Upload
dinhhuong
View
221
Download
2
Embed Size (px)
Citation preview
NATIONAL CLINICAL PRACTICE GUIDELINE
Colorectal Cancer Screening
Clinical Practice Guideline
These guidelines are informational only. They are not intended or designed as a substitute for the reasonable exercise of independent clinical judgment by practitioners, considering each patients needs on an individual basis.
Guideline recommendations apply to populations of patients. Clinical judgment is necessary to design treatment plans for individual patients.
Colorectal Cancer
Guideline Development Team
Approved by the
National Guideline Directors
December 2010
Table of Contents Introduction................................................................................................................................... 1 Guideline Summary...................................................................................................................... 5 Rationale Statements .................................................................................................................... 7
1. Factors Associated with an Increased Risk of Colorectal Cancer in the General Population 72. Effectiveness of Colorectal Cancer Screening Tests ........................................................... 23
3. Frequency of Colorectal Cancer Screening ......................................................................... 60
4. Age to Begin and End Colorectal Cancer Screening ........................................................... 68
5. Screening in Adults at Increased Risk of Colorectal Cancer............................................... 71
Appendix A: Criteria for Grading the Evidence ..................................................................... 80 Appendix B: Supporting Documentation ................................................................................. 82
1. Factors Assoc. with an Increased Risk of Colorectal Cancer in the General Population .... 82
Problem Formulation 1 ..................................................................................................... 82
Search Strategy 1 .............................................................................................................. 83
Table 1. Excluded Studies................................................................................................. 85
Evidence Tables 1 ............................................................................................................. 86
2. Effectiveness of Colorectal Cancer Screening Tests ........................................................... 95
Problem Formulation 2 ..................................................................................................... 95
Search Strategy 2 .............................................................................................................. 96
Evidence Tables 2 ........................................................................................................... 101
3. Frequency of Colorectal Cancer Screening ....................................................................... 115
Problem Formulation 3 ................................................................................................... 115
Search Strategy 3 ............................................................................................................ 116
Evidence Tables 3 ........................................................................................................... 117
4. Ages at Which to Begin and End Colorectal Cancer Screening........................................ 120
Problem Formulation 4 ................................................................................................... 120
Search Strategy 4 ............................................................................................................ 121
Evidence Tables 4 ........................................................................................................... 122
5. Screening in Adults at Increased Risk for Colorectal Cancer............................................ 124
Problem Formulation 5 ................................................................................................... 124
Search Strategy 5 ............................................................................................................ 125
Evidence Tables 5 ........................................................................................................... 126
References.................................................................................................................................. 133
2010 Kaiser Permanente Medical Care Program i For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Introduction
Kaiser Permanentes National Guideline Program The National Guideline Program (NGP) supports the development of a core set of explicit, scientifically-based clinical practice guidelines, practice resources, and evidence synopses to assist Kaiser Permanente (KP) physicians, administrators, and other health care professionals in determining the most effective medical practices.
This core set of evidence-based resources will: Create Programwide economies of scale, Support ongoing performance improvement activities, Consistently provide high quality resources for use in care delivery tools and systems, and Increase KP regions abilities to leverage clinical guidelines to improve clinical outcomes.
Clinical practice guidance, based on scientific evidence, is essential for providing high quality care and continuously improving on it. Such guidance needs to be integrated into the electronic medical record and other decision support tools to be accessible to clinicians at the point of care. In addition, engaging our members in collaborative, shared decision-making conversations regarding their personal preferences is an essential component of patient-centered quality care. Furthermore, cost-effectiveness of various evidence-based interventions and resource limitations are important considerations. This involves addressing health problems in ways that maximize the health of the population given the available resources.
Who are the National Guideline Directors? The National Guideline Directors (NGD) are a group of experts and advocates of evidence-based medicine who provide direction and oversight to the National Guideline Program (NGP). In this role, the NGD selects and approves topics for evidence-based knowledge products, owns Kaiser Permanentes Common Methodology, and is responsible for quality assurance review. This group is composed of representatives from the Care Management Institute (CMI) and all eight regions.
What Is the Guideline Quality Committee? The Guideline Quality (GQ) Committee is a subcommittee of the NGD consisting of a group of evidence experts from various KP regions and CMI who review and approve all the National Guidelines. This review ensures that the processes used to develop guideline content have adhered to KP evidence-based methods and that the labels applied to clinical recommendations therein are accurate (e.g., evidence-based or consensus-based).
2010 Kaiser Permanente Medical Care Program 1 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
How Are Guidelines Developed? Guidelines are developed with the use of an evidence-based methodology and involve a systematic literature search, critical appraisal of the research design and statistical results of relevant studies, and grading of the sufficiency (quantity, quality, consistency, and relevancy) of the evidence for drawing conclusions. An evidence search includes literature published in peer-reviewed scientific journals, existing evidence-based guidelines, consensus-based statements from external professional societies and government health organizations, and clinical expert opinion of KP regional specialty groups. For additional information on evidence grading, see Appendix A.
To develop a or revise a guideline, CMI consultants work with a multidisciplinary Guideline Development Team (GDT). Each GDT consists of a core group of physicians, representing primary care and the specialties most affected by the guideline topic, and, as appropriate, other content experts from disciplines such as pharmacy, nursing, and health education. The members of a GDT are nominated by the respective National Guideline Directors to represent their regions. The GDT reviews the appraisal of the evidence and develops or revises clinical recommendations based on the current evidence. Each regional representative then presents the draft guideline recommendations to key experts and champions in their regions for critical review and support to improve the likelihood of implementation once the guideline is published.
How Often Are Guidelines Reviewed and Revised? To keep current with changing medical practices, all guidelines are reviewed, and, if appropriate, revised at least every two years. To develop the Colorectal Cancer Screening Guideline, released in December 2010, a multidisciplinary, interregional GDT first met in February 2010 to define the scope of the guideline. The Project Management Team then performed systematic reviews of the medical literature on each of the clinical questions identified by the GDT, assembled the evidence, and developed draft recommendations for review by the GDT. All of the recommendations and supporting evidence were reviewed in depth by the GDT in a series of meetings from September through November 2010. The GQ Committee reviewed and approved the guideline in December 2010. In 2010, a limited review was done, meaning that only Problem Formulations 1 and 2 were updated.
What Does It Mean for a Guideline to Be Evidence-Based? Each clinical recommendation within a guideline is labeled as evidence-based or consensus-based. A recommendation is considered evidence-based if there has been a systematic review of the evidence, the evidence is sufficient, and the recommendation is consistent with the evidence. A recommendation can also be considered evidence-based if there is insufficient evidence but either no particular intervention is recommended or options are recommended without favoring one of the options over others. A recommendation is considered consensus-based if there has been a systematic review of the evidence, the evidence is insufficient to support an evidence-based recommendation, and the GDT decides to make a consensus recommendation.
2010 Kaiser Permanente Medical Care Program 2 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
What Does It Mean for a Guideline to Be Approved and National? A recommendation that is consistent with the above policies is labeled as National Guideline Directors Approved. A National Guideline Directors Approved guideline for which at least 90% of the recommendations are approved by at least six of the eight KP regions is a "National Guideline." On the topics for which they exist, National Guidelines are the preferred evidence source for KP HealthConnect content.
Note: This guideline addresses colorectal cancer screening recommendations in the general, asymptomatic adult population seen in the primary care setting. It does not address screening and/or surveillance in adults with a personal history of colorectal cancer or inflammatory bowel disease, or a family history of hereditary colorectal cancer syndromes, such as familial adenomatous polyposis (FAP), Gardners syndrome, and hereditary nonpolyposis colon cancer (HNPCC or Lynch syndrome).
Contact Information: Theodore R. Levin, MD Marguerite A. Koster, MA, MFT Gladys I Tom, MS Director of Colorectal Cancer Practice Leader Senior Manager Screening TAG Unit Care Management Institute The Permanente Medical Group Southern California Permanente Kaiser Permanente (TPMG) Medical Group (SCPMG) Program Office Phone: (925) 295-6548 Phone: (626) 405-5462 Phone: (510) 271-2331 E-mail: [email protected] E-Mail: [email protected] Email: [email protected]
2010 Kaiser Permanente Medical Care Program 3 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Acknowledgements The Kaiser Permanente (KP) Colorectal Cancer Screening Clincal Practice Guidelines are the result of the extensive clinical expertise, collaborative efforts, and outstanding personal contributions of the following participants:
KP Colorectal Cancer Screening Guidelines Project Management Team Theodore R. Levin, MD Clinical Lead KP-Northern California Christy Pham, MPH Lead Analyst KP-Southern California Marguerite A. Koster, MA, MFT Team Leader, TAG Unit KP-Southern California Elizabeth Liles, MD EBM Methodologist KP-Northwest Gladys Tom Senior Manager, Knowledge Services KP-Program Office Tabitha Pousson Staff Assistant KP-Program Office
No members stated any conflicts of interest.
