Embed Size (px)
Citation preview

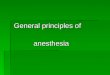
ICD-9-CMADOPTED FORHOSPITAL USE
ICD-9-CMADOPTED FOR
PHYSICIAN USE
WORLD HEALTHORGANIZATIONADOPTS ICD-10
HIPAA LEGISLATIONINTERRUPTS US ICD-10 ADOPTION
CMS PROPOSED RULE TO ADOPT ICD-10 OCT 2011
CMS FINAL RULETO ADOPT ICD-10
OCT 2013
CMS DELAYSIMPLEMENTATION
ONE YEAR
CONGRESS DELAYSIMPLEMENTATION
ONE YEAR
IMPLEMENTATIONOCTOBER 1
1979
1988
1994
1996
2008
2009
2013 2015
2014
ICD-10 HISTORY
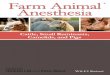
CODE STRUCTURE
ICD-9-CM CODE FORMAT
X X X X X
CATEGORY ETIOLOGY,ANATOMIC SITE,MANIFESTATION
3 TO 5 CHARACTERSFIRST DIGIT IS NUMERIC OR E OR VALL OTHER DIGITS ARE NUMERIC
ICD-10-CM CODE FORMAT
X X X
CATEGORY
X X X
ETIOLOGY,ANATOMIC SITE,MANIFESTATION
X
EXTENSION
1 TO 7 CHARACTERSFIRST DIGIT IS ALPHAALL DIGITS EXCEPT SECOND ALPHA OR NUMERIC
NUMBER OF CODES
ICD-9DIAGNOSIS CODES
ICD-10DIAGNOSIS CODES
69,00014,000
PERFORMANCE THAT MATTERS
Common Anesthesia Diagnoses: ICD-9 to ICD-10 Mapping
AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611

Anesthesia Diagnoses: ICD-9 to ICD-10 Mapping
Introduction ................................................................................................. 1
Most Common ICD-9 Anesthesia Codes and ICD-10 Documentation Issues............ 3
Ulcers ......................................................................................................... 4
Glaucoma ................................................................................................... 6
Tears and Ruptures .................................................................................... 7
Neoplasm of Breast .................................................................................... 8
Fractures .................................................................................................... 9

1
Introduction
ICD-10 CM coding for anesthesia needs increased levels of specificity that should be included in
physician documentation. This document provides an overview of the top diagnosis codes for
anesthesia and the critical changes in ICD-10 that may impact coding and claim submission.
The table on the next page shows 3 categories of changes that impact documentation:
1) Diagnoses that require specificity that must be included before claims can be submitted
for payment. If a coder receives documentation without the specificity, it must be
returned to the provider for additional information. This category is highlighted in
red.
2) Diagnoses that request specificity, but “unspecified” or “other” codes are available as a
default. Because the intention of ICD-10 is to capture additional detail, it is unclear
whether payers will accept “unspecified” codes or if they will be denied or delayed.
Therefore, we encourage providers to include the detail in their documentation; the claim
will only be returned to the provider in the event of a denial from the payer. This category
is highlighted in yellow.
3) Conditions which generally provide a straightforward 1-to-1 transition from ICD-9 to
ICD-10. No change to the documentation is required. This category is highlighted in
green.
Following the table is an overview of top anesthesia codes and the documentation issues present
with ICD-10.
Subsequent pages highlight the top diagnoses and the specific documentation requirements and
issues for converting from ICD-9 to ICD-10.

