Embed Size (px)
Citation preview

Review ArticleComparison between Minimally Invasive Plate Osteosynthesis and Conventional Open Plating for Midshaft Clavicle Fractures: A Systematic Review and Meta-Analysis
Enzhe Zhao ,1 Rui Zhang,1 Dou Wu,2 Yao Guo,1 and Qiang Liu 2
1Shanxi Medical University, Taiyuan, Shanxi 030001, China2Department of Orthopedics, Shanxi Dayi Hospital A�liated to Shanxi Medical University, Shanxi Academy of Medical Science, Taiyuan, Shanxi 030032, China
Correspondence should be addressed to Qiang Liu; [email protected]
Received 24 April 2019; Revised 7 August 2019; Accepted 16 August 2019; Published 16 October 2019
Academic Editor: Bryan Cornwall
Copyright © 2019 Enzhe Zhao et al. �is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objective. �e aim of this study was to compare the functional outcome and complications in midsha� clavicle fractures receiving minimally invasive plate osteosynthesis and conventional open plating. Methods. Relevant studies were searched in the databases of Medline, EMBASE, Cochrane Library, Ovid, and Web of Science from inception to March 1, 2019. Pooled data were analyzed with Cochrane Collaboration’s Review Manager 5.3. Results. A total of 7 studies were included, of which 2 were randomized controlled trials, 3 were retrospective cohort studies, and 2 were prospective cohort studies including 316 patients. No statistical di�erences in functional outcome (weighted mean di�erence [WMD] = 0.99, � = 0.12), operation time (WMD = −10.44, � = 0.07) and time to bone union (WMD = −0.23, � = 0.70) were observed between the two groups. However, minimally invasive plate osteosynthesis reduced rates of skin numbness (odds ratio (OR) = 0.25, 95% CI : 0.13 to 0.48; � < 0.0001) and complications (OR = 0.33, 95% CI : 0.16 to 0.71; � = 0.005) compared with conventional open plating. Conclusion. �is systematic review and meta-analysis found no di�erences in terms of functional outcomes, operation time, and fracture healing time between minimally invasive plate osteosynthesis and conventional open plating. However, minimally invasive plate osteosynthesis had apparent advantages in rates of skin numbness and complications.
1. Introduction
�e clavicle fractures constitute an estimated 2% to 5% of all fractures in adults [1]. �ese fractures are most common in younger patients, and are o�en associated with direct clavicle injuries such as contact sports and motor vehicle accidents. It is estimated that approximately 80% occur in the middle third of the clavicle, of which half are displaced [2]. Traditionally, midsha� clavicle fractures were treated nonoperatively by closed reduction, sling or §gure-of-8 harness, and physical therapy, with a low rate of nonunion less than 1% [3]. However, several studies illustrated that the nonunion rate with nonsur-gical management is between 15% and 20% [4–6]. Furthermore, a current meta-analysis found that surgical treatment of mid-sha� clavicle fractures presented a signi§cantly lower nonun-ion rate compared with nonoperative treatment [7]. �erefore,
surgical treatment is o�en preferred for midsha� clavicle fractures today.
Open reduction and plate §xation is one of most com-monly performed surgical techniques for midsha� clavicle fractures. However, conventional open plating (COP) may compromise blood supply, so� tissues, and cause several adverse events especially anterior chest numbness or hypoes-thesia [8]. �e minimally invasive plate osteosynthesis (MIPO) technique was widely used for lower extremity fractures owing to its role in protecting periosteal blood supply of the fracture area [9]. Recently, MIPO technique has been utilized for the treatment of midsha� clavicle fractures with satisfactory clin-ical outcomes [10, 11]. To date, several clinical studies indi-cated that MIPO could achieve similar results with fewer complications compared with COP [12, 13]. However, the optimal surgical approach for midsha� clavicle fractures
HindawiBioMed Research InternationalVolume 2019, Article ID 7081032, 9 pageshttps://doi.org/10.1155/2019/7081032

BioMed Research International2
remains controversial. Based on the information all above, this systematic review and meta-analysis aims to compare func-tional outcome and complications of MIPO with COP in the treatment of midsha� clavicle fractures.
2. Methods
2.1. Search Strategy and Article Selection. �e literature searches were performed in the following databases: Medline, EMBASE, Cochrane Library, Ovid, and Web of Science from inception to March 1, 2019. �e key words used were “clavicle/collarbone/clavicular”, “midsha�/mid-sha�”, “fracture/broken”, “plate”, “open”, and “minimally invasive/MIPO” in combination with the Boolean operators “AND” or “OR”. Search the reference lists of selected articles manually as a secondary source. Articles were not restricted by languages and publication type.
Two reviewers (Enzhe Zhao, Rui Zhang) screened title and abstract of the search results independently, and removed duplicate articles. Both reviewers screened potentially relevant articles in full for evaluation. Disagreements were resolved by discussion with a third reviewer (Dou Wu).
