Embed Size (px)
Citation preview

Collaboration between hospital physicians andnurses: An integrated literature review
C.J. Tang1 Candidate Bachelor of Science (Nursing) (Honour) program,S.W. Chan2 PhD in Nursing, W.T. Zhou3 Advanced Practice Nurse, Master inNursing & S.Y. Liaw4 Registered Nurse, PhD in Medical Education
1 Student, 2 Professor, 3 Lecturer, 4 Assistant Professor, Alice Lee Centre for Nursing Studies, National University ofSingapore, National University Health System, Singapore, Singapore
TANG C.J., CHAN S.W., ZHOU W.T. & LIAW S.Y. (2013) Collaboration between hospital physicians andnurses: An integrated literature review. International Nursing Review 60, 291–302
Background: Ineffective physician–nurse collaboration has been shown to cause work dissatisfaction among
physicians and nurses and compromised the quality of patient care.
Aim: The review sought to explore: (1) attitudes of physicians and nurses toward physician–nurse
collaboration; (2) factors affecting physician–nurse collaboration; and (3) strategies to improve
physician–nurse collaboration.
Methods: A literature search was conducted in the following databases: CINAHL, PubMed, Wiley Online
Library and Scopus from year 2002 to 2012, to include papers that reported studies on physician–nurse
collaboration in the hospital setting.
Findings: Seventeen papers were included in this review. Three of the reviewed articles were qualitative studies
and the other 14 were quantitative studies. Three key themes emerged from this review: (1) attitudes towards
physician–nurse collaboration, where physicians viewed physician–nurse collaboration as less important than
nurses but rated the quality of collaboration higher than nurses; (2) factors affecting physician–nurse
collaboration, including communication, respect and trust, unequal power, understanding professional roles,
and task prioritizing; and (3) improvement strategies for physician–nurse collaboration, involving
inter-professional education and interdisciplinary ward rounds.
Conclusion: This review has highlighted important aspects of physician–nurse collaboration that could be
addressed by future research studies. These include: developing a comprehensive instrument to assess
collaboration in greater depth; conducting rigorous intervention studies to evaluate the effectiveness of
improvement strategies for physician–nurse collaboration; and examining the role of senior physicians
and nurses in facilitating collaboration among junior physicians and nurses. Other implications include
inter-professional education to empower nurses in making clinical decisions and putting in place policies to
resolve workplace issues.
Correspondence address: Dr Sok Ying Liaw, Alice Lee Centre for Nursing Studies, National University of Singapore, National University Health System, Level 2, ClinicalResearch Centre, Block MD 11, 10 Medical Drive, Singapore 117597, Singapore; Tel: (65)-65167451; Fax: (65)-67767135; E-mail [email protected].
Conflict of interest: No conflict of interest has been declared by the authors.
bs_bs_banner
Literature Review
© 2013 International Council of Nurses 291

Keywords: Attitudes, Inter-Professional Collaboration, Inter-Professional Education, Nurse–Physician Relations,
Physician–Nurse Collaboration
BackgroundPhysician–nurse collaboration is defined by Petri (2010) as aninterpersonal process where physicians and nurses present withshared objectives. Both parties should possess equal decision-making capacity, responsibility and power to manage patientcare (Petri 2010). There should also be mutual trust and respect,and open and effective communication in this relationship.Each profession needs to be aware and accept the roles, skillsand responsibilities of the other (Petri 2010). Historically, inter-actions between physicians and nurses were hierarchical(Thomas et al. 2003). Stein first wrote about the ‘Doctor-NurseGame’ in 1967, a key study demonstrating that traditional rela-tionships between both physicians and nurses were largely char-acterized by medical dominance and nursing subservience(Vazirani et al. 2005). Such relationships set physicians firmly incharge and superior to nurses. Nurses were then expected tocarry out orders and avoid open communication with physi-cians whenever possible (Vazirani et al. 2005). Many nurseshave described such practice as a stifling experience, whichdevalued nurses’ professional worth and increased their job dis-satisfaction (Sirota 2007).
Hostile and adversarial relationships between both profes-sions still largely exist in many Western countries such as theUSA, Italy, Germany, and Asian countries like China and Japan(Morinaga et al. 2008; Papathanassolgou et al. 2012; Rosenstein2002). Studies found that physicians tend to have rude andintimidating personalities (Robinson et al. 2010; Rosenstein2002; Rosenstein & O’Daniel 2005). They exhibited disruptivebehaviours such as yelling and using abusive language towardsnurses. Consequently, nurses experienced a lack of respect andautonomy (Robinson et al. 2010; Rosenstein 2002; Rosenstein &O’Daniel 2005). The ‘friendly stranger’ relationship was alsoevident in some studies where interactions between physiciansand nurses were solely characterized by formal exchanges ofinformation (Kramer & Schmalenberg 2003; Schmalenberg &Kramer 2009). Each party was fairly satisfied with only fulfillingtheir own tasks and responsibilities towards each other andpatients (Kramer & Schmalenberg 2003; Schmalenberg &Kramer 2009). Nonetheless, there is evidence suggesting thatphysician–nurse relationships are in fact improving and movingslowly towards a collegial or collaborative nature (Kramer &Schmalenberg 2003; Schmalenberg & Kramer 2009). Collegialrelationships are characterized by equal trust, respect and
autonomy over patient care. Both professions engage in opencommunication and value each other’s input about patient out-comes (Robinson et al. 2010; Schmalenberg & Kramer 2009).Collaborative relationships are based on mutual respect andtrust, though at times nurses are expected to cooperate withphysicians (Robinson et al. 2010; Schmalenberg & Kramer2009). Effective physician–nurse collaboration has been foundto greatly improve the quality of patient care and their healthoutcomes (Hughes & Fitzpatrick 2010; Messmer 2008; Rose2011). As described, the patterns of physician–nurse collabora-tion are diverse and this could be attributed to the different atti-tudes, values and interpersonal skills held by each individual(Rosenstein 2002; Vazirani et al. 2005). Furthermore, behav-iours of physicians and nurses are largely influenced by theirpre-licensure education and ward cultures, which differ acrossclinical settings and countries (Hughes & Fitzpatrick 2010;Robinson et al. 2010).
Ineffective physician–nurse relationships have led to workdissatisfaction, a lack of autonomy and poor health amongnurses (Lim et al. 2010; Sirota 2007). Such working relation-ships have also caused many nurses to leave the profession,making retention and recruitment of nurses increasingly diffi-cult (Nelson et al. 2008; Rosenstein 2002; Thomson 2007). Phy-sicians were also reported to be easily frustrated when orderswere not carried out timely and communication delivered wasunclear. This contributed largely to work dissatisfaction amongphysicians (Rosenstein 2002; Rosenstein & O’Daniel 2005).Most importantly, ineffective collaboration had a significantimpact on patient outcomes by compromising their quality ofcare and safety, which often led to increased mortality rates(Rosenstein 2002; Rosenstein & O’Daniel 2005). Moreover, poorphysician–nurse collaboration was known to affect the satisfac-tion levels of both patients and family members during theirhospital stay (McCaffrey et al. 2010; Robinson et al. 2010).
AimRecognizing that collaboration is a two-way interpersonalprocess, it is important to understand the attitudes of both phy-sicians and nurses towards collaborative practice. This will aidin identifying the areas of improvement for physician–nursecollaboration (Petri 2010; Seitz et al. 2007). This integratedliterature review therefore aimed to present the best available
292 C. J. Tang et al.
© 2013 International Council of Nurses

evidence on physician–nurse collaboration. The specific ques-tions to be addressed in this review include:1 What are the attitudes of physicians and nurses towardsphysician–nurse collaboration?2 What are the factors affecting physician–nurse collaboration?3 What strategies could be recommended to improvephysician–nurse collaboration?
