Embed Size (px)
Citation preview

Journal of Clinical Psychology in Medical Settings, Vol. 4, No. 3, 1997
Communication Differences Between Physiciansand Their Patients in an Oncology Setting
Tamara Goldman Sher,1-3 David Cella,2 William T. Leslie,2
Philip Bonomi,2 Samuel G. Taylor, IV,2 and Bernie Serafian2
The physician-patient relationship has critical importance in the quality ofmedical care, especially in the oncology setting. Of particular interest over thepast two decades has been the communication between physicians and theirpatients. It is understood that communication is related to patient andphysician satisfaction as well as other medical outcomes. However, despite thisinterest and attention, investigators have onfy recently begun to assess thecommunication between physicians and patients from the patient's point ofview. Additionally, previous investigations have primarily relied uponretrospective reports of the interaction from patients or physicians. The currentinvestigation assessed physician-patient communication in an oncology setting,both as it was occurring and following the interaction. The units of analysisincluded participant ratings as well as those of trained observers. Findingsrevealed that physicians and patients disagree as to the valence of the messageswhich transpired. Additionally, results suggest that it is the patients who distortthe messages in the positive direction. Research and clinical implications ofthis disagreement and positivity bias are discussed.
KEY WORDS: oncology; communication; physician; patient.
INTRODUCTION
The physician-patient relationship has critical importance in the qual-ity of medical care. It also has been described as one of the most complexinterpersonal relationships (Ong, DeHaes, Hoos, & Lammes, 1995). The
1Illinois Institute of Technology, Institute of Psychology, 1 IIT Center, Chicago, Illinois 60616.2Rush-Presbyterian-St. Luke's Medical Center, Chicago, Illinois.3To whom correspondence should be addressed.
281
1068-9583OT0900-0281$12.5(W e 1997 Plenum Publishing Corporation

282 Sher et al.
complexity of this relationship can be explained by the following: (a) itinvolves interaction between individuals in nonequal positions; (b) it isoften involuntary; (c) it concerns issues of vital importance; and (d) it isemotionally laden and requires close cooperation (Ong et al., 1995).
Communication between physicians and their patients is one aspectof the physician-patient relationship which has attracted much attentionover the last two decades. Research findings indicate that effective physi-cian-patient communication is related to patient satisfaction, physiciansatisfaction, compliance, and medical outcomes, making it a valuable toolin medical care. Also, "physician shopping" and malpractice claims areoften related to miscommunication between physicians and patients (Ep-stein, Campbell, Cohen-Cole, McWhinney, & Smilkstein, 1993). As a result,educators have increasingly included communication training into their cur-ricula with strategies such as encouraging physician attention and listeningto patients' problems, negotiating plans for evaluation and treatment, andincorporating patients' views and beliefs into the therapeutic strategies(Beckman, Kaplan, & Frankel, 1989).
Cancer is a chronic, life-threatening illness which poses many chal-lenges to the relationship between a physician and a patient. Treatmentdecisions present themselves frequently, often over a long trajectory, mak-ing it continually important for the physician and the patient to engage ineffective communication. Interestingly, however, there are very few studiesof communication in oncology (Ford, Fallowfield, & Lewis, 1996). Althoughsome of these studies focus on the content of the communication betweenan oncologist and patient (i.e. Ford et al., 1996), the majority focus on thepatient's need for more specific or detailed information (Bernheim, Ledure,Souris, & Razavi, 1987; Blanchard, Labrecque, Ruckdeschel, & Blanchard,1988; Cassileth, Volckman, & Goodman, 1980; Chaitchik, Kreitler, Shaked,Schwartz, & Rosin, 1992; Molleman, Krabbendam, & Annyas, 1984; Tat-tersall, Butow, Griffin, & Dunn, 1994). Specifically, recent studies havefound that between 80 and 94% of patients with cancer or other terminaldiagnoses desire all available information regarding their disease(Blanchard, 1988; Fallowfield, Ford, & Lewis, 1995; Kai et al., 1993). Simi-larly, Castejon et al., (1993) report that 52% of interviewed cancer patientsreported a desire for additional information, especially about prognosis,treatment, and handling of their disease. However, despite these consistentfindings, physicians routinely underestimate patients' need for complete in-formation (Blanchard, 1988; Waitzkin, 1984).
