Embed Size (px)
Citation preview

www.elsevier.com/locate/ygyno
Gynecologic Oncology 9
Conference Report
Communication between patients and healthcare
providers in oncologyi
A cancer diagnosis is often unexpected and stressful.
During the period of diagnosis and treatment for cancer,
patients interact and communicate with multiple healthcare
providers. Communication in a provider patient network may
be important for the satisfaction of both patients and
providers.
Communication is multidimensional and involves both
the content of the discussion and the relationship aspects of
the interaction. The communication may serve many
purposes including exchanging information, creating a good
interpersonal and supportive relationship, and making me-
dical decisions. Communication is important throughout all
phase of the cancer trajectory including screening, diagnosis,
treatment, surveillance, recurrence, and the end of life.
Patients may have difficulty conveying understanding,
processing, and remembering complex medical information.
Patients may be reluctant to bring up certain topics with
their providers, especially psychosocial concerns. Providers
may be reluctant to inquire actively about patients’ reactions
and feelings. Providers may also have difficulty conveying
information in ways that patients’ best understand.
Research suggests that good communication skills are
associated with important outcomes of care. To date there
has been very little research about communication in
cervical cancer. The extent to which findings of other
studies can be applied to cervical cancer is unknown.
Effective healthcare provider–patient communication in
part involves information exchange about issues such as
medical history, symptoms, diagnosis, and prescribed treat-
ment. One conceptual framework that has been proposed is
seen in Fig. 1. This framework demonstrates the complexity
and dynamic nature of the communication process as well as
the importance of the context in which the communication
occurs. Information exchange is critical to effective provider–
patient communication, but it may also be the source of
considerable misunderstanding, sometimes called a commu-
nication gap.
A study that assessed the perceptions of patients and their
oncologists regarding important topics discussed in clinical
encounters will be presented in order to demonstrate some
doi:10.1016/j.ygyno.2005.07.064
i This report is based on a presentation given at the 4th International
Conference on Cervical Cancer.
communication challenges. In this study, patients with
cancers of unknown primary were recruited to participate.
These cancers present as metastatic diseased without a
definitive diagnosis of origin. Approximately 3–5% of all
cancers in the United States carry this diagnosis. After a
thorough evaluation, approximately 25% of patients have a
primary diagnosis.
The goal of the study was to examine physicians and
patients perceptions about what was discussed and their
beliefs about key aspects of their disease during initial
outpatient oncology visits. Patients were recruited from the
unknown primary clinic at M. D. Anderson. Each patient
signed an informed consent. Participants were recruited from
the waiting area prior to their medical visit. The visits were
audiotaped with the consent of all parties. Immediately
following the visit, the physician and patient completed a
brief questionnaire about the visit. Measures that were
collected included demographics, the patient checklist
(perceptions about what was discussed and beliefs about
cancer and treatment), and the physician checklist (percep-
tions about what was discussed and beliefs about cancer and
treatment).
Seventy-eight patients participated in the study. Patients
were on average 61 years old and 69% were male. Patients
were primarily Caucasian (90%) and 90% were married or
living with a partner. Thirty-one percent worked full-time
and 56% had a college degree or higher education.
Results of this study indicated there were discrepancies
in perceptions between patients and physicians regarding
the extent to which several topics were discussed as well as
9 (2005) S137–S138
Fig. 1. Conceptual framework for communication.
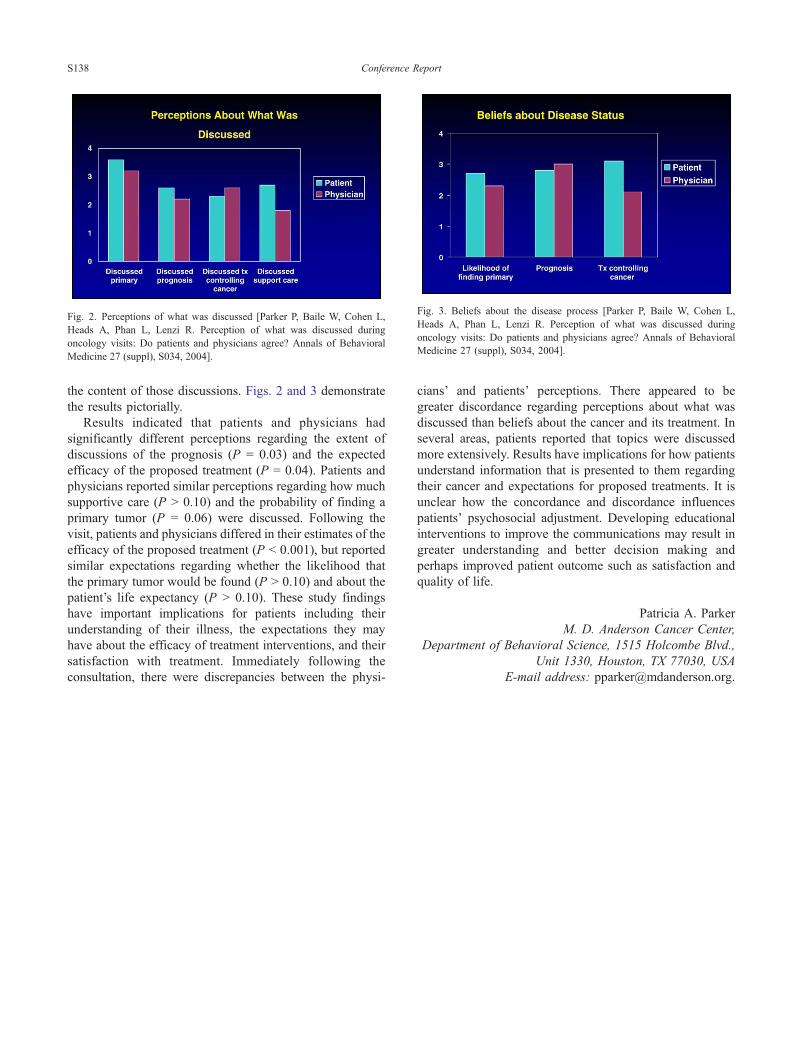
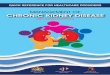
Fig. 2. Perceptions of what was discussed [Parker P, Baile W, Cohen L,
Heads A, Phan L, Lenzi R. Perception of what was discussed during
oncology visits: Do patients and physicians agree? Annals of Behavioral
Medicine 27 (suppl), S034, 2004].
Fig. 3. Beliefs about the disease process [Parker P, Baile W, Cohen L,
Heads A, Phan L, Lenzi R. Perception of what was discussed during
oncology visits: Do patients and physicians agree? Annals of Behavioral
Medicine 27 (suppl), S034, 2004].
Conference ReportS138
the content of those discussions. Figs. 2 and 3 demonstrate
the results pictorially.
Results indicated that patients and physicians had
significantly different perceptions regarding the extent of
discussions of the prognosis (P = 0.03) and the expected
efficacy of the proposed treatment (P = 0.04). Patients and
physicians reported similar perceptions regarding how much
supportive care (P N 0.10) and the probability of finding a
primary tumor (P = 0.06) were discussed. Following the
visit, patients and physicians differed in their estimates of the
efficacy of the proposed treatment (P b 0.001), but reported
similar expectations regarding whether the likelihood that
the primary tumor would be found (P N 0.10) and about the
patient’s life expectancy (P N 0.10). These study findings
have important implications for patients including their
understanding of their illness, the expectations they may
have about the efficacy of treatment interventions, and their
satisfaction with treatment. Immediately following the
consultation, there were discrepancies between the physi-
cians’ and patients’ perceptions. There appeared to be
greater discordance regarding perceptions about what was
discussed than beliefs about the cancer and its treatment. In
several areas, patients reported that topics were discussed
more extensively. Results have implications for how patients
understand information that is presented to them regarding
their cancer and expectations for proposed treatments. It is
unclear how the concordance and discordance influences
patients’ psychosocial adjustment. Developing educational
interventions to improve the communications may result in
greater understanding and better decision making and
perhaps improved patient outcome such as satisfaction and
quality of life.
Patricia A. Parker
M. D. Anderson Cancer Center,
Department of Behavioral Science, 1515 Holcombe Blvd.,
Unit 1330, Houston, TX 77030, USA
E-mail address: [email protected].