Methods
Search method and process
The search sought to identify published papers in Englishwhich reported primary research studies on physician–nurserelationship or collaboration in hospitals. Relevant studieswere searched via the following databases: CINAHL, PubMed,Wiley Online Library and Scopus. Key search terms includedsingly or in various combinations: ‘nurse-physician relations’,‘attitudes’, ‘inter professional collaboration’, ‘collaboration’,‘doctor’, ‘nurse’ and ‘hospital’. A manual search was carried outon Journal of Interprofessional Care and using the ancestryapproach, reference lists of each retrieved article were reviewedfor additional relevant journals. The search was limited tojournals published in the last 10 years, from January 2002 toDecember 2012.
Initial review identified 23 potential articles. Each journalarticle was then read in full to assess its relevance. Exclusion cri-teria were also taken into consideration while extracting rel-evant journals. Studies conducted in outpatient clinics, nursinghomes and operating theatres were excluded. Studies thatlargely discuss inter-professional education (IPE), work con-flicts and attitudes of healthcare students towards collaborativepractice were also excluded. Studies that explored working rela-tionships between doctors or nurses and other allied health pro-fessionals were not considered.
Search outcomes
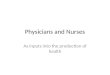
The search process, and total number of included and excludedarticles are illustrated in Fig. 1. A total of six articles wereexcluded for the following reasons: (1) focus of the studywas not largely based on physician–nurse collaboration;(2) explored relationships between physicians and advancednurse practitioners; and (3) inappropriate target group wheremedical students, nurses and nurse managers were recruited asparticipants. Finally, 17 articles were reviewed.
Of the 17 reviewed studies, three were qualitative studies thatused focus-group interviews or semi-structured interviews. Theother 14 articles were quantitative studies. Ten of them adopteddescriptive comparative designs, where questionnaires wereused to evaluate the different attitudes physicians and nurses
have towards collaboration. Four used experimental designsto evaluate the effectiveness of interventions in improvingphysician–nurse collaboration. Table 1 summarizes the method-ologies and findings of the reviewed studies. These findingswere pooled together and categorized into three key themes fordiscussion.
Results
Attitudes towards physician–nurse collaboration
The reviewed studies adopted different instruments to measureattitudes of physicians and nurses towards collaboration. The‘Jefferson Scale of Attitudes toward Physician-Nurse Collabora-tion (JSAPNC)’ has been used in four of the reviewed studies(Garber et al. 2009; Hojat et al. 2003; Hughes & Fitzpatrick2010; Thomson 2007). Other questionnaires used include‘Baggs Collaboration and Satisfaction about Care Decisions(CSACD)’, ‘Collaboration & Satisfaction with Patient Care Deci-sions (CSPCD)’, ‘Collaborative Practice Scale (CPS)’, ‘IntensiveCare Unit Management Attitudes Questionnaire (ICUMAQ)’,‘Nurse-Physician Collaboration Scale’ and ‘Nurse-PhysicianRelationship Survey’ (Messmer 2008; Nair et al. 2012;Nathanson et al. 2011; Nelson et al. 2008; Rosenstein 2002;Rosenstein & O’Daniel 2005; Thomas et al. 2003). The validitiesand reliabilities of all these abovementioned instruments werewell documented (Dougherty & Larson 2005; Thomas et al.2003).
The attitudes towards physician–nurse collaboration are cat-egorized into two subthemes – importance of physician–nursecollaboration and the quality of physician–nurse collaboration.
Importance of physician–nurse collaboration
Several reviewed studies found that physicians and nursesvalued collaboration (Hughes & Fitzpatrick 2010; Robinsonet al. 2010; Rosenstein 2002). Both professions recognized thateffective collaboration is essential in bringing about betterquality patient care, which ultimately leads to improved healthoutcomes for patients (Hughes & Fitzpatrick 2010; Robinsonet al. 2010; Rosenstein 2002). Two studies supported that physi-cians and nurses recognized the importance of collaboration inensuring patient safety, satisfaction, faster recovery and lowermortality rates (Messmer 2008; Rosenstein & O’Daniel 2005).
However, more of the reviewed studies reported that physi-cians viewed collaboration as less important when comparedwith nurses (Garber et al. 2009; Hughes & Fitzpatrick 2010;Rosenstein 2002; Thomson 2007). On the contrary, nurses whowere more likely to perceive collaboration as an importantfactor to providing better care demonstrate more interests andhave greater desires than physicians to work collaboratively
Physician–nurse collaboration 293
© 2013 International Council of Nurses

(Garber et al. 2009; Hughes & Fitzpatrick 2010; Rosenstein2002; Thomson 2007). The aforementioned studies that useddescriptive comparative designs were conducted in variousparts of USA and all revealed statistically significant differencesbetween physicians and nurses in their attitudes towards col-laboration (Garber et al. 2009; Hughes & Fitzpatrick 2010;Rosenstein 2002; Thomson 2007). Hojat et al. (2003) conducteda cross-cultural study to compare attitudes towards collabora-tion between 2522 physicians and nurses from USA, Mexico,Israel and Italy. The study reported that despite differences inculture, nurses demonstrated a significantly more positive atti-tude than physicians towards the importance of collaboration(Hojat et al. 2003).
These different perceptions on the importance of physician–nurse collaboration could be explained by the fact that
physicians and nurses have different training and they adoptdifferent care philosophies (Hughes & Fitzpatrick 2010; Sirota2007). While physicians were traditionally trained to developtechnical skills and focus on finding cure for diseases, nurseswere trained in developing interpersonal skills with patients andcolleagues, providing holistic care for patients and making deci-sions interdependently with physicians (Hughes & Fitzpatrick2010; Sirota 2007). As a result of the training that focused ondisease management, physicians were generally satisfied to prac-tice independently without much assistance from nurses(Hughes & Fitzpatrick 2010). In contrast, to achieve moreholistic care for patients including social and psychological well-being, nurses felt that their valuable perspectives should be con-sidered during times of decision-making (Dougherty & Larson2005). Nurses, therefore, see physician–nurse collaboration as
Key search terms: • Nurse–physician relations • Attitudes • Inter-professional collaboration • Collaboration • Doctor • Nurse • Hospital
Search strategies:
1. Searching for references through the use of the following databases: CINAHL, PubMed, Wiley Online Library and Scopus.
2. Manual search on Journal of Interprofessional Care.
3. Using the ancestry approach: the reference lists of each retrieved article were reviewed for additional relevant journals.
Inclusion criteria applied: • Primary research papers • Published in English • Published in the last 10 years, from January 2002
to December 2012 • Discuss about relationships or collaboration
between doctors and nurses in hospitals
23 potential journal articles were identified
and read in full to assess its relevance.
17 journal articles were included in the final
review
6 journal articles were
excluded
Reasons for exclusion: • Focus of study was not
largely based on physician–nurse collaboration (3)
• Explored relationships between physicians and advanced nurse practitioners (1)
• Inappropriate target group: medical students and nurses (1)
• Target group included nurse managers (1)
14 quantitative studies3 qualitative studies
Reasons for exclusion (67): • Commentaries, opinion papers
(12) • Literature reviews (10) • Conducted in outpatient
clinics, nursing homes and operating theatres (15)
• Largely discuss inter-professional education (10), work conflicts (7) and attitudes of healthcare students towards collaborative practice (8)
• Explored collaboration between doctors or nurses and other allied health professionals (5).
Fig. 1 Flow chart describing details of literature search.
294 C. J. Tang et al.
© 2013 International Council of Nurses

Tab
le1
Sum
mar
yof
revi
ewed
stu
die
son
phy
sici
an–n
urs
eco
llab
orat
ion
Aut
hors
Stud
yai
m(s
)St
udy
desi
gnSa
mpl
ech
arac
teri
stic
sK
eyfin
ding
s
McC
affr
eyet
al.(
2010
)To
deve
lop,
impl
emen
tan
d
eval
uat
ea
6-m
onth
edu
cati
onal
and
expe
rien
tial
prog
ram
desi
gned
for
the
new
med
ical
resi
den
tsan
dn
urs
esto
impr
ove
com
mu
nic
atio
nan
d
colla
bora
tion
.