There is some suggestion within this literature that a patient's needfor more information from a physician may mask a larger concern with thequality of communication between the patient and the physician (Cassilethet al., 1980). Others suggest that much of cancer patients' dissatisfaction

Physician-Patient Communication 283
with the exchange of information stems from a lack of concordance be-tween the perceptions of patients and those of physicians (Chaitchik et al.,1992).
In addition to studies related to the quality of physician-patient com-munication and those related to the patient's satisfaction with the physicianas a result of their communication, efforts have also focused on patients'recall of their conversations with their physicians. Results indicate that pa-tients often do not recall or understand what their physician has told them.In a review of three communication investigations, between 7 and 47% ofpatients did not understand what they were told regarding their diagnoses.Additionally, between 13 and 53% of these patients did not understandwhat they had been told regarding disease prognosis (Ley, 1988). That is,patients are not clearly hearing the important information that their phy-sicians are trying to relay.
The extent to which patient misinformation is due to physician with-holding versus patient forgetting or distortion remains unclear. However,what is known is that the potential costs of poor understanding includeloss of confidence in staff and dissatisfaction with medical care; increasedanxiety, distress, and coping difficulties; and noncompliance with treatment(Tattersall et al., 1994). Many investigations have found a discrepancy be-tween what physicians report having said and what patients report havingheard (e.g., Ley, 1988). Unfortunately, these studies all employ retrospec-tive recall of the interaction. Very few of them have directly assessed theinteraction itself. It remains unclear, then, to what extent the miscommu-nication originates from physician factors such as communication skill andwillingness to inform, versus patient factors such as anxiety and the needfor hope (Tattersall et al., 1994).
The extent to which patients distort information from their physicianshas rarely been addressed. Makoul, Arntson, & Schofield (1995) investi-gated health promotion communication in a primary care context. Theyassessed both actual communication between general practitioners and pa-tients as well as the perceptions of that communication using both codedtranscripts of the videotaped interactions and the patients' perceptions ofthe conversations following the conversations. This investigation focusedon communication and decision making about prescription medications.Results revealed that, of 226 patient reports and actual conversations,24.3% of the patients either moderately or very strongly agreed that theirphysician fully explained risks of the prescribed medication when coderswere unable to find any mention of side effects, precautions, or risks. Theseinvestigators concluded that for these patients, there would be an illusionof competence they would impart upon their physicians.

284 Sher et al.
Although communication is just emerging as a productive area forresearch within the health care field in general and the oncology settingin particular, research in assessing and improving couples' communicationhas been developing for more than two decades (Baucom & Adams, 1987;Baucom & Epstein, 1990). Research in couples' communication has high-lighted the importance of understanding potential distortions incommunication. For example, previous research which compared outsideobservers' ratings of communication with insiders' (i.e., partners') ratings,found gender differences which were related to marital satisfaction. Mentend to rate their partner's communication as more positive than do outsideobservers, whereas women tend to rate their partner's communication asmore negative than do outside observers (Floyd & Markman, 1983). Thispositive bias has been shown to predict relationship decline by promotingavoidance of direct conflict. Avoidance of direct conflict not only predictsrelationship decline, but also differentiates distressed from nondistressedcouples (Gottman & Krokoff, 1989).
The purpose of the current investigation was to understand betterthe physician-patient relationship through the assessment of the commu-nication between physicians and patients using a method developed formarital communication research. Unlike previous investigations, communi-cation was assessed by the patients and the physicians at both the globallevel, in terms of overall satisfaction ratings, and at the microanalytic level,as it was occurring. Communication was also assessed by outside observers(trained coders) in order to elucidate any potential distortions of the com-munication process. The communication was assessed during the firstappointment to avoid bias introduced by any relationship between the phy-sician and the patient. This eliminated the possibility that a privatecommunication system existed to which an outside observer would not haveaccess (Gottman & Krokoff, 1989).
METHOD
Participants
Over the course of one calendar year, consecutive patients attendingtheir first visit with a participating oncologist at a large metropolitan medi-cal center were approached to participate in this study. Of these, 31 agreedto participate, which was approximately one-half of those approached. Thephysician-patient dyads were assessed during the patient's first visit withthe physician. People with any cancer, diagnosed at any stage, were eligibleto participate. Physicians included five medical oncologists: four were at-

Physician-Patient Communication 285
tending physicians and one was an oncology follow, all from the same prac-tice group.