2
ICD10 Change Condition Documentation Requirements
Critical: Must be Included in
Documentation
Encounter/Episode of Care
Episode of care must be included for injuries, poisonings and other conditions. Designations include initial, subsequent, sequela. There is no "not otherwise specified" or "unspecified" option; the code must include the episode of care to be complete.
Fracture Type
Additional details related to fracture type must be included, such as whether the fracture is open or closed, as well as details about the healing phase whether healing is routine or with complications such as delayed healing, nonunion or malunion. Open fractures should include the Gustillo open fracture classification. There is no "not otherwise specified" option.
Important: Codes provide "Unspecified"
option but lack of specificity may
result in delayed or denied
payments by payor.
Site Specificity
Greater level of specificity required, including: * Specific area of limb (calf, ankle, etc) * Specific quadrant of breast or area of chest wall Unspecified codes are available.
Laterality Identify right/left/bilateral/unilateral limb, body location when available. Unspecified codes are available.
Primary/Post Traumatic/ Secondary
Conditions such as osteoarthritis, urethritis, and other UTI diagnoses should include whether it is primary, secondary, or post-traumatic.
Type of Tear Type of tear needed. Examples for cartilage/meniscus (bucket-handle, peripheral, complex) or rotator cuff (incomplete/complete). "Unspecified" and "Other" codes are available.
Patient History Neoplasm screening should include applicable patient history resulting in need for service
Artery and Chest wall specificity
With acute myocardial infarction, chest wall (anterior, inferior) and artery (circumflex coronary, descending coronary artery) should be included. The codes allow for "other sites" and "unspecified site."
Ulcer Stage Pressure ulcers should be categorized based on stages from National Pressure Ulcer Advisory Panel (NPUAP) stages 1-4.
Identification of pregnancy term
Issues related to pregnancy should identify the trimester.
Disease Type Type and origin of the disease should be included for diagnoses such as hypertension, COPD, and hyperlipedemia.
Acute V Chronic Conditions such as respiratory or digestive orders should be designated as "acute" or "chronic"
1-to-1 conversion from ICD9 to ICD10;
no additional documentation
required
Normal or C-section birth/delivery
1-to-1 conversion; no additional documentation required
Calculus of gallbladder or kidney
1-to-1 conversion; no additional documentation required

3
Most Common ICD-9 Anesthesia Codes and ICD-10 Documentation Issues
ICD-9
Code ICD-9 Description
ICD-10 Documentation Issues
Laterality
Episode of Care
Acute/ Chronic
Anatomical Site
Specificity Patient History Other
366.10 – 366.9
Cataract/Nuclear Sclerosis/ Eye conditions (multiple) x
Identify left, right or bilateral eye
365.11 Primary open-angle glaucoma
Specify stage (mild, moderate, severe,
indeterminate, unspecified).
V76.51 Special screening for malignant neoplasm x Direct correlation to ICD10 – Z12.11
Confirm screening not personal history.
174.9 Malignant neoplasm of breast, unspecified x x Specify male/female, specific breast and
quadrant when available
574.20 Calculus of gallbladder w/o mention of cholecystitis, w/o mention of obstruction
Direct correlation to ICD10-K80.20
659.71 Abnormality in Fetal Heart Rate or rhythm delivered w/wo antepartum condition
Direct correlation with ICD10 – O76
836.0 Tear of medial cartilage or meniscus of knee, current x x x x Need type of tear (bucket-handle,
peripheral, complex, other, unspecified)
840.4 Rotator cuff sprain x x
354.0 Carpal tunnel x
654.21 Previous C/S delivery w/wo mention antepartum condition
Direct correlation with ICD10 – O34.21
727.03 Trigger Finger (acquired) x x Specify finger, right/left
820.8 Closed fracture of unspecified part of neck or femur x x
X Specificity of fracture
site needed Need peritrochanteric / subtrochanteric
fracture type
726.10 Rotator cuff syndrome NOS x x
Bursitis vs tendinitis
Need unspecified /incomplete/complete tear or rupture
550.90 Inguinal hernia w/o obstruction or gangrene, unilateral or unspecified x X Identify unilateral or bilateral for inguinal
hernia
722.10 Displacement of lumbar intervertebral disc without myelopathy
x
lumbar vs lumbosacral
715.96 Osteoarthrosis, unspecified whether generalized or local, lower leg x
x
Identify primary/post-traumatic/secondary, bilateral/unilateral
540.9 Acute appendicitis NOS
X Mention peritonitis, abscess, etc . If applicable