Inte
rven
tion
stu
dyan
dre
gula
r
focu
sgr
oup
follo
wu
p
mee
tin
gsto
eval
uat
ech
ange
sin
com
mu
nic
atio
nan
d
colla
bora
tion
styl
es.
Con
duct
edat
ah
ospi
tali
n
Flor
ida
wit
h50
new
med
ical
resi
den
tsan
d65
nu
rses
•O
vera
llim
prov
emen
tsin
com
mu
nic
atio
n,c
olla
bora
tion
,pat
ien
t
outc
omes
and
job
sati
sfac
tion
•P
rom
oted
com
mon
goal
,ope
ndi
scu
ssio
n,a
nd
acce
ptan
ceof
idea
s
amon
gre
side
nts
and
nu
rses
.
•Im
prov
edin
ter-
prof
essi
onal
com
mu
nic
atio
nan
dco
llabo
rati
on
incr
ease
dpa
tien
ts’s
atis
fact
ion
.
Gar
ber
etal
.(20
09)
Toex
amin
eth
eat
titu
des
of
nu
rses
,phy
sici
ans
and
resi
den
tsto
war
dsco
llabo
rati
on
and
toas
sess
thei
r
self
-per
cept
ion
ofse
rvan
t
lead
ersh
ipch
arac
teri
stic
s.
Des
crip
tive
,com
para
tive
stu
dy
usi
ng
Th
eJe
ffer
son
Scal
eof
Att
itu
des
tow
ard
Phy
sici
an-N
urs
eC
olla
bora
tion
and
Bar
buto
–Wh
eele
rSe
rvan
t
Lead
ersh
ipQ
ues
tion
nai
re
419
nu
rses
,61
phys
icia
ns
and
17
resi
den
tsin
Sou
thea
ster
n
Un
ited
Stat
esh
ealt
hsy
stem
wer
esu
rvey
edvi
ath
eIn
tran
et
•A
ttit
ude
sof
nu
rses
tow
ards
colla
bora
tion
wer
esi
gnifi
can
tly
mor
e
posi
tive
than
that
ofph
ysic
ian
s.
•N
urs
esh
ada
sign
ifica
ntl
ym
ore
posi
tive
self
-per
cept
ion
of
them
selv
esas
serv
ant
lead
ers
than
phys
icia
ns
do.
Hoj
atet
al.(
2003
)To
com
pare
atti
tude
sof
phys
icia
ns
and
nu
rses
tow
ards
colla
bora
tion
inU
SA,I
srae
l,
Ital
yan
dM
exic
o.
Cro
ss-c
ult
ura
lstu
dyu
sin
gT
he
Jeff
erso
nSc
ale
ofA
ttit
ude
s
tow
ard
Phy
sici
an-N
urs
e
Col
labo
rati
on
850
phys
icia
ns
and
1672
nu
rses
from
USA
,Isr
ael,
Ital
yan
d
Mex
ico
•R
egar
dles
sof
the
cou
ntr
y,n
urs
essc
ored
sign
ifica
ntl
yh
igh
erth
an
phys
icia
ns
onth
eto
tala
ttit
ude
scal
e.
•T
he
hig
hes
tm
ean
scor
eson
‘sh
ared
edu
cati
onan
dte
amw
ork’
,
‘car
ing
vs.c
uri
ng’
and
‘nu
rses
’au
ton
omy’
wer
eob
tain
edby
Am
eric
anan
dIs
rael
inu
rses
,wh
ich
was
sign
ifica
ntl
ydi
ffer
ent
from
any
phys
icia
ngr
oup.
Th
omas
etal
.(20
03)
Tom
easu
rean
dco
mpa
recr
itic
al
care
phys
icia
ns
and
nu
rses
’
atti
tude
sab
out
team
wor
k.
Cro
ss-s
ecti
onal
stu
dyu
sin
gth
e
ICU
MA
Q
90ph
ysic
ian
san
d23
0n
urs
es
from
eigh
tin
ten
sive
care
un
its
insi
xh
ospi
tals
inH
oust
on,
Texa
s
•33
%of
the
nu
rses
rate
dth
equ
alit
yof
colla
bora
tion
and
com
mu
nic
atio
nw
ith
phys
icia
ns
ash
igh
orve
ryh
igh
.73%
of
phys
icia
ns
rate
dco
llabo
rati
onan
dco
mm
un
icat
ion
wit
hn
urs
esas
hig
hor
very
hig
h.
•N
urs
esre
port
edth
atit
isdi
fficu
ltto
spea
ku
p,di
sagr
eem
ents
are
not
appr
opri
atel
yre
solv
ed,m
ore
inpu
tin
tode
cisi
on-m
akin
gis
nee
ded,
and
nu
rse
inpu
tis
not
wel
lrec
eive
d.
Ros
enst
ein
&O
’Dan
iel(
2005
)To
asse
ssth
epe
rcep
tion
sof
the
impa
ctof
disr
upt
ive
beh
avio
ur
onn
urs
e–ph
ysic
ian
rela
tion
ship
san
dpa
tien
t
clin
ical
outc
omes
.
Des
crip
tive
stu
dyu
sin
g
ques
tion
nai
resu
rvey
desi
gned
asa
follo
w-u
pto
prev
iou
s
VH
AW
est
Coa
stsu
rvey
con
duct
edin
Ros
enst
ein
’s
(200
2)st
udy
1091
regi
ster
edn
urs
es,4
02
phys
icia
ns
and
16
exec
uti
ve-l
evel
adm
inis
trat
ors
from
50V
HA
hos
pita
lsac
ross
Wes
tC
oast
•N
urs
esbe
hav
eddi
sru
ptiv
ely
alm
ost
asfr
equ
entl
yas
phys
icia
ns.
•D
isru
ptiv
ebe
hav
iou
rn
egat
ivel
yaf
fect
edbo
thn
urs
esan
d
phys
icia
ns
inte
rms
ofst
ress
,fru
stra
tion
,con
cen
trat
ion
,
com
mu
nic
atio
n,c
olla
bora
tion
,in
form
atio
ntr
ansf
eran
d
rela
tion
ship
s.
•N
egat
ive
orw
orse
nin
gef
fect
sof
disr
upt
ive
beh
avio
ur
onad
vers
e
even
ts,m
edic
aler
rors
,pat
ien
tsa
fety
,mor
talit
y,qu
alit
yof
care
and
sati
sfac
tion
.
Vaz
iran
iet
al.(
2005
)To
dete
rmin
eth
eim
pact
ofa
mu
ltid
isci
plin
ary
inte
rven
tion
ona
com
mu
nic
atio
nan
d
colla
bora
tion
amon
gdo
ctor
s
and
nu
rses
onan
acu
te
inpa
tien
tm
edic
alu
nit
.
Inte
rven
tion
stu
dyin
volv
edth
e
addi
tion
ofa
nu
rse
prac
titi
oner
toea
chm
edic
alte
am,
appo
intm
ent
ofa
hos
pita
list
med
ical
dire
ctor
,an
d
inst
itu
tion
ofda
ily
mu
ltid
isci
plin
ary
rou
nds
Con
duct
edin
ah
ospi
tala
tLo
s
An
gele
s,w
her
eov
era
2-ye
ar
peri
od,i
nte
rven
tion
and
con
trol
un
its
wer
ecr
eate
d
invo
lvin
g11
1h
ouse
offi
cers
,45
atte
ndi
ng
phys
icia
ns
and
123
nu
rses
•P
hysi
cian
sin
the
inte
rven
tion
grou
pre
port
edsi
gnifi
can
tly
grea
ter
colla
bora
tion
and
bett
erco
mm
un
icat
ion
wit
hn
urs
esth
andi
d
phys
icia
ns
inth
eco
ntr
olgr
oup.
•In
con
tras
t,n
urs
esin
both
grou
psre
port
edsi
mila
rle
vels
of
com
mu
nic
atio
nan
dco
llabo
rati
onw
ith
phys
icia
ns.
Physician–nurse collaboration 295
© 2013 International Council of Nurses

Tabl
e1
Con
tin
ued
Aut
hors
Stud
yai
m(s
)St
udy
desi
gnSa
mpl
ech
arac
teri
stic
sK
eyfin
ding
s
Mes
smer
(200
8)To
dete
rmin
eth
ele
velo
f
nu
rse–
phys
icia
nco
llabo
rati
on
duri
ng
sim
ula
tion
trai
nin
g.
Inte
rven
tion
desc
ript
ive
stu
dy
usi
ng
the
KSN
PS,
Col
labo
rati
on&
Sati
sfac
tion
wit
hPa
tien
tC
are
Dec
isio
ns,
and
Clin
ical
Pra
ctic
eG
rou
p
Coh
esio
nto
eval
uat
eth
eir
team
perf
orm
ance
55pa
edia
tric
med
ical
resi
den
ts
and
50n
urs
esfr
oma
child
ren
’sh
ospi
tali
n
Sou
thea
ster
nU
nit
edSt
ates
form
ed18
code
team
san
d
un
derw
ent
thre
esi
mu
lati
on
sess
ion
sof
life-
thre
aten
ing
scen
ario
sin
child
ren
•H
igh
leve
lsof
grou
pco
hes
ion
,col
labo
rati
onan
dsa
tisf
acti
onw
ith
pati
ent
care
deci
sion
sw
ere
iden
tifi
edam
ong
both
phys
icia
ns
and
nu
rses
.
•T
he
thre
ein
depe
nde
nt
obse
rver
su
sin
gth
eK
SNP
Sre
port
edth
at
wit
hm
ore
sim
ula
tion
sess
ion
s,co
llabo
rati
vere
lati
onsh
ips
impr
oved
wit
hgr
eate
rco
mm
un
icat
ion
and
colle
gial
exch
ange
s.
Nat
han
son
etal
.(20
11)
Tom
easu
reth
ede
gree
of
sim
ilari
tyof
atti
tude
son
colla
bora
tion
betw
een
nu
rses
and
jun
ior
doct
ors
inth
eIC
U.
Des
crip
tive
stu
dyu
sin
ga
mod
ified
vers
ion
ofth
eB
aggs
Col
labo
rati
onan
dSa
tisf
acti
on
abou
tC
are
Dec
isio
ns
inst
rum
ent
31n
urs
esan
d46
jun
ior
doct
ors
from
am
edic
al/s
urg
ical
ICU
in
the
Nor
thea
ster
nU
nit
edSt
ates
•M
odes
tag
reem
ent
amon
gth
epa
rtic
ipan
tsth
atde
cisi
on-m
akin
g
resp
onsi
bilit
ies
are
not
shar
ed.N
urs
espe
rcei
veth
isas
inad
equ
ate
colla
bora
tion
.
•Ju
nio
rdo
ctor
sw
ere
sati
sfied
wit
hco
llabo
rati
on.
•Si
gnifi
can
tdi
ffer
ence
betw
een
jun
ior
doct
ors
and
nu
rses
’ove
rall
sati
sfac
tion
wit
hte
amde
cisi
ons.
Wel
ler
etal
.(20
11)
Tou
nde
rsta
nd
the
nat
ure
of
inte
ract
ion
s,ac
tivi
ties
and
issu
esaf
fect
ing
med
ical
and
nu
rsin
ggr
adu
ates
inor
der
to
info
rmin
terv
enti
ons
to
impr
ove
inte
r-pr
ofes
sion
al
colla
bora
tion
inth
isco
nte
xt.
Qu
alit
ativ
est
udy
usi
ng
sem
i-st
ruct
ure
din
terv
iew
s
13ju
nio
rdo
ctor
san
d12
jun
ior
nu
rses
from
hos
pita
lsac
ross
New
Zea
lan
d
•A
codi
ng
theo
reti
calf
ram
ewor
kw
asid
enti
fied
,sh
owin
gth
e
fact
ors
nec
essa
ryfo
rco
llabo
rati
on.
•Q
ual
ity
ofco
llabo
rati
on:m
utu
alre
spec
t,tr
ust
,org
aniz
atio
nal
stru
ctu
reor
cult
ure
.
•Sh
ared
men
talm
odel
s:h
owin
form
atio
nis
shar
ed,s
har
ed
prio
riti
es.
•Te
amco
ordi
nat
ion
:defi
nin
gro
les
wit
hin
the
team
,coo
rdin
atin
g
deci
sion
-mak
ing
acro
ssth
ete
am,t
eam
lead
ersh
ip,o
rien
tin
gn
ew
team
mem
bers
•C
omm
un
icat
ion
envi
ron
men
t:op
enn
ess
ofco
mm
un
icat
ion
,
spea
kin
gu
p.
Hu
ghes
&Fi
tzpa
tric
k(2
010)
Toev
alu
ate
atti
tude
sto
war
ds
colla
bora
tion
amon
gn
urs
es
and
phys
icia
ns.
Com
para
tive
desc
ript
ive
stu
dy
usi
ng
Th
eJe
ffer
son
Scal
eof
Att
itu
des
tow
ard
Phy
sici
an-N
urs
eC
olla
bora
tion
118
nu
rses
and
53ph
ysic
ian
s
from
aco
mm
un
ity
hos
pita
lin
the
Nor
thea
ster
nU
nit
edSt
ates
•N
urs
esh
ave
asi
gnifi
can
tly
mor
epo
siti
veat
titu
deth
anph
ysic
ian
s
tow
ards
colla
bora
tion
.
•N
urs
espe
rcei
veth
eim
port
ance
ofsh
ared
edu
cati
onm
ore
than
phys
icia
ns.
Nu
rses
scor
edh
igh
erth
anph
ysic
ian
son
‘phy
sici
an’s
auth
orit
y’.
Nel
son
etal
.(20
08)
Tode
scri
ben
urs
e–ph
ysic
ian
perc
epti
ons
ofco
llabo
rati
on
rela
tion
ship
onge
ner
al
med
ical
surg
ical
un
its.
Des
crip
tive
stu
dyu
sin
gth
eC
PS
95n
urs
esan
d49
phys
icia
ns
from
ah
ospi
tali
nSa
nD
iego
,
Cal
ifor
nia
•St
atis
tica
lsig
nifi
can
tdi
ffer
ence
inp
erce
ptio
ns
ofco
llabo
rati
ve
beh
avio
urs
betw
een
the
nu
rses
and
phys
icia
ns.
•N
urs
esla
ckas
sert
iven
ess
inco
mm
un
icat
ing
wit
hdo
ctor
sth
eir
con
trib
uti
ons
topa
tien
tca
re.
•P
hysi
cian
sva
lue
and
use
inpu
tfr
omn
urs
esan
dar
eco
mfo
rtab
le
wit
hth
ero
leof
phys
icia
n–n
urs
eco
llabo
rati
onim
prov
ing
pati
ent
care
.
Th
omso
n(2
007)
Tode
term
ine
atti
tude
sof
nu
rses
and
phys
icia
ns
rega
rdin
gth
eir
colla
bora
tion
.
Des
crip
tive
pros
pect
ive
stu
dy
usi
ng
Th
eJe
ffer
son
Scal
eof
Att
itu
des
tow
ard
Phy
sici
an-N
urs
eC
olla
bora
tion
65n
urs
esan
d37
phys
icia
ns
from
am
edic
alce
ntr
ein
Sou
ther
n
Un
ited
Stat
es
•N
urs
esh
adm
ore
posi
tive
atti
tude
sth
anph
ysic
ian
sto
war
ds
colla
bora
tion
.
