Embed Size (px)
DESCRIPTION
View this SignatureSeries white paper published by Progressive Medical.
Citation preview
Collaboration Curves the Opioid Trend
SeriesPresented by Progressive Medical

Page l 2 Collaboration Curves the Opioid Trend l October 2013
Collaboration Curves the Opioid Trend
Discussions on pain and the inclusion of opioid analgesics as part of the phar-macologic therapy regimen to address
workers’ compensation injuries are rampant throughout our industry. Along with these conversations undercurrents of anxiety to find a solution for the coinciding misuse and abuse runs swiftly. Drug manufacturers are working hard to develop abuse-deterrent formulations while physicians are being pushed to change prescribing practices. Claims professionals are strained to keep up with the demands of their case load, charged with keeping a watchful eye for the signs of malingering, misuse or abuse. Payors are challenged to deliver strong performance ratios and stability, stressing the importance of efficiency and cost containment. Legislatures and regulatory bodies at all levels of government are under pressure to enact tougher legislation. In fact, to say the entire system is under a good deal of stress to better address opioid analgesics would not be an overstatement.
As a workers’ compensation pharmacy benefit manager, Progressive Medical is at the epicenter of the conversa-tion. Our regulatory and compliance team, along with our vice president of government affairs, is tirelessly engaged in the ongoing rhetoric throughout the country. Meanwhile our clinical services and analytics teams are determinedly working with clients to identify potential high-cost, misuse or abuse situations earlier by leveraging data gathered by the network. More control and better outcomes are the fruits of this labor.
Earlier this year in our annual Drug Trend Report we reported an overall prescription spend decrease of 0.5% for our book of business, as well as a 4.2% decrease in the prescription cost per claim of opioid analgesics. We also noted that as a percentage of total prescrip-tion volume, utilization of long-acting opioid analgesics was down compared to the prior year. We concurrently reported on the impact of the Texas Closed Formulary, legislation that limits the prescribing of “N” drugs as indicated by the Official Disability Guidelines (ODG). Clients affected by the change experienced a 16.8% decline in the number of claims using opioid analgesics in the first year of injury after September 1, 2011.4
Subsequent to the release of the Drug Trend Report, a conversation with Peter Rousmaniere, a columnist with Risk & Insurance, sparked a bit of curiosity regarding the influence of legislative changes on opioid utilization in states other than Texas. As we continuously evaluate our program with respect to new legislation it only made sense that we delve further into the subject to see what we would find. In the end, our research and analysis on three specific state regulations revealed some interesting (albeit inconclusive) findings that substantially affirm the need for collaboration among all stakeholders in the system to effectively curve the opioid trend.
400%
The Centers for Disease Control and Prevention reports staggering statistics regarding the severity of the prescription drug epidemic in our country.
Page l 3Collaboration Curves the Opioid Trend l October 2013
The Research
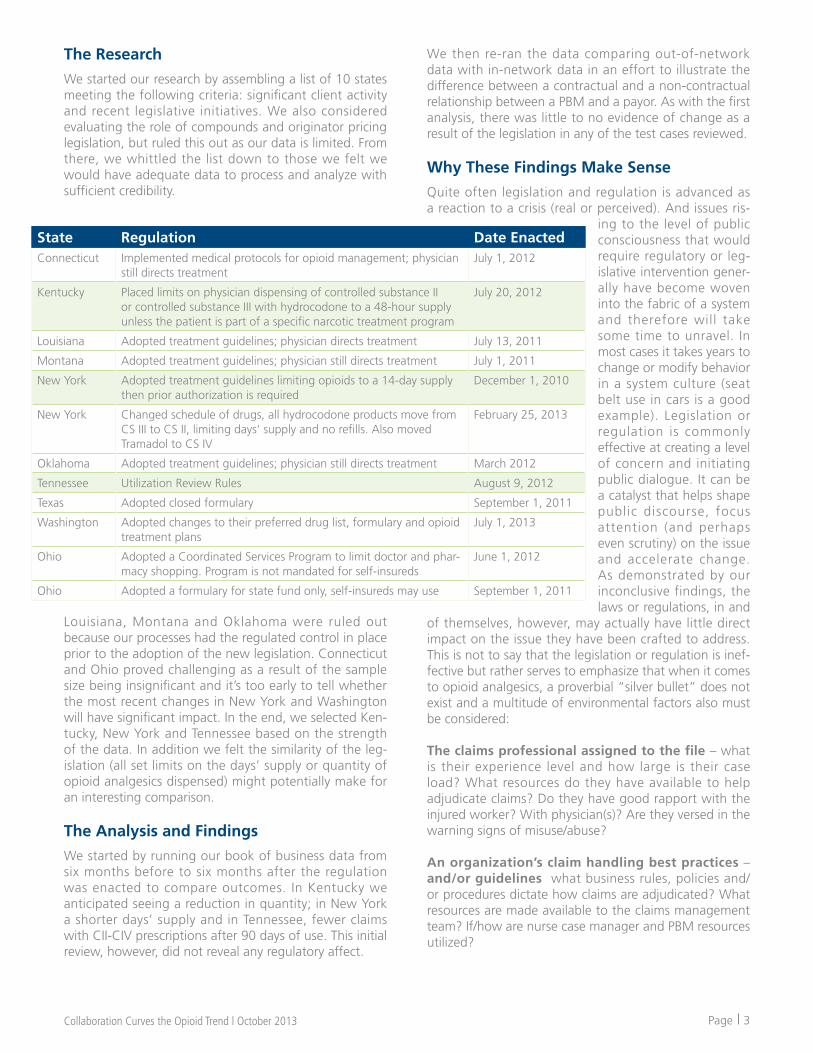
We started our research by assembling a list of 10 states meeting the following criteria: significant client activity and recent legislative initiatives. We also considered evaluating the role of compounds and originator pricing legislation, but ruled this out as our data is limited. From there, we whittled the list down to those we felt we would have adequate data to process and analyze with sufficient credibility.
