Embed Size (px)
Citation preview
Colorectal Cancer Screening 101
Patient Education December 2014
Colon Anatomy, Polys, Colorectal Cancer
(CRC) &
Colorectal Cancer Screening Exams
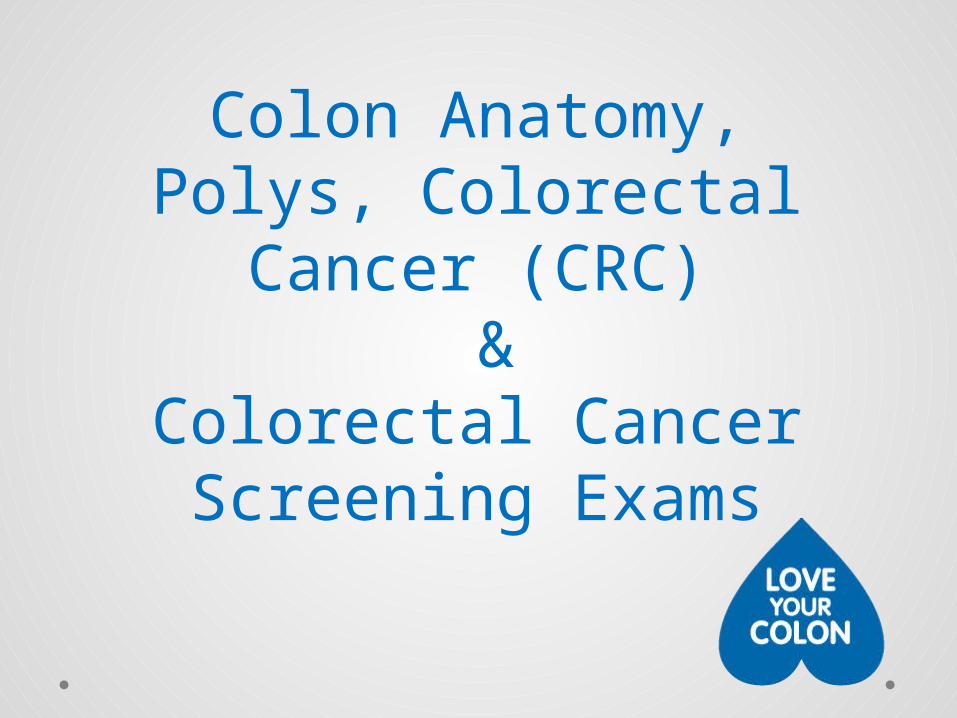
What is the colon?
• Also called the large intestine or large bowel
• Part of the digestive system
• About five (5) feet long
• Absorbs water and nutrients from food you eat
• Removes waste (feces) from your body
http://www.aboutcancer.com/colon_and_rectal_anatomy.htm
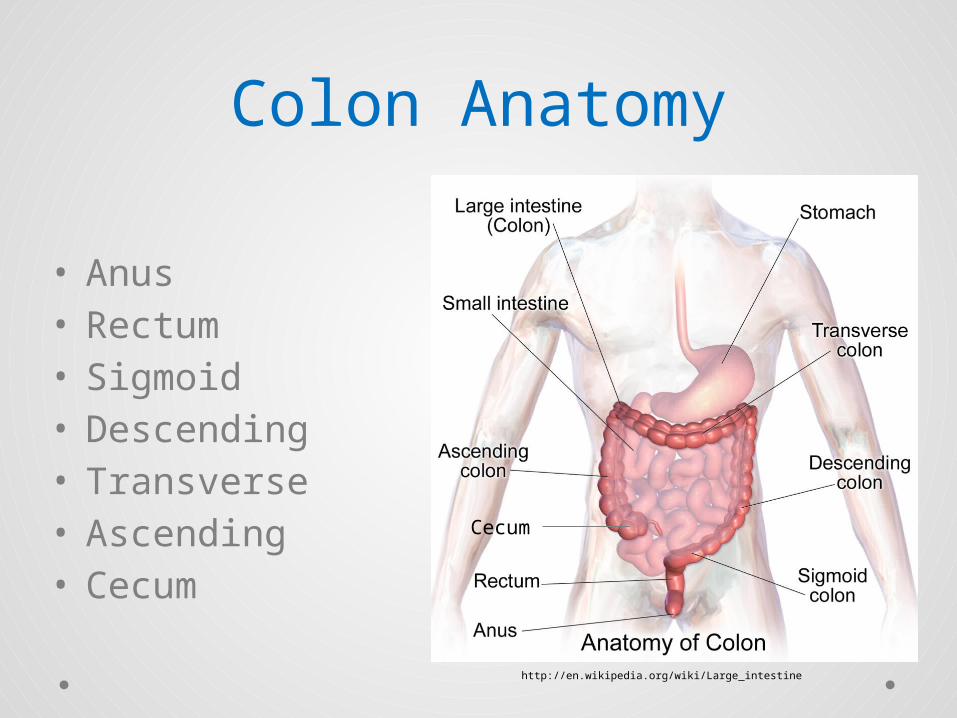
Colon Anatomy
• Anus• Rectum• Sigmoid• Descending• Transverse• Ascending• Cecum
http://en.wikipedia.org/wiki/Large_intestine
Cecum
Colon Polyps• Noncancerous or cancerous growths in the lining of
the colono Vary in sizeo May have a stalk or may be flato Common in adultso Unknown what causes them
Lifestyle factors: High-fat, low-fiber diet, obesity, sedentary lifestyle, etc.