Materials
Communication Box (CB). A modified version of the communicationbox procedure as described by Markman (1984) was used to obtain mi-croanalytic ratings of both physicians and patients of their owncommunication. Initial pilot work with this procedure in a medical settingsuggested one deviation from the usual CB protocol used with couples ina laboratory setting. Instead of rating each message, participants made rat-ings regarding the tone of the conversation as it had taken place over thepreceding 90 sec. More information regarding this change in protocol canbe found elsewhere (see Sher, Cella, Serafian, & Leslie, 1993). Participantswere instructed to make ratings which reflected how positive or negativethe previous 90 sec of conversation seemed to them. The CB itself is asmall, hand-held plastic box with seven buttons, ranging from 1 = verynegative to 7 = very positive. The box is attached by cable to an IBMlaptop computer, which translated responses into an ASCII file for lateranalysis.4 Physicians and patients were blind to each other's ratings. Vide-otapes were made of every interaction to permit scoring by outsideobservers.
Ratings of Outside Observers. Because of our interest in any potentialbias that might exist for either patients or physicians, outside observersrated the communication in the same fashion as the subjects. That is, theyrated each 90-sec block of communication from the videotape, as to hownegative or positive it appeared to them on the same 7-point scale. Theywere trained, using the Affect component of the Couples' Interaction Scor-ing System (CISS; Notarious & Markman, 1981), to observe both verbaland nonverbal cues in an effort to judge the overall valence of each 90-secunit. Interrater reliability (percentage agreement) following training was70.5% based on 25% of the interactions being rated by two observers.
Doctors'/Patients' Post-Session Questionnaire (D-PSQ or P-PSQ). Thesequestionnaires were designed for the current study in order to assess threedifferent areas of interest: (a) physicians' and patients' global ratings of thecommunication which transpired between them; (b) their perception oftheir relationship; and (c) the ease of using the communication box. Theissue of communication box ease and utility with this population has beenaddressed elsewhere (see Sher et al., 1993).
4The computer program used for the communication box is available from the authors.

286 Sher et al.
Procedure
Five oncologists who had previously agreed to participate in the cur-rent investigation were approached whenever a new patient was scheduledto be seen. The patients were approached by the study team and the studyintroduced in the following manner: "We are conducting a study of com-munication between physicians and patients. In this study, we are testinga piece of equipment that helps compare the differences between what peo-ple say to one another and what they hear from one another. Are youinterested in hearing more about it?"
Communication Session. The CB and accompanying video equipmentwere set up in a conference room within the oncology clinic. Instructionsfor the use of the box were given to each patient. Practice time was allottedand comfort with the apparatus was assured before the video equipmentwas activated. The physician, having been pretrained, was not part of thepractice session. No specific topic was offered for participants other thana reminder to "talk as you normally would." Following the conversationbetween the physician and patient, the video equipment was disconnectedand the P/D-PSQ was distributed to both patient and physician. Patientsand physicians completed the PSQs in different rooms. Videotapes of theinteraction were coded by observers at another time.
An additional, follow-up session was initially planned as part of thisinvestigation in order to assess the relationship between communicationvariables and both disease and compliance variables. However, of the 31original patients, only 9 returned for a follow-up appointment. Most pa-tients who did not return were seeking a second opinion consultation. Asa result, follow-up analyses were not conducted.
Finally, demographic and disease information was obtained from thepatient's medical chart, with the patient's permission.
RESULTS
Demographics
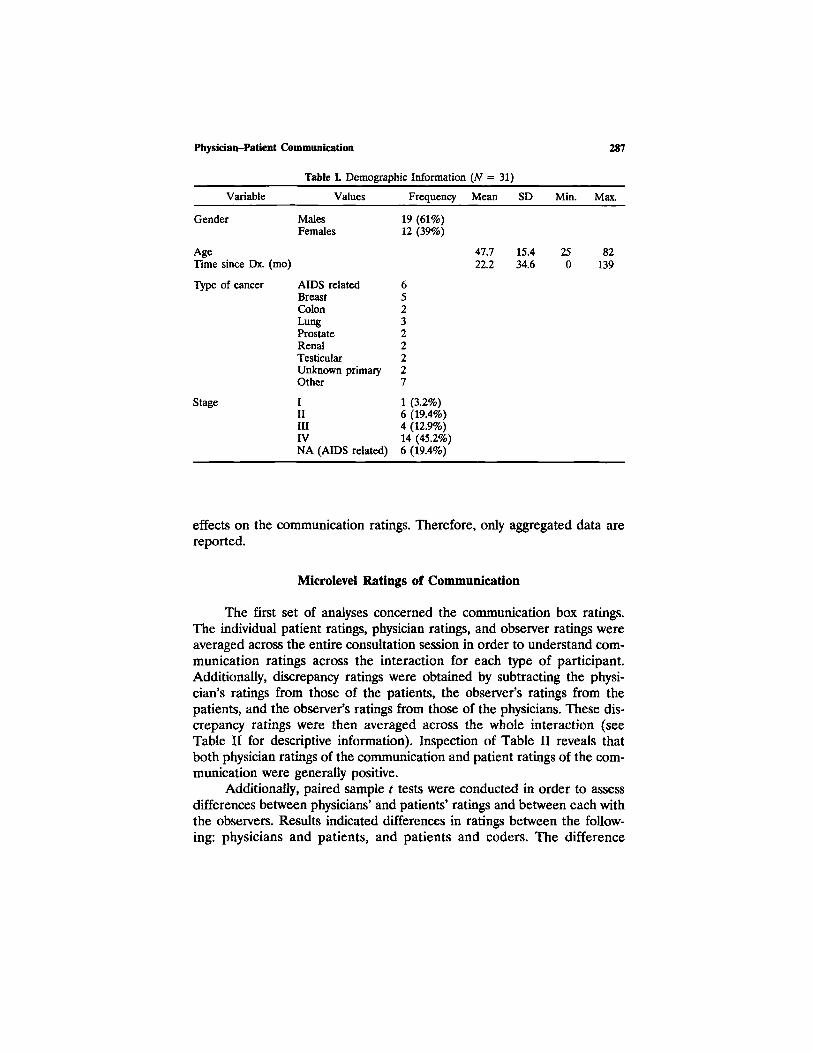
The gender, age, race, months post-cancer diagnosis, type of cancer,and stage of disease of the patients are listed in Table I. The five physicianswere all male; four were Caucasian and one was African American. Eachphysician saw between 1 and 17 patients. The results are combined due tono significant differences emerging by physician. Similarly, as indicated byindependent-sample t tests, there were no patient gender or stage of illness
Physician-Patient Communication 287
Table I. Demographic Information (N = 31)
Variable
Gender
AgeTime since Dx. (mo)
Type of cancer
Stage
Values
MalesFemales
AIDS relatedBreastColonLungProstateRenalTesticularUnknown primaryOther
IIIIIIVNA (AIDS related)
Frequency
19 (61%)12 (39%)
652322227
1 (3.2%)6 (19.4%)4 (12.9%)14 (45.2%)6 (19.4%)
Mean
47.722.2
SD
15.434.6
Min.
250
Max.
82139
effects on the communication ratings. Therefore, only aggregated data arereported.
Microlevel Ratings of Communication
The first set of analyses concerned the communication box ratings.The individual patient ratings, physician ratings, and observer ratings wereaveraged across the entire consultation session in order to understand com-munication ratings across the interaction for each type of participant.Additionally, discrepancy ratings were obtained by subtracting the physi-cian's ratings from those of the patients, the observer's ratings from thepatients, and the observer's ratings from those of the physicians. These dis-crepancy ratings were then averaged across the whole interaction (seeTable II for descriptive information). Inspection of Table II reveals thatboth physician ratings of the communication and patient ratings of the com-munication were generally positive.
Additionally, paired sample t tests were conducted in order to assessdifferences between physicians' and patients' ratings and between each withthe observers. Results indicated differences in ratings between the follow-ing: physicians and patients, and patients and coders. The difference

288 Sher et al.
Tabler II. Communication Ratings (N = 31 Patients, 5 Physicians)
Variable
Average physician ratingsAverage patient ratingsAverage discrepancy*
Patient/physicianc
Patient/observe/Physician/observer*
Mean
4.65"5.39*
.74
.67
.23
SD
.71
.99
1.00.61.73
Min.