Louisiana, Montana and Oklahoma were ruled out because our processes had the regulated control in place prior to the adoption of the new legislation. Connecticut and Ohio proved challenging as a result of the sample size being insignificant and it’s too early to tell whether the most recent changes in New York and Washington will have significant impact. In the end, we selected Ken-tucky, New York and Tennessee based on the strength of the data. In addition we felt the similarity of the leg-islation (all set limits on the days’ supply or quantity of opioid analgesics dispensed) might potentially make for an interesting comparison.
The Analysis and Findings
We started by running our book of business data from six months before to six months after the regulation was enacted to compare outcomes. In Kentucky we anticipated seeing a reduction in quantity; in New York a shorter days’ supply and in Tennessee, fewer claims with CII-CIV prescriptions after 90 days of use. This initial review, however, did not reveal any regulatory affect.
State Regulation Date EnactedConnecticut Implemented medical protocols for opioid management; physician
still directs treatmentJuly 1, 2012
Kentucky Placed limits on physician dispensing of controlled substance II or controlled substance III with hydrocodone to a 48-hour supply unless the patient is part of a specific narcotic treatment program
July 20, 2012
Louisiana Adopted treatment guidelines; physician directs treatment July 13, 2011
Montana Adopted treatment guidelines; physician still directs treatment July 1, 2011
New York Adopted treatment guidelines limiting opioids to a 14-day supply then prior authorization is required
December 1, 2010
New York Changed schedule of drugs, all hydrocodone products move from CS III to CS II, limiting days’ supply and no refills. Also moved Tramadol to CS IV
February 25, 2013
Oklahoma Adopted treatment guidelines; physician still directs treatment March 2012
Tennessee Utilization Review Rules August 9, 2012
Texas Adopted closed formulary September 1, 2011
Washington Adopted changes to their preferred drug list, formulary and opioid treatment plans
July 1, 2013
Ohio Adopted a Coordinated Services Program to limit doctor and phar-macy shopping. Program is not mandated for self-insureds
June 1, 2012
Ohio Adopted a formulary for state fund only, self-insureds may use September 1, 2011
We then re-ran the data comparing out-of-network data with in-network data in an effort to illustrate the difference between a contractual and a non-contractual relationship between a PBM and a payor. As with the first analysis, there was little to no evidence of change as a result of the legislation in any of the test cases reviewed. Why These Findings Make Sense
Quite often legislation and regulation is advanced as a reaction to a crisis (real or perceived). And issues ris-
ing to the level of public consciousness that would require regulatory or leg-islative intervention gener-ally have become woven into the fabric of a system and therefore will take some time to unravel. In most cases it takes years to change or modify behavior in a system culture (seat belt use in cars is a good example). Legislation or regulation is commonly effective at creating a level of concern and initiating public dialogue. It can be a catalyst that helps shape public discourse, focus attention (and perhaps even scrutiny) on the issue and accelerate change. As demonstrated by our inconclusive findings, the laws or regulations, in and
of themselves, however, may actually have little direct impact on the issue they have been crafted to address. This is not to say that the legislation or regulation is inef-fective but rather serves to emphasize that when it comes to opioid analgesics, a proverbial “silver bullet” does not exist and a multitude of environmental factors also must be considered:
The claims professional assigned to the file – what is their experience level and how large is their case load? What resources do they have available to help adjudicate claims? Do they have good rapport with the injured worker? With physician(s)? Are they versed in the warning signs of misuse/abuse?
