Embed Size (px)
Citation preview

2 VIEWS & REVIEWS
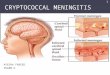
Commenting on cryptococca) meningitis therapy
Based on their comparative study of oral fluconazole and IV amphotericin, Dr MS Saag and colleagues from the US concluded that oral fluconazole could be considered as an effective alternative in the initial treatment of acute cryptococcal meningitis complicating AIDS [see 800141683]. This conclusion prompted the following queries:
Would higher fluconazole doses yield a higher success rate? Drs B Dupont and G Pialoux from France achieved negative CSF cultures in 50 and 87% of patients treated with fluconazole 200 and 400mg, respectively, for 45-60 days indicating a dose-response effect '. Based on these data they believe that a comparative trial of higher doses of amphotericin B and fluconazole would produce a greater success rate. In reply, Dr Saag and colleagues report no .difference in outcomes among patients whose fluconazole dosage was increased to 400 mg/day compared with those patients whose dosage remained at 200 mg/day.
Could treatment outcome be improved by the uninterrupted use of amphotericin B rather than turning to new agents? The use of amphotericin B is frequently limited by the onset of adverse effects, particularly nephrotoxicity, states Dr JP Tolins from the US1. The need for discontinuation of amphotericin B or alternateday dosing may be avoided if strategies for preventing the development of nephrotoxicity, such as salt-loading or concomitant administration of calcium antagonists. are employed. Before replacing amphotericin B with potentially less efficacious drugs. '," it is importallt that the effects of these IIew strategies be evaluated ill well-desiglled c1illical trials' concludes Dr Tonlis.
Is baseline CSF pressure of prognostic value? According to Drs F Menichetti and C Tascini from italy, fluconazole may be inadequate primary therapy in patients with high CSF opening pressures because of the slow sterilisation of CSF3. Dr Saag and colleagues agree that elevated CSF pressure at baseline may predict a risk for failure of antifungal therapy. They have addressed this issue in their current ongoing trial which examines aggressive initial antifungal therapy for AIDS-associated cryptococcal meningitis4. While oral fluconazole is a viable alternative for patients with normal mental status at presentation, neither fluconazole nor amphotericin B appear to be optimal for patients at high risk of dying (predominantly those with altered mental status at baseline). Therefore, the trial assesses the potential benefits of ~ 2 weeks of aggressive initial therapy with high dose amphotericin B ± flucytosine in these patients. 1. Dupont B. et al. Amphotericin versus fluconazole in cryptococcal meningitis. New England Journal of Medicine 326: 1568. 4 Jun 1992 2. Tolins JP. Amphotericin versus fluconazole in cryptococcal meningitis. New England Journal of Medicine 326: 1567·1568.4 Jun
20 Jun 1992 INPHARMA ®
1992 3. Menichetti F. et al. Amphotericin versus fluconazole in cryptococcal meningitis. New England Journal of Medicine 326: 1568. 4 Jun 19924. Saag MS. et al. Amphotericin versus fluconazole in cryptococcal meningitis. Reply. New England Journal of Medicine 326: 1568·1569. 4 Jun 1992 ""
ISSN 0156·2703/92/0620·0004/$1.00/0 © Adis International lid