Colorectal Cancer Screening Guideline Development Team (GDT) Colorado Northwest Craig Robbins, MD EBM Director Elizabeth Liles, MD EBM MethodologisW Karin Kempe Director of Clinical Prevention .HYLQ-RQHV0'*DVWURHQWHURORJ\Tom Matzakos, MD Gastroenterology
OhioGeorgia William Schwab, MD Geriatrics Rodney Harris, MD Quality Management Ronald Adams, MD3K\VLFLDQ Hawaii Southern California Robert Decker, MD Gastroenterology Timothy Jenkins, MD Gastroenterology Northern California Stanford Gertler, MD Gastroenterology Theodore R. Levin, MD Gastroenterology
2010 Kaiser Permanente Medical Care Program 4 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Z176586Text BoxJames Cotter, MD - Medicine
Guideline Summary The following recommendations are composites of several component recommendations regarding the population to be screened, screening modality, and frequency of screening.
1. Colorectal cancer screening is strongly recommended for all asymptomatic, average-risk adults aged 50 to 75.
a. Any of the following tests and frequencies are acceptable options for colorectal cancer screening in asymptomatic, average-risk adults:*
High-sensitivity guaiac fecal occult blood test (gFOBT) every 1 to 2 years. Immunochemical fecal occult blood test (iFOBT/FIT) every 1 to 2 years , Flexible sigmoidoscopy at least every 10 years. Colonoscopy every 10 years. A combination of iFOBT/FIT every 1 to 2 years and flexible sigmoidoscopy every
10 years. A combination of high-sensitivity gFOBT every 1 to 2 years and flexible
sigmoidoscopy at least every 10 years.
b. The following additional screening tests are either less-preferred options or not recommended for screening. Although an adult who has had one of these tests is considered screened, follow-up screening using a preferred option is recommended.
Standard guaiac FOBT (gFOBT) Air contrast barium enema CT colonography (virtual colonoscopy) Fecal DNA testing
c. For those with no history of routine screening, discontinuation is recommended at age 80. The decision to discontinue screening should be based on physician judgement, patient preference, the increased risk of complications in older adults, and existing comorbidities.
* There is insufficient evidence to choose one screening test over another.
If a patient has had a normal colonoscopy within the last 10 years, there is insufficient evidence that supplemental gFOBT or iFOBT adds any incremental benefit.
FIT is a preferred option over standard gFOBT (Hemoccult II) due to its higher sensitivity and higher patient adherence rates.
Please note that fecal DNA testing, air contrast barium enema and CT colonography are not listed as appropriate screening tests in 2010 HEDIS specifications fro colorectal cancer screening.
2010 Kaiser Permanente Medical Care Program 5 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
2. Colonoscopy screening beginning at age 40, or 10 years younger than the earliest diagnosis in the first-degree relative, is recommended in adults with the following significant family history of colorectal cancer: One first-degree relative (parent, sibling, or offspring) with a diagnosis of colorectal
cancer at age 60 or younger. Two or more first-degree relatives diagnosed with colorectal cancer at any age.
3. For adults with a first-degree relative with a history of advanced adenomas ( 10 mm, with villous features, or high-grade dysplasia) presenting before age 60, colonoscopy screening beginning at age 50, at least every 10 years, may be the preferred option.*
4. For evaluation and follow-up of hereditary colorectal cancer syndromes and inflammatory bowel disease, referral to Gastroenterology is recommended.
5. For blacks/African-Americans, special efforts should be made to ensure that screening occurs using any of the accepted screening modalities.
* There is fair evidence that a family history of advanced adenomas presenting before age 60 is associated with an increased risk of adenomas or colorectal cancer.
Hereditary syndromes include familial adenomatous polyposis (FAP), Gardners syndrome, and hereditary nonpolyposis colon cancer (HNPCC or Lynch syndrome).
Observational national data demonstrate an increased risk of colorectal cancer and a more advanced stage of disease at diagnosis among blacks/African-Americans than among whites. It is not clear whether this disparity is due to differences in the biological behavior of colorectal cancer in blacks/African-Americans, differences in socioeconomic status, or differences in access to care.
2010 Kaiser Permanente Medical Care Program 6 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Rationale Statements
1. Factors Associated with an Increased Risk of
Colorectal Cancer in the General Population 1.A. A significant family history is associated with an increased risk of colorectal cancer.
(See Problem Formulation #5 for screening recommendations and specific definition of family history.) Evidence-based: A
1.B. Advancing age is associated with an increased risk of colorectal cancer.* Evidence-based: B
1.C. There is fair evidence that blacks/African-Americans are at increased risk for colorectal cancer compared with whites. Evidence-based: C
1.D. There is fair evidence that a history of advanced adenomas ( 10 mm, with villous features, or high-grade dysplasia) presenting before age 60 in a first-degree relative is associated with an increased risk of colorectal cancer. Evidence-based: C
1.E. There is fair evidence for the association of male gender with an increased risk of colorectal cancer. Evidence-based: B
Rationale: 2010 Update Search Results, Methodology and Key Terminology A broad literature search was conducted incorporating terms for gender, race, family history, and terms to signify adenomas. Terms to address the risk imposed by lifestyle factors, including obesity or tobacco use were not included. Two large population-based cohort studies were identified (Brenner 2010(1) and Brenner 2007(2)) which evaluated the association of gender with incidence of CRC. SEER data summaries of CRC incidence and mortality for black/African-American men and women in comparison to white men and women were also updated. No new studies met inclusion criteria to address the risk factors of race, family history of adenomas or family history of CRC.
For the current update, we considered inclusion and exclusion criteria, and optimal study design to address the various risk factors of interest (i.e., gender, age, family history, and race). Large registry or electronic database cohort studies (e.g., the German registry as noted below) are likely to provide the highest levels of evidence demonstrating association of age or gender with CRC incidence and mortality; age and gender can be easily ascertained from electronic data. Systematic review or meta-analysis of smaller studies are expected to provide the best estimates of association of family history or race with CRC incidence or mortality, (e.g., Butterworth, et al.); survey data or interview data are needed to assess family history and race status. Inclusion and exclusion criteria for this problem formulation are below.
* Indirect evidence from analyses using cancer registry, Medicare, and other surveillance data indicates that the risk of cancer and advanced colonic neoplasms increases with age.
2010 Kaiser Permanente Medical Care Program 7 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Problem Formulation Population Study Design Setting Outcomes Exclusions
PF1 Factors associated with increased risk for CRC incidence
Age 40 y; average risk
Systematic evidence review; meta-analysis; RCT/CCT; registries, large database observational studies cohort studies, cross-sectional studies
Any CRC incidence, as associated with sex, age, race or family history of CRC or adenomas.
Studies examining the association of risk factors with adenomas, advanced adenomas or polyps were excluded.
Many studies examine the association of age, gender, race and family history with the endpoint of prevalence of adenomas or advanced adenomas (which is a composite endpoint including adenomas with certain histologic features, plus CRC). These studies were excluded because the natural history of advanced adenomas is unknown. Some adenomas progress to cancer, but many of them either do not progress, or regress.
Evidence Summary There is fair evidence that male gender is associated with an increased risk of colorectal cancer from two large population-based cohort studies (Brenner 2010(1) and Brenner 2007(2)), upon which this part of the evidence summary is based. The more recent of these two studies, which offers a rigorous analysis of data from 2,185,153 screening colonoscopies, indicates that men are estimated to reach the same prevalence of CRC 3.4 years earlier than women. Results from a second study (Brenner 2007) indicate that men reach the same level of cumulative mortality from CRC about four to six years sooner than women. There is moderate certainty, based on these two studies, that there is a moderate increase in risk for CRC among men compared to women of the same age.
In this report, an update of SEER data is included, which continues to demonstrate higher CRC incidence in black/African-American men compared to men of other races, for every age group older than 40. Similarly, the incidence of CRC in black/African-American women is higher than that of women of other races, for every age group older than 40. It is unclear whether the earlier CRC incidence and mortality in black/African-American men and women may be related to lower screening rates in this population, differences in socioeconomic status, differences in cancer biology among black/African-American individuals compared with white individuals, or other contributing variables. SEER data do not account for these factors. There is therefore low to moderate certainty that there is a moderate increase in risk for CRC among black/African-American individuals compared to white individuals.
2010 Kaiser Permanente Medical Care Program 8 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Risk of Colorectal Cancer Associated with Gender In a recent national prospective cohort, Brenner et al. (2010)(1) estimated the association of age, gender and birth cohort with prevalence of advanced colorectal neoplasms (AN) and colorectal cancer (CRC) among 2,185,153 participants aged 55 to 75 years who have had a screening colonoscopy. This cohort analysis examined data from a prospective registry for a German population-based screening colonoscopy program, for 2003 to 2007. Only primary screening colonoscopies conducted by gastroenterologists or experienced surgeons were included in the registry. The authors conducted several separate analyses, to determine the independent effects of age, birth cohort and sex on prevalence of CRC and advanced neoplasia, but they did these analyses using two general approaches: (1) They utilized a cross-sectional analysis with a log-binomial model to estimate relative prevalence of CRC and any advanced neoplasm for men compared with women, with sex and age as independent variables and (2) They utilized a log linear regression model incorporating birth cohort (year of birth), age, and gender as independent variables. From both models, they estimated adjusted risk-advancement periods, defined as the number of years earlier the prevalence of CRC or advanced neoplasia was reached in men compared to women. The authors applied the birth cohort analysis in addition to the cross-sectional analysis to highlight and control for the confounder effects from year of birth and age gradient. They provided several estimates of relative prevalence in their results, considering five year age intervals, ten year age intervals, birth cohorts (year of birth separated by two year intervals), and other metrics.