4
Ulcers
Documentation for treating ulcers of the limb requires two different types of specificity in ICD-
10:
Site Specificity. Documentation should include the specific area of the body impacted.
For example, in ICD-9, Ulcer of the limb was acceptable. In ICD-10, documentation
should provide the detail required to identify the specific area of the limb (i.e, thigh, calf,
ankle).
Laterality. In addition to site specificity, documentation should include the specific side
of the body impacted (right ankle, left calf).
When reporting ulcers using ICD-10-CM, the severity of the ulcer should be documented. For
non-pressure ulcers, the following levels should be included in the documentation:
Limited to breakdown of skin
Fat layer exposed
With Necrosis of muscle
With Necrosis of bone
With unspecified severity
For pressure ulcers, severity should use the National Pressure Ulcer Advisory Panel (NPUAP)
stages 1-4 and unstageable, listed below:
Stage 1: Pressure pre-ulcer skin changes limited to persistent focal edema
Stage 2: Pressure ulcer with abrasion, blister, partial thickness skin loss involving
epidermis and/or dermis
Stage 3: Pressure ulcer with full thickness skin loss involving damage or necrosis if
subcutaneous tissue
Stage 4 : Pressure ulcer with necrosis of soft tissues through to underlying muscle,
tendon, or bone
Unstageable: Based on clinical documentation pressure ulcers are those “whose stage
cannot be clinically determined (e.g., the ulcer is covered by eschar or has been
treated with a skin or muscle graft) and pressure ulcers that are documented as deep
tissue injury but not documented as due to trauma.”
Unspecified: The ICD-10-CM unspecified coding option is not considered a part of
the NPUAP staging but is provided for reporting when the documentation is
insufficient to assign a more specific code.
The Draft Guidelines note that if the documentation does not provide enough information to
stage the pressure ulcer, the provider should be queried. Pressure ulcers are not reported if they
are documented as healed.

5
Here is an example of the transition from ICD-9 to ICD-10 adding site specificity, laterality and
pressure ulcer stage:
DIAGNOSIS ICD-9 ICD-10 ICD-10 Description (if different)
Pressure Ulcer of ankle 707.06 L89.5 Category: Pressure ulcer of ankle
L89.500 Pressure ulcer of unspecified ankle, unstageable
L89.501 Pressure ulcer of unspecified ankle, stage 1
L89.502 Pressure ulcer of unspecified ankle, stage 2
L89.503 Pressure ulcer of unspecified ankle, stage 3
L89.504 Pressure ulcer of unspecified ankle, stage 4
L89.509 Pressure ulcer of unspecified ankle, unspecified stage
L89.510 Pressure ulcer of right ankle, unstageable
L89.511 Pressure ulcer of right ankle, stage 1
L89.512 Pressure ulcer of right ankle, stage 2
L89.513 Pressure ulcer of right ankle, stage 3
L89.514 Pressure ulcer of right ankle, stage 4
L89.519 Pressure ulcer of right ankle, unspecified stage
L89.520 Pressure ulcer of left ankle, unstageable
L89.521 Pressure ulcer of left ankle, stage 1
L89.522 Pressure ulcer of left ankle, stage 2
L89.523 Pressure ulcer of left ankle, stage 3
L89.524 Pressure ulcer of left ankle, stage 4
L89.529 Pressure ulcer of left ankle, unspecified stage

6
Glaucoma ICD-10 Documentation for glaucoma includes two components:
Severity: Documentation should include severity of the disease:
o Mild
o Moderate
o Severe
o Indeterminate
Laterality: While not all ICD-10 codes require it, identify right, left, bilateral when
possible.
DIAGNOSIS ICD-9 ICD-10 ICD-10 Description (if different)
Primary open angle glaucoma 365.11 H40.11 Primary Open-angle glaucoma
H40.11X0 Stage unspecified
H40.11X1 Mild stage
H40.11X2 Moderate stage
H40.11X3 Severe stage
H40.11X4 Indeterminate stage
Acute angle-closure glaucoma 365.22 H40.21 Acute angle-closure glaucoma
H40.211 Right eye
H40.212 Left eye
H40.213 Bilateral
H40.219 Unspecified eye