Genetic factors
• Polyps must be removed to determine if the polyp is cancerous or noncancerous
• Biggest risk of developing polyps is being over 50 years
http://www.colon-cleanse-information.com/colon-polyps.html
Common Terms re: Polyps
• Hyperplastico Common, abnormal noncancerous growthso Do not cause any symptoms
• Adenomatouso Pre-cancerous polypso May cause symptoms
• Sessileo Polyps that grow in a flat, broad-based structure
• Serratedo Polyps that have a saw tooth like appearance
• Dysplasiao Describes how much the polyp looks like cancer
• Low-grade: mild or moderate; does not look much like cancer• High-grade: severe; has characteristics of cancer
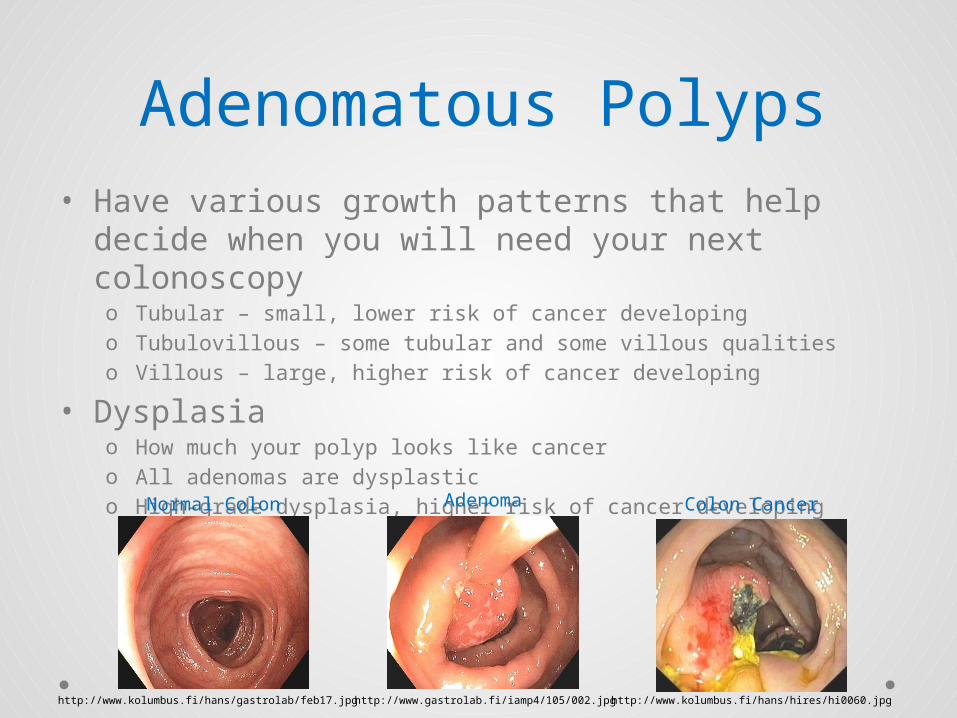
Adenomatous Polyps• Have various growth patterns that help decide
when you will need your next colonoscopyo Tubular – small, lower risk of cancer developingo Tubulovillous – some tubular and some villous qualities o Villous – large, higher risk of cancer developing
• Dysplasiao How much your polyp looks like cancero All adenomas are dysplastico High-grade dysplasia, higher risk of cancer developing
Normal Colon Adenoma Colon Cancer
http://www.kolumbus.fi/hans/hires/hi0060.jpghttp://www.gastrolab.fi/iamp4/105/002.jpghttp://www.kolumbus.fi/hans/gastrolab/feb17.jpg
What is Colorectal Cancer (CRC)?
• Second leading cause of death because of cancer in the U.S.
• Third most common cancer diagnosed in men and women in the U.S.
• It is expected that over 50,000 people will die from colorectal cancer in the U.S. in 2014
• The risk of developing colorectal cancer in your lifetime is about 1 in every 20 people
American Cancer Society. Colon/Rectum Cancer: Detailed Guide. 2013 (revised 1/31/2014). http://www.cancer.org/cancer/colonandrectumcancer/detailedguide/index
CRC in Colorado• About 1,720 people will get colorectal cancer in
Colorado in 2014
o About 44 out of 100,000 men will get CRCo About 34 out of 100,000 women will get CRC
• About 670 people will die from colorectal cancer in Colorado in 2014
o About 17 men out of 100,000 will die from CRCo About 12 women out of 100,000 will die from CRC
American Cancer Society, Cancer Facts & Figures 2014http://www.cancer.org/acs/groups/content/@research/documents/webcontent/acspc-042151.pdf
CRC Risk Factors• Risks you cannot change
o Ageo Family historyo Personal historyo Raceo Genetics
• Risks you can changeo Diet high in red meat/processed meat consumptiono Sedentary lifestyleo Obesityo Cigarette smokingo Alcohol consumption
American Cancer Society. Colon/Rectum Cancer: Detailed Guide. 2013 (revised 1/31/2014). http://www.cancer.org/cancer/colonandrectumcancer/detailedguide/index
Can you prevent CRC?• Screening is the best way to prevent colorectal
cancer
• Screening looks for cancer or pre-cancerous polyps in people who do not have symptoms
• If polyps are found they can be removed before they turn into cancer, preventing colorectal cancer altogether
American Cancer Society. Colon/Rectum Cancer: Detailed Guide. 2013 (revised 1/31/2014). http://www.cancer.org/cancer/colonandrectumcancer/detailedguide/index
Choosing the Right CRC Screening Test for
You
Colonoscopy
Flex Sig
Virtual ColonoscopyPillCam
Stool Testing
CRC Screening Methods• Detect Polyps and Cancer
o Flexible Sigmoidoscopyo Colonoscopyo Computed Tomographic Colonography (virtual colonoscopy)
• Detect Polyps/Abnormalitieso Video capsule (PillCam)
• Detect Cancero High sensitivity FOBT/FITo Stool/Fecal DNA test
Bowel Preparation• Many CRC screening methods require bowel
preparationo Flexible Sigmoidoscopyo Colonoscopyo Computed Tomographic Colonographyo Video Capsule
• Necessary in order to be able to see the colon and find abnormalities and/or polyps
• Requires diet and/or fluid restrictions but will vary according to your doctor’s instructions
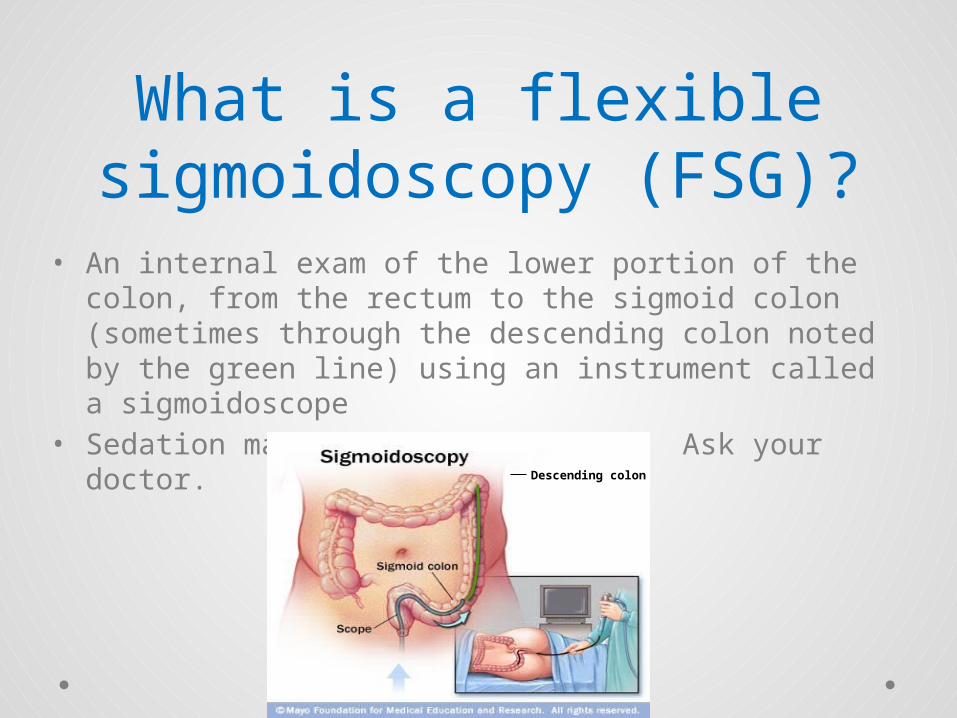
What is a flexible sigmoidoscopy (FSG)?
• An internal exam of the lower portion of the colon, from the rectum to the sigmoid colon (sometimes through the descending colon noted by the green line) using an instrument called a sigmoidoscope
• Sedation may or may not be used. Ask your doctor.
Descending colon
What to expect: FSG• The procedure takes about 10 – 20 minutes
• You will lie on your side with knees drawn up toward your chest
• The sigmoidoscope is inserted through the anus and gently advanced
• Air will be inserted through the scope to provide a better view of the colon
• Careful examination is done during the insertion and withdrawal of the scope
FSG Procedure• Tissue samples may be taken or polyps may be
removed during the procedure
• You may feel pressure and slight cramping during the exam
• If you experience abdominal pain, fever and chills or rectal bleeding following the exam contact your navigator or doctor immediately
• FSG is not sufficient to detect polyps or cancer in the remaining portion of the colon and you may be advised to complete a colonoscopy
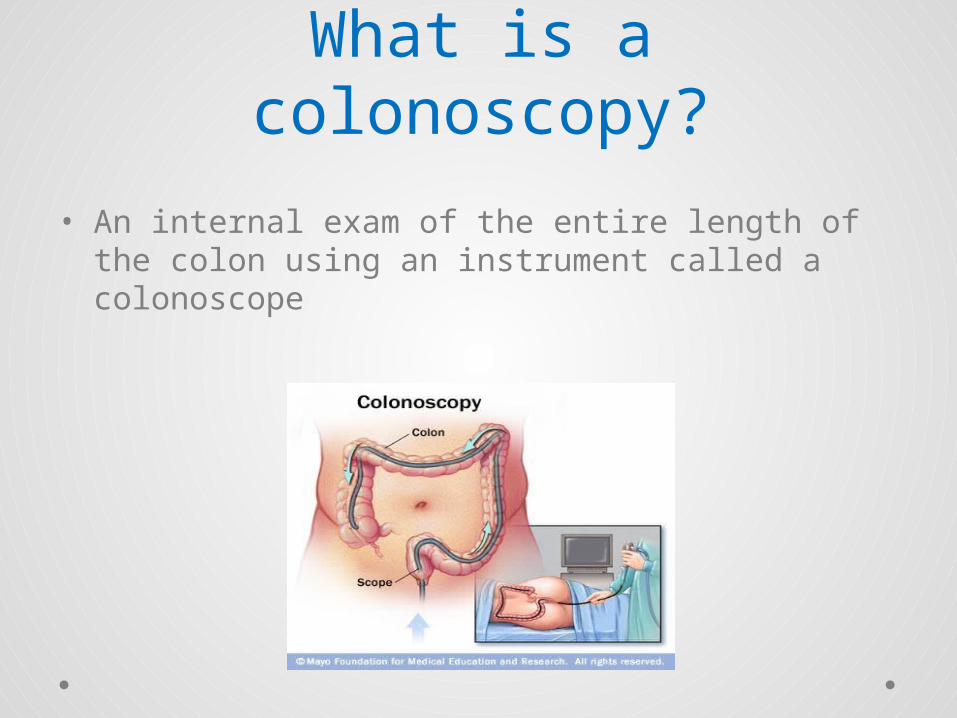
What is a colonoscopy?
• An internal exam of the entire length of the colon using an instrument called a colonoscope
What to expect: Colonoscopy
• The procedure takes about 30 – 60 minutes
• You will lie on your side with knees drawn up toward your chest
• Sedation is provided to the patient
• After being given the sedative, the colonoscope is inserted through the anus and gently advanced
The Colonoscopy
• Air will be inserted through the scope to provide a better view of the colon
• Suction may be used to remove any secretions in the colon
• Better views are seen during withdrawal of the colonoscope so a more careful examination is done during withdrawal of the scope
• Tissue samples and/or polyps may be taken with tiny forceps inserted through the scope
The Colonoscopy• You must have someone bring you to the exam.
You will not be able to drive because sedation is used
• Risk of complications is low but could includeo Tear in the colon/rectum wall (perforation)o Bleeding from the site where a tissue sample or polyp was removed
from the colon/rectum wallo Adverse event related to sedation (e.g. breathing problems)
What is a computed tomographic (CT)
colonography?• Procedure that uses low dose radiation CT
scanning to get a view of the inside of the colon • Also referred to as a virtual colonoscopy
Image from a CT colonography
http://www.massgeneral.org/imaging/services/procedure.aspx?id=2254
What to expect: CT Colonograpy?
• The procedure takes about 15 minutes
• You will be positioned on the CT exam table lying on your back
• A small tube will be inserted into the rectum to allow air to be pumped into the colon to help eliminate folds/wrinkles that may hide polyps
• The table will move through the scanner to obtain the images
What to expect: CT Colonograpy?
• You may experience a feeling of fullness or a need to pass gas
• Pain and discomfort are uncommon
• Risk of complications is low but may includeo Inflation of the colon could injure or perforate the bowelo Exposure to radiation
• You may be asked to follow up with a colonoscopy
What is capsule endoscopy?
• A noninvasive procedure that uses a wireless camera, small enough to fit inside a vitamin-sized disposable capsule, that you swallow
• Allows physician to view the entire colon to detect polyps without sedation or radiation
http://thefutureofthings.com/5306-the-pillcam-colon-video-capsule/
What to expect: Capsule Endoscopy
• A belt with sensors and a data recorder will be placed around your waisto Allows the capsule to wirelessly transmit images of your colon
• You will swallow the capsule with a glass of watero You will drink about 2 cups of bowel prep solution shortly after
• You are free to go about your regularly scheduled day
What to expect: Capsule Endoscopy
• Approximately 10 hours later you will return the belt to your doctor’s office
• The capsule usually naturally passes with a bowel movement within 24 hours o The capsule is disposable and does not need to be retrieved
• There should be no discomfort when swallowing the capsule, it traveling through your colon or eliminating it during a bowel movement
• You may be asked to follow up with a colonoscopy
What are Stool-based Screening Tests?
• Noninvasive, take home tests that look for signs of colorectal cancer in stool (feces)
• You collect stool specimens in the comfort of your home
• A positive result will require follow up with a colonoscopy
http://www.mountainside-medical.com/hemoccult-sensa-single-slide-tests.html
http://seekingalpha.com/article/1575652-exact-sciences-line-your-pockets-not-your-toilet-bowl-3-of-5
http://fightcolorectalcancer.org/research-treatment/medicare-now-covers-stool-dna-screening-test-cologuard/
What to expect: Fecal Occult Blood Test (FOBT)?• Looks for hidden (occult) blood in the stool
o Cannot determine if blood is from the colon or other parts of the digestive tract
o Not specific to human hemoglobin
• Must collect an actual stool sampleo Requires multiple samples from different bowel
movements
• Involves dietary restrictions • Positive test requires a colonoscopy• Must be done annually to provide adequate
screening
What to expect: Fecal Immunochemical Test
(FIT)?• Looks for hemoglobin protein found in red blood
cellso Specific for human hemoglobino Less likely to react to bleeding from upper digestive tract
• No dietary restrictions• No actual stool collected
o Brush stool surface or, if loose stool, stir the water around the stoolo Requires multiple samples from different bowel movements
• Positive test requires a colonoscopy• Must be completed annually to provide adequate
screening
What to expect: DNA Stool Test
• Looks for abnormal sections of DNA from cancer or polyps
• Tests for blood in the stool• Requires no dietary restrictions and one bowel
movement• Must handle and collect stool sample
according to the manufacturer’s instructions• Positive test requires a colonoscopy• Interval testing is every 3 years
How Do You Pay For Screening?
• Preventive services, to include CRC screening, are covered by Medicaid, Medicare and private insurance
• Check with your insurance to see if a co-payment is required if:o A polyp is removed during a colonoscopy o You have a colonoscopy following a positive stool testo You have a colonoscopy following a FSG, virtual colonoscopy
or PillCam
• CCSP will cover the cost of endoscopic screening (FSG and colonoscopy) for individuals uninsured or underinsured who meet further criteria through June 30, 2015.
Questions?