•B
oth
shar
edpo
siti
veat
titu
des
rega
rdin
gco
llabo
rati
onin
area
sof
shar
eded
uca
tion
and
team
wor
k,ca
rin
gvs
.cu
rin
g,an
dn
urs
es’
auto
nom
y.
296 C. J. Tang et al.
© 2013 International Council of Nurses

Bu
rns
(201
1)To
dete
rmin
eif
war
dro
un
ds
impr
ove
phys
icia
n–n
urs
e
colla
bora
tion
.
Inte
rven
tion
stu
dyw
her
e
phys
icia
n–n
urs
ero
un
dsw
ere
impl
emen
ted
over
4w
eeks
,
follo
wed
byfi
ve-q
ues
tion
Like
rtsc
ale
surv
ey
Nu
rses
and
phys
icia
ns
from
a
45-b
edm
edic
alu
nit
ina
trau
ma
hos
pita
lwit
hin
ala
rge
Mid
wes
tern
city
•N
urs
e–ph
ysic
ian
rou
nds
incr
ease
dca
reef
fici
ency
.Ave
rage
nu
mbe
rof
calls
mad
eto
phys
icia
ns
decr
ease
daf
ter
impl
emen
tati
onof
rou
nds
.
•N
urs
e–ph
ysic
ian
rou
nds
impr
oved
qual
ity
ofpa
tien
tca
rean
d
inte
r-pr
ofes
sion
alco
mm
un
icat
ion
.
Ros
enst
ein
(200
2)To
asse
ssth
eat
mos
pher
ean
d
sign
ifica
nce
ofn
urs
e–ph
ysic
ian
rela
tion
san
dde
term
ine
the
infl
uen
ceof
disr
upt
ive
phys
icia
nbe
hav
iou
ron
nu
rse
sati
sfac
tion
and
rete
nti
on.
Des
crip
tive
stu
dyu
sin
g
Nu
rse-
Phy
sici
anR
elat
ion
ship
Surv
ey
720
nu
rses
and
173
phys
icia
ns
from
84h
ospi
tals
acro
ssW
est
Coa
st
•P
hysi
cian
sra
ted
atm
osph
ere
ofw
ork
rela
tion
ship
sm
ore
posi
tive
lyth
ann
urs
es,v
iew
edw
ork
rela
tion
ship
sle
sssi
gnifi
can
t
than
nu
rses
,an
dpe
rcei
ved
that
they
valu
en
urs
es’i
npu
tsan
d
colla
bora
tion
.
•N
urs
esra
ted
‘phy
sici
anaw
aren
ess
ofim
port
ance
ofth
e
nu
rse-
phys
icia
nre
lati
onsh
ipto
nu
rse
sati
sfac
tion
’low
erth
an
phys
icia
ns
did.
•D
isru
ptiv
eph
ysic
ian
beh
avio
ur
affe
cted
nu
rse
rete
nti
onra
tes,
sati
sfac
tion
leve
lsan
dm
oral
e.
Mill
eret
al.(
2008
)To
exam
ine
nu
rsin
gem
otio
n
wor
kan
din
ter-
prof
essi
onal
colla
bora
tion
inor
der
to
un
ders
tan
dan
dim
prov
e
colla
bora
tive
nu
rsin
gpr
acti
ce.
Qu
alit
ativ
est
udy
usi
ng
non
-par
tici
pan
tob
serv
atio
n,
shad
owin
gan
d
sem
i-st
ruct
ure
din
terv
iew
s
Con
duct
edin
thre
epu
blic
hos
pita
lsin
Can
ada
wit
h20
nu
rses
,7do
ctor
s,18
allie
d
hea
lth
prof
essi
onal
san
d5
adm
inis
trat
ive/
man
agem
ent
staf
f
•N
urs
es’c
olla
bora
tion
wit
hot
her
hea
lth
prof
essi
onal
sis
show
nto
bein
flu
ence
dby
emot
ion
wor
kco
nsi
dera
tion
s.
Rob
inso
net
al.(
2010
)To
expl
ore
nu
rse
and
phys
icia
n
perc
epti
ons
ofef
fect
ive
and
inef
fect
ive
com
mu
nic
atio
n
betw
een
the
two
prof
essi
ons.
Qu
alit
ativ
est
udy
usi
ng
focu
s
grou
pin
terv
iew
s
Con
duct
edat
ah
ealt
hsc
ien
ce
cen
tre
inth
eU
SA,w
ith
18
regi
ster
edn
urs
esan
d
phys
icia
ns
ofat
leas
t5
year
sof
wor
kin
gex
peri
ence
s
•T
hem
esch
arac
teri
zin
gef
fect
ive
com
mu
nic
atio
nan
din
effe
ctiv
e
com
mu
nic
atio
nw
ere
iden
tifi
ed.
•Fo
ref
fect
ive
com
mu
nic
atio
n:c
lari
tyan
dpr
ecis
ion
ofm
essa
ge
that
relie
son
veri
fica
tion
,col
labo
rati
vepr
oble
mso
lvin
g,ca
lman
d
supp
orti
vede
mea
nou
ru
nde
rst
ress
,mai
nte
nan
ceof
mu
tual
resp
ect,
and
auth
enti
cu
nde
rsta
ndi
ng
ofth
eu
niq
ue
role
.
•Fo
rin
effe
ctiv
eco
mm
un
icat
ion
:mak
ing
som
eon
ele
ssth
an,
depe
nde
nce
onel
ectr
onic
syst
ems,
and
lingu
isti
can
dcu
ltu
ral
barr
iers
.
Nai
ret
al.(
2012
)To
delin
eate
freq
uen
tly
use
dfr
om
infr
equ
entl
yu
sed
colla
bora
tive
beh
avio
urs
ofn
urs
esan
d
phys
icia
ns
inor
der
toge
ner
ate
data
tosu
ppor
tsp
ecifi
c
inte
rven
tion
sfo
rim
prov
ing
colla
bora
tive
beh
avio
ur.
Des
crip
tive
stu
dyu
sin
gth
e
Nu
rse-
Phy
sici
anC
olla
bora
tion
Scal
edi
vide
din
toth
ree
subs
cale
s:sh
arin
gpa
tien
t
info
rmat
ion
,dec
isio
n-m
akin
g
proc
ess,
and
rela
tion
ship
betw
een
nu
rse
and
phys
icia
n.
Item
sw
ere
scor
edu
sin
ga
5-it
emLi
kert
scal
e(1
=al
way
s,
5=
nev
er)
Con
duct
edat
anac
ute
care
hos
pita
lin
the
Mid
wes
t,w
ith
114
nu
rses
and
33ph
ysic
ian
s
from
over
37cl
inic
al
spec
ialt
ies.
•T
he
mos
tfr
equ
entl
yu
sed
nu
rse–
phys
icia
nco
llabo
rati
ve
beh
avio
urs
repo
rted
byn
urs
esw
ere
insu
bsca
le1:
shar
ing
pati
ent
info
rmat
ion
.
•T
he
mos
tfr
equ
entl
yu
sed
nu
rse–
phys
icia
nco
llabo
rati
ve
beh
avio
urs
repo
rted
byph
ysic
ian
sw
ere
insu
bsca
le3:
the
rela
tion
ship
betw
een
nu
rses
and
phys
icia
ns.
•T
he
mos
tin
freq
uen
tly
use
dn
urs
e–ph
ysic
ian
colla
bora
tive
beh
avio
urs
repo
rted
bybo
thw
ere
insu
bsca
le2:
deci
sion
-mak
ing
onca
re/c
ure
.
ICU
,in
ten
sive
care
un
it;I
CU
MA
Q,I
nte
nsi
veC
are
Un
itM
anag
emen
tA
ttit
ude
sQ
ues
tion
nai
re;K
SNP
S,K
ram
eran
dSc
hm
alen
berg
Nu
rse-
Phy
sici
anSc
ale;
CP
S,C
olla
bora
tive
Pra
ctic
eSc
ale.