2.2. Eligibility Criteria. �e inclusion criteria were as follows: (a) study design: randomized controlled study (RCT) or nonRCT;
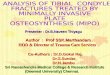
(b) patients with midsha� clavicle fractures (15.2 according to AO/OTA classi§cation [14] or type 2 according to the Robinson classi§cation [15]) (Figure 1); (c) intervention: MIPO and COP; (d) at least one of following data were reported: functional outcomes, operative time, union time, and complications.
�e exclusion criteria were as follows: (a) studies without controlled groups; (b) duplicate publication; (c) pathological fractures; (d) unavailable relevant data.
2.3. Quality Assessment. Modi§ed version of the Cochrane Collaboration’s tool was applied to assess the risk of bias in RCTs [16]. �e Methodological Index for Nonrandomized Studies (MINORS) methodology was used to evaluate other nonRCTs [17]. According to the Cochrane Collaboration recommendations, two reviewers (Enzhe Zhao and Yao Guo) assessed the methodological quality of each included study independently, and a third reviewer (Dou Wu) solved any possible inconsistency.
2.4. Data Extraction and Outcome Measurement. A spreadsheet for data extraction was created prior to this study. Two researchers independently extracted the baseline study data as follows: the §rst author’s name, study design, year of publication, interventions, sample size, mean age, follow-up time, operative time, complications, time to bone union, and functional outcomes.
15.2A Simple fracture
15.2B Wedge fracture
15.2C Multifragmentary fracture
AO/OTA classi�cation Robinson classi�cation
Type 2A1 Undisplaced
Type 2A2 Angulated
Type 2B1 Simple or wedge comminuted
Type 2B2 Isolated or comminutedsegmental
Figure 1: AO/OTA classi§cation and Robinson classi§cation of midsha� clavicle fractures.

3BioMed Research International
�e primary outcome of this meta-analysis was Constant-Murley Shoulder score. Secondary outcomes were operative time, time to bone union, skin numbness/hypoesthesia, and the other complications (e.g., infection, hypertrophic scaring, nonunion, re-fracture, implant failure, skin irritation, and painful shoulder). Fracture union was assessed using radio-graphic evidence, such as callus formation and bony bridging across the fracture site. Nonunion de§ned as a lack of complete osseous bridging a�er 6 months.
2.5. Statistical Analysis. �e Review Manager so�ware (RevMan 5.3, �e Nordic Cochrane Center, �e Cochrane Collaboration, Copenhagen, Denmark) was used for data analysis [18]. �e weighted mean di�erences (WMDs) and odds ratios (ORs) were used to represent continuous and dichotomous outcomes, respectively. Data were pooled using the inverse-variance method for continuous outcomes and Mantel-Haenszel method for dichotomous outcomes. All data were reported with WMD or OR and the 95% con§dence intervals (CI). Heterogeneity between studies was assessed using Chi-square test and I-squared test (�2). Fixed-e�ects model was used if no signi§cant heterogeneity existed (� > 0.1, �2 < 50%). If signi§cant heterogeneity was present (� < 0.1 or �2 > 50%), data were rechecked §rst, then a random-e�ects model was used when heterogeneity persisted. Sensitivity analysis was evaluated by sequentially removing outlier studies, one at a time.
3. Results
3.1. Search Results. A systematic search strategy was created and a total of 114 relevant articles were identi§ed. A�er removal of duplicates, 64 articles were screened based on title and abstract for eligibility, and 7 articles were selected. A�er reading the full text of these 7 articles, no article was excluded based on the selection criteria. �erefore, 7 articles were included in the systematic review [12, 13, 19–23] (Figure 2).
3.2. Quality Assessment. �e quality of RCTs was evaluated by modi§ed version of the Cochrane Collaboration Risk of Bias Tool (Figure 3), and MINORS methodology was used to evaluate nonRCTs (Table 1).
3.3. Study Characteristics. A total of 316 patients with mid-sha� clavicle fractures were involved, including 158 patients treated by COP and 158 patients treated by MIPO. Of the 7 included studies, 2 were randomized controlled trials, 3 were retrospective cohort studies, and 2 were prospective cohort studies. �e full characteristics of the included studies are listed in Table 2.
3.4. Outcomes of Meta-Analysis
3.4.1. Functional Outcome. Five studies [12, 13, 20, 21, 23] reported Constant-Murley scores at one-year follow-up. However, one study [12] was excluded from this analysis,
Additional records identi�edthrough other sources
(n = 0)
Records identi�ed throughdatabase searching
(n = 114)
Records a�er duplicate removed(n = 64)
Records screened(n = 7)
Records excluded bytitle and abstract
(n = 57)
Full-text articles assessed for eligibility
(n = 7)
Full-text articles excluded(n = 0)
Studies included inqualitative synthesis
(n = 7)
Studies included inquantitative synthesis
(meta-analysis)(n = 7)
Iden
ti�ca
tion
Scre
enin
gEl
igib
ility
Incl
uded
Figure 2: Preferred Reporting Items for Systematic Reviews and Meta-Analyses ·ow diagram of study selection process.

