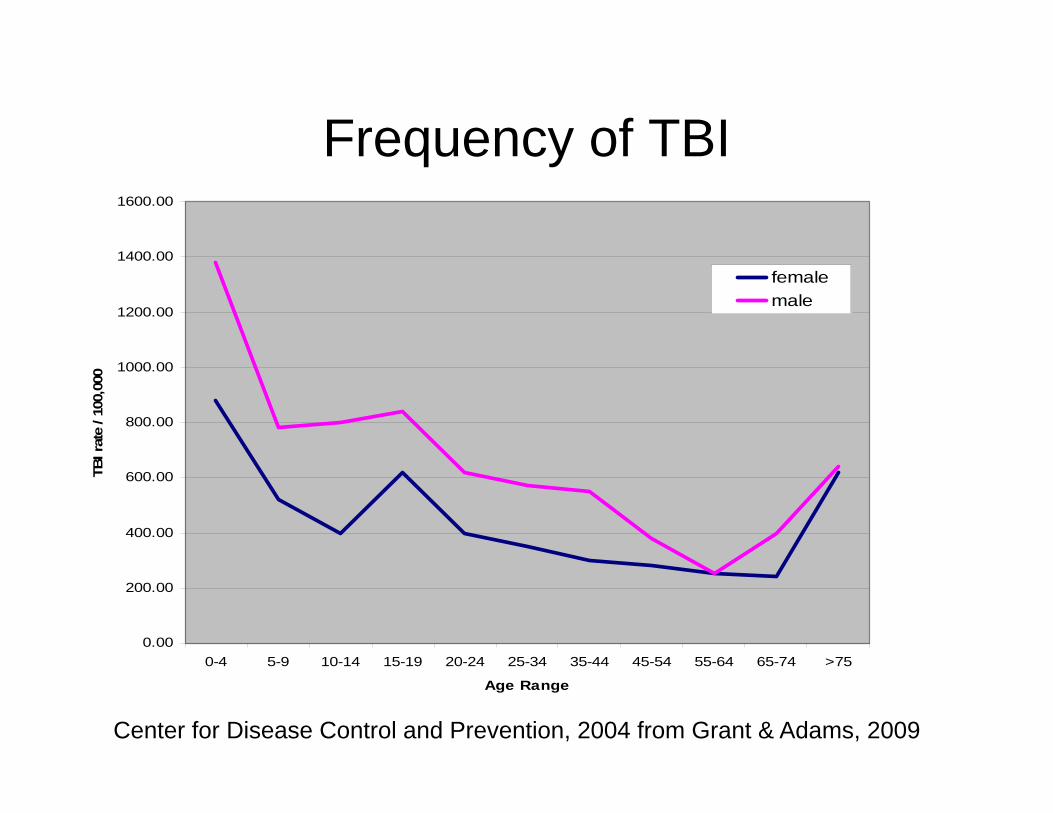
Frequency of TBI
0.00
200.00
400.00
600.00
800.00
1000.00
1200.00
1400.00
1600.00
0-4 5-9 10-14 15-19 20-24 25-34 35-44 45-54 55-64 65-74 >75
Age Range
TBI r
ate
/ 100
,000
femalemale
Center for Disease Control and Prevention, 2004 from Grant & Adams, 2009
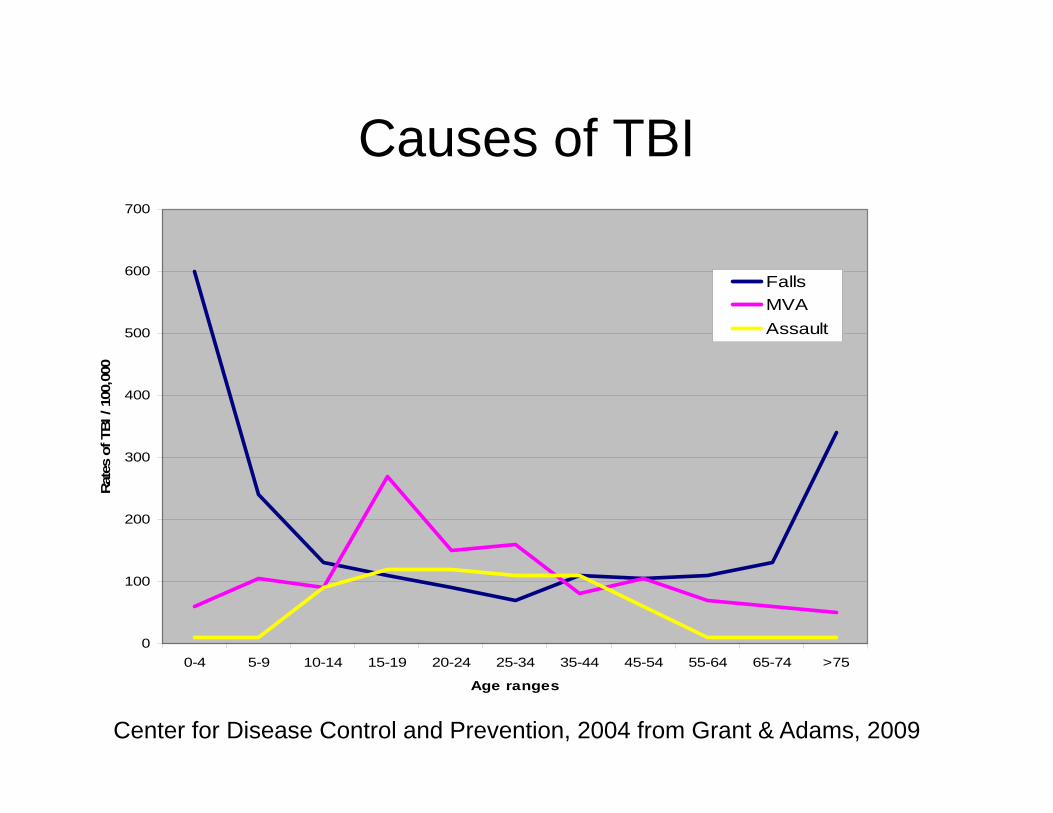
Causes of TBI
0
100
200
300
400
500
600
700
0-4 5-9 10-14 15-19 20-24 25-34 35-44 45-54 55-64 65-74 >75
Age ranges
Rate
s of
TBI
/ 10
0,00
0
FallsMVAAssault
Center for Disease Control and Prevention, 2004 from Grant & Adams, 2009
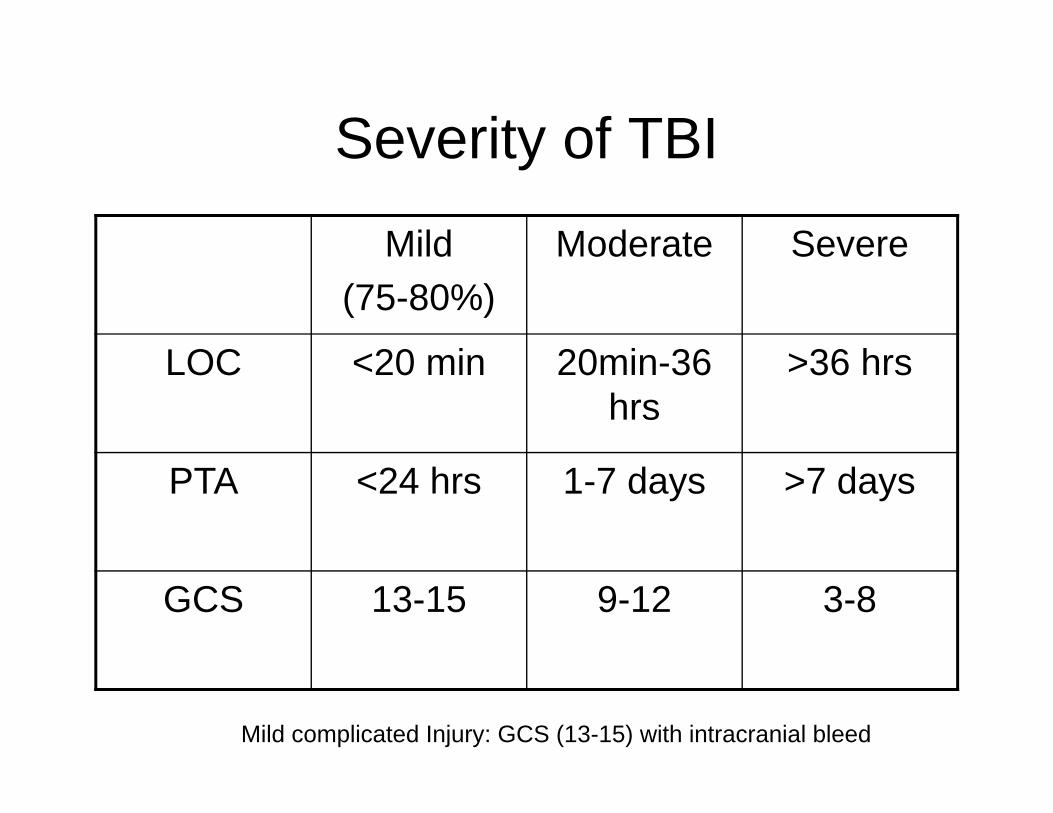
Severity of TBI
Mild (75-80%)
Moderate Severe
LOC <20 min 20min-36 hrs
>36 hrs
PTA <24 hrs 1-7 days >7 days
GCS 13-15 9-12 3-8
Mild complicated Injury: GCS (13-15) with intracranial bleed
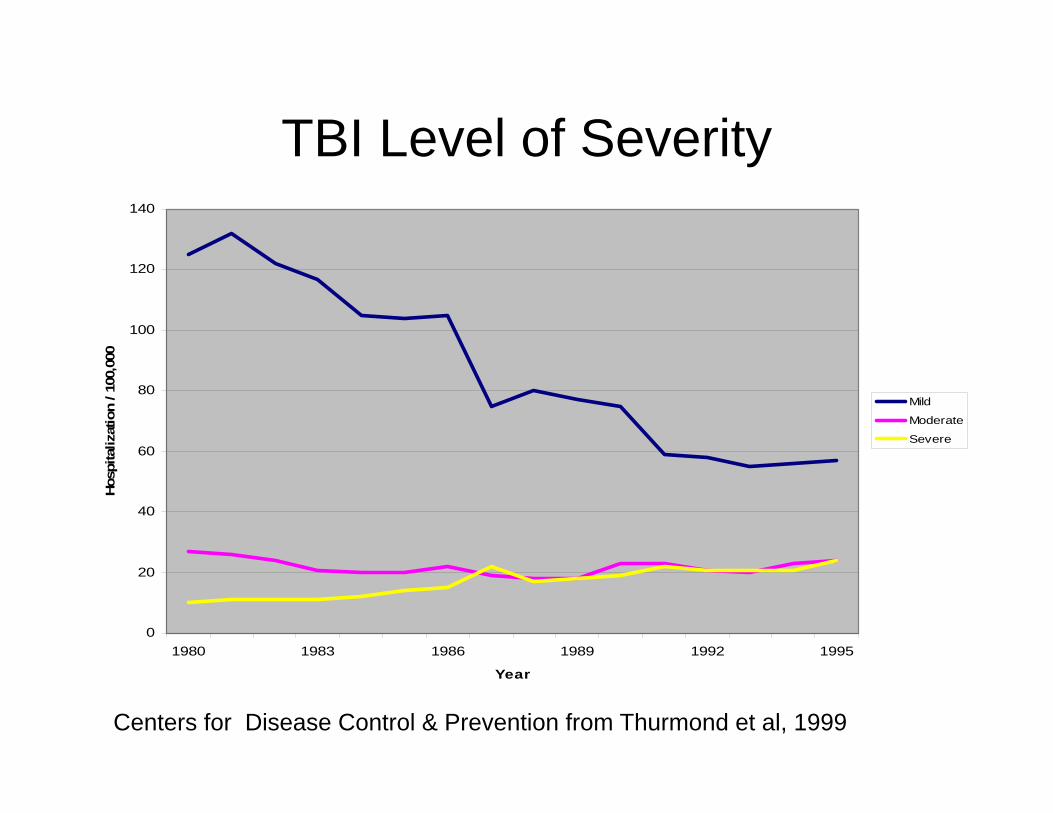
TBI Level of Severity
0
20
40
60
80
100
120
140
1980 1983 1986 1989 1992 1995
Year
Hos
pita
lizat
ion
/ 100
,000
Mild
Moderate
Severe
Centers for Disease Control & Prevention from Thurmond et al, 1999
Education• Cognitive Reserve Theory (Satz et al, 1993; Stern 2006)
– Higher levels of education and intellectual functioning protect against functional impairment as a result of neurological insult.
• Educational level has a moderating effect on memory functioning after severe TBI – Kreutzer et al, 1993
• One of the strongest predictors of social integration and outcome after TBI is pre-morbid cognitive functioning– Hanks et al, 1999
Alcohol Use• Effects of alcohol use is much debated
• Problematic drinking pre-injury has been related to greater memory deficits after severe TBI– Brooks et al 1989
• Those with a history of premorbid alcohol problems did not show any greater impairment than those without pre-existing alcohol use– Instead, subtype of individuals with low education, low
verbal intellect, and problematic drinking are at increased risk for brain injury
• Dikmen, 1993
Medication Cognitive Side Effects
• Anticholinergic agents • Anticonvulsants• Antipsychotics• Beta-blockers• Benzodiazepines• Barbituates• Cardiac glycosides• Centrally-acting anti-hypertensives• Gastric motility agents• Hypnotics• Opiates
Awareness• Capacity to perceive the “self” in objective terms, while
maintaining the subjective perception of one’s thoughts and feelings is difficult after TBI– Less accurate in reporting cognitive or emotional status– Suggests need for multiple measures to assess level of awareness
• Sherer et al (1998) – up to 70% of patients have impaired self-awareness after moderate to severe TBI
• Prigatano et al (1990) – more severe TBI, more variability in awareness
• Self-awareness better for physical abilities– less for cognitive and emotional/behavioral problems
Prognostic Indicators
• Positive Indicators– Initial GCS>9– PTA<24 hours– LOC<6 hours– Limited imaging findings– No dural penetration– No pupillary response
abnormalities– No hypoxia– No systemic complications
• Negative Indicators– GCS<9– PTA>24 hours– LOC>24 hours– CT / MRI findings– Pupillary response
abnormalities– Hypoxia– Ocular motor abnormalities– Secondary systemic
complications
Cognitive Effects of Adult TBI
Cognitive Impairment After TBI• Degree of neuropsychological impairment is greater
soon after injury with recovery occurring over days, weeks, months, years
• At one year post-injury, there is a dose response relationship between length of coma and cognitive outcome– More severe injury, more severe cognitive impairment– Length of coma most highly related to deficits in
WAIS-R PIQ at one month • Similar results at one year
– Dikmen et al, 1995
Cognitive Effects of TBIDikmen et al (1995) studied 436 people 1 yr after TBI
•TBI patients performed significantly worse than general trauma group on cognitive testing
- Most significant deficits on tests of attention, memory, and processing speed (most sensitive to TBI)
- Also more diffuse deficits in general intellect, motor skills, and problem solving
- If TFC less than one hour: same cognitive performance as trauma controls- If TFC between 1-24 hours: more impaired attention and memory- If TFC greater than 1-2 weeks: more global impairment
Arousal & Orientation After TBI• Deficits (and recovery) parallel severity of injury
• Changes in arousal common due to disruption between brainstem reticular formation & cortex caused by DAI– May be related to slowed reaction time and information
processing speed, and other attentional deficits
• Transient loss of orientation common– Orientation recovers first to person, then place, then time– Older patients have longer periods of impaired orientation– Older patients (and those with frontotemporal lesions) have
greater backward displacement than other groups• Backward displacement in time shrinks as recovery continues
• Older memories are less susceptible to disruption by cerebral insult than more recent memories
Attention After TBI• Span of attention preserved in most TBI patients
although can be compromised during post-traumatic amnesia (PTA)– 7 +/- 2 for 30-45 seconds
• Goldstein et al, 2001
• Attentional problems are typically more apparent in higher order tasks involving divided attention and cognitive flexibility– Impairment seen in reverse digit span or supraspan with 12-20
words
Memory After TBI• Impairment in memory also evident after TBI
– Slowed attention and information processing may contribute to clinical picture
• Severity of deficits related to severity of initial injury
• During PTA, often just procedural learning maintained
• After PTA clears, more forgetfulness and increased susceptibility to interference
• New learning on delayed tasks may be markedly impaired, if there is damage to medial temporal, hippocampal, and thalamic areas in moderate to severe injuries
• Degree of memory impairment may be disproportionate to impairment in intellectual functioning– 15% moderate TBI patients show worse memory than intellect– 30% severe TBI patients show worse memory than intellect
• Levin et al 1988 (5 months to 4 years post injury)
Memory After TBI• Poor consolidation and retrieval, with worse retrieval
• TBI patients make clear gains when given external structure, but not perfect– Show more semantic intrusions in free recall and recognition
• Impaired memory for contextual cues (time, frequency, source) – frontal damage
• More severe TBI reduced ability to benefit from repetition (reach learning plateau early)– Deshpande, Millis, Reeder, Fuerst, & Ricker, 1996
• TBI patients generally show poor awareness and significantly underestimate magnitude of memory deficits– Particularly in geriatric population
Language After TBI• Not classical aphasias after TBI, unless penetrating
injury or hematoma in language area
• See decreased comprehension, naming, spontaneous word-finding, and phonemic word generation
• Left prefrontal lesions– disorganized and impoverished language
• Right prefrontal lesions– tangential and socially inappropriate language
• Dysarthria also seen, not related to aphasia, and persist long past language recovery
Visuospatial Skills After TBI• Deficits may range from extraoccular
movements (compression of optic nerve) to cortical impairments in visuospatial organization
• Often TBI patients have deficits in early feature recognition such that they do not process small visual details as efficiently or as accurately
• May also see alexia, agraphia, agnosia, and poor visual concept formation
Executive Functioning After TBI• Executive dysfunction: perseverative language or
behavior, decreased cognitive & behavioral initiation, problems with interference control, decreased self-monitoring, poor planning, & poor problem-solving
• Tests tapping higher-order skills frequently are difficult for TBI patients due to the requirement of manipulation of multiple sets of data at one time
• These tests do not localize to a specific cortical region, but rather involve complex interactions between a variety of cortical regions that may be mediated by prefrontal areas
Effect of Executive Functioning Deficits on Other Cognitive Domains• May lose the ability to carry out a goal-directed
behavior due to problems with modulation of attention and behavioral action, as well as lack of initiation manifested in both inappropriate and impoverished verbal and behavioral activities
• Inability to maintain a goal state for an extended period of time may manifest as poor prospective memory (Fuster, 1995)– Seen in patients who cannot carry out a plan but can
verbally report what they were supposed to do
Executive Functioning Deficits Mimic Psychiatric Disturbance
• Set-switching and cognitive flexibility are particularly impaired after moderate and severe brain injuries
• Deficits in ability to anticipate consequences may manifest as impulsivity
• Deficits in ability to derive and implement a plan may manifest as overreliance on previously used plans of action (inflexibility) and becoming very anxious or irritated if deviations of pattern occur
• Concrete, rigid approach to problem-solving combined with inability to constructively incorporate feedback, individuals often find themselves in situations that are extremely frustrating
Cognitive Recovery in Adult TBI and
Recommendations to Address Cognitive Deficits
Recovery After Mild TBI• Multiple studies show cognitive problems after
mild TBI resolve within weeks to 3 months spontaneously without treatment – Dikmen et al, 1986; Dikmen et al, 2001; Levin et al,
1987; Barth et al, 1989; Macciocchi et al, 1996; McCrea et al 2003
• May have attention, processing ,and memory trouble at 1 month but normal at 3 months– 90% experience spontaneous recovery– Of 10% with persistent symptoms, factors such as
physical problems (dizziness, headaches), pain, fatigue, adjustment to return to work may affect cognitive and emotional functioning
Recovery After Mild TBI
• Minderhoud et al (1980)– Those informed about expected recovery from
concussion reported significantly fewer symptoms 6 months post-injury than comparison group
• Gronwall (1986)– Control group was 9 times more likely to have
significant PCS symptoms at 3 months as opposed to adequately educated group
Cognitive Recovery after Moderate to Severe TBI
• Millis et al 2001– Five years after TBI (N = 182)– Significant variability ranging from no
impairment to severe impairment• Using reliable change index:
– 22.2% improved– 15.2% declined– 62.6% unchanged
• Improvement most apparent on tasks of processing speed, visuoconstruction, verbal memory
Cognitive Recovery After TBI• Those with moderate TBI have more problems after
injury but recover similarly to mild complicated injuries – mildly impaired or WNL cognitive performance at 1 year
• Kashluba, Hanks, Casey, & Millis 2008
• After 1 year, TBI patients with more severe injuries performed 25 percentile points lower than trauma controls in attention, memory, & executive functioning – Dikmen, 1995
• Compared to controls, moderate to severe TBI patients showed deficits in sustained attention, verbal learning, & reaction time but preserved spatial working memory– Salmond et al 2005
Recovery and Outcome Prediction
• Best predictor of later cognitive functioning is early neuropsychological status
• Neuropsychological results shown to be better predictor than neurological severity– Hanks et al 2008– Those with severe cognitive impairment early
on make greater recovery over time • But when individuals have profound impairment,
little improvement.
Enhancing Cognition
• Not all cognitive deficits are organic:– r/o medication side effects and neurological
conditions– r/o mood disorders– r/o premorbid factors
General Intellectual Functioning
• Severe TBI associated with decrease in IQ– Particularly PIQ– …but do see recovery in PIQ
• 37% of severe TBI patients scored within one SD of normal at one year post-injury
– 44% VIQ and PIQ one SD lower than controls– 19% greater than three SD lower than controls
» IQ does not consistently associate with memory» Dikmen et al, 1995
Attention• Allow patient extra time to complete activities• Break down multi-step instructions to small bits• Prompting may help the patient stay on task• Focus attention over brief circumscribed time
periods. Short breaks may prevent cognitive fatigue or frustration
• Remove all potential sources of distraction• Devices (e.g., timers) may help focus attention• Psychostimulants
– Ritalin, Straterra• Improve arousal and speed of functional recovery
Initiation
• Problems with initiation result from damage to dorsolateral frontal, limbic, hippocampus, reticular activating system, substantia nigra, and locus coruleus– Implementing schedule and making it visible– Increase enjoyable activities– Psychostimulants can increase DA
(amphetamine, Ritalin) in mesolimbic areas– DA agonists (amantadine, bromocriptine) act
in bilateral thalamic and other diffuse areas to decrease apathy
Memory
• Due to damage to frontal, temporal, and thalamic areas
• Rule out attentional basis for problems
• Acetylcholine agonists (Aricept) can improve memory outcome
• Neuropeptides – excitation of limbic areas and enhancement of glutamate
Memory Behavioral Recommendations
• Associating new information with information with which the patient is already familiar
• Use of external memory aids– Pillbox – Notebook; lists; notes around the house– Audible timer
• Present information in a meaningful way• Information should be presented using both
verbal and visual information • Encourage patient to paraphrase, in their own
words what they hear
Language & Visuospatial Skills
– Language and visuospatial skills recovered to WNL within one year even after severe TBI
• Levin et al 1990– Comprehension recovers well, but naming, word
finding and word generation deficits more likely to remain (but subtle)
– Use direct and simple language; always reducing verbal instructions to their smallest units
– Incorporate visual aids as much as possible
Executive Functioning
• Structuring day-to-day functions through the use of routine and keeping a structured living environment with increased organization and consistency
• Setting up multi-step procedures so that one step leads directly to & cues the next step
• Behavioral recommendations to increase structure and implement problem solving strategies– Better executive functioning predicts better functional
outcomes
Aging with a TBI• Few studies have explored it
– Corkin et al, 1989: exacerbation of cognitive decline in WW II veterans with penetrating TBI
• First assessment was 10 years after injury• Second assessment 30 years later• Veterans with TBI showed greater decline than those with
peripheral nerve injuries
– Other studies have not shown this decline• Newcombe, 1996• Wood & Rutterford, 2006
– Drawbacks of such longitudinal design
Alzheimer’s and TBI• TBI is a risk factor for Alzheimer’s disease (AD)
• Case control studies generally support this association– Canadian Study of Health and Aging (1994)
• Brain injury is a borderline significant risk factor for AD
• Plassman (2000) WWII non-penetrating TBI vs unrelated condition– 50 years later – Moderate and severe TBI associated with
increased risk of dementia.– Nemetz et al (1999) showed no such association
• Meta-analysis of case-control studies showed significant association between TBI and AD in men but not women– Fleminger et al 2003, Mortimer et al, 1991
Vocational Outcome After TBI
• Pre-injury job stability (6 months prior to injury) is best predictor of return to work– Speed of information processing factors– Personality issues and premorbid
phsychological status– Post-injury attributional style
• Dikmen et al, 1995
Emotional and Behavioral Issues Associated with TBI
• Brain injury greatly increases risk of developing neuropsychiatric symptoms
• Profile of injury predicts neuropsychiatric symptoms
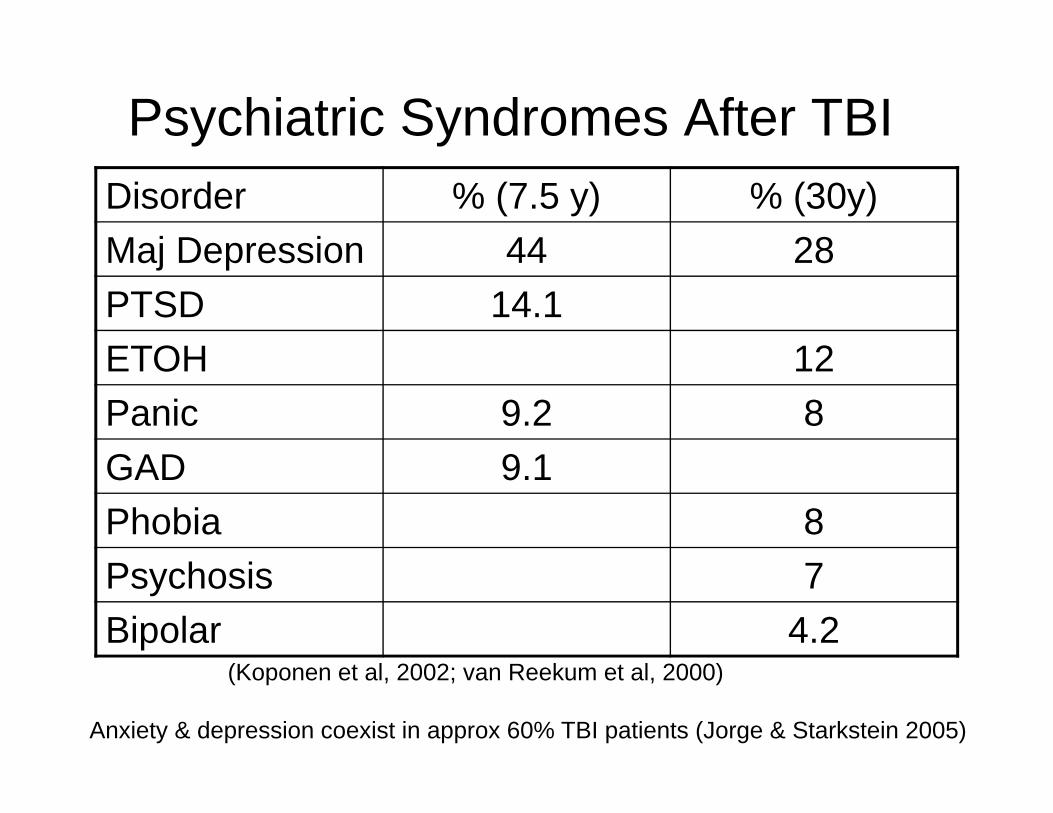
Psychiatric Syndromes After TBIDisorder % (7.5 y) % (30y)Maj Depression 44 28PTSD 14.1ETOH 12Panic 9.2 8GAD 9.1Phobia 8Psychosis 7Bipolar 4.2
(Koponen et al, 2002; van Reekum et al, 2000)
Anxiety & depression coexist in approx 60% TBI patients (Jorge & Starkstein 2005)
Depression After TBI
• MDD present in 40% of hospitalized TBI patients– 33% of 91 patients depressed during first year after TBI
• Premorbid depression is risk factor• Associated with lower executive functioning
– Jorge & Starkstein (2005)
• Increased likelihood with left dorsolateral frontal lesions and/or left basal ganglia lesions– Federoff et al (1992)
• Moderate to severe depression ranged from 31% at 1 month post-TBI to 17% at 3-5 years post-TBI– Dikmen et al (2004)
Anxiety After TBI• GAD in general population 5.1%
• GAD after TBI is unknown– Lower prevalence (2.5%; Deb et al 1999)– Higher prevalence (10.2% Hiott & Labbate 2002)– Associated with patient awareness of disability
• Concerns about future and ability to support self– Bimodal
• Mild TBI – frightened by mild changes and produce anxiety• Severe TBI – no anxiety
– Pathological absence of anxiety may be associated with frontal lobe functions
• Luria 1948/1963
Psychosis After TBI
• Uncommon but has been observed– Fujii et al 2004
• Schizophrenic like disorders are 2-3 times more common in patients with history of TBI
• Frontal lobe damage?• Impaired self-awareness?
– Arciniegas et al 2003, Silver et al 2001
• Risk factors– Left hemisphere injury– More severe injuries– Prior CNS injury
• Premorbid characteristics plus added brain trauma
Typical Approach to Psychosis After TBI
• Atypical antipsychotic trial– Risperidone (0.5 mg/d – 4.0 mg/d)
• Second atypical antipsychotic trial– Olanzapine, Quetiapine, Ziprazidone
• Typical antipsychotic trial– Haloperidol (0.5mg/d – 10 mg/d)
• Consider Clozapine, ECT, other
Emotional Problems After TBI• Lack of empathy
– 60.7% compared to 31% controls• Woods and Williams 2008
• Irritability– Common
• 37% of TBI patients age 18-65 reported it (Deb & Burns 2007) – Linked to disinhibition / frontal lobe deficits
• Socially Inappropriate Language– Not just disinhibition– Bilateral frontal lobe dysfunction with impairment in self-
awareness (Prigatano, 1999)
Agitation and Irritability• Most common complaints identified by patients
and spouses– Independent of severity of initial injury– Related to:
• Tiring more easily• Trouble following conversations
• Hypoarousal and agitation may manifest as anger, combativeness– Uninhibited movements, restlessness may
manifest as anxiety• Later, fatigue & sleep disruption may manifest as
depression
Emotional / Behavioral Changes and Recovery after TBI
• Moderate TBI patients report greater difficulty than those with mild or severe injuries– Mild due to lack of significant injury– Severe due to lack of awareness
• Over one year, improvement in cognitive clarity, dysphoric mood, and emotional stability but more difficulty with anger management, antisocial behaviors and self-monitoring
Important Psychosocial Aspects• Preserved problem-solving• Perceived social support
– Predicts 10% of variance in life satisfaction score– Less caregiver distress with increased perceived social support
• Positive affectivity• Strength of character
– Bravery– Humor– Spirituality– Kindness
Psychological Treatment After TBI
• Sources of Rater Bias– Relatives
• Overestimate problems due to stress• Underestimate problems due to denial• Tendency to over-pathologize• Overestimate pre-morbid functioning
– Patients• Overestimate what they can and cannot do
Treatment of Mood Disorders
• Presence of mood disorder affects long-term social and functional recovery
• No controlled psychopharmacological agent studies of mood and anxiety in TBI
• SSRIs appear to work best with least side effects
CBT in Mild TBI• Miller and Mittenberg, 1998
– Symptom attribution is primary element in maintenance of PCS symptoms
– Brief psychological treatment appears to significantly reduce the severity and duration of symptoms following mild head trauma
• Ferguson and Mittenberg (1995) developed 12 week outpatient treatment protocol
– Educate about typical recovery from mild TBI and help patient understand that symptoms maintained and intensified by anxiety, negative cognitions, misattributions
– teach coping skills, cognitive restructuring, stress management techniques
– Resume pre-injury activity level by activity scheduling
Social Support After TBI
• Social support has been shown to be best predictor of family functioning
• Social support powerful moderator of caregiver psychological distress
• Mentor programs are widely recognized as effective interventions– Enhance academic and vocational success
• Clifford & Green, 1996– Interventions best when mentor is peer who
shares similar characteristics with patient
Positive Psychology and TBI(Christopher Peterson & Martin Seligman)
• To explore character strengths that contribute to recovery from TBI
• Reinforce character strengths– Bravery– Humor– Spirituality– Kindness
Family Adjustment After TBI
• Brain injury is one of the most difficult situations to which a family must adjust (Stebbins, 1997)– Contributing:
• Survivor’s neurobehavioral disturbance– Neurobehavioral disturbance of the person with the injury is strongest
predictor of caregiver distress (Ergh et al 2002)
• Burden of care– Brooks, 1991
• Disruption of family patterns of relating– Curtiss et al, 2000
• Extra-patient factors– Financial impact - Time economy– Family planning - Environmental modifications– Community access - Obtaining treatment– Family members’ emotional status
Family Systems• Increased incidence of anxiety, depression, and
adjustment difficulty in family members of patients with TBI– Pattern of functioning greatly disrupted
• Marsh et al 1998
• Survivors with unhealthy family functioning demonstrate less improvement on disability rating scale at 5 months post-TBI especially on level of function & employability scores– Sander, 2002
Pre-injury Factors
• Caregiver functioning post-TBI associated with pre-injury factors– Livingston (2001)
• caregiver’s pre-injury health and psychiatric status is best predictor of caregiver functioning at 1 year post injury
– Gillen et al (1998)• 41% caregivers had depression prior to the injury• Majority of caregivers depressed at 1.5 years post-
injury were those who had pre-injury depression
Burden of care• Psychosocial stress more important than
physical demands– Survivor’s neurobehavioral disturbance
• (Kreutzer, Gervasio, & Camplair, 1994)– Survivor social isolation
• (Marsh, Kersel, Havill, and Sleigh, 2002)– Caregiver’s loss of social connections
• (Brooks 1991; Kreutzer, Serio, & Bergquist, 1994)– Changes of relating within family
• (Brooks, 1991; Curtiss, Klentz, & Vanderploeg, 2000)– Physical dependence
• (Machamer, Temkin, & Dikmen, 2002)
• Caregiver status is a good predictor of patient outcome
Model of Family Functioning after TBI
• Developmental Model– Turnbull & Turnbull, 1991– Response of family depends on:
• Family characteristics• Interactions• Functions family needs• Where TBI happened in terms of family life cycle
Family Interventions• Multi-Family group Support
– Peer-facilitated groups– Group psychotherapy– Peer mentoring
– Tasks in Family Support• Expose families to role models of adaptive coping• provide long-term, reliable support• Educate regarding available resources• Provide extensive support and assistance during crisis
Family Interventions
• Transition Planning – Turnbull & Turnbull, 1991
• Clients attend psychotherapy when they are experiencing a life transition
• Systemic Therapy– Intervene to change structure of family, not
just treat “patient”• Joining, reframing, enactment• Reinforcement of appropriate behavior
Summary:Working with Adults with a TBI
• Understand the type and severity of injury to know what should be expected in terms of patient functioning
• Assess premorbid characteristics and rule-out other sources of patient dysfunction
• Cognitively– Prepare for deficits in attention, memory, processing speed, and
executive functioning– Set up behavioral plans to compensate for cognitive deficits
• Psychologically– Evaluate for mood disorders common after TBI– Assess family functioning and patient support– Treat mood disorders
References• Arciniegas DB. The cholilnergic hypothesis of cognitive impairment caused by traumatic brain injury. Current Psychiatry
Reports. 2003; 5: 391-399.• Barth JT, Alves WM, Ryan TV, et al. Mild head injury in sports: Neuropsychological sequela and recovery of function. In
Levin HS, Eisenberg HM, Benton AL, eds. Mild Head Injury. New York: Oxford, 1989: 257-275.• Brooks N, Symington C, Beattie A, Campsie L, Bryden J & McKinlay W. Alcohol and other predictors of cognitive
recovery after severe head injury. Brain Injury. 1989; 3: 235-246.• Brooks N. The head-injured family. Journal of Clinical and Experimental Psychology. 1991; 13: 155-158. • Clifford EF. & Green VP. The mentor-protégé relationship as a factor in preservice teacher education: A review of the
literature. Early Child Development and Care. 1996; 125: 73-83.• Corkin S, Rosen TJ, Sullivan EV, Clegg RA. Penetrating head injury in young adulthood exacerbates cognitive decline in
later years. J Neuroscience. 1989; 9: 3876–83.• Curtiss G, Klentz S, & Vanderploeg RD, Acute impact of severe traumatic brain injury on family structure and coping
responses. Journal of Head Trauma Rehabilitation. 2000; 15: 1113-1122.• Deb S, Lyons I, Koutzoukis C, Ali I, & McCarthy G. Rate of psychiatric illness 1 year after traumatic brain injury.
American Journal of Psychiatry. 1999; 156: 374-378.• Deb S & Burns J. Neuropsychiatric consequences of traumatic brain injury: A comparison between two age
groups. Brain Injury. 2007; 21:301–7.• Desphande SA, Millis SR, Reeder KP, Fuerst D & Ricker JH. Verbal learning subtypes in traumatic brain injury: A
replication. Journal of Clinical and Experimental Neuropsychology. 1996; 18: 836-842.• Dikmen S, McLean A, & Temkin N. Neuropsychological outcome at one-month postinjury. Archives of Physical Medicine
and Rehabilitation. 1986; 67: 507-513.• Dikmen S, Machamer J, Temkin N. Mild Traumatic Brain Injury: Facts and artifacts. Journal of Clinical and Experimental
Neuropsychology. 2001; 11: 69-88.• Dikmen S & Levin H. Methodological issues in the study of mild head injury. Journal of Head Trauma Rehabilitation.
1993; 8: 30-37. • Dikmen S, Machamer J, Winn R, & Temkin N. Neuropsychological outcome at 1-year post head injury.
Neuropsychology. 1995; 9: 80-90. • Dikmen S, Bombardier CH, Machamer JE, Fann JR, Temkin NR. Natural history of depression in traumatic brain injury.
Archives of Physical Medicine and Rehabiltiation. 2004; 85: 1457-1464.• Ergh T, Rapport L, Coleman R, Hanks R. Predictors of caregiver and family functioning following traumatic brain injury:
Social support moderates caregiver distress. Journal of Head Trauma Rehabilitation. 2002; 17: 155-174.• Ergh T, Hanks R, Rapport L, Coleman R. Social support moderates caregiver life satisfaction following traumatic brain
injury. Journal of Clinical and Experiemental Psychology. 2003; 25: 1090-1101.
• Fedoroff JP, Starkstein SE, Forrester AW, Geisler FH, Jorge RE, Arndt SV & Robinson RG. Depression in patients with acute traumatic brain injury. The American Journal of Psychiatry. 1992; 149: 918-923.
• Ferguson RJ & Mittenberg W. 1995. Cognitive-behavioral treatment of postconcussion syndrome: A therapists manual. In V.B. Van Hasselt & M. Hersen (Eds.), Sourcebook of Psychological Treatment Manuals for Adult Disorders (pp 615-656). New York: Plenum.
• Fleminger S, Oliver D, Williams W, Evans J. The neuropsychiatry of depression after brain injury. Neuropsychological Rehabilitation. 2003; 13: 65-87.
• Fujii D, Ahmed I, Hishinuma E. A neuropsychological comparison of psychotic disorder following traumatic brain injury, traumatic brain injury without psychotic disorder, and schizophrenia. Journal of Neuropsychiatry and Clinical Neuroscience. 2004; 16: 306-314.
• Fuster, J.M. (1995). Memory in the Cerebral Cortex—An Empirical Approach to Neural Networks in the Human and Nonhuman Primate (Cambridge, MA: MIT Press).
• Gillen R, Tennen H, Affleck G & Steinpreis R. Distress, depressive symptoms, and depressive disorder among caregivers of patients with brain injury. Journal of Head Trauma Rehabilitation. 1998; 13: 31-43.
• Goldstein F, Levin H, Golgman W, Clark A & Altonen T. Cognitive and neurobehavioral functioning after mild versus moderate traumatic brain injury in older adults. Journal of the International Neuropsychological Society. 2001; 7: 373-383.
• Grant I & Adams KM. Neuropsychological Assessment of Neuropsychiatric and Neuromedical Disorders. 3rd ed. New York: Oxford University Press: 2009.
• Gronwall D. Rehabilitation programs for patients with mild traumatic brain injury: Components, problems, and evaluation. Journal of Head Trauma Rehabilitation. 1986; 1: 53-62.
• Hanks R, Temkin N, Machamer J & Dikmen S. Emotional and behavioral adjustment after traumatic brain injury. Archives of Physical Medicine & Rehabilita991-997.
• Hanks R, Millis S, Ricker J, Giacino J, Nakese-Richardson R et al. The predictive validity of a brief inpatient neuropsychological battery for persons with traumatic brain injury. Archives of Physical Medicine and Rehabilitation. 2008; 89: 950-957.
• Hiott DW & Labbate L. Anxiety disorders associated with traumatic brain injuries. NeuroRehabilitation. 2002; 17: 345-355.• Jorge R & Starkstein S. Pathophysiologic aspects of major depression following traumatic brain injury. Journal of Head
Trauma Rehabilitation. 2005; 20: 475-487.• Kashluba S, Hanks RA, Casey JE, & Millis S. Neuropsychological and functional outcome after mild complicated
traumatic brain injury. Archives of Physical Medicine and Rehabilitationtion. 1999; 80:. 2008; 89: 904-911.• Koponen S, Taiminen T, Portin R, Himanen L, Isoniemi H, Heinonen H, Hinka S & Tenovuo O. Axis I and II psychiatric
disorders after traumatic brain injury: A 30 year follow-up study. American Journal of Psychiatry. 2002; 159: 1315-1321.• Kreutzer JS, Gordon WA, Rosenthal M & Marwitz J. Neuropsychological characteristics of patients with brain injury:
Preliminary findings from a multicenter investigation. Journal of Head Trauma Rehabilitation. 1993; 18: 128-138.• Kreutzer JS, Gervasio AH & Camplair PS. Primary caregivers' psychological status and family functioning after traumatic
brain injury. Brain Injury. 1994; 8: 197-210.• Kreutzer JS, Serio CD & Bergquist S. Family needs after brain injury: A quantitative analysis. Journal of Head Trauma
Rehabilitation. 1994; 9: 104-115.