Physician–nurse collaboration 297
© 2013 International Council of Nurses

more important to achieve better patient outcomes (Dougherty& Larson 2005; Hughes & Fitzpatrick 2010; Sirota 2007).
Quality of physician–nurse collaboration
Three quantitative studies (Rosenstein 2002; Thomas et al.2003; Vazirani et al. 2005) revealed that physicians rated thequality of collaboration – effectiveness and satisfaction level –higher than that of nurses. For example, Thomas et al. (2003)conducted a study in eight intensive care units (ICUs) withinHouston where 90 physicians and 230 nurses were surveyedusing the ICUMAQ. Seventy-three per cent (n = 90) of physi-cians rated the quality of collaboration and communicationwith nurses as high or very high. However, only 33% (n = 230)of nurses rated the quality of collaboration with physicians ashigh or very high (Thomas et al. 2003). The results could berelated to how the two professions defined physician–nurse col-laboration. Physicians equated collaboration with giving ordersand expecting cooperation from nurses to follow through withtheir decisions (Sirota 2007). Although nurses were able toperform tasks and carry out physicians’ orders correctly, manyof them looked forward to having greater autonomy and shareddecision-making capacities with physicians to influence patientcare (Sirota 2007; Vazirani et al. 2005).
Physicians and nurses’ satisfaction with their collaborationmay also be influenced by traditionally rooted stereotypicalideals that society imposes on their roles as healthcare profes-sionals (Hojat et al. 2003; Thomas et al. 2003). Nurses wereoften viewed as ‘handmaidens’ of physicians, while physicianswere perceived as leaders of the healthcare team. The differentstatuses and autonomy attached with these stereotypical idealshave made collaboration a stifling experience for many nurses(Thomas et al. 2003; Vazirani et al. 2005). Conversely, physi-cians possess greater power in decision-making which couldhave caused them to have a lesser interest and thereby lowerexpectations for effective collaboration (Hansson et al. 2009;Hojat et al. 2003).
Factors affecting physician–nurse collaboration
Many of the reviewed studies have identified major factors thataffected collaboration such as communication, respect andtrust, and unequal power between physicians and nurses(McCaffrey et al. 2010; Robinson et al. 2010; Rosenstein 2002;Rosenstein & O’Daniel 2005; Thomas et al. 2003; Weller et al.2011). The lack of understanding about each others’ profes-sional roles and task prioritizing were also found to be influenc-ing factors (Nathanson et al. 2011; Robinson et al. 2010;Rosenstein 2002; Weller et al. 2011).
Communication
Effective communication is essential to building good workingrelationships between physicians and nurses (Petri 2010) andensuring patient care is delivered correctly and timely (Sirota2007). However, four reviewed studies found that communica-tion between both professions tends to be unclear and imprecise(McCaffrey et al. 2010; Robinson et al. 2010; Rosenstein 2002;Weller et al. 2011). This resulted in delayed delivery of patientcare and more frequent medical errors that ultimately jeopard-ized patients’ safety (McCaffrey et al. 2010; Rosenstein 2002).Such problematic communication issues between physiciansand nurses were reported to occur more commonly in medical–surgical wards than in ICUs (McCaffrey et al. 2010; Robinsonet al. 2010; Rosenstein 2002; Weller et al. 2011). Unlike inmedical–surgical wards, a continuous and regular presence ofdoctors in ICUs enabled nurses to clarify any doubts face-to-face and thereby improve the communication process(Schmalenberg & Kramer 2009). Furthermore, a higher acuityof patients in ICUs may have encouraged greater vigilanceamong physicians and nurses in ensuring their clarity of com-munication (Robinson et al. 2010; Sirota 2007).
Ambiguous communication between physicians and nurseshas led to unpleasant behaviours, especially among the physi-cians. A study by Rosenstein (2002) on the perceptions of 720nurses and 173 physicians from 84 hospitals in Northern Cali-fornia towards collaboration highlighted that nurses often failedto gather all relevant patient information before calling the phy-sicians. This unclear communication caused physicians to raisetheir voices rudely, which significantly affected the nurses’ atti-tudes towards patient care and hindered teamwork (Rosenstein2002). Moreover, Weller et al. (2011) observed that physiciansand nurses nowadays communicated more frequently throughwritten patient care records, where information was not alwaysconveyed accurately or read timely. The dependence on elec-tronic messaging systems has also caused more problems incommunication between physicians and nurses (Robinson et al.2010).
Respect and trust
Nurses in several reviewed studies perceived that their effort,professional assessments or inputs regarding patient care werenot valued by the physicians (Robinson et al. 2010; Rosenstein2002; Rosenstein & O’Daniel 2005; Thomas et al. 2003; Welleret al. 2011). This finding was evident across both medical–surgical wards and ICUs (Thomas et al. 2003; Weller et al.2011). Such dismissive attitudes caused nurses to experience alack of respect and trust, which significantly hampered thedevelopment of a more collaborative physician–nurse relation-ship (Thomas et al. 2003; Weller et al. 2011). The perceived
298 C. J. Tang et al.
© 2013 International Council of Nurses

arrogance of some physicians further contributed to the hostileworking environment, making it difficult to establish respectfulrelationships (Sirota 2007; Weller et al. 2011). In contrast, aquantitative study conducted by Nelson et al. (2008) using ‘Col-laborative Practice Scale (CPS)’ revealed that physicians actuallyhighly valued and utilized the inputs contributed by nurses.Although this finding was incongruent to the other reviewedstudies, the possibility of research biases from single site studyand convenience sampling has been acknowledged by theauthors (Nelson et al. 2008).
Many reviewed studies found that physicians tended todisplay disruptive behaviours towards nurses, though some-times the reverse is observed as well (Robinson et al. 2010;Rosenstein 2002; Rosenstein & O’Daniel 2005). In a qualitativestudy using focus group interviews, nurses expressed that physi-cians often used words that were rude and humiliating. Thismade them feel incompetent and intimidated, which hadresulted in a lack of and fear of communication with physicians(Robinson et al. 2010). Other disruptive behaviours reportedincluded yelling, using condescending tones towards another,and berating patients and colleagues. These behaviours had sig-nificantly affected the nurses’ work satisfaction, their attitudestowards patients, and perceptions towards collaboration(Rosenstein 2002; Vazirani et al. 2005). It had also compromisedthe quality and safety of patient care delivered (Rosenstein2002; Rosenstein & O’Daniel 2005).
Understanding professional roles
Robinson et al. (2010) pointed out that there is a lack of under-standing about the unique professional role of nurses, leading toineffective collaboration between physicians and nurses. Nurseswere often perceived by physicians to be only responsible forcarrying out their treatment orders (Robinson et al. 2010).Sirota (2007) highlighted that nurses, who have frequentcontact with patients and family members, could actually con-tribute more to patient care by offering their perspectives andparticipate in decision-making. However, physicians tend tohave minimal insights into these roles of nurses and this couldbe observed through certain dismissive words or behavioursthey exhibit (Sirota 2007). Hence, the important role of nursesin making such contributions towards patient care is disre-garded (Nathanson et al. 2011; Robinson et al. 2010). Thisinevitably caused nurses to experience a lack of autonomy andlower professional worth with respect to decision-making,which in turn limits the effectiveness of physician–nurse col-laboration (Nathanson et al. 2011).
Task prioritizing
Two of the reviewed studies, despite varying in methodologicalapproaches, reported consistently that collaboration was
affected by the different priorities physicians and nurses hadwith regard to patient care (Rosenstein 2002; Weller et al. 2011).The junior physicians in Weller et al.’s study (2011) reportedthat nurses did not always understand the rationale behindcertain treatments. As a result, given limited work time, nurseschose to complete other tasks that they perceived as moreimportant or urgent (Weller et al. 2011). These differences intask prioritizing not only caused physicians and nurses todevelop feelings of frustration towards each other, but in somecases led to delays in the delivery of effective patient care(Rosenstein 2002; Weller et al. 2011).
Similarly, junior nurses reported feeling annoyed when physi-cians chose to disregard certain important concerns they hadabout patients’ condition and progress (Weller et al. 2011).Stein-Parbury & Liaschenko (2007) explained that this phe-nomenon could be due to physicians and nurses possessing dif-ferent knowledge about their patients. Physicians tend to assesspatients’ conditions based on objective values such as vital signsand laboratory investigations whereas nurses tend to use moreof their intuitions, observations and understanding of humanexperiences of diseases (Stein-Parbury & Liaschenko 2007).Therefore, it was observed that physicians chose to reviewpatients more promptly when nurses reported factual evidenceof deterioration such as vital signs, rather than their generalobservations of patients (Stein-Parbury & Liaschenko 2007;Weller et al. 2011).
Unequal power
Petri (2010) advocated that physicians and nurses shouldpossess equal decision-making capacity, responsibility andpower. However, a descriptive comparative study by Nelsonet al. (2008) reported that nurses did not feel confident or asser-tive enough to communicate and discuss patient care on equalplatforms with physicians. Nurses perceived a power imbalancebetween both professions (Nelson et al. 2008). Hansson et al.(2009) explained that this unequal power could be attributed tothe different levels of education, status and prestige that areunique to each profession. Although both aforementionedstudies were conducted in medical–surgical wards, similar find-ings were observed in studies carried out within ICUs(Papathanassolgou et al. 2012; Rose 2011). In several reviewedstudies, it was also suggested that interactions between physi-cians and nurses were strongly influenced by their traditionalcultural roots, where typically there was medical dominanceand nursing subservience (Hansson et al. 2009; Hojat et al.2003; Thomas et al. 2003; Vazirani et al. 2005). By possessingmore powerful positions, physicians often do not see collabora-tion with nurses or shared decision-making as being necessary
Physician–nurse collaboration 299
© 2013 International Council of Nurses

for effective patient care. Furthermore, nurses at the same timehesitate to communicate on ground levels with physicians(Hansson et al. 2009).
Another descriptive comparative study by Nair et al. (2012)found that ‘decision-making on care or cure’ was the least fre-quent physician–nurse collaborative behaviour used by bothprofessions. Physicians tended to dominate the decision-makingprocess whereas nurses were usually seen to simply follow suit(Hansson et al. 2009; Hojat et al. 2003; Nair et al. 2012). Asnurses were traditionally more likely to use obliging and com-promising conflict management styles and avoid assertivebehaviours, it allowed physicians to possess greater authority inclinical decision-making (Nair et al. 2012). This has furthercontributed to the power imbalance between both healthcareprofessions (Nair et al. 2012).
Improvement strategies for physician–nurse collaboration
Majority of the reviewed studies strongly proposed the imple-mentation of strategies to enhance physician–nurse collabora-tion. The strategies implemented by four interventional studiesinclude IPE (McCaffrey et al. 2010; Messmer 2008) and inter-disciplinary ward rounds (Burns 2011; Vazirani et al. 2005).
IPE
McCaffrey et al. (2010) implemented an inter-professional edu-cational program in a hospital setting over a 6-month period,involving 50 medical residents and 65 nurses who worked inmedical wards. The program covered topics such as effectivecommunication skills, body language, and essential determi-nants of good collaborative practice (McCaffrey et al. 2010).The effectiveness of the program was evaluated using focusgroup interviews. Both physicians and nurses shared that theprogram has helped them foster comfortable friendships,develop positive communication skills, learn to accept eachothers’ perspectives regarding patients’ condition, and prioritizepatient care together (McCaffrey et al. 2010).
Using a quantitative study approach, Messmer (2008) con-ducted an inter-professional simulation program in a children’shospital, where physicians and nurses were exposed to three dif-ferent life-threatening simulated situations. Their performancesand interactions were observed and scored by three independ-ent observers using the Kramer and Schmalenberg Nurse-Physician Scale. The study outcome revealed that with moresimulation exposures, physician–nurse collaboration improvedsignificantly where both professions treated each other withgreater respect and trust, and gained deeper insights into eachothers’ roles and responsibilities (Messmer 2008).
Interdisciplinary ward rounds
Two intervention studies explored the effectiveness of interdis-ciplinary ward rounds in medical units in different parts of theUSA (Burns 2011; Vazirani et al. 2005). Both studies providedevidence on the effectiveness of daily medical ward rounds inimproving the quality of patient care and physician–nurse com-munication. With effective ward rounds, communication ofimportant information could be done face-to-face and therebyreducing the need for subsequent phone calls to clarify doubts(Burns 2011; Vazirani et al. 2005). A similar outcome was alsoreported in Schmalenberg & Kramer’s (2009) study, whichevaluated interdisciplinary ward rounds in ICUs and specializedunits from across 26 hospitals in 2003 and 34 hospitals in 2007within the USA. The study reported that regular interdiscipli-nary rounds with active participation from nurses could boosttheir self-confidence in communicating with physicians. Suchintervention also significantly improved physician–nurse col-laboration (Schmalenberg & Kramer 2009).
Despite the effectiveness of ward rounds in improving col-laboration, the heavy patient workload and insufficient time tocomplete individual tasks had affected the doctors and nurses’willingness and sense of urgency to round as a team (Burns2011; Miller et al. 2008; Rosenstein 2002; Weller et al. 2011). InBurn’s study (2011), it was observed that participation rates inward rounds declined after the fourth week of implementa-tion. Vazirani et al. (2005) recommended that the implementa-tion and evaluation of interdisciplinary ward rounds beconducted over a longer period, for example, 2 years, in orderto observe any significant improvements in physician–nursecollaboration.
DiscussionPhysician–nurse collaboration is a complex interpersonalprocess between physicians and nurses. In reviewing the litera-ture on the attitudes of hospitals’ physicians and nursestowards collaboration, it was found that such attitudes havebeen explored mainly in the hospitals in Western countries,especially those within the USA. Little is known about the atti-tudes of physicians and nurses towards collaboration in hospi-tals beyond this region. As a result of possible cultural andsocial differences, findings of studies conducted in one countryor region may not be fully applicable to other countries. Amutual understanding of attitudes towards collaboration canserve as a first step for physicians and nurses to recognize spe-cific challenges both face in working together, and identifysolutions to enhance partnership (James et al. 2010). Morefuture studies are therefore needed to continue exploringthe attitudes of physicians and nurses towards collaborationin various settings. Besides exploratory studies, the review
300 C. J. Tang et al.
© 2013 International Council of Nurses

identified the need for more intervention research studies thatuse more rigorous methodology such as randomized controlledtrials to evaluate their effectiveness on improving physician–nurse collaboration.
Different types of questionnaires were adopted by thereviewed studies to measure attitudes of physicians and nursestowards collaboration. Although the validities and reliabilities ofthese questionnaires were well documented, each questionnairewas developed to only intentionally measure attitudes towardscertain aspects of collaboration in specific settings (Dougherty& Larson 2005). A broad rather than narrow focus is importantin enhancing the understanding of physician–nurse collabora-tion. Moreover, the findings of this review have identifiedseveral factors affecting physician–nurse collaboration in a hos-pital environment. Future research could aim to develop a com-prehensive instrument that explores attitudes in a greater depthand broader scope.
The review identified a considerable amount of literatureaddressing perceptions towards improving collaboration fromphysicians and nurses working on the ground level. There hasbeen little research that examined the role of senior physiciansand nursing administrators in facilitating collaboration. Jameset al. (2010) highlighted a need for the executive hospital com-mittee from both medicine and nursing to clarify perceptionsand define expectations for the two professions before takingthe lead to develop a partnered plan for enhanced workingrelationships.
In view of unequal power existing between physicians andnurses, policy makers could look more into regulation of thenursing profession whereby nurses are granted more autonomyin making clinical decisions on patient care. To furtherempower nurses with clinical knowledge and decision-makingskills, there could be hospital-based IPE programs for both phy-sicians and nurses to learn from one another. With greaterknowledge and capacity to make clinical decisions, it is believedthat nurses may become more confident in communication andsatisfied with the collaborative practice experience. Further-more, leaders of the hospital management boards could takemore concrete steps to deal with workplace issues such as con-flicts and disagreements between both professions, for instance,by creating an open forum and conducting regular discussionsessions for physicians and nurses to resolve differences or shareany unpleasant experiences related to collaboration (Rosenstein2002). Conflict management guidelines could also be drawn upand disseminated to both professions, so that any discontent-ment can be addressed promptly and effectively.
This literature review has several limitations. Althoughundertaken carefully and systematically, the listed search strat-egy might not have identified all the relevant literature. The
relatively small number of articles that met the inclusion criteriain this review and their methodological approaches could haveintroduced bias.
ConclusionThis integrated literature review has sought to present the bestavailable evidence on physician–nurse collaboration. The reviewfound that both physicians and nurses working in the hospitalsetting possessed differing attitudes towards the importance andquality of physician–nurse collaboration. Their attitudes werefound to be influenced by factors including communication,respect and trust, unequal power, understanding other profes-sional roles, and task prioritizing. The review also identifiedstrategies such as IPE and interdisciplinary ward rounds thatcould improve physician–nurse collaboration. More researchefforts, along with policy and practice implications, would bekey to improving collaborative practice between hospital physi-cians and nurses.
Author contributionsAll the above authors have approved the final version of thearticle. I acknowledge that all those entitled to authorship arelisted as authors. Charmaine Tang has contributed to the con-ception design of the study, acquisition of data, analysis andinterpretation of the data, drafting the article, and critical revi-sion of the article. Sally Wai-chi Chan has contributed to theconception design of the study and critical revision of thearticle. Wentao Zhou has contributed to the critical revision ofthe article. Sok Ying Liaw has contributed to the conceptiondesign of the study, analysis and interpretation of the data, criti-cal revision of the article, and supervision.
ReferencesBurns, K. (2011) Nurse-physician rounds: a collaborative approach to
improving communication, efficiencies, and perception of care. Medsurg
Nursing, 20 (4), 194–199.
Dougherty, M.B. & Larson, E. (2005) A review of instruments measuring
nurse-physician collaboration. The Journal of Nursing Administration,
35 (5), 244–253.
Garber, J., Madigan, E., Click, E. & Fitzpatrick, J. (2009) Attitudes towards
collaboration and servant leadership among nurses, physicians and resi-
dents. Journal of Interprofessional Care, 23 (4), 331–340.
Hansson, A., et al. (2009) Working together- primary care doctors’ and
nurses’ attitudes to collaboration. Scandinavian Journal of Public Health,
38, 78–85.
Hojat, M., et al. (2003) Comparisons of American, Israeli, Italian and
Mexican physicians and nurses on the total and factor scores of the
Jefferson scale of attitudes toward physician-nurse collaborative relation-
ships. International Journal of Nursing Studies, 40, 427–435.
Physician–nurse collaboration 301
© 2013 International Council of Nurses

Hughes, B. & Fitzpatrick, J. (2010) Nurse-physician collaboration in an
acute care community hospital. Journal of Interprofessional Care, 24 (6),
625–632.
James, J., Butler-Williams, C., Hunt, J. & Cox, H. (2010) Vital signs for
vital people: an exploratory study into the role of the healthcare
assistant in recognising, recording and responding to the acutely ill
patient in the general ward setting. Journal of Nursing Management, 18,
548–555.
Kramer, M. & Schmalenberg, C. (2003) Securing ‘good’ nurse physician
relationships. Nursing Management, 34 (7), 34–38.
Lim, J., Bogossian, F. & Ahern, K. (2010) Stress and coping in Singaporean
nurses: a literature review. Nursing and Health Sciences, 12,
251–258.
McCaffrey, R., et al. (2010) A program to improve communication and
collaboration between nurses and medical residents. Journal of Continu-
ing Education in Nursing, 41 (4), 172–178.
Messmer, P. (2008) Enhancing nurse-physician collaboration using pediat-
ric simulation. Journal of Continuing Education in Nursing, 39 (7), 319–
327.
Miller, K.L., et al. (2008) Nursing emotion work and interprofessional col-
laboration in general internal medicine wards: a qualitative study.
Journal of Advanced Nursing, 64 (4), 332–343.
Morinaga, K., Ohtsubo, Y., Yamauchi, K. & Shimada, Y. (2008) Doctors’
traits perceived by Japanese nurses as communication barriers: a
questionnaire survey. International Journal of Nursing Studies, 45, 740–
749.
Nair, D.M., et al. (2012) Frequency of nurse-physician collaborative behav-
iors in an acute care hospital. Journal of Interprofessional Care, 26 (2),
115–120.
Nathanson, B.H., et al. (2011) How much teamwork exists between nurses
and junior doctors in the intensive care unit? Journal of Advanced
Nursing, 67 (8), 1817–1823.
Nelson, G., King, M. & Brodine, S. (2008) Nurse-physician collaboration
on medical-surgical units. Medsurg Nursing, 17 (1), 35–40.
Papathanassolgou, E.D.E., et al. (2012) Professional autonomy, collabora-
tion with physicians, and moral distress among European intensive care
nurses. American Journal of Critical Care, 21, e41–e52.
Petri, L. (2010) Concept analysis of interdisciplinary collaboration. Nursing
Forum, 45 (2), 73–82.
Robinson, F., Gorman, G., Slimmer, L. & Yudkowsky, R. (2010) Perceptions
of effective and ineffective nurse-physician communication in hospitals.
Nursing Forum, 45 (3), 206–216.
Rose, L. (2011) Interprofessional collaboration in the ICU: how to define?
Nursing in Critical Care, 16 (1), 5–10.
Rosenstein, A.H. (2002) Nurse-physician relationships: impact on nurse
satisfaction and retention. The American Journal of Nursing, 102 (6),
26–34.
Rosenstein, A.H. & O’Daniel, M. (2005) Disruptive behavior & clinical out-
comes: perceptions of nurses & physicians. Nursing Management, 36 (1),
18–29.
Schmalenberg, C. & Kramer, M. (2009) Nurse-physician relationships in
hospitals: 20 000 nurses tell their story. Critical Care Nurse, 29 (1),
74–83.
Seitz, S.J., Lord, C.G. & Taylor, C.A. (2007) Beyond pleasure: emotion
activity affects the relationship between attitudes and behavior. Personal-
ity and Social Psychology Bulletin, 33 (7), 933–947.
Sirota, T. (2007) Nurse/physician relationships: improving or not? .
Nursing, 37 (1), 52–56.
Stein-Parbury, J. & Liaschenko, J. (2007) Understanding collaboration
between nurses and physicians as knowledge at work. American Journal
of Critical Care, 16 (5), 470–478.
Thomas, E.J., Sexton, J.B. & Helmreich, R.L. (2003) Discrepant attitudes
about teamwork among critical care nurses and physicians. Critical Care
Medicine, 31 (3), 956–959.
Thomson, S. (2007) Nurse-physician collaboration: a comparison of the
attitudes of nurses and physicians in the medical-surgical patient care
setting. Medsurg Nursing, 16 (2), 87–91.
Vazirani, S., Hays, R.D., Shapiro, M.F. & Cowan, M. (2005) Effect of a
multidisciplinary intervention on communication and collaboration
among physicians and nurses. American Journal of Critical Care, 14 (1),
71–77.
Weller, J., Barrow, M. & Gasquoine, S. (2011) Interprofessional collabora-
tion among junior doctors and nurses in the hospital setting. Medical
Education, 45 (5), 478–487.
302 C. J. Tang et al.
© 2013 International Council of Nurses