BioMed Research International4
follow-up. A §xed-e�ects model was performed without heterogeneity (� = 0.56, �2 = 0%). Overall, the pooled results showed that skin numbness occurred more o�en a�er COP (OR = 0.25, 95% CI : 0.13 to 0.48; � < 0.0001) (Figure 7).
3.4.5. Complications. �e reported complications used for this analysis included infection, hypertrophic scaring, nonunion, re-fracture, implant failure, skin irritation, and painful shoulder except skin numbness/hypoesthesia. A full list of complications can be viewed in Table 3. Two studies [19, 20] reported no complication except skin numbness/hypoesthesia. A §xed-e�ects model was applied without heterogeneity (� = 0.50, �2 = 0%). �e pooled results showed that complications signi§cantly favored COP (OR = 0.33, 95% CI : 0.16 to 0.71; � = 0.005) (Figure 8).
4. Discussion
�e present systematic review and meta-analysis, comparing MIPO versus COP for the treatment of midsha� clavicle frac-tures, found no di�erences in terms of long term functional outcomes, operation time, and time to bone union between MIPO and COP. However, MIPO had apparent advantages in rates of skin numbness and complications. �ese results sug-gested that MIPO is a safe surgical treatment of midsha� clav-icle fractures with fewer complications.
Postoperative functional recovery, one of the most crucial outcomes, is closely related to the quality of life of patients. Clinical scores such as American Shoulder and Elbow Surgeons (ASES) score, Constant-Murley score and Disabilities of the Arm, Shoulder, and Hand (DASH) were o�en used to assess the postoperative functional recovery. We also employed the Constant-Murley score, including pain, range of motion and activities of daily living, to evaluate postoperative func-tional recovery. Although several studies [10, 11, 24–26] have reported the good clinical outcomes of MIPO, this meta-anal-ysis found no di�erence in terms of long term functional out-comes at one-year follow-up between MIPO and COP (� = 0.12).
Two studies [20, 23] showed mean operation time of MIPO was shorter than COP. However, Zehir et al. [22] reported the operation time of COP was shorter. Our meta-analysis found no signi§cant di�erence in operation time between MIPO and COP (� = 0.07). �ere was a signif-icant heterogeneity between the two groups (� < 0.00001, �2 = 94%), and sensitive analysis showed the total pooled e�ect size was greatly a�ected by the study of Zehir [22]. Operation time of COP was shorter than MIPO in the study of Zehir [22] might be due to repetitive ·uoroscopy use for fracture reduc-tion and placement of plate and high loss to follow-up (10/32) in the MIPO group.
MIPO technique, used to stabilize acute fractures without extensive so� tissue dissection, was believed to promote bone healing by preserving the enveloped so� tissue and periosteal circulation [10]. However, this meta-analysis found no signi§-cant di�erence in time to bone union between MIPO and COP groups (� = 0.70). �is might be due to low sample size of
for reason that both standard deviation and standard error were not available from the full text. A §xed-e�ects model was used without heterogeneity (� = 0.31, �2 = 17%). Finally, it was found that the Constant-Murley scores at one-year follow-up did not di�er between two groups (WMD = 0.99, 95% CI : −0.25 to 2.23; � = 0.12) (Figure 4).
3.4.2. Operation Time. Six studies [12, 13, 19, 20, 22, 23] which involved 243 cases provided data of operation time. �e random-e�ects model was performed due to a remarkable heterogeneity across studies (� < 0.00001, �2 = 94%). No signi§cant di�erence was found between MIPO and COP in the pooled estimate of operation time (WMD = −10.44, 95% CI : −21.63 to 0.75; � = 0.07) (Figure 5). Sensitive analysis showed that the total pooled e�ect size was greatly a�ected by the study of Zehir [22] (�2 = 93%; WMD = −14.77, 95% CI : −28.63 to −0.91; � = 0.04).
3.4.3. Time to Bone Union. Time to bone union was reported in all seven studies. However, one study [19] only reported the maximum and minimum values of healing time without mean values and standard deviation, thus a total of six studies [12, 13, 20–23] were included in this analysis. A random-e�ects model was applied due to the remarkable heterogeneity across studies (� = 0.03, �2 = 60%). �ere was no signi§cant statistical di�erence between MIPO and COP regarding time to bone union (WMD = −0.23, 95% CI : −1.42 to 0.96; � = 0.70) (Figure 6). In addition, a sensitive analysis by excluding outlier study [22] showed that the result was robust (�2 = 15%; WMD = 0.20, 95% CI : −0.62 to 1.02; � = 0.63).