7
Tears and Ruptures Documenting tears and ruptures for ICD-10 presents significant differences and increased levels
of specificity. Notable changes are:
Encounter/Episode of Care: Documentation must include whether the visit is defined
as initial, subsequent, or sequela.
Type of Tear: Documentation should include the type of tear, such as bucket-handle,
peripheral, or complex, as well as specific location, such as medial or lateral meniscus.
Laterality: Documentation should include whether the fracture is on the right or left side
of the body.
Acute/Chronic: As with ICD-9, documentation for ICD-10 should include
acute/chronic.
Below is an excerpt and partial list of the additional level of specificity needed for a tear of
medial cartilage or meniscus of knee:
DIAGNOSIS ICD-9 ICD-10 ICD-10 Description (if different)
Tear of medial cartilage or meniscus of knee, current
836 S83.2 Category: Tear of meniscus, current injury
S83.20 Tear of unspecified meniscus, current injury
836.2 S83.200 Bucket-handle tear of unspecified meniscus,
current injury, right knee
S83.200A -Initial encounter
S83.200D -Subsequent encounter
S83.200S -Sequela
S83.201 Bucket-handle tear of unspecified meniscus, current injury, left knee
S83.201A -Initial encounter
S83.201D -Subsequent encounter
S83.201S -Sequela
S83.202 Bucket-handle tear of unspecified meniscus, current injury, unspecified knee
S83.202A -Initial encounter
S83.202D -Subsequent encounter
S83.202S -Sequela
836.0 S83.21 Bucket-handle tear of medial meniscus, current
injury
S83.211 Bucket-handle tear of medial meniscus, current injury, right knee
S83.211A -Initial encounter
S83.211D -Subsequent encounter
S83.211S -Sequela

8
Neoplasm of Breast ICD-10 offers specific codes to identify laterality (right, left), site specificity (quadrant, specific
area), as well as gender (male, female). While the latter is typically provided in documentation
presently, it is important to note that ICD-10 does not provide an “unspecified” gender code for
malignant neoplasm conditions. Documentation which does not identify the gender for
Neoplasm of Breast cannot be processed without this identification.
Below is an example of the ICD-9 to ICD-10 transition based on gender identification, site
specificity, and laterality. Please note that unspecified codes for laterality and site specificity are
available.
DIAGNOSIS ICD-9 ICD-10 ICD-10 Description (if different)
Malignant Neoplasm of Breast C50 Category: Malignant Neoplasm of Breast
C50.0 Malignant neoplasm of nipple and areola
C50.011 Malignant neoplasm of nipple and areola, right female breast
C50.012 Malignant neoplasm of nipple and areola, left female breast
C50.019 Malignant neoplasm of nipple and areola, unspecified female breast
C50.021 Malignant neoplasm of nipple and areola, right male breast
C50.022 Malignant neoplasm of nipple and areola, left male breast
C50.029 Malignant neoplasm of nipple and areola, unspecified male breast
C50.2 Malignant neoplasm of upper-inner quadrant of breast
C50.211 Malignant neoplasm of upper-inner quadrant of right female breast
C50.212 Malignant neoplasm of upper-inner quadrant of left female breast
C50.219 Malignant neoplasm of upper-inner quadrant of unspecified female breast
C50.221 Malignant neoplasm of upper-inner quadrant of right male breast
C50.222 Malignant neoplasm of upper-inner quadrant of left male breast
C50.229 Malignant neoplasm of upper-inner quadrant of unspecified male breast

9
Fractures
ICD-10 coding for fractures represents some of the most significant changes in the transition
from ICD-9 to ICD-10. ICD-10 differentiates traumatic fractures from pathological fractures,
and requires increased specificity in the documentation including:
Encounter/Episode of Care: Documentation must include whether the visit is defined
as initial, subsequent, or sequela.
Open/Closed Fracture: Documentation must include a statement describing the fracture
as open or closed.
Classification: Depending on the fracture type, documentation may require the inclusion
of the Gustillo classification of the fracture (such as for an open traumatic fracture of the
long bone).
Fracture Pattern: Documentation should include fracture details such as transverse,
oblique, spiral, segmental, etc.
Alignment: Documentation must note the alignment of the bones, specifically whether
the fracture is displaced or Nondisplaced.
Site Specificity: Documentation should include additional specificity regarding the name
of bone and specific location of the fracture on the bone.
Laterality: Documentation should include whether the fracture is on the right or left side
of the body.
Healing: Documentation is required to identify whether healing is routine, delayed,
malunion or nonunion for each encounter.

10
Here is an example of the increased level of specificity needed in the documentation for ICD-10: