Embed Size (px)
DESCRIPTION
Communication Skills Using Simulation for Physicians (Dealing with Angry Patients and Cultural Sensitivities) Iblagh,Nadia BSc,MA.Leadership MSc.Med.Ed &Diabetes Candidate-University ofDundee. Introduction. - PowerPoint PPT Presentation
Citation preview
Communication Skills Using Simulation for Physicians(Dealing with Angry Patients and Cultural Sensitivities)
Iblagh,Nadia BSc,MA.Leadership
MSc.Med.Ed &Diabetes Candidate-University ofDundee
1
2
Introduction• Good non- technical (eg. vigilance, anticipation, clear
communication, team coordination) can reduce the likelihood of error consequently of accidents.
• Simulation is a powerful tool because it allows the trainer to systematically control the schedule prime, presentation of feedback and introduction( or suppression) of environmental distractions, within a safe, controlled environment.
3
4
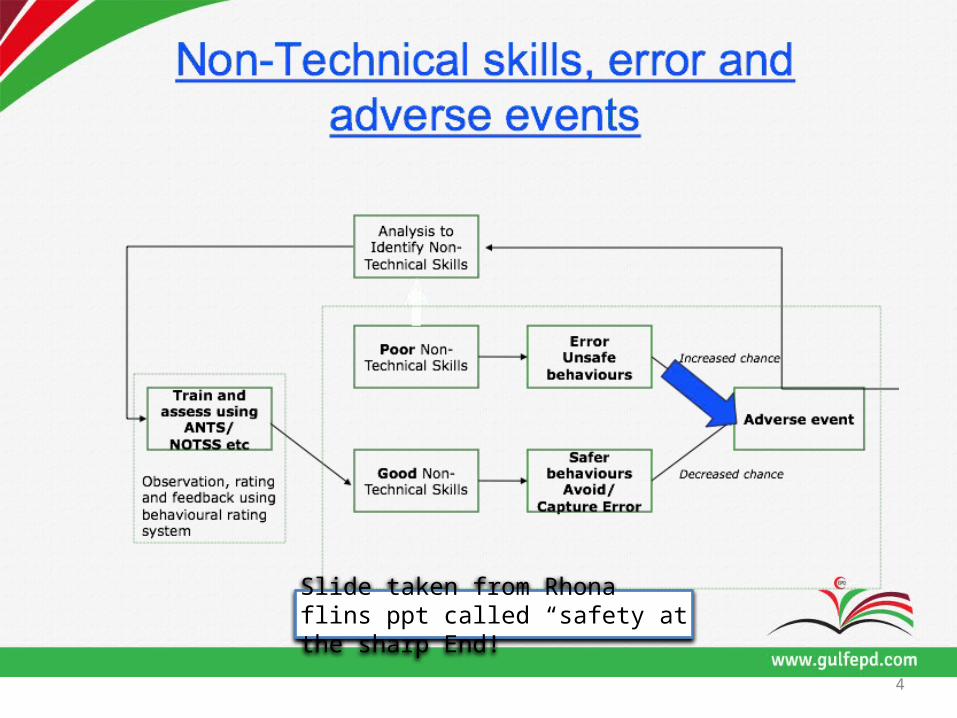
Slide taken from Rhona flins ppt called “safety at the sharp End!
5
• Leadership
• Team Work
• Communication
• Situation Awareness
• Decision Making
• Personal Limitations – managing stress and fatigue
• Reports of problems caused by mis-communication amongst
Practitioners themselves Patients and the practitioners
• Non- technical clinical skills vs Technical skills training in Kuwait
6
Objectives Designing a training session for HCP to train them on one NTS at a time .
7
8
1. Identifying techniques for effective communication skills
focus on dealing with angry patients2. Being able to handle cultural issues
effectively.
Learning Outcomes
Methods
• Standardized patients (SPs), a trained actor used as "real" simulators
• The SP playing a specific role based on given scenario.
9
Teaching Strategies
Number of strategies 1- SISFR 2- STEPS
10
11
• S = Set the context and identify roles and outcomes.
• I = Immerse in roles and practice for agreed time frame
• S = Summary presentation of progress with scenario
• F = Feedback from self, peers, and tutors• R = Refine practice building on feedback. I
1- SISFR
Feedback
• Information describing students' performance in a given activity.
• Key step in the acquisition of clinical skills.
• Often omitted or handled improperly in a clinical training.
12
• When effective feedback is provided and focuses on directly observable skills and behaviors, important personal and educational progress can occur, Katz
13
Feedback & Debriefing Importance of the feedback & debriefing
SETGO :• What student Saw.• What else the group/student Saw• What the student Thinks• What Goal do we want to achieve.• Any offers how we get there
14
The Intervention
• Videotaping• Setting the simulated scenario• Immersion & belief
15
Evaluation &
Feedback• Comments on : the strategies used• The reflection• Authenticity• Future trainings
16
17
Limitations
Notes
Improved performance ?
true progression ? or
an artificial improvement!!
18
Conclusion/ Reflection
• The results for this study would be used designing and providing non-technical skills session. offering practitioners, clinical skill sessions, using simulation equipped with standards teaching strategies to master those skills is a milestone towards a better health outcome.
19
References
20
21
1. Leonard M, Graham S, Bonacum D. The Human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care 2004;13(Suppl 1):i85–90.
2. BeaubienJ,BakerP. The use of simulation fortraining teamwork skills in healthcare:how low can you go?QualSafHealthCare. 2004;13(Suppl ):i51–6.
3. MaguireP,PitceathlyC. Key communication skills and how to acquire them. BMJ.2002;325:697–700.
4. Johnston P, Fioratou E, Flin R. Non-technical skills in histopathology: Definition and discussion. Histopathology 2011; 59: 259– 367.
5. Flin R, OConnor P, Crichton. Safety at the Sharp End. A Guide to Non-Technical Skills. Aldershot: Ashgate; 2008.
6. Mitchel, A. M, Fioravanti M, Founds S, Hoffmann, R. L., & Libman, R. Using simulation to bridge communication and cultural barriers in health care encounters: Report of an international workshop. Clinical Simulation in Nursing, 2010; 6(5):193–198.
22
7. Fay-Hiller TM, Regan RV, Gordon MG. Communication and Patient Safety in Simulation for Mental Health Nursing Education. Issues in Mental Health Nursing 2012; 33(11):718-726.
8. KaufmanD.M.,ABC of learning and teaching in medicine: Applying educational henry in practice.BMJ(2003),326,213-216
9. JarcheH. Modelling,nots haping.[homepageontheInternet].2012[cited2012Nov 29]. Available from: http://www.jarche.com/2012/01/modelling-not-shaping/
23
10. Torre D.M., Daley B.J., Sebastian J.L., Elnicki D.M. Overview of Current Learning
11. Theories for Medical Educators. American Journal of Medicine 2006;119 (10):903-907.
12. Chronister C, Brown D. Comparison of Simulation Debriefing Methods. Clinical Simulation
in Nursing, 2012; 8(7):281-288.
13. Pendleton D, Schofield T, Tate P., A method for giving feedback. In: The consultation: an
approach to learning and teaching.Oxford: Oxford University Press, 1984. 68–71.
14. Carr S., The foundation program assessment tools: an opportunity to enhance
2006;82:576-9.
24

Thank You





























