Embed Size (px)
Citation preview

Community Organization and How to Get Programs
School Liaisons: Started
Mary Ann Pentz
ABSTRACT: This paper briefly reviews four intervention models, Rothman’s community organization, Green’s system- centered education, Rogers’ innovation-decision process, and Watzlawick’s planned change, for their applicability to help initiate community-based programs for drug abuse prevention and health promotion in youth. An expanded model is described, including preprogram assessment of the target population, community, and drug use problem, and continuous evaluation of program process and product. School liaisons are emphasized as a key factor in early adoption and demonstration of a community-based program for youth. The expanded model, including school liaisons, is applied to a comprehensive community drug abuse prevention project being implemented in the Greater Kansas City area. The model - and the project - suggest methods for organizing communities for long-term drug prevention, initialb at the level of school and school district, and later to the family, mass media, and community organizations in a proximal-to-distal sequence of programming. ( J Sch Health 1986;56(9):382-388)
he 1979 U.S. Surgeon General’s Report on Healthy T People, as well as national surveys of health risk behaviors, have pointed to the need for population-wide disease prevention strategies to achieve significant reductions in cancer, heart disease, and drug abuse by the end of this century.lv2 To accomplish these goals requires the implementation of proven prevention technologies in a large scale such as a community or city, utilizing the multiple channels that constitute the target population’s everyday environment.
Unfortunately, reports and surveys documenting the need for community-based prevention programs do little to prepare prospective programmers for entry into the community or for successful program implementa- t i~n . ’ -~ Previous research suggests that three factors may determine successful entry, implementation, and ulti- mately, “institutionalization” of a community-based prevention program: sequential use of multiple channels for community program delivery; availability of com- munity resourcs to support the program; and commun- ity “ownership” of the program.6-8 In drug abuse pre- vention, a fourth factor is community awareness of the drug abuse p r ~ b l e m . ~ In contrast to general health promotion or to prevention of heart disease, readily accepted as a physical illness, drug abuse is often associated with personal or family mental health p r ~ b l e m s . ~ - ~ ~ Research indicates that these associations carry negative connotations in a society that prides itself on maintaining positive images of individuals and f a m i l i e ~ . ~ J ~ J ~ Thus, drug abuse prevention often is met with fear, denial, and misunderstanding by one or more constituencies in the community.
Most typically, fear is exhibited by one constituency but not another, producing an inherent conflict and the establishment of pressure or advocacy groups within the community. See, for example, a description of Roth- Mary Ann Pentz, PhD, Associate Professor for Research, Institute for Health Promotion and Disease Prevention Research, University of Southern California, 35 N. Lake Ave., Suite 200, Pasadena, CA 91101. This paper was presented at the Henry J . Kaiser Family Foundation and The Pew Charitable Trusts “Conference on Community-based Health Promotion and Drug Abuse Prevention for Youth,” Menlo Park, Calif., April 27-29. The work was supported, in
part, by a grant from the National Institute on Drug Abuse DA03976.
man’s6 social action model of community organization. A school which otherwise serves as a major liaison with community groups and as a microcosm of a functioning community can be particularly averse to initiating drug abuse prevention, and generating media attention in the process, because it may be regarded by the community as an admission that the school has a drug p r ~ b l e m . ~ J ~ J ~
Ironically, even if the need for drug abuse preven- tion is accepted by all the constituencies in a community, controversy may still arise over the type of prevention approach. Several approaches have emerged, most not- ably drug control, drug information, and drug resist- ance.” Only drug resistance, the most recently develop- ed approach, has been shown to have a consistent pre- ventive effect on drug abuse in large population samples of y o ~ t h . ~ , ~ ~ , ~ * However, communities continue to adhere to control and information approaches, both of which have received considerable attention in the media and in schools.9J9
Discussing the problems of community-based drug prevention is not intended to deter the prospective pro- grammer. Rather, the intention is to point out the many steps the prospective programmer must take to initiate and maintain a program, including community accep- tance of the need for the program, and to generate support from all constituencies and a sense of commun- ity ownership.
A brief overview of four intervention models reveals consensus about the importance of several of these steps, and elaborates on each one. The models were selected from different bodies of research literature to demon- strate the applicability and generalizability of steps to community organization, regardless of topical area.
OVERVIEW OF MODELS FOR COMMUNITY ORGANIZATION
Rothman’s Model of Community Organization Developed from research in organization develop-
ment and social work, Rothman’s community organiza- tion model has been applied successfully in the Min- nesota Heart Health Project, the North Karelia Project, and several other community health promotion pro- jects.6J0,’2,20v21 The model is based on proactive program
382 Journal of School Health November 1986, Vol. 56, No. 9
planning and analysis that is initiated by professional change agents who are outside the community, and on training local leaders to promote community recogni- tion of a need for prevention programming. Central to Rothman’s model is the focus on initiating the program in one or a few communities. The trial community serves as a model to other prospective program communities, creating a high demand/low supply incentive for com- munities to “wait list” for programming. Once a site is selected by external programmers, extensive interviews with key community leaders are conducted by program- mers. Typically, the interview process yields a hierarchial structure consisting of a steering committee or advisory board of a few individuals who sanction the program and assist the programmers make future contacts or com- munity entry, a greater community council who assist in concrete program planning, monitoring, and decision- making, and one or more task forces or subcommittees that support program implementation by developing periodic campaigns or events.
A unique feature of the community organization mod- el is the use of a formal needs assessment, such as a baseline survey of drug use, to help community leaders define the health problem, generate channels and re- sources for program delivery, and develop a sense of early participation in program planning that later translates to community ownership. Other unique fea- tures are a feasibility analysis to determine the likeli- hood of collaboration between internal programmers, representatives from the community organization struc- ture, and external programmers during program plan- ning, and the continuous use of research and evaluation to guide entry, planning, and actual program implementation. Green’s System-centered Education Model
This model was developed from research in public health, and outlines four steps or phases for community organizations: the “start up” phase (similar to Roth- man’s steps for identifying community leaders and establishing an organization structure); “initial involvement” of the community through workshops and short-term health promotion events; “installation of change” through the development of long-term educational and task force programs, and community support groups; and “maintenance of change” through extension of prevention skills to new target populations and health behaviors.2 The model differs from Roth- man’s in that the lay community, rather than profes- sional programmers, is responsible for program plan- ning and delivery, and needs assessment is a continuous process that serves to redefine goals at regular intervals during program implementation. The use of continuous needs assessment may provide more “real-life” rele- vance or ecological validity for community program- ming than Rothman’s model. However, reliance on the lay community could reduce the potential for adopting theory-based programming, standardized program delivery, and long-term program maintenance.18Jg
Roger’s Innovation-decision Process Model Roger’s innovation-decision process model is more
widely recognized as a component of his diffusion of innovation theory in communications research than as a model of community organization.22 However, the five
steps in the process are particularly relevant to initiating community-based prevention programs. The five steps are promoting initial knowledge of the program among community leaders, utilizing persuasion strategies to promote adoption, providing a mechanism such as a town council meeting for formal program adoption, en- couraging initial implementation of the program, and expediting confirmation of the original decision to adopt the program.
There is one disadvantage to the innovation-decision process model. It does not provide a structure for organizing councils, task forces, or support groups. However, it does suggest definite steps to engage community leader support. It also emphasizes the need for early reinforcement and feedback. An additional feature is the considerable body of research developed from the diffusion of innovation theory suggests specific characteristics to seek, or at least expect, in community leaders and other early program adopters.22 The charac- teristics include high levels of education, socioeconomic status, interpersonal communication and mass media use, and competitive risk-taking and modeling be- havior. Watzlawick’s Model of Planned Change
The model most associated with the program plan- ning step in community organization is the model of planned change developed by Watzlawick and others,B-n primarily from the fields of consultation and organiza- tion development. In this model, a programmer pro- ceeds through five steps of planned change: analysis of antecedent conditions in the community, preparation for actual program adoption, planning the program, implementing and monitoring the program, and refin- ing the program based on initial program results. The planned change model has an advantage over other models. Individual (particularly programmer) and situa- tion characteristics are considered in the program initia- tion, and a method for engaging resistant communities is recommended. This method is referred to as “second- order change,” which challenges community leaders to justify whether a program is n e c e s s a r ~ . ~ ~
AN EXPANDED MODEL OF COMMUNITY ORGANIZATION
The four models share a fundamental emphasis on the steps to successfully initiate community-based pro- grams: 1) recognize the need for prevention; 2) identify community or opinion leaders, and establish a commun- ity decision-making structure; 3) complete a formal decision-making process for program adoption; 4) pre- program planning directed by the external professional programmer, with facilitation by the community organ- ization structure; 5 ) train community leaders using a team of external and internal programmers; 6) imple- ment initial program in a single community or a portion of the community; 7) confirm the initial decision to adopt (reinforcement and feedback); and 8) continue program monitoring and evaluation to maintain the quality of implementation and to refine the program on a regular basis.
Journal of School Health November 1986, Vol. 56, No. 9 383
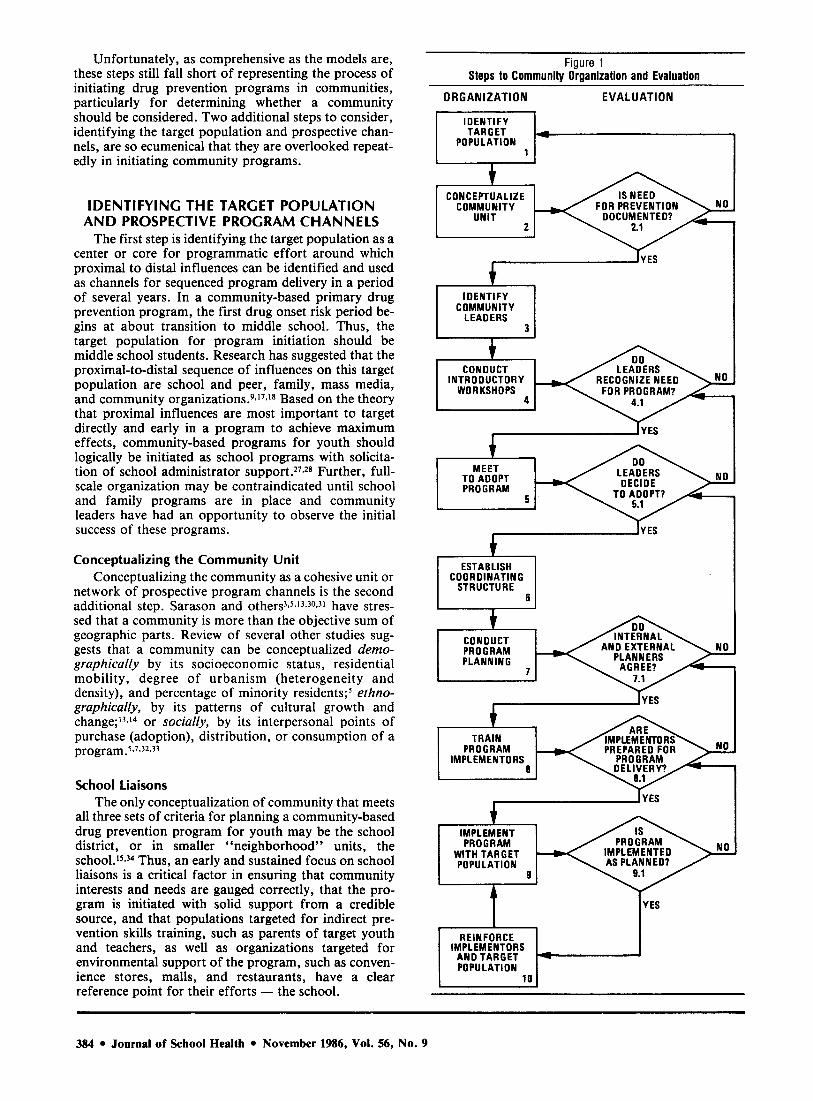
Unfortunately, as comprehensive as the models are, these steps still fall short of representing the process of initiating drug prevention programs in communities, particularly for determining whether a community should be considered. Two additional steps to consider, identifying the target population and prospective chan- nels, are so ecumenical that they are overlooked repeat- edly in initiating community programs.
IDENTIFYING THE TARGET POPULATION A N D PROSPECTIVE PROGRAM CHANNELS
The first step is identifying the target population as a center or core for programmatic effort around which proximal to distal influences can be identified and used as channels for sequenced program delivery in a period of several years. In a community-based primary drug prevention program, the first drug onset risk period be- gins at about transition to middle school. Thus, the target population for program initiation should be middle school students. Research has suggested that the proximal-to-distal sequence of influences on this target population are school and peer, family, mass media, and community organizati~ns.~J~J* Based on the theory that proximal influences are most important to target directly and early in a program to achieve maximum effects, community-based programs for youth should logically be initiated as school programs with solicita- tion of school administrator Further, full- scale organization may be contraindicated until school and family programs are in place and community leaders have had an opportunity to observe the initial success of these programs.
Conceptualizing the Community Unit Conceptualizing the community as a cohesive unit or
network of prospective program channels is the second additional step. Sarason and ~ t h e r ~ ~ ~ ~ J ~ ~ ~ ~ J ~ have stres- sed that a community is more than the objective sum of geographic parts. Review of several other studies sug- gests that a community can be conceptualized demo- graphically by its socioeconomic status, residential mobility, degree of urbanism (heterogeneity and density), and percentage of minority residents; ethno- graphically, by its patterns of cultural growth and change;13J4 or socially, by its interpersonal points of purchase (adoption), distribution, or consumption of a program.’v7J2J3
School liaisons The only conceptualization of community that meets
all three sets of criteria for planning a community-based drug prevention program for youth may be the school district, or in smaller “neighborhood” units, the s ~ h o o l . ~ ~ . ~ ~ Thus, an early and sustained focus on school liaisons is a critical factor in ensuring that community interests and needs are gauged correctly, that the pro- gram is initiated with solid support from a credible source, and that populations targeted for indirect pre- vention skills training, such as parents of target youth and teachers, as well as organizations targeted for environmental support of the program, such as conven- ience stores, malls, and restaurants, have a clear reference point for their efforts - the school.
Figure 1 Steps to Community Organization and Evaluation
ORGANIZATION EVA1 U AT1 0 N - I t
CON C EPTU A L IZE
UNIT COMMUNITY FOR PREVENTION
2
IDENTIFY COMMUNITY I LEADERS II
CONDUCT LEADERS INTROOUCTORY
WORKSHOPS FOR PROGRAM?
,I YES I t
MEET TO ADOPT PROGRAM
1 5
ESTABLISH COORDINATING
STRUCTURE
v I I
TRAIN PRO GRAM PREPARED FOR
IMPLEMENTORS PRO GRAM
I IYES
IMPLEMENT PROGRAM IMPLEMENTED 0 ; A M Y WITH TARGET POPULATION AS PLANNED?
9
1 IYES - I REINFORCE
IMPLEMENTORS AND TARGET POPULATION
I 10 I
384 Journal of School Health November 1986, Vol. 56, No. 9
The school serves as a liaison between programmers and the community to the extent that it can share infor- mation with community leaders and other early pro- gram adopters. Newman’ suggests that school adminis- trators may be in the best position to serve in an infor- mation-sharing liaison role with the community. Unlike parents and school board members who tend to react to community pressures, particularly financial, and unlike teachers who may resent programs initiated from out- side of the community, and students whose main concern is daily functioning under the constraints of a class schedule, administrators are able to recognize and open the channels of feedback and communication between a school adopting a community-based program for class- room use, and the community waiting to disseminate the program throughout the population.15J4
In addition to their information-sharing role, ad- ministrators make early sanction and adoption decisions for the larger community-based effort and typically are among the first individuals selected for representation on a community council for prevention. Teachers can assist dministrators prepare the community for program adoption by sharing knowledge about prevention skills demonstrated in the classroom, by reinforcing students who practice prevention skills in settings other than the school, such as through the use of extra-credit home- work assignments involving parents or siblings, and by demonstrating adult health behavior, such as voluntary smoking cessation. 1 8 ~ 9 ~ 1
Summarizing these considerations, an expanded model of community organization is presented in Figure 1. Expanding Rothman’s structural model, ten distinct organizational steps are outlined, from initial entry into the community through actual program implementa- tion. The model incorporates a formal decision-making process of adoption by community leaders, which pre- cedes any formal program planning (see steps 5-7). Program implementors subsequently are trained, and reinforced for early adoption and implementation fol- lowing Roger’s model (see steps 8-10). At each organiza- tional step, a continuous evaluation of organizational process and outcome is emphasized to ensure effective program implementation, following the models of Green and Watzalawick (evaluation is conceptualized as
Figure 2 Program Sequence
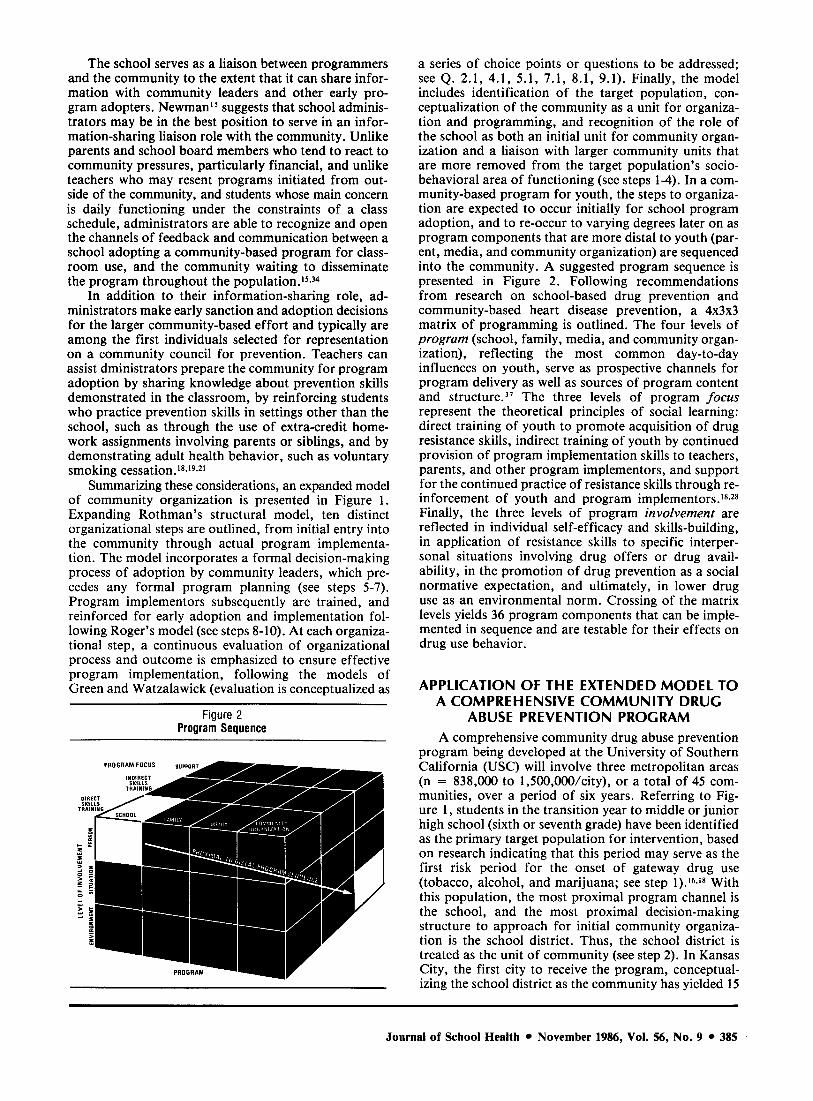
a series of choice points or questions to be addressed; see Q. 2.1, 4.1, 5.1, 7.1, 8.1, 9.1). Finally, the model includes identification of the target population, con- ceptualization of the community as a unit for organiza- tion and programming, and recognition of the role of the school as both an initial unit for community organ- ization and a liaison with larger community units that are more removed from the target population’s socio- behavioral area of functioning (see steps 1-4). In a com- munity-based program for youth, the steps to organiza- tion are expected to occur initially for school program adoption, and to re-occur to varying degrees later on as program components that are more distal to youth (par- ent, media, and community organization) are sequenced into the community. A suggested program sequence is presented in Figure 2. Following recommendations from research on school-based drug prevention and community-based heart disease prevention, a 4 x 3 ~ 3 matrix of programming is outlined. The four levels of program (school, family, media, and community organ- ization), reflecting the most common day-to-day influences on youth, serve as prospective channels for program delivery as well as sources of program content and ~tructure.’~ The three levels of program focus represent the theoretical principles of social learning: direct training of youth to promote acquisition of drug resistance skills, indirect training of youth by continued provision of program implementation skills to teachers, parents, and other program implementors, and support for the continued practice of resistance skills through re- inforcement of youth and program implementors.1s.2s Finally, the three levels of program involvement are reflected in individual self-efficacy and skills-building, in application of resistance skills to specific interper- sonal situations involving drug offers or drug avail- ability, in the promotion of drug prevention as a social normative expectation, and ultimately, in lower drug use as an environmental norm. Crossing of the matrix levels yields 36 program components that can be imple- mented in sequence and are testable for their effects on drug use behavior.
APPLICATION OF THE EXTENDED MODEL TO A COMPREHENSIVE COMMUNITY DRUG
ABUSE PREVENTION PROGRAM A comprehensive community drug abuse prevention
program being developed at the University of Southern California (USC) will involve three metropolitan areas (n = 838,000 to 1,500,000/city), or a total of 45 com- munities, over a period of six years. Referring to Fig- ure 1, students in the transition year to middle or junior high school (sixth or seventh grade) have been identified as the primary target population for intervention, based on research indicating that this period may serve as the first risk period for the onset of gateway drug use (tobacco, alcohol, and marijuana; see step l).16-i* With this population, the most proximal program channel is the school, and the most proximal decision-making structure to approach for initial community organiza- tion is the school district. Thus, the school district is treated as the unit of community (see step 2). In Kansas City, the first city to receive the program, conceptual- izing the school district as the community has yielded 15
Journal of School Health November 1986, Vol. 56, No. 9 385
distinct communities. In 13 of these communities, the school district is also the geographic boundary of the community; in the remaining two communities, the school district encompasses several small geographi- cally-bounded communities that can be aggregated for community organization.
At both the school and school district level, the need for prevention was documented by USC and Kansas City-based project staff, who conducted baseline sur- veys of drug-use behavior in sixth, seventh, eighth, tenth, and 12th grade students in fall 1984 (see Q. 2.1). Revealing drug use levels similar to those reported else- where, the results were returned to school administra- tors (superintendents and principals), who were identi- fied as community leaders in the early stages of the project (see step 3).'6,'8
An introductory half-day workshop was conducted with school administrators to acquaint them with the need for a resistance skills approach to drug prevention (see step 4, Q. 4.1). The workshop consisted of an over- view of psychosocial influences on drug use, demonstra- tion of resistance skills, brief review of research on resistance skills-based programs, and presentation of a five-year plan for community drug abuse prevention, beginning with a school program and progressing to parent, community organization, and health policy programs. Administrators subsequently met with their respective school districts and teaching staff to decide whether to adopt a USC-developed resistance skills school program for implementation in Kansas City in 1984-1985 (see step 5 ; Q. 5.1). Those schools scheduling specific teachers and courses for program training and implementation in 1984-1985 were considered to have formally adopted the program. All 26 schools desig- nated by research design for program implementation in 1984-1985 subsequently scheduled, trained for, and implemented the program; the remaining 26 designated to serve as controls in 1984-1985 scheduled training and implementation in 1985-1986, and subsequently imple- mented the school program as planned. The school pro- gram included a ten-session curriculum on resisting pressures to use drugs and counteracting drug use influ- ences, a five-session booster curriculum, and homework sessions with parents.
Once school administrators had decided to adopt the program, a coordinating structure was developed to faciliate program planning and subsequent implementa- tion (see step 6). The coordinating structure consisted of representative school district and school-level adminis- trators, the Kansas City project director and school pro- gram coordinator as primary internal planners for the project, and USC investigators. As external planners, USC investigators met with the internal project director to standardize teacher training and program imple- mentation; a teacher training manual was revised to include use of role plays that were contextually relevant to Kansas City schools (see step 7). These meetings yielded an agreed-upon protocol to maximize the proba- bility that program and research integrity would be maintained throughout the project (see Q. 7. l).3s,3h.37 The protocol includes an operations manual that provides information about data collection procedures, test schedules, and procedures for contacting schools and community organizations, and a series of six-month
planning manuals, that provide details about program development, use of personnel and materials, and co- ordination of program and research implementation activities.
Internal and external planners subsequently trained teachers for school program delivery in the half of the schools designated for implementation in 1984-1985 (see step 8). Immediately after training, teachers and USC staff rated teacher preparedness for program implemen- tation (see Q. 8.1). Follow-up meetings were conducted by Kansas City project staff to review any remaining questions about preparation prior to program initiation. The program subsequently was implemented, and exten- sive process and program implementation data were col- lected by USC and Kansas City staff to determine if the program had been implemented as planned including data on number and length of program sessions, difficulty experienced in role playing, and level of disruptive behavior displayed by students during program sessions (see step 9, Q. 9.1).
Preliminary incidence and prevalence data on drug use in youth currently are available for Kansas City communities. The results are consistent with data from other regional and national studies and have been pre- sented to communities as evidence that prevention is a timely and beneficial approach. Extensive program implementation and process also are available. These and preliminary results of outcome data were reported to school administrators in fall 1985 to promote confirmation of their original decision to adopt the school program and to promote adoption of the next program component, the parent/family program, in 1986-1987. Kansas City staff have reinforced adminis- trators, teachers, and students for program imple- mentation through the use of award certificates, special ceremonies and dinners, tickets to sports activities, and news coverage of the school program in operation (see step 10).
Currently, the community project is retracing the steps in Figure 1 to organize parents as community leaders, in preparation for the 1986-1987 parent pro- gram. The goals of the program include training parents to practice pressure resistance and communication skills, and to develop school drug abuse prevention guidelines, community and support activities that promote a drug- free environment. In spring 1986, 156 parent group leaders, 52 student skill leaders, and 26 principals from one-half of the Kansas City middle schools were trained to achieve these goals through the organization of parent prevention groups (n = 26). By the end of spring, 46% of the groups already had developed pre- vention guidelines for their schools. In subsequent years of the project, the steps will be repeated to include media representatives and local government and civic service agency directors as community leaders. Simul- taneously, programming is expanding in a proximal-to- distal sequence as presented in Figure 2, with a com- munity-wide, environmental support-focused program (a health policy change intervention) serving as the last component to be added in the sequence.
CONCLUSION Consensus has been reached in several bodies of
386 Journal of School Health November 1986, Vol. 56, No. 9

research literature about the necessary steps for success- ful community organization and program initiation. Elaboration of these steps yields a ten-step model that goes beyond simple initiation of a single program in a community to the sequenced implementation of several programs in multiple communities. The model is partic- ularly suited to the organization and implementation of a proximal-to-distal sequence of comprehensive pro- gramming for drug abuse prevention in youth.
The community organization model and program- sequencing scheme presented in this paper have pro- duced effective developed program implementation in the first two years of the community project. However, several complex questions remain, suggesting that suc- cessful community organization may be as much as art as a science. Results of one study suggest that com- munity leaders’ initial level of involvement in pre- vention is related to their perception of change in drug use in the community.16 One possible reason for this finding is that organizations may expect more immedi- ate change than prevention efforts typically demon- strate; once involved, they may modify their expecta- tions accordingly to expect less immediate change, but more long-term ~hange.’~,’6 A second possible reason is that organizations may apply different evaluation criteria to successful program implementation and out- come than do researchers.6.21 Specifically, whether or not program implementors and the target population like a program may be more important to a community than if it was implemented correctly or produced statistically significant changes in drug use.13,24 If not resolved at the program planning level between internal and external planners (step 7 in Figure l ) , these differ- ences in perception about what constitutes an important program outcome may lead to rejection of an otherwise effective drug prevention program and, alternatively, adoption of a prevention program that is popular but not effective.
Related to the question of valid program outcome measures is program process, specifically, whether all proposed organizational steps must be followed, in order and in a timely sequence, to be considered representative of (and thus testable as) a “community organization” effort for prevention. If internal and external planners do not agree about a school-based pre- vention program to be implemented, internal planners continue program planning and implementation with their own resources (a “grass-roots’l effort), and train- ing of program implementors is not provided because of budget constraints, is the community organization effort a failure? If no change in drug use occurs in the target population after the program has been imple- mented, is the lack of effect due to an ineffective pro- gram, insufficient external planner involvement, inade- quate preparation of implementors, poor evaluation measures (or procedures), or all of these?
Because of the multiple possibilities for breakdown of the model, internal and external planners alike may want first, to develop an attenuated community organi- zation model that is feasible and maintainable over the long term, relies on no or few outside resources, and can be implemented through an established organizational structure in the commlunity, such as a parent teacher organization. The attenuated model then can serve as a
minimal standard or “criterion-reference’’ test by which the community evaluates its ability to implement a com- munity-based prevention program. Any additions to the plan, such as the establishment of a new coordinating structure, can be evaluated as measures of community organization transfer or generalization. Development of a minimal standard does not require the inclusion of a coordinating structure, extensive program planning, training, or large-scale program implementation (steps 6-8 and 10 in Figure l ) , the organizational steps that are most subject to modification and deletion in community organization e f f o r t ~ . ~ I - ~ ~
Program outcome, implementation, and process measures should “match” the standard for community organization accepted by program planners. Matching enables a test of the community organization model as well as a test of later prevention program imple- mentation and o u t c ~ m e . ~ ~ . ~ ~ If a community decides to follow an attenuated organizational model as described above, a matched measure of community organization outcome would include the number of steps from one- five and nine that were completed, the time to completion of each, and the proportion of community leaders or program planners participating at each step. See goal attainment scaling for a more complete discus- sion of matching measures to desired ~utcomes . ’~ Pro- gram implementation and process measures would be limited to short-term program implementation on a small scale, use of program materials rather than implementor preparedness, and extent of program implementation in the absence of reinforcement. Pro- gram outcome might be limited to short-term changes in drug use behavior or intentions to use drugs. To the extent that they evaluate community organization as planned apriori by the community, the measures can be used to evaluate the steps and sequencing of steps con- tributing to successful program implementation and outcome. The measures also are useful in evaluating model expansion (inclusion of other steps) in the com- munity and potential for model replicability in other communities.
Additional to issues of model variation and measurement is the question of whether program integrity can be maintained over the long term.
To address this question, the community project will include extensive implementation and process assess- ment throughout all years of the program. Results will be analyzed both descriptively and statistically to determine what exactly constitutes a community pro- gram for drug abuse prevention; and how person, situa- tion, and program environment characteristics interact to affect program adoption and o ~ t c o m e . ’ ~ Specific attention will be paid to typical program integrity prob- lems that Green and others have noted.2J5 These include fragmentation of program adoption by some groups within a community but not others; overemphasis on initial motivation and emotional excitement to the detriment of long-term planning for program mainten- ance, overemphasis on short-term activities and on program content focused more on health knowledge than behavior change, and dependence on external pro- grammers to ensure program dissemination. Pentz et al’* contains an extended discussion of these problems. Answers to these questions will help determine the long-
Journal of School Health * November 1986, Vol. 56, No. 9 * 387
term diffusion question of whether or not community- based programs for drug prevention and health promo- tion in youth are feasible, replicable, and maintainable in other communities. 0
References 1. Fingerhut LA, Wilson RW, Feldman JJ: Health and disease in
the United States. Ann Rev Public Health 198O:l:l-36. 2. Green LW: Toward a Healthy Community: Organizing events
for community health promotion. Washington, DC, US Dept of Health and Human Services, US Public Health Service, 1985;
3. Archer SE, Kelly ED, Bisch SA: Implementing Change in Com- munities: A collaborative process. St. Louis, CV Mosby, 1984.
4. Barry M: A theoretical framework for community organiza- tion. Health Educ Mono, no 3, 1958, reprinted in the SOPHE Heritage Collection of Health Education Monographs, vol 1, Oakland, Third Party Publishing Co, 1982;181-197.
5 . Bonjean CM: The community as research site and object of inquiry, in Bonjean CM, et a1 (eds): Community Politics: A behavioral approach New York, Free Press, 1971, pp 5-15.
6. Rothman J: Three models of community organization practice, their mixing and phasing, in Cox FM et al (eds): Strategies of Com- munity Organization, 3rd ed. Itasca, Ill, FE Peacock Publishers, 1979, pp 25-45.
7. Brown ER: Community organization influence on local public health care policy: A general research model and comparative case study. Health Educ Q 1984;10:205-233.
8. D’Augelli AR, Vallance TR: The helping community: Issues in the evaluation of a preventive intervention to promote informal helping. J Comm Psychol 1982;lO: 199-209.
9. Johnson CA, Hansen WB, Pentz MA: Comprehensive com- munity programs for drug abuse prevention. J Child Contemp SOC 1986:18, nos 1 and 2.
10. Blackburn H: Research and demonstration projects in com- munity cardiovascular disease prevention. J Public Health Pol 1983;4:398-421.