• Levin HS, Mattis S, Ruff RM, Eisenberg HM, Marshall LF, Tabaddor K, High WM & Frankowski RF. Neurobehavioral outcome following mild head injury: A three-center study. Journal of Neurosurgery. 1987; 66: 234-243.
• Levin HS, High WM, Golstein FC et al. Sustained attention and information processing speed in chronic survivors of severe closed head injury. Scandinavian Journal of Rehabilitation Medicine. 1988; 17: 33-40.
• Levin H, Gary H, Eisenberg H, Ruff R, Barth J, Kreutzer J, High W, Portman S, Foulkes M, Jane J, Marmarou A & Marshall L. Neurobehavioral outcome 1 year after severe head injury. Journal of Neurosurgery. 1990; 73, 699-709.
• Livingston MG. Head injury: The relatives’ response. Brain Injury. 2001;1:33-9.• Luria AR. Restoration of function after brain trauma (in Russian). Moscow: Academy of Medical Science; London:
Pergamon.• Macciocchi SN, Barth JT, Alves W et al. Neuropsychological functioning and recovery after mild traumatic brain injury in
collegiate athletes. Neurosurgery. 1996; 39: 510-514 • Machamer J, Temkin N & Dikmen S. Significant other burden and factors related to it in traumatic brain injury. Journal of
Clinical and Experimental Neuropsychology. 2002; 24: 420-433.• Marsh NV, Kersel DA, Havill JH, Sleigh JW. Caregiver burden at 6 months following severe traumatic brain injury. Brain
Injury. 1998; 12: 225-238.• Marsh NV, Kersel DA, Havill JA & Sleigh JW. Caregiver burden during the year following severe traumatic brain injury.
Journal of Clinical and Experimental Neuropsychology. 2002; 24: 434-447. • McCrea M, Gusikiewicz KM, Marsahll SW et al. Acute effects and recovery time following concussion in collegiate football
players: The NCAA concussion study. Journal of the American Medical Association. 2003; 290: 2556-2563.• Miller LJ & Mittenberg W. Brief cognitive-behavioral interventions in mild traumatic brain injury. Applied Neuropsychology.
1998; 4: 172-183.• Millis SR, Rosenthal M, Novack TA, Sherer M, Nick TG, Kreutzer JS, High WM & Ricker JH. Long-term
neuropsychological outcome after traumatic brain injury. Journal of Head Trauma Rehabilitation. 2001; 16: 343-355. • Minderhoud JM, Boelens ME, Huizenga J & Saan RJ. Treatment of minor head injuries. Clinical Neurology &
Neurosurgery. 1980; 82: 127-140. • Mortimer JA, van Duijn CM, Chandra V, Fratiglioni L, Graves AB, Heyman A, et al. Head trauma as a risk factor for
Alzheimer’s disease: A collaborative reanalysis of case-control studies. EURODEM Risk Factors Research Group. International Journal of Epidemiology.1991; 20: S28–35.
• Nemetz PN, Leibson C, Naessens JM, Beard M, Kikmen E, Annegars JF et al. Traumatic brain injury and time to onset of Alzheimer’s disease: A population based study. American Journal of Epidemiology. 1999; 149: 32-40.
• Newcombe F. Very late outcome after focal wartime brain wounds. Journal of Clinical & Experimental Neuropsychology. 1996; 18: 1–23.
• Plassman BL, Havlik RJ, Steffens DC, Helms MJ, Newman TN, Drosdick D, et al. Documented head injury in early adulthood and risk for Alzheimer’s disease and other dementias. Neurology. 2000; 55: 1158-1166.
• Prigatano GP & Altman IR. Impaired awareness of behavioral limitations after traumatic brain injury. Archives of Physical Medicine & Rehabilitation. 1991; 71: 1058-1064.
• Salmond CH, Chatfield DA, Menon DK, Pickard JD & Sahakian BJ. Cognitive sequelae of head injury: Involvement of basal forebrain and associated structures. Brain. 2005; 128: 189-200.
• Sander AM, Atchison T, High W et al. Relationship between family functioning and outcome following TBI. Journal of the International Neuropsychological Society. 2002; 8:169.
• Satz P. Brain reserve capacity on symptom onset after brain injury: A formulation and review of evidence for threshold theory. Neuropsychology. 1993; 7: 273–95.
• Sherer M, Bergloff P, Levin E, High WM, Oden KE & Nick TG. Impaired awareness and employment outcome after traumatic brain injury. Journal of Head Trauma Rehabilitation. 1998; 13: 52-61.
• Silver JM, Kramer R, Greenwald S & Weissman M. The association between head injuries and psychiatric disorders: Findings from the New Haven NIMH Epidemiologic Catchment Area Study. Brain Injury. 2001; 15: 935-945.
• Stebbins, P. Long term changes in family needs after brain injury: A preliminary review. Australian Journal of Rehabilitation Counseling 1997; 3: 30-39.
• Stern Y, editor. Cognitive reserve – theory and applications. Psychology Press; 2006.• The Canadian Study on Health and Aging: Risk Facots for Alzheimer’s Disease in Canada. Neurology. 1994; 44: 2073-
2080.• Thurman DJ, Alverson C, Dunn KA, Guerroro J & Sniezek JE. Traumatic Brain Injury in the United States: A Public
health perspective. Journal of Head Trauma Rehabilitation. 1999; 14: 602-615.• Turnbull, A.P., & Turnbull, H.R. Understanding families from a systems perspective. In J.M. Williams & T. Kay (Eds.),
Head injury: A family matter (pp. 37–63). Baltimore, MD. 1991: Paul H. Brookes.• Van Reekum R, Cohen T, Wong J. Can traumatic brain injury cause psychiatric disorders? Journal of Neuropsychiatry.
2000; 12: 316-327.• Wood RL & Rutterford NA. Long-term effect of head trauma on intellectual abilities: A 16 year outcome study. Journal of
Neurology, Neurosurgery, and Psychiatry. 2006; 77: 1180-1184.• Wood RLL & Williams C. Inability to empathize following traumatic brain injury. Journal of the International
Neuropsychological Society. 2008; 14: 289-296.