33
-1-1-1
Max.
67
421
Note. Average ratings over the entire session are reported here. Communicationratings were made every 90 sec. Ratings were on a 7-point scale, from 1 =very negative to 7 = very positive.
"Physicians less positive than patients [/(30) = 4.14, p < .001].''Discrepancy = the difference between the average of two raters.'Patient more positive than physician (p < .001).^Patient more positive than observer (p < .001).eNot significant.
between physicians and coders, however, was not statistically significant[t(29) = 1.76, p =.09; see Table II]. Inspection of the means revealed thatfor both comparisons including the patient (i.e., doctor and observer), thepatient was more positive than the other rater.
Global-Level Satisfaction Ratings
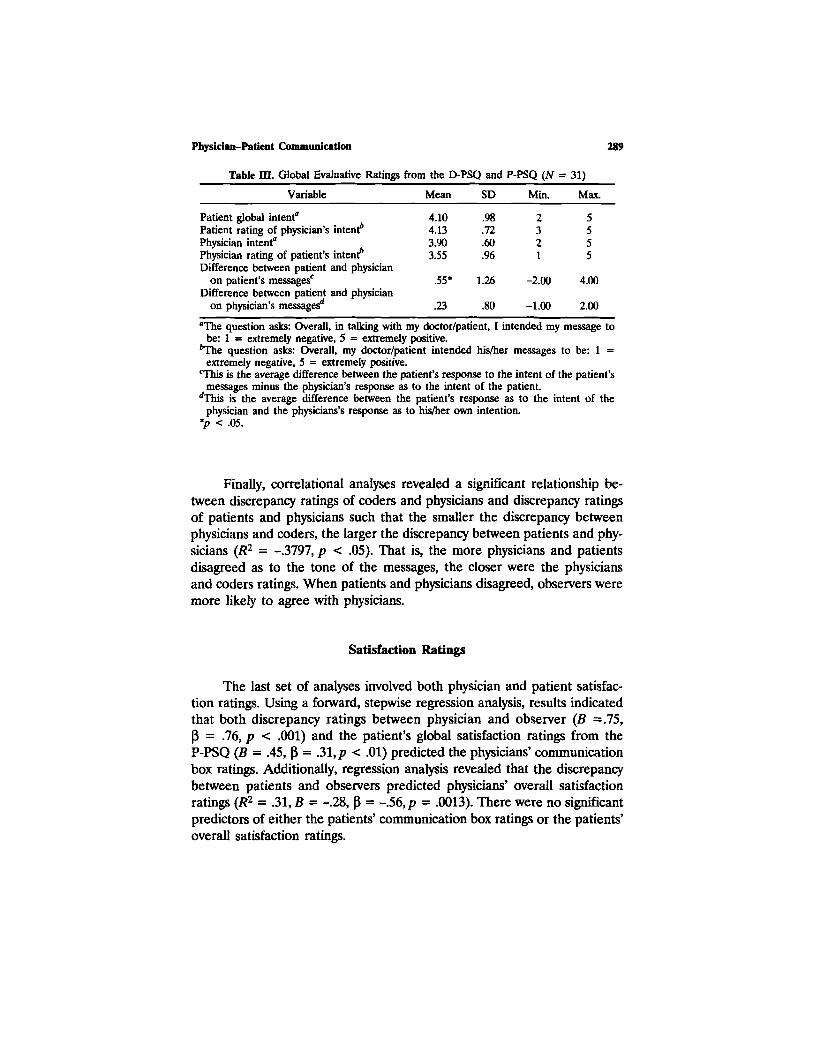
Global ratings of the communication were assessed using the D-PSQand the P-PSQ. Two questions were used to assess the patients' and thephysicians' overall belief as to the valence of the communication (questions1 and 2). The means and standard deviations for both questions, as wellas the wording of the questions, are listed in Table III. Means are alsoprovided for the discrepancy between how physicians and patients ratedthe patients' intent overall (patient rating minus physician rating) and howphysicians and patients rated the physicians' intent overall (patient ratingminus physician rating).