11. Farquhar JW, Maccoby N: The community approach to health promotion and disease prevention. Read before the Carnegie Foundation Conference on Unhealthful Risk Taking Behaviors Among Adolescents. Palo Alto, Calif, 1984. 12. Maccoby N, Solomon DS: Heart disease prevention: Commun-
ity studies, in Rice RE et al (eds): Public Communication Campaigns. Beverly Hills, Calif, Sage Publications, 1981, pp 105-125. 13. Wandersman A, Giamartino GA: Community and individual
difference characteristics as influences on initial participation. Am J Comm Psychol 1980;8:217-228. 14. Iscoe I, Harris LC: Social and community interventions. Ann
Rev Psychol 1984;35:333-360. 15. Newman IM: Mobilizing school systems for community pre-
vention. Prepared for the Community Prevention Research: Technical Review. Rockville, Md, National Institute on Drug Abuse and National Institute on Alcohol Abuse and Alcoholism, 1983. 16. Pentz MA, Johnson CA, Flay BR, Hansen WB: A comprehen-
sive community approach to drug abuse prevention. Read before the American Psychological Association, Los Angeles, 1985. 17. Johnson CA, Solis J: Comprehensive community program for
80-501 13.
drug abuse prevention: Implications of the community health programs for future research, in Glynn T, et al (eds): Preventing Adolescent Drug Abuse: Intervention strategies. Rockville, Md, National Institute on Drug Abuse, no 47, 1983, pp 76-1 14.
18. Pentz MA: Prevention of adolescent substance abuse through social skill development. National Institute on Drug Abuse Research Monography I983;47: 195-232. 19. Bartlett EE: The contribution of school health education to
community health promotion: What can we reasonably expect. Am J Public Health 1981 ;7 1 : 1384-1391. 20. McAlister A, Puska P, Salonen JT, Tuomilehto J, et al: Theory
and action for health promotion: Illustrations from the North Karelia project. Am J Public Health 1982;72:43-50. 21. Rothman J, Erlich JL, Teresa JG: Changing Organizations and
Community Programs. Beverly Hills, Calif, Sage Publicatons, 1981. 22. Rogers EM: The Diffusion of Innovations. New York, Free
Press, 1983. 23. Kettner P, Daley JM, Nichols AW: Initiating Change in Organ-
izations and Communities: A macro practice model. Monterey, Calif, BrooksKole, 1985. 24. Wandersman A: A framework of participation in community
organizations. J Appl Behav Sci 1981;17:27-58. 25. Watzlawick F, Weakland JH, Fisch R: Change: Principles of
problem formation and problem resolution. New York, WW Norton, 1974. 26. Zaltman G: Theory and use among change agents, in Seidman
E (ed). Handbook of Social Intervention. Beverly Hills, Calif, Sage Publications, 1983. 27. O’Neill P, Trickett EJ: Community Consultation. San Fran-
cisco, Jossey-Bass, 1982. 28. Bandura A: Social Learning Theory. Englewood Cliffs, NH,
Prentice Hall, 1977. 29. Puska P, Nissinen A, Tuomilehto J, et al: The community-based
strategy to prevent coronary heart disease: Conclusions from the ten years of the North Karelia Project. Ann Rev Public Health 1985;6:
30. Wilson RN: Community Structure and Health Action: A report on process analysis. Washington, DC, National Commission on Community Health Services, Public Affairs Press, 1970. 3 1. Sarason SB: The Psychological Sense of Community: Prospects
for a community psychology. San Francisco, Jossey-Bass, 1976. 32. Gray HJ: The role of business in health promotion: A brief
overview. Prev Med 1983; 12:654-657. 33. Jason LA, Liotta RF: Assessing community responsiveness in a
metropolitan area. Eva1 Rev 1982;6:703-712. 34. Newman IM, Martin GL, Weppner R: A conceptual model for
developing prevention programs. Int J Addict 1982; 17:493-504. 35. Kornitzer M: Why those differences between the UK and the
Belgian heart disease prevention project results? Prev Med 1984; 13:
36. Klos DM, Rosenstock IM: Some lessons from the North Karelia Project. Am J Public Health 1982;72:53-54. 37. Perry CL, Jessor R: The concept of health promotion and the
prevention of adolescent drug abuse. Health Educ Q 1985;12: 169-184. 38. Pentz MA, Cormack C, Flay BR, Hansen WB, et al: Balancing
program and research integrity in community drug abuse prevention: Project STAR Approach. J Sch Health, 1986;56(9):389-393. 39. Kiresuk TJ, Lund SH: Goal attainment scaling, in Thxisson
CC, et a1 (eds): Evaluation of Human Service Programs, 1978, pp 341-370.
147-1 93.
136-139.
388 Journal of School Health November 1986, Vol. 56, No. 9





