3.4.4. Skin Numbness. Skin numbness or hypoesthesia was assessed in all seven studies with a minimum of 6 months
? ? ? ?
??+ –
– +
+ + +
+
Rand
om se
quen
ce g
ener
atio
n (s
elec
tion
bias
)
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
Blin
ding
of p
artic
ipan
ts a
nd p
erso
nnel
(per
form
ance
bia
s)
Blin
ding
of o
utco
me a
sses
smen
t (de
tect
ion
bias
)
Inco
mpl
ete
outc
ome
data
(attr
ition
bia
s)
Sele
ctiv
e re
port
ing
(rep
ortin
g bi
as)
Oth
er b
ias
Jiang 2012
Kim 2018
Figure 3: Risk of bias assessment summary of randomized controlled trials. “+” = risk of bias not present, “−” = risk of bias present, and “?” = insuºcient information to judge risk of bias.

5BioMed Research International
[28, 29]. Several investigations reported MIPO technique sig-ni§cantly reduced the anterior chest wall numbness compared with COP [19, 21]. Similarly, our meta-analysis found that MIPO was superior to OCP in skin numbness (� < 0.0001). Anatomically, no branch of supraclavicular nerve was found within 2.7 cm of the sternoclavicular joint or within 1.9 cm of the acromioclavicular joint [30]. �e medial and lateral inci-sion selected by the MIPO technique was precisely within these two areas with no neural branches. Although an addi-tional central incision on the fracture site is needed for ana-tomical reduction in MIPO (the technique used in studies of
included studies and the careful dissection during COP to avoid damaging blood supply. Although there was a signi§cant het-erogeneity between the two groups (� = 0.03, �2 = 60%), these §ndings were reliable because the result of sensitive analysis did not alter signi§cance by excluding the outlier study [22] (�2 = 15%; WMD = 0.20, 95% CI : −0.62 to 1.02; � = 0.63).
Previous studies have shown that anterior chest wall numbness is one of the most common complications in the treatment of clavicle fracture with plate, by reason of damage to branches of supraclavicular nerve [27, 28]. �e incidence of skin numbness a�er COP has been reported to be 12%–83%
–10 –5 0 5 10Favours COP
Constatnt-Murley score MIPOMean SD Total Total
WeightMean SD
COP Mean di�erence Mean di�erenceStudy or subgroup IV, Fixed, 95% CI IV, Fixed, 95% CI
Kim 2018 [18]Sohn 2015 [13]You 2018 [19]You 2019 [21]
88.4695.7594.1895.3
10.524.253.993.1
15 81.2719 94.7438 93.7420 94.1
8.364.463.714.1
15143520
3.3%16.9%49.4% 30.4%
7.19 [0.39, 13.99]1.01 [–2.01, 4.03]0.44 [–1.33, 2.21]1.20 [–1.05, 3.45]
Total (95% CI) 92 84 100.0% 0.99 [–0.25, 2.23]Heterogeneity: χ2 = 3.60, df = 3 (P = 0.31); I2 = 17%Test for overall e�ect: Z = 1.57 (P = 0.12)
Favours MIPO
Figure 4: Forest plot diagram of Constant-Murley scores compared between MIPO and COP.
Operation time (min)
Study or Subgroup Mean
MIPO COP
SD Total Mean SD TotalWeight Mean di�erence Mean di�erence
IV, Random, 95% Cl IV, Random, 95% Cl
Beirer 2015 [19]Jiang 2012 [12]Kim 2018 [20]Sohn 2015 [13]You 2019 [23]Zehir 2018 [22]
93.5 26.611.2513.8717.32
6.27.78
6052.3377.1936.7
53.59
12 97.1 24.9 12 11.8% –3.60 [–24.22, 17.02]0.00 [–5.51, 5.51]
–58.00 [–72.64, –43.36]–10.31 [–22.86, 2.24]–5.70 [–9.86, –1.54]
6.69 [3.03, 10.35]
18.9%14.8%15.8%19.3%19.4%
3215142030
11.2525.3918.79
7.24.72
60110.33
87.542.446.9
3215192022
Favours MIPO Favours COP–50 –25 0 25 50
Total (95% CI) 120 123 100.0% –10.44 [–21.63, 0.75]Heterogeneity: τ2 = 164.68; χ2 = 82.34, df = 5 (P <0.00001); I2 = 94% Test for overall e�ect: Z = 1.83 (P = 0.07)
Figure 5: Forest plot diagram of operation time (min) compared between MIPO and COP.