Results: Overall, 56% of patients were female, and women were particularly overrepresented in the younger age groups (Age 55 to 59: 60%, age 60 to 64: 57%, age 65 to 69: 54%, age 70 to 74: 52%). 17,196 (0.8%) participants had CRC and 152,429 (7%) had AN, which reflects the usual prevalence of these endpoints in an average-risk population. The authors contrasted findings between the two approaches to data analysis; log binomial analysis incorporating sex and age, and log-linear regression incorporating sex, age and birth cohort. In cross-sectional analysis, the prevalence of CRC and AN, stratified by age, was up to two-fold higher in men compared to women within each five year age group. Controlling for birth cohort in the second analysis showed that age gradient strongly increased in analyses of CRC and AN prevalence. In cross-sectional analysis (with age and sex as variables), risk-advancement periods for men compared with women were estimated at 8.4 and 16.1 years for CRC and any advanced neoplasm, respectively. After additionally controlling for birth cohort in log-linear regression, risk-advancement periods for men compared with women were 3.4 and 6.9 years for CRC and any advanced neoplasm, respectively. Therefore, men were estimated to reach equivalent CRC and advanced neoplasm prevalence 3.4 and 6.9 years earlier than women. Risk-advancement periods by decade of birth cohorts were estimated to be 5.9 and 5.7 years, respectively. Race information was not disclosed in the study; therefore, generalizability of results to mixed-race population similar to the US and the possible disproportionate effect of race are unclear. In addition, the authors did not discuss controlling for other potentially confounding factors such as socioeconomic status or BMI.
2010 Kaiser Permanente Medical Care Program 9 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
In an analysis of cancer registry data from the United States and national mortality statistics from different countries, Brenner et al.(2007) compared cumulative ten-year incidence and mortality for CRC between men and women. Age and sex specific data on CRC incidence and mortality were obtained for the years 2000 to 2003 in the US from the National Cancer Institutes Surveillance, Epidemiology and End Results (SEER) Program. In addition, national age- and sex-specific mortality data referring to the year 2001 were obtained for 11 large countries from different parts of the world: Australia, Asia (Russia, Japan), Europe (France, Germany, Italy, Poland, Spain, United Kingdom), and North America (Canada, US), utilizing the World Health Organisation (WHO) mortality database. Starting from the calculated levels of ten-year cumulative incidence among men at ages 50, 55, and 60 (determined from the SEER database), the authors determined at what ages the same levels of ten-year cumulative incidence were observed among women. Analogous calculations of risk advancement periods were then carried out for ten-year cumulative mortality on the basis of the national vital statistics data for other countries.
Results: The SEER incidence database included 74,111 men and 72,290 women diagnosed with CRC in 2000 to 2003. Among men, cumulative incidence in the subsequent 10 years increased from 0.8% at age 50 to 1.2% at age 55 and 1.9% at age 60. Among women, comparable levels of ten-year cumulative incidence were reached at ages 54, 60 and 66 only, i.e., four, five, and six years later, respectively. Analogous calculations for ten-year cumulative CRC mortality in 2001 in 11 large countries from different parts of the world showed very similar age differences between women and men, despite some major variation in the overall levels of CRC mortality. The ten-year cumulative mortality seen among men at age 50 was reached by women between ages 54 and 56 in nine out of 11 countries (median: 55 years); slightly lower and higher ages were only seen for the Russian Federation (52 years), and Japan (57 years), respectively. The ten-year cumulative mortality seen among men at age 55 was reached by women between ages 60 and 62 in the same nine countries (median: 61 years). The ten-year cumulative mortality seen among men at age 60 was reached by women between ages 66 and 68 in nine countries (median: 67 years) and at ages 69 and 70 in Spain and Japan, respectively.
The SEER Cancer Registry reported the age-adjusted incidence rate of colorectal cancer from 2000 to 2005 stratified by gender and race or ethnicity (Evidence Tables 1.5 and 1.6). Men had a higher incidence of cancer then women for all races combined (61.7 cases per 100,000 men vs. 45.3 cases per 100,000 women), and the relative incidence in men was 1.36 times higher than in women.
Risk of Colorectal Cancer Associated with Race An update of SEER data (see Evidence Table 1.9) indicates that From 2000 to 2007, there was an overall decrease in the incidence of invasive colorectal cancer across race and gender, from 53.20 (52.44 to 53.97) to 44.22 (43.56 to 44.88) per 100,000. However blacks/African-Americans and males in particular, continue to have a much higher incidence than whites. Among males in 2007, the incidence for black/African-American males was 11.56 per 100,000 greater than white males: 61.16 (57.01 to 65.51) vs. 49.60 (48.42 to 50.80) per 100,000 men, for black/African-American men and white men, respectively.
2010 Kaiser Permanente Medical Care Program 10 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Although the incidence of colorectal cancer is much lower in women, there was a similar gap in the incidence rates between black/African-American and white women: In 2007, 50.11 (47.04 to 53.32) vs. 37.91(36.99 to 38.85) per 100,000 women, for black/African-American and white women, respectively. Comparative incidence rates when grouped by five year age range cohorts similarly indicate that incidence of colorectal cancer is highest in black/African-American men at all five year age intervals, when compared to men of other races (see Evidence Table 1.10). The same is true for black/African-American women at all five year age intervals. However, the actual risk-advancement period for individuals based on race alone is difficult to estimate from these data. For example, the incidence for white men aged 50 to 54 (59.97 per 100,000) is lower than for black/African-American men aged 50 to 54 (79.91 per 100,000), but higher than for black/African-American men aged 45 to 49 (36.82 per 100,000). As well, these data do not take screening rates and socioeconomic status into account as potential confounders.
Risk of Colorectal Cancer Associated with a Family History of Colorectal Cancer A comprehensive meta-analysis by Butterworth et al.(2006)(3) on the relative and absolute risk of colorectal cancer for individuals with a family history was identified. This meta-analysis included 57 papers containing data from 60 studies, 43 of which were case-control or cross-sectional studies and 17 of which were cohort studies.
Butterworth et al. (2006)(3) estimated that the probability that a person under the age of 40 would develop colorectal cancer over the next ten years was less than 1%, regardless of family history. The estimated probability that a person 40 years of age or older would develop colorectal cancer before the age of 75 was 2.5%, for the general population. They found a relative risk of 2.24 for persons with a first-degree relative with colorectal cancer, which represents a doubling of the risk of developing colorectal cancer (an absolute risk of 4.7%). Having multiple affected first-degree relatives increased an individuals risk even further; a relative risk of 3.97 (95% CI: 2.60 to 6.06), based on nine studies (absolute risk of 9.6%). The relative risk for those with an affected relative under the age of 50 was 3.55 (95% CI: 1.84 to 6.83), based on four studies. They did not find evidence that having an affected second-degree relative conferred increased risk for developing colorectal cancer. (see Figure 1.1, Evidence Tables 1.1 and 1.2 for details.)
Case-control, cohort, and other observational studies have indicated that adults with a family history of colorectal cancer are at a higher risk for developing colorectal cancer. This body of evidence is difficult to interpret as a whole, because the populations, comparison groups, ages at which the relatives were diagnosed, and cut-points used in the analyses vary widely among the studies. In addition, selection bias is a problem, because few studies have made the comparison between a group of asymptomatic adults with first-degree relatives with colorectal cancer and a group of asymptomatic average-risk adults (i.e., those with and without a family history, which more closely represents the general population). Nearly half of the studies are subject to recall bias, because the diagnoses in relatives were not verified. Referral bias is also of concern, especially in studies of colorectal cancer risk in relatives of patients with adenoma, some of which included cases referred for colonoscopy due to a family history of colorectal cancer. Finally, many trials did not control for confounding factors other than age and sex, which may account for differences between adults with a positive family history and those at average risk for colorectal cancer.
2010 Kaiser Permanente Medical Care Program 11 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
http:37.91(36.99
Risk of Colorectal Cancer Associated with Colorectal Cancer in a First-Degree Relative The Butterworth et al. (2006)(3) meta-analysis found a relative risk of 2.24 for persons with a first-degree relative with colorectal cancer, which represents a doubling of the risk of developing colorectal cancer. It was the consensus of the GDT to use a threshold of 2.0 to evaluate risk factors that might warrant screening recommendations different from those for persons at average risk.
Butterworth et al. (2006)(3) evaluated 47 studies of the risk of developing colorectal cancer in persons who had at least one first-degree relative with a previous diagnosis of colorectal cancer. All studies showed a positive association, with relative risk estimates ranging from 1.29 to 10.0, although in most studies the relative risk was between 1.5 and 4.0. The pooled relative risk estimate was 2.11 (95% CI: 2.02 to 2.22) under a fixed-effects model and 2.24 (95% CI: 2.06 to 2.43) under a random-effects model (p = 0.022). A significant difference in relative risk estimates was seen between parents and siblings of affected individuals (p = 0.005), with sibling history carrying a greater risk than parental history. There was no significant difference between relative risk estimates for cancers in the colon or rectum, contrary to the results of individual studies. Please see Figure 1.1 for a forest plot of the relative risks and random-effects model estimate. Inspection of the funnel plot (data not included) suggested the presence of publication bias.
Risk of colorectal cancer associated with colorectal cancer in multiple first-degree relatives Having multiple affected first-degree relatives increased an individuals risk even further.
A meta-analysis of nine studies found that having at least two affected first-degree relatives led
to a relative risk of 3.97 (95% CI: 2.60 to 6.06).
Risk of colorectal cancer associated with colorectal cancer in a first-degree relative < 50 years of age Four studies in Butterworth et al. (2006)(3) had relative risk estimates stratified by the age of the affected relative (above or below 50 years). The relative risk for those with an affected relative under the age of 50 was 3.55 (95% CI: 1.84 to 6.83), and the estimate for those with an affected relative at or above 50 years of age was 2.18 (95% CI: 1.56 to 3.04). There was no significant difference between age categories (p = 0.19). Stratification according to the age of the individual at risk was available in 12 studies, which showed that the relative risk was significantly greater (p = 0.003) for younger relatives of affected individuals. If a subject was under the age of 50 and had an affected relative diagnosed with colorectal cancer at any age, then the relative risk of colorectal cancer was 3.17 (95% CI: 2.37 to 4.25). For subjects aged 50 and older, the relative risk of colorectal cancer if a family member was previously diagnosed was 1.90 (95% CI: 1.59 to 2.28).
2010 Kaiser Permanente Medical Care Program 12 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
A previous meta-analysis by Johns and Houlston (2001)(4) suggested a possible cut-point of risk associated with having a relative diagnosed with colorectal cancer under age 60, but other studies suggest that risk increases when the age at diagnosis of the index case is lower. A well-designed case-control study by St. John et al. (1993)(5) found that a diagnosis of colorectal cancer at age 55 in the index case confers a relative risk of colorectal cancer that is 3.5 times higher than that for an average person. The study found having an affected first-degree relative who was 55 or older at diagnosis increased the relative risk of colorectal cancer, but the risk was not significantly higher than that of an average person.
Risk of Colorectal Cancer Associated with Colorectal Cancer in a Second-Degree Relative According to a meta-analysis by Butterworth et al. (2006)(3) of five cross-sectional and cohort studies, having an affected second-degree relative conferred a relative risk of 1.73 (95% CI: 1.02 to 2.94). After the individual studies used to determine the pooled risk had been reviewed, however, the body of evidence was considered insufficient. This is because two studies (Andrieu et al., 2003; Jenkins et al., 2002) did not find a statistically significant effect. One study (Bhatia et al., 1999) used relatives of probands whose median age at diagnosis was under 21 years (an extremely rare diagnosis); one study (Mitchell et al., 2004) had a primary outcome of accuracy of reporting among relatives of probands, rather than actual risk assessment; and one study was unobtainable due to a publication date of March 1960.
Risk of Colorectal Cancer Associated with Adenoma in a First-Degree Relative There is fair evidence that a history of advanced adenomas (adenomas that are 10 mm, with villous features, or high-grade dysplasia) presenting before age 60 in a first-degree relative is associated with an increased risk of colorectal cancer.
A case-control study by Cottet et al. (2007)(6) assessed the risk of colorectal adenomas and cancers using colonoscopic screening in first-degree relatives of patients with large adenomas. Colonoscopies were offered to first-degree relatives of 306 index cases with large adenomas of 10 mm if they were alive, aged 40 to 75 years, and could be contacted by the index case. Among them, 168 were examined and matched for age, sex, and geographic area with two controls (n = 307). Although the index cases had large adenomas (and no diagnosed cancers at the time of the study), the results reported for first-degree relatives included all types of colorectal neoplasia, including cancer. The study found that the prevalence rates of large adenomas or cancers were 8.4% and 4.2% in relatives and controls, respectively. Five cases of colorectal cancer (3%) were identified in the relative group (n = 168) versus three cases (1%) in the matched control group (n = 307) (OR = 3.90, 95% CI: 0.89 to 17.01, p = 0.07) (see Evidence Table 1.3).
2010 Kaiser Permanente Medical Care Program 13 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
The prevalence of adenomas was higher in men than in women among both relatives (24.0% vs. 16.1%) and controls (17.3% vs. 14.9%). The odds ratios associated with a history of large adenomas in relatives were 2.27 (95% CI: 1.01 to 5.09, p = 0.046) for cancers or large adenomas, 1.21 (95% CI: 0.68 to 2.15, p = 0.52) for small adenomas, and 1.56 (95% CI: 0.96 to 2.53, p = 0.075) for all colorectal neoplasias. The researchers also found that the risk of large adenomas and cancers was higher if the relative was younger than 60 years of age (OR = 3.82, 95% CI: 0.92 to 15.87, p = 0.07) or if the index case had large distal adenomas (OR = 3.14, 95% CI: 1.27 to 7.73, p = 0.01). The authors concluded that first-degree relatives of patients with large adenomas had an increased risk of both colorectal cancer and large adenomas (whereas this is probably not the case for relatives of index cases with small adenomas). The strength of the relationship varied according to the age and gender of the index case and the size and location of the adenoma in the index case. Limitations of the study include the lack of information about the completeness of colonoscopy in 20% of relatives (who were generally examined outside study centers) and a low participation rate for first-degree relatives.
Of nine studies in Johns and Houlston (2001)(4) reporting the risk of colorectal cancer associated with adenoma in a first-degree relative, eight found an increased risk (pooled RR = 1.99; 95% CI: 1.55 to 2.55). The authors suggested that there was strong evidence from two studies (Winawer et al., 1996;(7) Ahsan et al., 1998(8)) that the risk of colorectal cancer in first-degree relatives increases as the age of the affected relative at diagnosis of the adenoma decreases. Ahsan et al. (1998)(8)found that first-degree relatives of patients diagnosed with adenoma at age 50 or younger had four times the risk of colorectal cancer (RR = 4.36; 95% CI: 2.24 to 8.81) as first-degree relatives of patients who were 60 or older at diagnosis. Winawer et al. (1996)(7) found a similar relationship between siblings of patients diagnosed with an adenoma at age 60 or younger and siblings of patients diagnosed with adenoma at more than 60 years of age (RR = 2.59; 95% CI: 1.46 to 4.58).
In one screening-based cross-sectional study published after the Johns and Houlston analysis, Nakama et al. (2002)(9) evaluated the risk of colorectal cancer in 44,821 subjects who underwent a consecutive two-day immunochemical fecal occult blood test (iFOBT). A self-completed questionnaire on family history of colorectal adenomatous polyps was used to divide subjects into two groups: one with and one without a family history of adenomatous polyps. Of those with a family history, 8.5% had a positive iFOBT, compared with 4.8% of subjects without a family history. The positive predictive value (PPV) of iFOBT for colorectal cancer was 6.8% in the group with a family history vs. 2.4% in the group with no family history. Statistically significant differences between the groups in iFOBT positivity rate (p < 0.01) and PPV for colorectal cancer (p < 0.05) were also reported.
The results from Cottet et al. (2007)(6) indicate that the risk of finding large adenomas or cancers in first-degree relatives was higher when the index case presented with a large adenoma in the distal colorectum (OR = 3.14, 95% CI: 1.27 to 7.73, p = 0.01) or had an advanced adenoma (OR = 2.31, 95% CI: 0.88 to 6.04, p = 0.09).
2010 Kaiser Permanente Medical Care Program 14 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Lynch et al. (2003)(10) studied 3,121 patients undergoing screening colonoscopy as part of the VA Cooperative Colonoscopy Study Group 380 to determine whether colonic neoplasia found on screening was related to a history of colorectal cancer in the patients parents or siblings. Family history was determined by participant self-report. The authors also analyzed data on the characteristics of the detected adenomas (size, number, histology, and degree of dysplasia), and participants were grouped according to the most advanced lesion. The authors found that participants with adenomas were more likely to have a family history of colorectal cancer than were participants without adenomas (OR = 1.36; 95% CI: 1.09 to 1.70). When the most advanced lesion was a small (< 1 cm) tubular adenoma, there was only a slight increase in the odds of colorectal cancer in a family member (OR = 1.26; 95% CI: 0.99 to 1.61). The presence of an advanced adenoma, however, was associated with a higher probability of colorectal cancer in a family member (OR = 1.62; 95% CI: 1.16 to 2.26). The study reported no association between younger age at diagnosis of adenoma and an increased prevalence of colorectal cancer in family members.
Risk of Colorectal Cancer Associated with Increasing Age Observational evidence from analyses of Medicare, surveillance, and cancer registry data indicates that the risk of cancer and advanced colonic neoplasms increases with age. SEER Cancer Registry data (1973 to 2003) show that the incidence of colorectal cancer increases beginning at about age 50 and continues to increase through age 80 (see Figure 4.1).
According to SEER data and with the reference category set at age 50 to 59, the relative incidence of colorectal cancer nearly doubles in the 60 to 64 age category (see Evidence Table 1.4). For the group 85 years of age or older, the relative incidence is over six times that of the 50 to 59 age group. Although SEER data are useful for identifying increased risk with age, the relative incidence numbers are crude analyses from registry data, and the results should be interpreted with caution. In addition, one of the difficulties in interpreting SEER data is that the SEER population includes adults with and without risk factors for colorectal cancer. Consequently, it is not possible to determine the degree to which age is confounded with a family history of or genetic susceptibility to colorectal cancer.
Two studies have reported an association between age and high-risk adenomas:
Levin et al. (1999)(11) found that, among 2,972 people screened with colonoscopy, the strongest predictor of advanced proximal neoplasia was the presence of villous architecture in the distal polyp. For those patients who did not have a distal villous or tubulovillous adenoma, an age of 67 or older was the best predictor of advanced proximal neoplasia; more important than the number of distal tubular adenomas or a family history of colorectal cancer.
2010 Kaiser Permanente Medical Care Program 15 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Lieberman et al. (2000)(12) found a statistically significant trend toward an increased prevalence of advanced proximal neoplasia with age (p < 0.001). The prevalence of advanced neoplasia increased from 5.7% in those aged 50 to 59 to 12.9% in patients aged 60 to 69, and 13.3% in patients aged 70 to 79. Is the increasing prevalence of advanced neoplasia (presumably advanced proximal neoplasia) by age group out of proportion to the increasing incidence of colorectal cancer by age group? The approximate doubling between the age groups 50 to 59 and 60 to 69 seems about the same as the increase in Evidence Table 1.3, but there is no increase in the age group 70 to 79 to match the SEER data. This might mean that the increase in advanced proximal neoplasia with age is not as rapid as the increase in total colorectal cancer.
No other trials on age as a risk factor for colorectal cancer were identified. On the basis of the grading scheme described in the Appendix, there is evidence that increasing age is a risk factor for colorectal cancer.
Risk of Colorectal Cancer Based on Environmental Factors The evidence does not show a strong association between obesity and increased colorectal cancer incidence. The inconsistent measures for obesity in the meta-analysis below preclude a clear association of obesity with increased risk for colorectal cancer. The evidence also does not show a strong association between alcohol intake and increased colorectal cancer incidence. The major methodologic limitation of studies of alcohol intake is that self-report is unreliable.
Obesity A meta-analysis by Dai et al. (2007)(13) evaluated the association between obesity and colorectal cancer risk in 6,458 colorectal cancer cases among 1,058,883 participants from 15 cohort studies. The researchers also assessed whether the potential association differs by gender and cancer subsites. Since previous studies had not standardized the definition, obesity here was defined as body mass index (BMI) in kg/m2 or waist-to-hip ratio or waist circumference (per the World Health Organization). Because waist circumference and WHR (waist-to-hip ratio) varied across the studies, the researchers combined different outcomes between the smallest waist or WHR quantile and the largest waist or WHR quantile in studies using relative risks in meta-analysis of random effects. Overweight was defined as BMI 25.0 to 29.9, obesity as BMI 30, and normal as BMI 18.5 to 24.9). Heterogeneity for each pooled estimate was also assessed.
Compared with those in the normal BMI range, the pooled RR for colorectal cancer of overweight and obese men was 1.37 (95% CI: 1.21 to 1.56), with no significant heterogeneity (p = 0.42). The pooled RR for colorectal cancer of overweight and obese women was 1.07 (95% CI: 0.97 to 1.18), with no significant heterogeneity (p = 0.29).
Compared with those in the lowest quantile for waist circumference the pooled RR for colon cancer was 1.68 (95% CI: 1.36 to 2.08) for men and 1.48 (95% CI: 1.19 to 1.84) for women, with no significant heterogeneity (p = 0.31). The pooled RR for rectal cancer was 1.26 for men (95% CI: 0.90 to 1.77, p = 0.95) and 1.23 for women (95% CI: 0.81 to 1.86), with the highest quantile of waist circumference (p = 0.95).
2010 Kaiser Permanente Medical Care Program 16 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Similarly, compared with those in the lowest quantile, the pooled RR for colon cancer was 1.91 for men (95% CI: 1.46 to 2.49, p = 0.23) with the highest quantile of WHR and 1.49 for women (95% CI: 1.23 to 1.81), with no significant heterogeneity (p = 0.76). The pooled RR for rectal cancer was 1.93 for men (95% CI: 1.19 to 3.13) and 1.20 for women (95% CI: 0.81 to 1.78) with the highest quantile of WHR.
In assessing the relation between obesity and the risk of colorectal cancer in different subsites, the pooled RR for proximal colon cancer was 1.14 (95% CI: 0.88 to 1.47) for the overweight, with no significant heterogeneity (p = 0.39), and 1.41 (95% CI: 0.66 to 3.01) for the obese, with significant heterogeneity (p = 0.04), when compared with those in the normal range. Compared with those in the lowest quantile, the pooled RR for proximal colon cancer was 2.05 (95% CI: 1.23 to 3.41) for those in the highest quantile of waist circumference, with no significant heterogeneity (p = 0.63), and 1.66 (95% CI: 0.69 to 3.99) for those in the highest quantile of WHR. Compared with those in the normal range, the pooled RR for distal colon cancer was 1.38 (95% CI: 1.02 to 1.87) for the overweight, with no significant heterogeneity (p = 0.59), and 1.23 (95% CI: 0.80 to 1.90) for the obese, with significant heterogeneity (p = 0.76). Compared with those in the lowest quantile, the pooled RR for proximal colon cancer was 1.86 (95% CI: 1.05 to 3.30) for those in the highest quantile of waist circumference, with no significant heterogeneity (p = 0.80), and 1.79 (95% CI: 0.82 to 3.90) for those in the highest quantile of WHR.
Alcohol Intake A meta-analysis of prospective cohort studies conducted by Moskal et al. (2007)(14) evaluated the relationship between alcohol intake and colorectal cancer. Sixteen prospective cohort studies including more than 6,300 patients with colorectal cancer were appraised. For both men and women, the RR was 1.53 (95% CI: 0.87 to 2.69); for men, the RR was 1.73 (95% CI: 1.00 to 2.98, p = 0.02) and for women, 0.88 (95% CI: 0.61 to 1.27, p = 0.44). Two studies reported a significantly increased risk of colorectal cancer only among men, while the remaining studies did not report significant associations. Overall, alcohol intake was positively but not significantly associated with colorectal cancer (RR = 1.34; 95% CI: 0.92 to 1.96), with heterogeneous results across cohorts (p = 0.002). High alcohol intake was significantly associated with colorectal cancer in men but not in women. The results of the studies included in this analysis were heterogeneous, and this trend may be attributable to the geographic area in which the study was conducted. For instance, alcohol intake levels ranged from 154 to 462 g/week in Asian studies, from 15 to 159 g/week in American studies, and from 194 to 492 g/week in European studies.
2010 Kaiser Permanente Medical Care Program 17 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
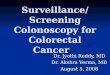
Figure 1.1: Forest plot of the relative risk associated with having at least one first-degree relative with colorectal cancer. Data from Butterworth et al., 2006.(3, 3)
Study Woolf 1958 Lovett 1976 Martinex 1979 Duncan 1982 Maire 1984 Pickle 1984 Rozen 1987 Bonelli 1988 Ponz de Leon 1989 Fisher 1989 Kune 1989 Weber-Stadel 1990 Yang 1992 Le Vecchia 1992 Centonze 1993 St John 1993 Nelson 1994 Fuchs 1994 Goldgar 1994 Kotake 1995 Hall 1996 Freedman 1996 Hall (b) 1996 Le Marchand 1996 Carstensen 1996 Karner-Hanus 1997 Ghadirian 1998 Negri 1998 Kerber 1998 Bhatia 1999 Yoo 1999 Newcomb 1999 Poole 1999 Coogan (b) 2000 Coogan 2000 Sandhu 2001 Seow 2002 Levi 2002 Boutron 2002 Jenkins 2002 Johns 2002 Dora 2003 Minami 2003 Keku 2003 Andrieu 2003 Erlinger 2004 Mitchell 2004 Overall
Relative Risk (95% CI) 3.53 (1.42-8.70) 3.52 (1.87-6.63) 2.53 (1.06-6.05) 9.33 (0.48-182.97) 6.34 (2.30-17.48) 5.89 (2.63-13.20) 1.93 (1.11-3.35) 2.36 (1.54-3.61) 7.50 (2.28-24.68) 2.50 (0.79-7.91) 2.13 (1.53-2.96) 1.80 (1.40-2.31) 2.28 (1.37-3.80) 2.03 (1.52-2.71) 5.87 (1.60-21.52) 2.10 (1.43-3.07) 1.29 (0.90-1.85) 1.72 (1.35-2.20) 2.55 (2.11-3.08) 2.04 (1.23-3.38) 5.21 (1.61-16.88) 3.12 (1.77-5.51) 2.27 (1.42-3.62) 2.50 (1.82-3.44) 2.02 (1.81-2.25) 4.61 (2.40-8.84) 1.65 (1.08-2.53) 2.80 (2.24-3.50) 1.77 (1.47-2.13) 10.0 (0.16-626.05) 2.58 (1.77-3.76) 2.07 (1.60-2.68) 1.60 (1.32-1.93) 1.90 (1.48-2.43) 2.00 (1.65-2.42) 2.32 (1.43-3.76) 6.70 (2.40-18.70) 3.23 (1.47-7.09) 1.90 (1.07-3.39) 3.20 (2.16-4.74) 3.54 (2.62-4.79) 2.07 (1.25-3.44) 1.64 (1.06-2.53) 2.40 (1.83-3.15) 1.71 (1.36-2.15) 1.56 (0.61-4.00) 2.51 (1.39-4.54) 2.24 (2.06-2.43)
Relative Risk 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
2010 Kaiser Permanente Medical Care Program 18 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
http:2.06-2.43http:1.39-4.54http:0.61-4.00http:1.36-2.15http:1.83-3.15http:1.06-2.53http:1.25-3.44http:2.62-4.79http:2.16-4.74http:1.07-3.39http:1.47-7.09http:2.40-18.70http:1.43-3.76http:1.65-2.42http:1.48-2.43http:1.32-1.93http:1.60-2.68http:1.77-3.76http:0.16-626.05http:1.47-2.13http:2.24-3.50http:1.08-2.53http:2.40-8.84http:1.81-2.25http:1.82-3.44http:1.42-3.62http:1.77-5.51http:1.61-16.88http:1.23-3.38http:2.11-3.08http:1.35-2.20http:0.90-1.85http:1.43-3.07http:1.60-21.52http:1.52-2.71http:1.37-3.80http:1.40-2.31http:1.53-2.96http:0.79-7.91http:2.28-24.68http:1.54-3.61http:1.11-3.35http:2.63-13.20http:2.30-17.48http:0.48-182.97http:1.06-6.05http:1.87-6.63http:1.42-8.70
Figure 1.2: Forest plot of the relative risk of being overweight and/or obese and colorectal cancer in men (A) and women (B). Data from Dai et al. (2007).
2010 Kaiser Permanente Medical Care Program 19 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Figure 1.3: Forest plot of the relative risk of waist circumference and colorectal cancer (A), and waist-to-hip ratio and colorectal cancer risk (B). Data from Dai et al. (2007).
2010 Kaiser Permanente Medical Care Program 20 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Figure 1.4: Forest plot of the relative risk of developing colon cancer with alcohol intake. Data from Moskal et al. (2007).
2010 Kaiser Permanente Medical Care Program 21 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Figure 1.5: Forest plot of the relative risk of developing rectal cancer with alcohol intake. Data from Moskal et al. (2007).
2010 Kaiser Permanente Medical Care Program 22 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
2. Effectiveness of Colorectal Cancer Screening Tests 2.A. Colorectal cancer screening is strongly recommended for all asymptomatic, average-risk
adults. Evidence-based: A 2.B. Any of the following tests are acceptable options for colorectal cancer screening in
asymptomatic, average-risk adults:*
High-sensitivity guaiac fecal occult blood test (gFOBT). Consensus-based Immunochemical fecal occult blood test (iFOBT/FIT). Consensus-based Flexible sigmoidoscopy. Evidence-based: A Colonoscopy. Consensus-based A combination of high-sensitivity guaiac FOBT and flexible sigmoidoscopy.
Consensus-based A combination of Immunochemical fecal occult blood test (iFOBT/FIT) and
flexible sigmoidoscopy. Consensus-based
2.C. The following additional screening tests are either less-preferred options or not recommended for screening. However, an adult who has had one of these tests is considered screened. Follow-up screening using a preferred option is recommended. An annual standard guaiac fecal occult blood test (gFOBT) is a less-preferred
option. Consensus-based Air contrast barium enema is not recommended as a screening strategy for average-
risk adults. Consensus-based Virtual colonoscopy is not recommended as a screening strategy for average-risk
adults.* Consensus-based Fecal DNA is not recommended as a screening strategy for average-risk adults.
Consensus-based
NOTE: For fecal blood tests, inform patients of the potential risks associated with false-
positive test and false-negative test results, as well as the need for prompt follow-up of a
positive test result. For flexible sigmoidoscopy, inform patients that the test has a small risk
of complications and is not a complete examination of the entire colon.
* There is insufficient evidence to choose one screening test over another. If a patient has had a normal colonoscopy within the last 10 years, there is insufficient evidence that
supplemental fecal testing adds any incremental benefit. Even though there is sufficient evidence in support of this screening modality, it is not a preferred option due to
its low sensitivity and low compliance rates. Please note that fecal DNA testing and virtual colonoscopy are not listed as appropriate screening tests in
2010 HEDIS specifications for colorectal cancer screening, and therefore regions may choose to screen members with other appropriate tests.
2010 Kaiser Permanente Medical Care Program 23 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Evidence Grade* Evidence for Recommendation 2A: Good. Evidence for Recommendation 2B: Fair.
Rationale: 2010 Update The current review recognizes the high level of evidence supporting flexible sigmoidoscopy for CRC screening. The 32% reduction in CRC-related mortality for one-time completion of flexible sigmoidoscopy is comparable to the 33% reduction in CRC-related mortality observed in a randomized trial of standard gFOBT (when screened annually for several consecutive years). Hesitation to recommend flexible sigmoidoscopy as the favored method of screening stems from consensus discussion around the decreasing patient interest in flexible sigmoidoscopy across the KP regions. This update newly addresses the topic of CRC screening test adherence with a systematic review; results indicate that adherence to one-time completion of one-sample FIT is higher than adherence to one-time completion of three-sample gFOBT, flexible sigmoidoscopy or colonoscopy. Because of the different types and levels of evidence included in this review and the different benefits and risks of each type of test, the recommendations continue to provide broad options for screening, allowing flexibility in specific choices at the regional level. Because of the widespread use of FIT throughout the regions, specific brand-name search terms in the literature searches to cover every FDA approved, CLIA waived type of fecal test currently available were utilized. Lastly, because we had systematically searched for and located studies demonstrating screening test effectiveness, we also systematically searched for studies demonstrating the harms, specifically of colonoscopy, flexible sigmoidoscopy and CT colonography.
Search Results and Key Terminology The focus of this review included the effectiveness, harms/adverse events, test performance characteristics, and adherence to (compliance with) the CRC screening tests noted above (colonoscopy, flexible sigmoidoscopy, high-sensitivity gFOBT, FIT, or a combination of fecal testing and flexible sigmoidoscopy). Double air contrast barium enema was not included in the 2010 HEDIS list of appropriate screening tests, and so the GDT agreed to exclude it from the evidence update at this time. While the original intent of this review was to assess the effectiveness of screening, it became clear that the outcomes of interest, as stated in the problem formulation, were broad, ranging from CRC morbidity and mortality to test performance characteristics, harms of testing, and test adherence. Because of the complexity of the literature about colorectal cancer screening and the range of tests available, the GDT believes it was important to systematically review test performance, harm, and adherence by adding literature search terms (and in some cases, extra searches); please refer to the search strategies in the appendix for additional information.
* The criteria for grading the strength of the evidence as either good, fair, or insufficient adheres to the KP National Guideline Programs Policies and Procedures documents entitled Label and Language of Recommendations and KP System for Grading the Strength of a Body of Evidence, which are located in Appendix A.
2010 Kaiser Permanente Medical Care Program 24 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
The effectiveness of CRC screening tests was addressed in four new studies [two for FS (Atkins 2010, Hoff 2009), and two for colonoscopy (Kahi 2009, Baxter 2009)]. Harms or adverse events due to screening were examined in four new studies [Rabeneck 2008, Crispin 2009, Bokemeyer 2009 and Ko 2010] and three previous studies [Levin 2006, Korman 2003, Rathgaber 2006]. Test performance characteristics among the different tests were described in three new studies [Hundt 2009, Sohn 2005, Park 2010]. Adherence to test completion was addressed in 13 new studies [Hol 2010, Hol 2009, Federici 2005, Levi 2010, Lisi 2010, Berry 1997, Cole 2003, MACS 2006, Hoffman 2010, Segnan 2005, Segnan 2007, Verne 1998, Brevinge 1997] and three previously included studies [Van Rossum 2008, Federici 2006, Rasmussen 1999]. .
Evidence Summary Effectiveness There is direct, longitudinal evidence from a good quality RCT demonstrating the effectiveness of screening flexible sigmoidoscopy, when high (70%) adherence is achieved. CRC-related mortality, but not all-cause mortality was reduced 32%, CRC incidence was reduced 23%, and rectosigmoidal CRC incidence was reduced 36% after a mean of 11 years of screening. There is direct evidence from four RCTs and a meta-analysis of these RCTs demonstrating the effectiveness of utilizing standard gFOBT for screening. CRC-related mortality, but not all-cause mortality is reduced 13 to 21% (pooled estimate: RR = 0.85; 95% CI: 0.78 to 0.92), after 8 to 13 years in biennial gFOBT screening programs. CRC-related mortality, but not all-cause mortality was reduced 33% in a single trial of annual screening with standard gFOBT. Indirect evidence for the effectiveness of standard gFOBT plus sigmoidoscopy comes from a single nonrandomized trial (Winawer 1993) indicating a potential 43% reduction in CRC-mortality after nine years from combined testing compared with rigid sigmoidoscopy alone, although differences were not statistically significant. There is indirect evidence for the effectiveness of colonoscopy, based on two fair quality case-control studies (one of them recent) and a fair quality prospective cohort study (recent). Both case control studies showed a lower odds of having had prior colonoscopy (OR = 0.63 (95% CI: 0.57 to 0.69; P < 0.001 in the larger study) among those dying of CRC. In the more recent case-control study, patients who had died from right-sided CRC had similar prevalence of complete colonoscopy to controls [(OR = 0.99 (95% CI: 0.86 to 1.14)]. The retrospective cohort study compared the incidence of CRC in a predominantly white, middle to upper SES population who had screening colonoscopy to that of a historical reference cohort with a broader demographic range of participants; this comparison resulted in a CRC incidence ratio of 0.52 (95% CI: 0.22 to 0.82). The USPSTF has previously cited the National Polyp Study as evidence for colonoscopy effectiveness, however the GDT has previously excluded the study due to it being done in a population of high-risk patients with polyps. There are no studies demonstrating the effectiveness of FIT, high-sensitivity gFOBT, fecal DNA testing, or CT colonography for CRC screening.
2010 Kaiser Permanente Medical Care Program 25 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Harm Based on seven large cohort studies of colonoscopy complications, the rate of perforation from colonoscopy (1.6 to 9 perforations per 10,000 procedures) is similar to or higher than that from CT colonography (0.9 to 6.0 per 10,000 procedures) and is higher than that from flexible sigmoidoscopy (0.46 per 10,000 procedures). A recent large retrospective cohort study of Canadian administrative and hospital data (N = 97,091) estimated a mortality rate due to colonoscopy of 0.74 per 10,000 procedures. Other included studies reported no deaths or one death, or did not appear to evaluate the rate of death as a measurable outcome. CT colonography has additional potential harms of extra-colonic findings (in 5 to 23% of individuals) that may lead to invasive procedures or repeated CT scans. The long-term effects of the radiation exposure from CT colonography are also unknown. These harms are the primary reason for the GDT previously recommending against CT colonography for screening. The potential harm from fecal testing (FIT, fecal DNA testing, or high-sensitivity gFOBT) is considered proportionate to the number of unnecessary colonoscopies that each type of test would generate, estimated from test sensitivity and specificity.
Test performance characteristics Studies comparing CTC and colonoscopy indicate that colonoscopy is similar to or superior to CTC for detecting adenomas 6 mm in size, and superior to CTC for detecting adenomas 6 mm in size. Comparative estimates of test performance characteristics for flexible sigmoidoscopy are based upon simulated data, but indicate that FS is significantly less sensitive for advanced neoplasia throughout the colon than CTC or colonoscopy, due to its limited reach. All three of these procedures can miss cases of CRC (e.g., the study of N = 452 participants by Johnson 2007, in which colonoscopy missed four out of five cancers), and none of them serves as a perfect reference standard.
Based on previous studies and on three recent studies of fecal immunochemical testing (FIT), three FITs (Monohaem, OC-Hemodia, and OC-Micro) have sufficient evidence to recommend them, are FDA approved (CLIA-waived) and are currently available in the United States. Monohaem is more sensitive for CRC than is Hemoccult II, and requires only one sample. OC-Hemodia and OC-Micro, utilizing three-samples, both demonstrate superior sensitivity and comparable specificity to both Hemoccult II and high sensitivity guaiac FOBT (Hemoccult Sensa), which also require three-samples. OC-Micro is the only FIT with automated development that is FDA approved and available in the United States. Single-sample OC-Micro is used already in several Kaiser regions, and is demonstrated to have superior test performance over gFOBT (Hemoccult II) when the positivity threshold of 100 ng/ml is used. The studies reporting test performance characteristics for this FIT are small or done in populations that are difficult to compare to an average-risk American population. Best estimates for sensitivity of this FIT are 25 to 70% for CRC, and approximately 32% for advanced neoplasia, with a single use of a single-sample test. Estimated positive predictive value of this FIT for advanced neoplasia is 40%. Single-sample OC-Micro is an acceptable substitute for standard gFOBT (Hemoccult II) currently.
2010 Kaiser Permanente Medical Care Program 26 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Adherence To Organized Outreach Programs The current update includes a systematic review of adherence because of the effect and complexity of patient participation for CRC screening; a test can only be effective when it is completed accordingly.
A review of randomized trials comparing screening completion rates for different CRC screening tests produced sixteen new studies. See Evidence Table 2.7 for a summary of studies comparing completion rates for different fecal tests. There is evidence that mailed invitations with a one-sample fecal test enclosed, with mailed return of the test, can achieve a high single-test completion rate (~60%) within some settings. Two recent large randomized controlled trials of screening outreach programs in the Netherlands utilizing mailed fecal tests demonstrate one-time adherence to one-sample OC-Micro FIT of approximately 60% (12% higher than for three-sample gFOBT). Each trial utilized Internet resources or a help desk phone number to answer patient questions throughout the trial duration. A third trial that required participants to pick up either of the same two tests and deliver it for processing, and that did not utilize Internet or telephone resources for patients achieved 20 to 25% lower overall fecal test completion rates in both arms of the trial. Cumulative adherence to annual, year-after-year FIT testing is unknown. Summary of cumulative adherence to biennial screening with gFOBT was beyond the scope of this review. See Evidence Table 2.8 for a summary of studies comparing completion rates for gFOBT only, FS only, and for a combined protocol (gFOBT + FS). Three of the studies assessing completion rates for combined gFOBT + FS screening achieved a 40% completion rate of the combined gFOBT plus FS. All three of these studies occurred in Europe in the early or mid-1990s. As well, it is unclear from the studies which outreach approach for the FS part of the combined screening would most likely result in FS completion, without decreasing overall screening rates (i.e., discouraging patients from completing any test). Studies that directly compared completion of fecal testing to completion of flexible sigmoidoscopy alone were also examined (see Evidence Table 2.9). In the three studies that utilized mailed fecal tests and the same number of reminders in each arm, completion of fecal testing was 10 to 17% higher than completion of FS. Completion rates for a fecal test that had to be picked up by the patient were similar to completion of FS in two studies that utilized up to three reminders to complete FS and up to one reminder to complete the fecal test. Lastly, three studies were found comparing completion of fecal testing to completion of colonoscopy (see Evidence Table 2.10). In all three studies, the rate of completion of fecal testing was significantly higher (6 to 17%) than the rate of completion of colonoscopy, even when extra reminder efforts were made in the colonoscopy arm.
2010 Kaiser Permanente Medical Care Program 27 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
Screening Effectiveness Summary
Problem Formulation Population Study Design Setting
Outcomes of interest Other
PF2a Effectiveness: Impact of screening on incidence or mortality .
Age 40 y; average risk, recruited from primary care or primary care comparable population.
Systematic evidence review; RCT; cluster RCT; well-designed CCT, cohort, and case control studies .
Primary care or other setting with primary care comparable population.
Mortality (all-cause or CRC-specific); Incidence of CRC.
Studies with advanced neoplasia as the outcome were excluded.
Flexible Sigmoidoscopy (refer to Evidence Tables 2.1 and 2.2 for details) In this review, direct evidence emerged for the effectiveness of screening flexible sigmoidoscopy, utilizing a specific protocol. In a high-quality RCT (N = 170,432) CRC-related mortality, but not all-cause mortality was reduced 32% (HR = 0.69 (95% CI: 0.59 to 0.80), p < 0.0001), after a mean of 11 years of screening (Atkin et al. 2010(15)). CRC at all sites had 23% lower incidence in the screening group compared to control [HR = 0.77 (95% CI: 0.7 to 0.84), p < 0.001), and rectosigmoidal cancer had a 36% lower incidence [HR = 0.64 (95% CI: 0.57 to 0.72), p < 0.001)] in the screening group also. These results provide information about the effectiveness of flexible sigmoidoscopy screening when only patients with high-risk polyps within the reach of sigmoidoscopy (about 5% of patients) received referral for colonoscopy, and when adherence to the test is high (70%). A smaller RCT (N = 55,736) of flexible sigmoidoscopy using broader referral criteria (which resulted in a 19% referral rate to colonoscopy) showed no significant difference between groups in all-cause mortality, CRC-related mortality, rectosigmoid cancer-related mortality, or cumulative incidence of CRC after six to seven years of follow-up (Hoff et al., 2009(16)). A longer period of follow-up is needed to determine the long-term effects of flexible sigmoidoscopy when using this protocol (and in a study this size), given the high prevalence of screen-detected cancers in the screening group.
Four additional studies provide observational evidence for the effectiveness of flexible sigmoidoscopy: The 2002 USPSTF review reported a reduction in CRC incidence with flexible
sigmoidoscopy (FS) screening (RR = 0.20, 95% CI: 0.03 to 0.95) and a nonsignificant,
but possible, reduction in CRC mortality based on the results of a small CCT of FS.
[Thiis-Evensen 1999]
One high-quality, case-control study of rigid sigmoidoscopy found nine percent of those
dying from CRC within 20 cm of the anus had had a previous sigmoidoscopy, while 24 percent of persons with CRC within 20 cm of the anus who did not die of this cancer had received the test. The reduction in distal CRC mortality (adjusted OR = 0.41, 95% CI: 0.25 to 0.69 was not seen in those dying of more proximal colonic cancers (adjusted OR = 0.96), suggesting that screening reduced risk for death from CRC located in the sections of the colon reached by the sigmoidoscope. [Selby 1992]
2010 Kaiser Permanente Medical Care Program 28 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
A second case-control study of flexible sigmoidoscopy detailed in the USPSTF 2002review found risk of death from colorectal cancer was reduced among individuals having
had a single examination by screening sigmoidoscopy (OR = 0.21, 95% CI: 0.08 to 0.52),
compared with the risk for those who never had one. [Newcomb 1992]
A more recent case-control study of flexible sigmoidoscopy found that incidence of distal
colorectal cancer was reduced among individuals who had a single examination by screening sigmoidoscopy (OR = 0.24, 95% CI: 0.17 to 0.33) compared to those who never had one. [Newcomb 2003]
Guaiac Fecal Occult Blood Testing (refer to Evidence Table 2.1 for details) As has been discussed in previous updates, there is direct evidence from longitudinal results of RCTs supporting the effectiveness of screening with the guaiac fecal occult blood test (gFOBT) alone, annually or biennially. CRC-related mortality, but not all-cause mortality is reduced 13 to 21% (pooled estimate: RR = 0.85, 95% CI: 0.78 to 0.92), after 8 to 13 years in biennial gFOBT screening programs (Hewitson 2007). Higher mortality reductions have been seen in the single annual screening trial (33%) (Mandel 1999).
Combined gFOBT plus Flexible Sigmoidoscopy (refer to Evidence Table 2.2 for details) The 2008 USPSTF review provides an additional summary of prior evidence for the combination of gFOBT and FS for screening:
Evidence to support gFOBT combined with sigmoidoscopy came from a nonrandomized trial suggesting a 43 percent reduction in CRC-mortality after nine years from combined testing compared with rigid sigmoidoscopy alone, although differences were not statistically significant. [Winawer 1993]
Colonoscopy (refer to Evidence Table 2.2 for details) A recent case-control study (Baxter et al. 2009(17)) of Canadian adults aged 52 to 90 (N = 61,752) showed that patients who had died from CRC were less likely than controls to have undergone complete colonoscopy (OR = 0.63, 95% CI: 0.57 to 0.69; P < 0.001). Patients who had died from left-sided (rectosigmoidal) CRC were also significantly less likely than controls to have undergone complete colonoscopy (OR = 0.33, 95% CI: 0.28 to 0.39), however those who had died from right-sided CRC had similar prevalence of complete colonoscopy to controls (OR = 0.99, 95% CI: 0.86 to 1.14). A major limitation of this study is that the indication for colonoscopy was unknown in each case, and adjustments to the data for inferring the indication may have significantly biased results.
2010 Kaiser Permanente Medical Care Program 29 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
A prospective cohort study (Kahi et al. (2009)(17)) of 715 colonoscopy-screened medical and dental professionals (and their spouses) reported on the incidence of CRC and CRC-related death in comparison to that of a historical cohort (calculated age- and sex-specific rates from the SEER database). The approximate follow-up period ranged from 14 to 18 years. A standardized incidence ratio of 0.52 (95% CI: 0.22 to 0.82) indicated a relative risk reduction for CRC of 48% in the study cohort. In the study cohort, three patients died from CRC (95% CI: 0 to 9), compared to nine deaths calculated from the SEER data, yielding a standardized mortality ratio of 0.35 that does not reach statistical significance (95% CI: 0.0 to 1.06). A major limitation of this study lies in the limited size and diversity of the patient population, which consisted of predominantly Caucasian volunteers of a mid- to high educational level, which may have had a lower overall CRC risk than the population of the SEER database.
The 2008 USPSTF review provides an additional summary of prior evidence for the effectiveness of screening colonoscopy:.
The [2002 USPSTF] review reported one case-control study, which showed lower odds of having had a previous colonoscopy in those dying from CRC (OR = 0.43, 95% CI: 0.30 to 0.73), compared to controls without CRC. [Muller 1995]
CT Colonography No studies in the present update or in prior updates demonstrate the effectiveness of screening with CT colonography.
Fecal Immunochemical Testing No studies in the present update or in prior updates demonstrate the effectiveness of screening with fecal immunochemical testing.
High-sensitivity Guaiac Fecal Occult Blood Testing No studies in the present update or in prior updates demonstrate the effectiveness of screening with high-sensitivity guaiac fecal occult blood testing.
Fecal DNA Testing No studies in the present update or in prior updates demonstrate the effectiveness of screening with fecal DNA testing.
2010 Kaiser Permanente Medical Care Program 30 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
New Study Details Sigmoidoscopy A recent study by Atkin et al. 2010(15) randomized 170,432 adult volunteers aged 55 to 64 years to a no-screening control group (n = 113,195) or one-time flexible sigmoidoscopy (n = 57,237) and reported on CRC mortality and incidence after a mean of 11 years. Randomization was stratified by trial center (14 UK centers participated: 11 in England, two in Wales, one in Scotland), general practice within center, and household type (household was indicated by self-report on questionnaire: single man, woman, couples, other). Sample size was calculated to give 90% power to detect a 20% difference between the intervention and control groups in incidence of CRC at 10 years and mortality at 15 years since randomization, assuming a conservative attendance rate for flexible sigmoidoscopy of 55%. The study cohort (N = 170,432) consisted of those who were (1) among the 88% of general practices who agreed to participate and (2) among the 53% of individuals originally contacted within those practices, who indicated that they would likely attend the screening, (3) among those who did not meet exclusion criteria, and (4) who were not among the 16,014 excluded prior to randomization because they were calculated to be in excess (presumably of what was needed for a sufficiently powered study). The mean age was 60 + 2.9 years and there were 51% women in both the intervention and control groups. Participants underwent FS with polypectomy for small (< 1 cm) polyps and referral for colonoscopy if they had high-risk polyps (1 cm or larger; three or more adenomas; tubulovillous or villous histology, severe dysplasia or malignant disease found within the small polyp; or 20 or more hyperplastic polyps above the distal rectum).
Results: Of those in the study randomized to the intervention group (N = 57,237), 40,621 (71%) attended the flexible sigmoidoscopy. Of these, 5% (n = 2,131) received referral to colonoscopy, of whom 96% (n = 2,051) completed the colonoscopy. Intention-to-screen analysis showed a 23% lower incidence of CRC at all sites in the intervention group compared to control (HR = 0.77, 95% CI: 0.7 to 0.84), p < 0.001), while per-protocol analysis showed a 33% lower incidence of CRC at all sites in the intervention group compared to control (HR = 0.67, 95% CI: 0.60 to 0.76)]. The incidence of distal colon cancer (defined as occurring in the sigmoid colon and rectum) was 36% lower in the intervention group in the intent-to-screen analysis (HR = 0.64, 95% CI: 0.57 to 0.72), p < 0.001)], and 50% lower in the intervention group in the per-protocol analysis (HR = 0.50, 95% CI: 0.42 to 0.59). Mortality from colorectal cancer as certified by the Office for National Statistics was reduced by 32% in the intervention group in the intention-to-screen analysis (HR = 0.69, 95% CI: 0.59 to 0.80), p < 0.0001], and by 43% in the intervention group in the per-protocol analysis (HR = 0.56, 95% CI: 0.45 to 0.69). By both intent-to-screen analysis and by per-protocol analysis, there was no significant difference between the intervention and control groups in (1) Proximal colorectal cancer incidence, (2) Mortality due to non-colorectal cancer causes, or in (3) Cumulative all-cause mortality, at the end of the follow-up period. The effectiveness of flexible sigmoidoscopy is well-demonstrated in this population that achieved high adherence; high adherence is due in part to the select population. In contrast, in the U.S., where colonoscopy is a more frequently recommended test, adherence to FS may be lower and more resources required in order to reproduce the high patient participation observed in this study.
2010 Kaiser Permanente Medical Care Program 31 For use within Kaiser Permanente only. 12/10 National Colorectal Cancer Screening Clinical Practice Guideline
A seven-year follow-up study (Hoff et al., 2009(16)) of the randomized trial of FS conducted by the Norwegian Colorectal Cancer Prevention Study Group (NORCCAP, N = 55,736) was also identified. This trial compared CRC incidence and mortality in men and women aged 55 to 64 years, randomized to one of three groups: (1) FS screening (n = 6,915) (2) FS screening preceded by one round of fecal immunochemical (FIT) testing with the FIT Flexsure OBT (n = 6,908), or (3) No screening (n = 41,913). Authors reported cumulative incidence of CRC after seven years of follow-up and cumulative mortality after six years of follow-up. Participants received referral for colonoscopy if the FIT had a positive result or if the FS revealed a polyp > 10 mm in diameter, histologically verified adenoma irrespective of size, or carcinoma. Investigators estimated samples size based on (1) estimated adherence of 70%, (2) 50% coverage of the colorectal mucosa by flexible sigmoidoscopy, and (3) a power of 90% to detect a 30% reduction in CRC incidence after five years at a 5% significance level. Screening participants were drawn randomly from the national population registry for two counties in Norway, and the control group consistent of age-eligible individuals within these same areas and also from epidemiologically similar populations with similar access to routine endoscopic services. No organized CRC screening program utilizing any modality exists in Norway. Therefore, these investigators had the opportunity to compare flexible sigmoidoscopy with a control group that often went unscreened. A personal letter of invitation was mailed six to seven weeks prior to a suggested day for an appointment free of charge at the local screening center, with a single reminder letter mailed three weeks before the day of the appointment to non-responders.
Results: Both groups had s