Additionally, paired sample t tests were conducted in order to assessdifferences between the physicians' ratings of overall intent and the pa-tients' ratings of the physicians' intent, and vice versa. Results indicated asignificant difference in how each viewed the patients' comments overall[^(30) = 2.42, p < .05]. Inspection of the means indicates that patientsbelieved their messages to be more positive than their physicians perceivedthose same messages. The findings concerning the difference between howpatients and physicians viewed the physicians' overall intent were not sig-nificant [f(30) = 1.56, p = .129].
Physician-Patient Communication 289
Table m. Global Evaluative Ratings from the D-PSQ and P-PSQ (N = 31)
Variable
Patient global intent"Patient rating of physician's intent*Physician intent"Physician rating of patient's intent*Difference between patient and physician
on patient's messages1
Difference between patient and physicianon physician's messages.
Mean
4.104.133.903.55
.55*
.23
SD
.98
.72
.60
.96
1.26
.80
Min.
2321
-2.00
-1.00
Max.
5555
4.00
2.00
"The question asks: Overall, in talking with my doctor/patient, I intended my message tobe: 1 = extremely negative, 5 = extremely positive.
*The question asks: Overall, my doctor/patient intended his/her messages to be: 1 =extremely negative, 5 = extremely positive.
This is the average difference between the patient's response to the intent of the patient'smessages minus the physician's response as to the intent of the patient.
dThis is the average difference between the patient's response as to the intent of thephysician and the physicians's response as to his/her own intention.
*p < .05.
Finally, correlational analyses revealed a significant relationship be-tween discrepancy ratings of coders and physicians and discrepancy ratingsof patients and physicians such that the smaller the discrepancy betweenphysicians and coders, the larger the discrepancy between patients and phy-sicians (R2 = -.3797, p < .05). That is, the more physicians and patientsdisagreed as to the tone of the messages, the closer were the physiciansand coders ratings. When patients and physicians disagreed, observers weremore likely to agree with physicians.
Satisfaction Ratings
The last set of analyses involved both physician and patient satisfac-tion ratings. Using a forward, stepwise regression analysis, results indicatedthat both discrepancy ratings between physician and observer (B =.75,P = .76, p < .001) and the patient's global satisfaction ratings from theP-PSQ (B = .45, P = .31, p < .01) predicted the physicians' communicationbox ratings. Additionally, regression analysis revealed that the discrepancybetween patients and observers predicted physicians' overall satisfactionratings (R2 = .31, B = -.28, P = -.56, p = .0013). There were no significantpredictors of either the patients' communication box ratings or the patients'overall satisfaction ratings.

290 Sher et al.
DISCUSSION AND CONCLUSIONS
This study was designed in order to assess the communication processbetween oncologists and their patients during a first visit. It used a well-known methodology in marital research to assess communication at themicroanalytic level. Rather than explaining what is said, this approach per-mits understanding of the perceptions of the communicators regarding thevalence of the messages. Additionally, this study aimed to compare partici-pants' ratings of their own communication with that of observers who wereable to take a more objective view of the information that was being pre-sented. By adding observer ratings, we were able to assess distortions inthe communication process.
This study indicates that there is indeed a difference in the percep-tions of physicians and patients as to the valence of the communication.Patients hear information that is presented to them as more positive thanphysicians either intended it or believed that it was communicated. Thisfinding is true at both the microanalytic (message) level and the global(evaluative) level. These results are consistent with previous research whichhas found communication discrepancies between physicians and their pa-tients (e.g., Chaitchik et al., 1992).
This study points to a bias on the part of patients in terms of theirperceptions of their physicians' messages. Patients perceived messages morepositively than they were intended by the physician or perceived to be bythe observer. This finding is consistent with that of Makoul et al. (1995),in that patients were more positive about an interaction than was perhapswarranted. Although both studies agree on the presence of a "positive bias"in patients, Makoul et al. (1995) relied upon patients' recall of information,whereas this study obtained ratings as the communication occurred.
Finally, this study examined whether microanalytic ratings and globalratings of communication predicted satisfaction. In terms of the patient sat-isfaction ratings, there were no predictors. This may be because, as previousinvestigators have found, there was little variance in patients' overall sat-isfaction ratings (e.g., Kai et al., 1993; Rowland-Morin & Carroll, 1990).Previous studies have found that although patients are often dissatisfiedwith the information they receive (Ley, 1988), patients report satisfactionwith their care when asked (Kai et al., 1993). In the current study, all pa-tients were generally satisfied with the communication process. However,there were predictors of physicians' satisfaction, including differences be-tween observers and patients, suggesting that physicians are more satisfiedwith more positive distortion on the part of patients.
Perhaps, then, both patients and physicians benefit from patient po-sitivity bias. Although the current investigation was not designed to

Physician-Patient Communication 291
interpret this bias, several hypotheses are possible. First, patients may needto exaggerate the possibility of therapeutic benefit in order to consent tooften costly and toxic treatments which offer no guarantees of effectiveness.Second, patients may have a need to see their physicians more positivelythan is actually "earned" by the physicians due to the investment made inthem. Makoul et al. (1995) found this to be so, labeling it an "illusion ofcompetence." Future investigations may be better able to sort out whichof the above, or perhaps other, explanations may explain this positivity bias.
In terms of the physicians, perhaps they benefit (i.e., are more satis-fied) when patients are more positive because it eases the difficulty ofgiving bad news. This explanation is consistent with findings that physicianstypically underestimate a patient's desire for information (Waitzkin, 1984).They may underestimate it when they are faced with a negative reactionfrom a patient. A positive reaction may encourage more information to begiven, leading physicians to reinforce a patient positivity bias with moreinformation. Again, future studies should be designed in order to under-stand better the positivity bias that has been highlighted in this and otherinvestigations (e.g., Makoul et al., 1995).
The shortcomings of the current investigation include the small sam-ple size and the somewhat less than optimal interrater reliability as to thevalence of a message. The small sample size results from the difficulty ofscheduling the physicians for the communication session. Although they allagreed that the communication box was less intrusive than they had an-ticipated, it nonetheless required them to break from their normal clinicroutine.
While the interrater reliability was somewhat low (71%), it was notsignificantly lower than in other studies using trained raters. For example,Ford et al. (1996) reported interrater reliability at .78, using another stand-ardized measure of physician-patient behavior (Roter Interaction AnalysisSystem, RIAS). This lower number may reflect the complexity of the in-teraction for observers but is deemed high enough to make resultsinterpretable.
There are multiple clinical applications of the above findings. First,the way that patients interpret information received from their physicianneeds to be understood by the physician and other health care providers.This interpretation could influence other decisions such as the rejection ofnecessary intervention or an unrealistic expectation of health which mayprove harmful should a downturn occur. Second, medical education notonly needs to include information on successful communication strategieswhich engender more patient satisfaction but, in fact, should include a dis-cussion of a positivity bias and how communication might be altered toaccount for it. For example, more questions from the physician as to in-

292 Sher et al.
terpretation of information on the patient's part should also be included.In many cases, it may be up to the psychologist working with these patientsto help the physicians identify this bias and then work with patients whena more realistic interpretation of their status is deemed necessary.
Finally, there are measurement implications of the findings. Patientsshould not be the only source of information regarding the content andintention of messages given by their physicians. The decision to use self-report, while practical, should include input from physicians as well aspatients, so that discrepancies can be identified and hopefully reconciled.
It is clear that physician-patient communication is an important com-ponent of medical care. This investigation helps explain the interpretationsbehind the message. Just as discrepancies in message interpretation predictmarital dissatisfaction, they also appear to play an important role in thephysician-patient relationship.
ACKNOWLEDGEMENTS
This study was funded in part by the following grants to both authors:the Illinois Cancer Council and Rush-Presbyterian-St. Luke's MedicalCenter University Committee on Research award.
REFERENCES
Baucom, D. H., & Adams, A. (1987). Assessing communication in marital interaction. In K.D. O'Leary (Ed.). Assessment of marital discord (pp. 139-181). NY: Lawrence ErlbaumAssociates.
Baucom, D. H., & Epstein, N. (1990). Cognitive-behavioral marital therapy. New York:Brunner/Mazel.
Beckman, H., Kaplan, S. H., & Frankel, R. (1989). Outcome based research on doctor-patientcommunication: A review. In M. Stewart & Roter, D. (Eds.). Communicating with medicalpatients (pp. 223-227).
Bernheim, J. L., Ledure, G., Souris, M., & Razavi, D. (1987). Differences in perception ofdisease and treatment between cancer patients and their physicians. In N. K. Aaronson& J. Beckmann (Eds.), The quality of life of cancer patients. New York: Raven Press.
Blanchard, C. G., Labrecque, M. S., Ruckdeschel, J. C., & Blanchard, E. B. (1988).Information and decision-making preferences of hospitalized adult cancer patients. SocialScience and Medicine, 27, 1139.
Cassileth, B. R., Volckman, B. A., & Goodman, R. L. (1980). The effect of experience onradiation therapy patients' desire for information. International Journal of RadiationOncology, 6, 491-496.
Castejon, J., Lopez-Roig, S., Pastor, M. A., Pico, C., Reig, M. T., Rodriguez-Marin, J., &Terol, C. (1993). Cancer patients: health information and quality of life. In The 7thConference of the European Health Psychology Society, abstract.
Chaitchik S., Kreitler, S., Shaked, S., Schwartz, II, & Rosin, R. Doctor-patient communicationin a cancer ward. Journal of Cancer Education, 7, 41.

Physician-Patient Communication 293
Epstein, R. M, Campbell, T. L, Cohen-Cole, S. A., McWhinney, I. R., & Smilkstein, G.(1993). Perspectives on patient-doctor communication. Journal of Family Practice, 37,377-388.
Fallowfield, L., Ford, S., & Lewis, S. (1995). No news is not good news: Informationpreferences of patients with cancer. Psycho-oncology, 4, 197-202.
Floyd, F., & Markman, H. (1983). Observational biases in spouse observation: Toward acognitive/behavioral model of marriage. Journal of Consulting and Clinical Psychology, 51,450-457.
Ford, S., Fallowfield, L., & Lewis, S. (1996). Doctor-patient interactions in oncology. SocialScience and Medicine, 42, 1511-1519.
Gottman, J., & Krokoff, L. (1989). Marital interaction and satisfaction: A longitudinal view.Journal of Consulting and clinical Psychology, 57, 47-52.
Kai, L, Ohi, G., Yano, E., Kobayashi, Y., Miyama, T., Niino, N., & Naka, K (1993).Communication between patients and physicians about terminal care: A survey in Japan.Social Science and Medicine, 36, 1151-1159.
Ley, P. (1988). Communicating with patients. Improving communication, satisfaction andcompliance. London: Chapman and Hall.
Makoul, G., Arntson, P., & Schofield, T. (1995). health promotion in primary care:physician-patient communication and decision making about prescription medications.Social Science and Medicine, 41, 1241-1254.
Markman, H. J. (1984). The longitudinal study of couples' interactions: Implications forunderstanding and predicting the development of marital distress. In N. Jacobson & K.Hahlweg (Eds.), Marital Interaction: Analysis and Modification. New York: Guilford Press.
Molleman, E., Krabbendam, P. J., & Annyas, A. A. (1984). The significance of thedoctor-patient relationship in coping with cancer. Social Science and Medicine, 18, 475.
Notarious, C. I., & Markman, H. J. (1981). The Couples' Interaction Scoring System. In E.E. Filsinger & R. A. Lewis (Eds.), Assessing marriage: New behavioral approaches (pp.112-127). Beverly Hills, CA: Sage.
Ong, L. M. L., DeHaes, J. C. J., Hoos, A. M., & Lammes, F. B. (1995). Doctor-patientcommunication: A review of the literature. Social Science and Medicine, 40, 903-918.
Rowland-Morin, R. A., & Carroll, J. G. (1990). Verbal communication skills and patientsatisfaction. A study of doctor-patient interviews. Evaluation and the Health Professions,13, 168-185.
Sher, T. G., Cella, D., Serafian, B., & Leslie, W. (1993). An old procedure with a newpopulation: The use of the communication box in a medical setting. Behavior Therapist,248-250.
Tattersall, M. H. N., Butow, P. N., Griffin, A. M., & Dunn, S. M. (1994). The take-homemessage: patients prefer consultation audiotapes to summary letters. Journal of ClinicalOncology, 12, 1305-1311.
Waitzkin, H. (1984). Doctor-patient communication: Clinical implications of social scientificresearch. Journal of the American Medical Association, 252, 2441.





