Time to bone union (weeks)
Study or Subgroup Mean SD Total Mean
COP
SD TotalWeight Mean di�erence Mean di�erence
IV, Random, 95% CI IV, Random, 95% CI
–10 –5 0 5 10Favours MIPO Favours COP
Jiang 2012 [12] 12 3 32 13 4 32 18.9% –1.00 [–2.73, 0.73]4.07 [–2.89, 11.03]1.09 [–1.27, 3.45]0.80 [–0.46, 2.06]
–0.10 [–1.22, 1.02]–2.86 [–4.90, –0.82]
–0.23 [–1.42, 0.96]
2.7%14.1%23.3%24.7%16.4%
1514352030
6.532.932.51.9
4.52
17.1315.6915.314.416.5
1519382022
12.13.98
31.7
2.98
21.216.7816.114.3
13.64
Kim 2018 [20]Sohn 2015 [13]You 2018 [21]You 2019 [23]Zehir 2018 [22]
Total (95% CI)Heterogeneity: τ2 = 1.17; χ2 = 12.35, df = 5 (P = 0.03); I2 = 60%Test for overall e�ect: Z = 0.38 (P = 0.70)
146 146 100.0%
MIPO
Figure 6: Forest plot diagram of time to bone union (weeks) compared between MIPO and COP.

BioMed Research International6
MIPO
Events Total Events TotalWeight
M-H, Fixed, 95% Cl
Skin numbness
Study or Subgroup
COPOdds ratio Odds ratio
M-H, Fixed, 95% Cl
0.002Favours MIPO Favours COP
0.1 1 10 500
Beirer 2015 [19]Jiang 2012 [12]Kim 2018 [20]Sohn 2015 [13]You 2018 [21]You 2019 [23]Zehir 2018 [22]
10 12 9 12 3.6% 1.67 [0.22, 12.35]0.15 [0.03, 0.74]0.29 [0.03, 3.12]0.06 [0.00, 1.22]0.26 [0.08, 0.82]0.16 [0.02, 1.50]0.28 [0.05, 1.45]
22.7%6.8%
12.1%28.4%11.5%14.9%
321514352030
1034
1358
321519382022
210512
Total (95% CI) 158 158 100.0% 0.25 [0.13, 0.48]Total events 21 52Heterogeneity: χ2 = 4.91, df = 6 (P = 0.56); I2 = 0%Test for overall e�ect: Z = 4.20 (P < 0.0001)
Figure 7: Forest plot diagram of skin numbness compared between MIPO and COP.
0.005 0.1 1 10 200Favours MIPO Favours COP
Complications MIPO COPOdds ratio
M-H, Fixed, 95% CIOdds ratio
M-H, Fixed, 95% CIStudy or Subgroup Events
0 12 06
1226.0%
Not estimable
Not estimable0.67 [0.13, 3.30]0.09 [0.00, 1.75]0.32 [0.01, 8.26]0.53 [0.17, 1.61]
0.06 [0.00, 1.17]
14.8%18.8%5.9%
34.5%
321514352030
0441
17
321519382022
004009
Total Events TotalWeight
Beirer 2015 [19]Jiang 2012 [12]Kim 2018 [20]Sohn 2015 [13]You 2018 [21]You 2019 [23]Zehir 2018 [22]
Total eventsHeterogeneity: χ2 = 3.38, df = 4 (P = 0.50); I2 = 0%Test for overall e�ect: Z = 2.83 (P = 0.005)
Total (95% CI) 15813 32
158 100.0% 0.33 [0.16, 0.71]
Figure 8: Forest plot diagram of complications compared between MIPO and COP.
Table 1: Quality assessment of nonrandomized studies (methodological index for nonrandomized studies).
�e items are scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate).
Beirer 2015 [19] Sohn 2015 [13] You 2018 [21] Zehir 2018 [22] You 2019 [23]A clearly stated aim 2 2 2 2 2Inclusion of consecutive patients 2 2 2 2 2Prospective data collection 2 0 2 0 0End points appropriate to the aim of the study 1 2 2 2 2Unbiased assessment of the study end point 0 0 0 0 0A follow-up period appropriate to the aims of
study 1 2 2 2 2
Less than 5% loss to follow-up 2 2 2 0 2Prospective calculation of the sample size 0 0 0 0 0An adequate control group 2 2 2 2 2Contemporary groups 2 2 2 2 2Baseline equivalence of groups 2 2 2 2 2Adequate statistical analyses 2 2 2 2 2Total score 18 18 20 16 18

7BioMed Research International
Tabl
e 2:
Cha
ract
erist
ics o
f the
stud
ies.
M =
mal
es, F
= fe
mal
es, R
CT
= ra
ndom
ized
cont
rolle
d tr
ial,
RC =
retr
ospe
ctiv
e coh
ort,
PC =
pros
pect
ive c
ohor
t, M
IPO
= m
inim
ally
inva
sive p
late
ost
eosy
nthe
sis, C
OP
= co
nven
tiona
l ope
n pl
atin
g, O
TA =
orth
opae
dic
Trau
ma
Ass
ocia
tion.
Firs
t aut
hor
Year
Stud
y de
sign
Gro
upTo
tal n
umbe
rM
ean
age (
year
s)G
ende
r (M
/F)
Follo
w-u
p (m
onth
s)Fr
actu
re cl
assifi
catio
nO
pera
tive
tech
niqu
e
Jiang
[12]
2012
RCT
MIP
O32
4020
/12
15Ro
bins
on 2
B1, 2
B2
A ce
ntra
l inc
ision
ove
r the
frac
ture
sit
e (3
cm),
a di
stal
inci
sion
(1 cm
) an
d a
prox
imal
inci
sion
(1 cm
)
CO
P32
4520
/12
15A
tran
sver
se in
cisio
n ov
er th
e fr
ac-
ture
site
(8–1
0 cm
)
Sohn
[13]
2015
RCM
IPO
1946
.79
18/1
17.6
AO
/OTA
15.
2A, 1
5.2B
, 15
.2C
Two
smal
l ski
n in
cisio
ns (t
he m
edi-
al a
nd la
tera
l sid
es o
f the
clav
icle
)
CO
P14
44.1
412
/217
.6A
tran
sver
se in
cisio
n ov
er th
e fr
actu
re si
te
Beire
r [19
]20
15PC
MIP
O12
34.9
211
/16
AO
/OTA
15.
2A, 1
5.2B
, 15
.2C
A ce
ntra
l inc
ision
ove
r the
frac
ture
sit
e, a
med
ial s
tab
inci
sion
and
a la
tera
l sta
b in
cisio
n
CO
P12
41.4
211
/16
A tr
ansv
erse
inci
sion
over
the
frac
ture
site
Kim
[20]
2018
RCT
MIP
O15
38.1
310
/513
.33
AO
/OTA
15.
2A, 1
5.2B
, 15
.2C
Two
smal
l ski
n in
cisio
ns (t
he m
edi-
al a
nd la
tera
l sid
es o
f the
clav
icle
)
CO
P15
38.1
511
/413
.73
A tr
ansv
erse
inci
sion
over
the
frac
ture
site
You
[21]
2018
PCM
IPO
3838
.320
/18
12Ro
bins
on 2
A2,
2B1
, 2B2
Two
smal
l ski
n in
cisio
ns (t
he m
edi-
al a
nd la
tera
l sid
es o
f the
clav
icle
)
CO
P35
36.9
18/1
712
A tr
ansv
erse
inci
sion
over
the
frac
ture
site
Zehi
r [22
]20
18RC
MIP
O22
32.3
212
/10
14.5
6A
O/O
TA 1
5.2B
, 15.
2C
A ce
ntra
l inc
ision
ove
r the
frac
ture
sit
e, a
dist
al in
cisio
n an
d a
prox
imal
in
cisio
n (2
–3 cm
)
CO
P30
34.7
18/1
214
.79
A tr
ansv
erse
inci
sion
over
the
frac
ture
site
You
[23]
2019
RCM
IPO
2037
.211
/912
Robi
nson
2A
2, 2
B1, 2
B2
Two
smal
l ski
n in
cisio
ns (t
he m
edi-
al a
nd la
tera
l sid
es o
f the
clav
icle
)
CO
P20
35.1
13/7
12A
tran
sver
se in
cisio
n ov
er th
e fr
actu
re si
te

BioMed Research International8
numbness and complications appear to occur more frequently when COP is used. High quality clinical trials which include larger sample sizes and longer follow-up time are required to con§rm our conclusion.
Conflicts of Interest
�e authors declare that they have no con·icts of interest.
Acknowledgments
We would like to thank Yuehong Ma, MSc for kindly providing statistical consultation.
References
[1] O. A. van der Meijden, T. R. Gaskill, and P. J. Millett, “Treatment of clavicle fractures: current concepts review,” Journal of Shoulder and Elbow Surgery, vol. 21, no. 3, pp. 423–429, 2012.
[2] B. Wiesel, S. Nagda, S. Mehta, and R. Churchill, “Management of midsha� clavicle fractures in adults,” �e Journal of the American Academy of Orthopaedic Surgeons, vol. 26, no. 22, pp. e468–e476, 2018.
[3] N. Hussain, C. Sermer, P. J. Prusick, L. Ban§eld, A. Atrey, and M. Bhandari, “Intramedullary nailing versus plate §xation for the treatment displaced midsha� clavicular fractures: a systematic review and meta-analysis,” Scienti�c Reports, vol. 6, p. 34912, 2016.
[4] J. Nowak, M. Holgersson, and S. Larsson, “Sequelae from clavicular fractures are common: a prospective study of 222 patients,” Acta Orthopaedica, vol. 76, no. 4, pp. 496–502, 2005.
[5] M. D. McKee, E. M. Pedersen, C. Jones et al., “De§cits following nonoperative treatment of displaced midsha� clavicular fractures,” �e Journal of Bone and Joint Surgery American, vol. 88, no. 1, pp. 35–40, 2006.
[6] R. C. McKee, D. B. Whelan, E. H. Schemitsch, and M. D. McKee, “Operative versus nonoperative care of displaced midsha� clavicular fractures: a meta-analysis of randomized clinical trials,” �e Journal of Bone and Joint Surgery American, vol. 94, no. 8, pp. 675–684, 2012.
[7] E. Guerra, D. Previtali, S. Tamborini, G. Filardo, S. Za�agnini, and C. Candrian, “Midsha� clavicle fractures: surgery provides better results as compared with nonoperative treatment: a meta-analysis,” �e American Journal of Sports Medicine, 2019.
[8] F. J. Wijdicks, O. A. Van der Meijden, P. J. Millett, E. J. Verleisdonk, and R. M. Houwert, “Systematic review of the complications of plate §xation of clavicle fractures,” Archives of Orthopaedic and Trauma Surgery, vol. 132, no. 5, pp. 617–625, 2012.
[9] C. Krettek, P. Schandelmaier, T. Miclau, and H. Tscherne, “Minimally invasive percutaneous plate osteosynthesis (MIPPO) using the DCS in proximal and distal femoral fractures,” Injury, vol. 1383, no. 97, pp. A20–A30, 1997.
[10] H. S. Sohn, B. Y. Kim, and S. J. Shin, “A surgical technique for minimally invasive plate osteosynthesis of clavicular midsha� fractures,” Journal of Orthopaedic Trauma, vol. 27, no. 4, pp. e92–96, 2013.
Jiang [12], Beirer [19] and Zehir [22]), the incision length and so� tissue forcible retraction in MIPO were still less than COP. �ese might explain the reason why skin numbness occurred more o�en in the COP group.
In this meta-analysis, complications such as infection, hypertrophic scaring, nonunion, refracture, implant failure, skin irritation, and painful shoulder were evaluated also. �e reason why these complications were pooled together was that the sample size would be smaller if each complication was assessed separately. Pooled results indicated that patients receiving COP had more complications than MIPO, and this was found to be signi§cant (� = 0.005). Five of the included studies reported no major complications such as nonunion, re-fracture, and implant failure in both groups [12, 19–21, 23].�is might be due to the low sample size of included studies.
To our knowledge, this is the §rst systematic review and meta-analysis comparing MIPO and COP for the treatment of midsha� clavicle fractures. However, there were several limitations that should be noted. First, there were only two RCTs that met the eligibility criteria, and the sample sizes were small in most studies. Second, the follow-up duration was relatively short and might underestimate the complications. �ird, due to the lack of relevant data, we could not perform subgroup analysis according to fracture classi§cation. Finally, the existence of bias, owing to di�erent surgeons and surgical technologies, might have been inevitable in our research.
5. Conclusion
�is systematic review and meta-analysis found no di�erences in terms of functional outcomes, operation time, and fracture healing time between MIPO and COP. However, skin
Table 3: Reported complications between MIPO and COP groups.
aNeed operation, bnot need operation.
Study MIPO COP
Jiang 2012 [12]5 Hypertrophic
scarring1 Painful shoulder
Sohn 2015 [13]
1 Implant failure or screw looseninga
1 Implant failure or screw looseningb
2 Skin irritation or discomfort due to plate prominence
3 Skin irritation or discomfort due to plate prominence
1 NonunionBeirer 2015 [19]Kim 2018 [20]You 2018 [21] 4 Hypertrophic
scarring
Zehir 2018 [22]
1 Infection 2 Infection3 Skin irritation 4 Skin irritation
4 Painful shoulder 7 Painful shoulder1 Implant failurea 2 Implant failurea
2 NonunionYou 2019 [23] 1 InfectionTotal 13 32

9BioMed Research International
technique to aid the reduction with nail assistance,” Injury, vol. 44, no. 4, pp. 465–470, 2013.
[26] Y. Tieyi, L. Shuyi, Z. Yan, H. Guohua, S. Jin, and J. Rui, “Minimally invasive plating for fresh displaced midsha� fractures of the clavicle,” Orthopedics, vol. 37, no. 10, pp. 679–683, 2014.
[27] K. Wang, A. Dowrick, J. Choi, R. Rahim, and E. Edwards, “Post-operative numbness and patient satisfaction following plate fixation of clavicular fractures,” Injury, vol. 41, no. 10, pp. 1002–1005, 2010.
[28] T. J. Christensen, D. S. Horwitz, and E. N. Kubiak, “Natural history of anterior chest wall numbness a�er plating of clavicle fractures: educating patients,” Journal of Orthopaedic Trauma, vol. 28, no. 11, pp. 642–647, 2014.
[29] W. J. Shen, T. J. Liu, and Y. S. Shen, “Plate fixation of fresh displaced midsha� clavicle fractures,” Injury, vol. 30, no. 7, pp. 497–500, 1999.
[30] T. Nathe, S. Tseng, and B. Yoo, “�e anatomy of the supraclavicular nerve during surgical approach to the clavicular sha�,” Clinical Orthopaedics and Related Research, vol. 469, no. 3, pp. 890–894, 2011.
[11] Y. Zhang, J. Xu, C. Zhang, and Y. Sun, “Minimally invasive plate osteosynthesis for midsha� clavicular fractures using superior anatomic plating,” Journal of Shoulder and Elbow Surgery, vol. 25, no. 1, pp. e7–e12, 2016.
[12] H. Jiang and W. Qu, “Operative treatment of clavicle midsha� fractures using a locking compression plate: comparison between mini-invasive plate osteosynthesis (MIPPO) technique and conventional open reduction,” Orthopaedics & Traumatology, Surgery & Research, vol. 98, no. 6, pp. 666–671, 2012.
[13] H. S. Sohn, W. J. Kim, and M. S. Shon, “Comparison between open plating versus minimally invasive plate osteosynthesis for acute displaced clavicular sha� fractures,” Injury, vol. 46, no. 8, pp. 1577–1584, 2015.
[14] E. G. Meinberg, J. Agel, C. S. Roberts, M. D. Karam, and J. F. Kellam, “Fracture and dislocation classification compendium-2018,” Journal of Orthopaedic Trauma, vol. 32, no. suppl 1, pp. S1–S10, 2018.
[15] C. M Robinson, “Fractures of the clavicle in the adult,” �e Journal of Bone and Joint Surgery. British volume, vol. 80-B, no. 3, pp. 476–484, 1998.
[16] J. P. Higgins, D. G. Altman, P. C. Gotzsche et al., “�e cochrane collaboration's tool for assessing risk of bias in randomised trials,” BMJ (Clinical research ed), vol. 343, p. d5928, 2011.
[17] K. Slim, E. Nini, D. Forestier, F. Kwiatkowski, Y. Panis, and J. Chipponi, “Methodological index for non-randomized studies (minors): development and validation of a new instrument,” ANZ Journal of Surgery, vol. 73, no. 9, pp. 712–716, 2003.
[18] Review Manager (RevMan), �e Nordic Cochrane Centre, �e Cochrane Collaboration, Copenhagen, 5.3 edn edition, 2014.
[19] M. Beirer, L. Postl, M. Cronlein et al., “Does a minimal invasive approach reduce anterior chest wall numbness and postoperative pain in plate fixation of clavicle fractures?,” BMC Musculoskeletal Disorders, vol. 16, no. 1, 2015.
[20] J. Y. Kim, B. C. Yoo, J. P. Yoon, S. J. Kang, and S. W. Chung, “A comparison of clinical and radiological outcomes of minimally invasive and conventional plate osteosynthesis for midsha� clavicle fractures,” Orthopedics, vol. 41, no. 5, pp. e649–e654, 2018.
[21] J. M. You, Y. S. Wu, and Y. Wang, “Comparison of post-operative numbness and patient satisfaction using minimally invasive plate osteosynthesis or open plating for acute displaced clavicular sha� fractures,” International Journal of Surgery, vol. 56, pp. 21–25, 2018.
[22] S. Zehir, E. Sahin, M. Songür, T. Altunkiliç, and G. ÖZdemir, “Minimal invasive percutaneous plate osteosynthesis (MIPPO) vs. open plating in superior plating of midsha� clavicle fractures,” Acta Orthopaedica Belgica, vol. 84, no. 4, pp. 491–496, 2018.
[23] J. M. You, Y. S. Wu, and Y. Wang, “Case-control study on minimally invasive surgery and conventional open plating for displaced midsha� clavicular fracture based on 3D-print,” Zhongguo gu shang = China journal of orthopaedics and traumatology, vol. 32, no. 1, pp. 5–10, 2019.
[24] G. H. Jung, C. M. Park, and J. D. Kim, “Biologic fixation through bridge plating for comminuted sha� fracture of the clavicle: technical aspects and prospective clinical experience with a minimum of 12-month follow-up,” Clinics in orthopedic surgery, vol. 5, no. 4, pp. 327–333, 2013.
[25] H. J. Lee, C. W. Oh, J. K. Oh et al., “Percutaneous plating for comminuted midsha� fractures of the clavicle: a surgical

Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Disease Markers
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwww.hindawi.com Volume 2013
Hindawiwww.hindawi.com Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwww.hindawi.com Volume 2018
PPAR Research
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwww.hindawi.com Volume 2018
Journal of
ObesityJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwww.hindawi.com Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwww.hindawi.com Volume 2018
Diabetes ResearchJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Research and TreatmentAIDS
Hindawiwww.hindawi.com Volume 2018
Gastroenterology Research and Practice
Hindawiwww.hindawi.com Volume 2018
Parkinson’s Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwww.hindawi.com
Submit your manuscripts atwww.hindawi.com