An organization’s claim handling best practices – and/or guidelines what business rules, policies and/or procedures dictate how claims are adjudicated? What resources are made available to the claims management team? If/how are nurse case manager and PBM resources utilized?

Page l 4 Collaboration Curves the Opioid Trend l October 2013
The state of jurisdiction – different states have dif-ferent guidelines and every state has a unique statute addressing workers’ compensation; what is the impact on opioid analgesics? On claim handling? Similarly, geography and other demographics have been shown to influence prescribing patterns and attitudes toward opioid analgesics.
The physician’s experience and prescribing practices – does the physician have pain management expertise? Do they use medication agreements and other tools to monitor the patient’s response to pharmacologic treatment? Is there a referral relationship with another practice group(s)? How long have they been practicing medicine? How often does the physician treat workers’ compensation injuries vs. non-occupational injuries or conditions? Is the physician dispensing medications?
The influence (or lack thereof) of PDMPs – what are the requirements of prescription drug monitoring programs? What, if any, are the penalties for non-compli-ance? How is information gathered and accessed across the system?
Socioeconomic forces – politics, economics, social norms and customs, religious beliefs – all of these factors have influence on the workers’ compensation system in different ways, at different phases of the claim.
Injured worker’s demographics – age, gender, occupa-tion, where they live as well as their personal motivation to recover all influence the injured worker’s response to opioid analgesics, as does the existence (or lack) of a support system and any pre-existing conditions or co-morbidities that are involved, such as obesity, smoking or other behaviors.
Employer practices and policies – what is the safety culture? Do they have a risk management program? Are employees trained to spot (and report) the warning signs of misuse and abuse? How do they interact with their injured workforce? Is a urine drug monitoring program in place?
The legislation itself – how strongly has it been writ-ten? Is action “permitted” or “required”? Are there fines or penalties for non-compliance? Does the legislation include any contradictory or competing elements that might serve to diffuse the desired outcome? For instance, the New York legislation also permits claims professionals to authorize medications prescribed by the physician, while the Tennessee legislation allows for utilization review (UR) on prescriptions with more than 90 days of use; it is not mandated.
The Role of the Pharmacy Benefit Manager
By performing prospective, concurrent and retrospective utilization reviews against injury-specific medication plans or formularies and applying analytics models to flag claims for intervention, PBMs can greatly impact inappropriate opioid use among injured workers – ideally before it even occurs. Their direct collaboration with claims professionals, nurse case managers and physicians can positively influence medication therapy regimens. Meanwhile the pharmacologic expertise and resources they share promote deeper understanding while facilitat-ing a multifaceted approach.
Please bear in mind that PBM programs are influenced by the same “environmental” factors as legislation and regulation. There are numerous factors that can chip away at the effectiveness of the very controls that a PBM can put in place. In fact, legislation itself can impede the PBM’s performance by limiting (or denying) the application of certain controls to the very detriment of the payors the policy is intended to protect. These circumstances would appear to emphasize our conclusion that there is no single factor that can solve the issue of opioid analgesic misuse/overuse/abuse. Collaboration is essential. To serve the industry as a whole, a coordinated approach is needed. The more effectively we all work together, the better the outcome that is possible.

Page l 5Collaboration Curves the Opioid Trend l October 2013
Contributors
Brian Allen, vice president of government affairs Joe Anderson, director of analytic servicesSarah Berger, vice president of marketingTron Emptage, chief clinical officerBarry Jarnigan, chief marketing officerAngela Jenkins, director of regulatory complianceKimberly Schlosser, research analyst
About Progressive Medical
Progressive Medical is a workers’ compensation PBM whose responsibility is to make a difference. By combining the best aspects of PBM and third-party billing programs with evidence-based clinical programs, advanced clinical analytics, proac-tive government affairs and operational excellence, the company is accelerating change in the industry and evolving the traditional payor-PBM relationship. Visit www.progressive-medical.com to learn more.
Resources 1 “Prescription Painkiller Overdoses in the U.S.,” CDC Vital Signs, November 2011, Centers for Disease Control and
Prevention.2 “Opioids Drive Continued Increase in Drug Overdose Deaths,” CDC Newsroom, February 2013, Centers for Disease
Control and Prevention.3 “Prescription Painkiller Overdoses: A growing epidemic, especially among women,” CDC Vital Signs, July 2013, Centers
for Disease Control and Prevention.4 2013 Workers’ Compensation Drug Trend Report, Progressive Medical, April 2013.
















![Non-opioid & Opioid IV Anesthetics Copy [Compatibility Mode]](https://img.pdfslide.net/doc/110x75/55cf8c8a5503462b138d78d4/non-opioid-opioid-iv-anesthetics-copy-compatibility-mode.jpg)










